
Abstract
Even with technological advances in point-of-care rapid testing for HIV, hepatitis, and syphilis, individuals may still find the experience of submitting to testing, and receiving results, to be stressful. Participants completed the rapid test experience questionnaires to assess stress both prior to and after the specimen collection. Participants completed the risk behavior assessment, the coping strategies indicator, and the Barratt impulsivity scale. Participants chose which rapid tests they wanted using a list administered via computer. Logistic regression analysis was used to model self-reported stress prior to testing and after testing. A total of 1097 individuals completed testing. Individuals who scored high on avoidance reported a stressful experience at pretest (OR = 1.15, CI = 1.04, 1.26) while higher educational attainment was associated with no stress at both time points. Injection drug users, avoidant, and impulsive individuals experience stress either before or after rapid testing. Education appears to be protective against stressful testing.
Keywords
Currently, there are approximately 1.2 million people infected with human immunodeficiency virus (HIV) in the United States, with many more, approximately 3.2 million, infected with hepatitis C virus (HCV).1,2 Worldwide more pregnant women are infected with syphilis than HIV. 3 Rapid point-of-care (POC) HIV, syphilis, and HCV testing, which requires between 1 and 40 min to receive results using finger-stick capillary blood, allows for screening to be expanded outside of traditional clinical settings. Rapid POC testing has the potential to increase the number of individuals who receive test results with greatly reduced waiting time for results, resulting in increases in the number of individuals who learn that they are infected4–6 and who may subsequently enter treatment. POC rapid testing for HIV, as well as other infections such as syphilis and HCV, has advantages over routine laboratory testing in low-resource environments.7–10
Many studies have illustrated the high frequency of failure to return for HIV, HCV, and sexually transmitted infection (STI) test results that require laboratory processing of specimens and waiting times of from one to two weeks before results are available for the patient.11–18 A recent randomized controlled trial found differences between the standard serology-based arm (testing for hepatitis B, C, and HIV) of the study and the group randomized to simultaneous rapid POC tests for the same infections; only 64% of clients in the standard arm were tested and returned for results compared to 98% in the group receiving the rapid POC tests. 19
Few studies have attempted to directly examine the differences that cause an individual to choose between a rapid and standard HIV test when given a choice. One study by Marsh et al. 20 examined the differences between those who chose a standard HIV test and those who chose a rapid HIV test. Those who chose standard HIV testing were more likely to be Black, injection drug user (IDUs), and those who self-identified as homeless, while men who have sex with men (MSM) were more likely to choose the rapid test; these findings are consistent with other studies.16,21 One U.S. study found that among HIV testing clients, most preferred HIV rapid testing, but they were concerned about the accuracy or lack thereof of the rapid test. 22 Lack of trust in POC testing for HIV was a reason for opting for the standard two-week nonrapid testing. 23 Emergency department (ED)-based testing using either an ‘opt in’ or ‘opt out’ approach has been facilitated by the rapid POC tests, with mixed findings. Acceptance rates for ED-based HIV testing among patients ranges from around 48% 24 to 77%; 25 participants provided multiple reasons for not accepting rapid testing in the ED.24–27
Stressful testing is not only associated with HIV tests, but with testing for heart disease 28 and breast cancer, 29 mammogram results, 30 waiting for pregnancy test results after undergoing fertility testing, 31 and cystic fibrosis 32 to name only a few. The purpose of this study was to allow participants to choose which simultaneous POC rapid tests they wished to receive and then to assess how stressful the experience was: (a) before the tests were administered (but after test choice) and (b) after results of the rapid tests were received.
Method
The present study (Behavioral Aspects of Rapid Test Acceptance [BSARTA]) recruited participants through the Center for Behavioral Research and Services in Long Beach, California. In order to be eligible, participants had to be at least 15 years of age and have photo identification. The protocol was approved by the California State University Long Beach, Institutional Review Board.
Participants
The procedures for this study have been reported previously33,34 but briefly, clients who came in for HIV and other STI testing were screened for eligibility using a screening form developed for the study and based on behavioral risk groups (BRGs) as stipulated by the Office of AIDS Programs & Policy of the Los Angeles County Department of Public Health. BRGs were defined as follows: (1) IDUs with verified track marks (e.g. visible signs of injection); 35 (2) women who reported at least two male partners in the last two years or engaging in anal intercourse, sex trading, or sex with a men who have sex with men (MSM), an IDU, or an HIV-positive man; (3) MSM and men who have sex with men and women (MSMW); and (4) transgender (TRG) individuals. The program tested the accuracy of different experimental rapid tests for HIV, hepatitis B and C, and syphilis and has been described in detail previously.33,34 The prestudy HIV prevalence was 2.62%, the prestudy prevalence of HCV was 48.13%, the prestudy prevalence of syphilis rapid plasma reagin was 2.96%, and the prestudy prevalence of syphilis Treponema pallidum-particle agglutination was 8.08%. 33
Participants were presented a menu of rapid POC tests via computer. Prior known HIV or other positive test results were not used to place restrictions on the tests participants could select. Participants completed a number of behavioral risk and other assessments including the BSARTA screening form; the risk behavior assessment (RBA); 36 the coping strategies indicator (CSI);37,38 and a standardized measures of impulsivity, the Barratt Impulsiveness Scale (BIS). 39 Participants received a list of the different rapid tests they could choose from including information on the type of specimen required (oral fluid or whole blood), the length of time required for the test from specimen collection to result (1–40 min), and the blood-borne infection being tested for; some test kits were combination tests (i.e. HIV + HCV, HIV + HCV + syphilis). Participants chose which tests they wished to receive using a computer program with touch screen and these choices went into a shopping basket. The information from the shopping basket was then used by phlebotomists in performing the actual tests.
A California state licensed phlebotomist drew a venous blood sample, by standard laboratory practices, for the POC tests, as well as the gold standard confirmatory tests (which were required by the study protocol). Participants were given the results of the POC tests by the phlebotomist/HIV test counselor as soon as they were available (1–40 min, depending upon the test kit).
Measures
BSARTA screening form
The screener used for the study was to assess classification into one of the BRGs: (1) IDUs with verified track marks (e.g. visible signs of injection); 35 (2) women who reported at least two male partners in the last two years or engaging in anal intercourse, sex trading, or sex with a MSM, an IDU, or an HIV-positive man; (3) MSM and MSMW; and (4) TRG individuals. It was also used to collect information on whether eligible individuals accepted or declined to participate in the study.
RBA
The RBA is a structured interview that captures the risky drug and sexual behaviors in a participants’ lifetime, as well as their recent (in the last 30 days) risky behaviors. Many previous studies have shown high test–retest reliability of RBA items regarding drug use, sexual behavior, and HIV risk behaviors.36,40,41
CSI
The CSI37,38 is a 33-item measure that assesses three types of coping behaviors: avoidance, seeking support, and problem-solving. The responses are measured on a three-point scale of: ‘a lot’ (3), ‘a little’ (2), or ‘not at all’ (1) with higher scores on a subscale indicate a greater use of the coping behavior. The Cronbach’s alpha coefficients for the problem-solving subscale, seeking social support subscale, and avoidance subscale were found to be.89, .93, and .84, respectively. 37
Impulsivity measure
The BIS-11 is a 30-item measure of impulsivity and has 11 items assessing nonimpulsiveness. 42 The BIS asks respondents to indicate the frequency with which they engage in impulsive or nonimpulsive behaviors using a four-point Likert scale ranging from ‘Rarely/Never’ to ‘Almost always/Always.’ Three subscales assessing the core aspects of impulsivity including attentional impulsivity, nonplanning impulsivity, and motor impulsivity as well as a total score are derived from item responses. 43 The total score has a test–retest reliability of .83 and a Cronbach α = .83. The attentional subscale has a reliability of .61 and α = .74. The motor subscale has a reliability of .67 and α = .59. The nonplanning subscale has a reliability of .72 and α = .72.
Rapid test choice
The rapid test choice questionnaire was administered to participants immediately following test choice via computer, but before any specimen collection (finger stick, oral swab). The specific question used for assessing pretest stress was, ‘The idea of getting more than one test was stressful.’ The response option was a dichotomous response of Yes/No.
Rapid test experience
The rapid test experience questionnaire was administered to participants to assess whether or not the participant experienced stress immediately after receiving the results of the rapid test(s). The main outcome variable for the assessment of posttest stress was the question: ‘Getting the results of the rapid test(s) was stressful’ with a dichotomous response option of Yes/No.
Statistical analysis
Univariate and bivariate statistical analyses were conducted to identify factors associated with pre- or posttest stress. Bivariate tests were also conducted to determine whether any of the POC tests were more or less likely to be chosen by participants because of associations with the two stress outcome variables. For participants who actually chose each of the tests (rather than those whose pretest stress led them to avoid or fail to choose tests), additional analysis was conducted to determine whether the test, once chosen, was associated with pre- or posttest stress. Empirical results of the bivariate tests were then used to develop two separate logistic regression models for the two stress outcomes. The data were analyzed in SAS 9.1.3 service pack 4. Model building followed methods for selecting variables and a method for assessing adequacy presented in Hosmer et al. 44 We aimed to identify a parsimonious model: one that was numerically stable, more easily adopted by others, with small standard errors. The first step in the Hosmer et al. purposeful selection method of model building is to start with a careful univariable analysis of each candidate independent variable. The logistic regression models used reference cell coding for the categorical variables of education and marital status in accordance with recommendations in Hosmer et al. 44
Results
Sample demographics and categorical variables for sample by pretest ‘the idea of getting more than one test was stressful.’
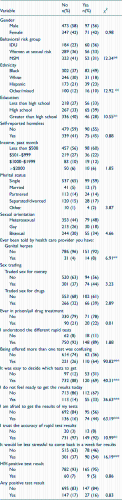
IDU: injection drug user; HIV: human immunodeficiency virus; MSM: men who have sex with men.
Note: **p < .01, ***p < .001.
Sample demographics and categorical variables for sample by posttest ‘getting the results of the rapid tests was stressful.’
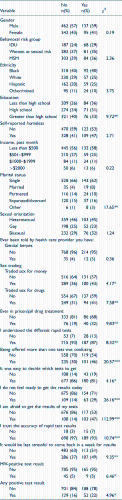
IDU: injection drug user; HIV: human immunodeficiency virus; MSM: men who have sex with men.
Note: *p < .05, **p < .01, ***p < .001.
Several perception variables were significantly associated with stressful testing including reporting that being offered more than one test was confusing, finding that it was easy to decide which tests to get, not feeling ready to receive test results today, being afraid of getting the results of the rapid tests, lack of trust in the accuracy of the rapid tests, and endorsing that it would be less stressful to come back in a week to get test results. Having received a positive test result for HIV was associated with stressful testing at posttest.
Selected continuous variables with ‘the idea of getting more than one test was stressful’ at pretest.
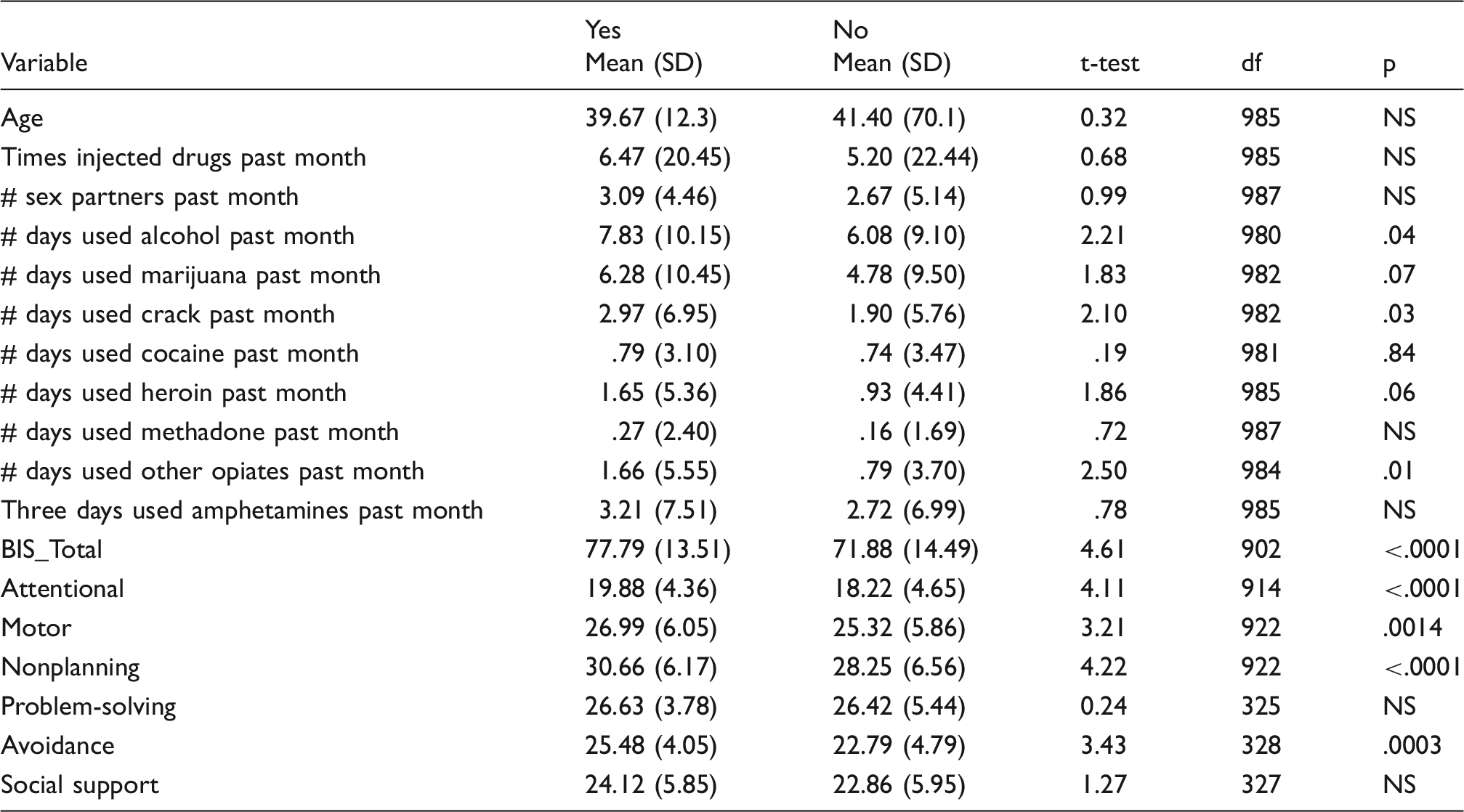
#: number of; NS: not significant; SD: standard deviation.
Selected continuous variables with ‘getting the results of the rapid tests was stressful’ at posttest.

#: number of; NS: not significant; SD: standard deviation.
Test kit chosen for sample by pretest variable (‘The idea of getting more than one test was stressful’).
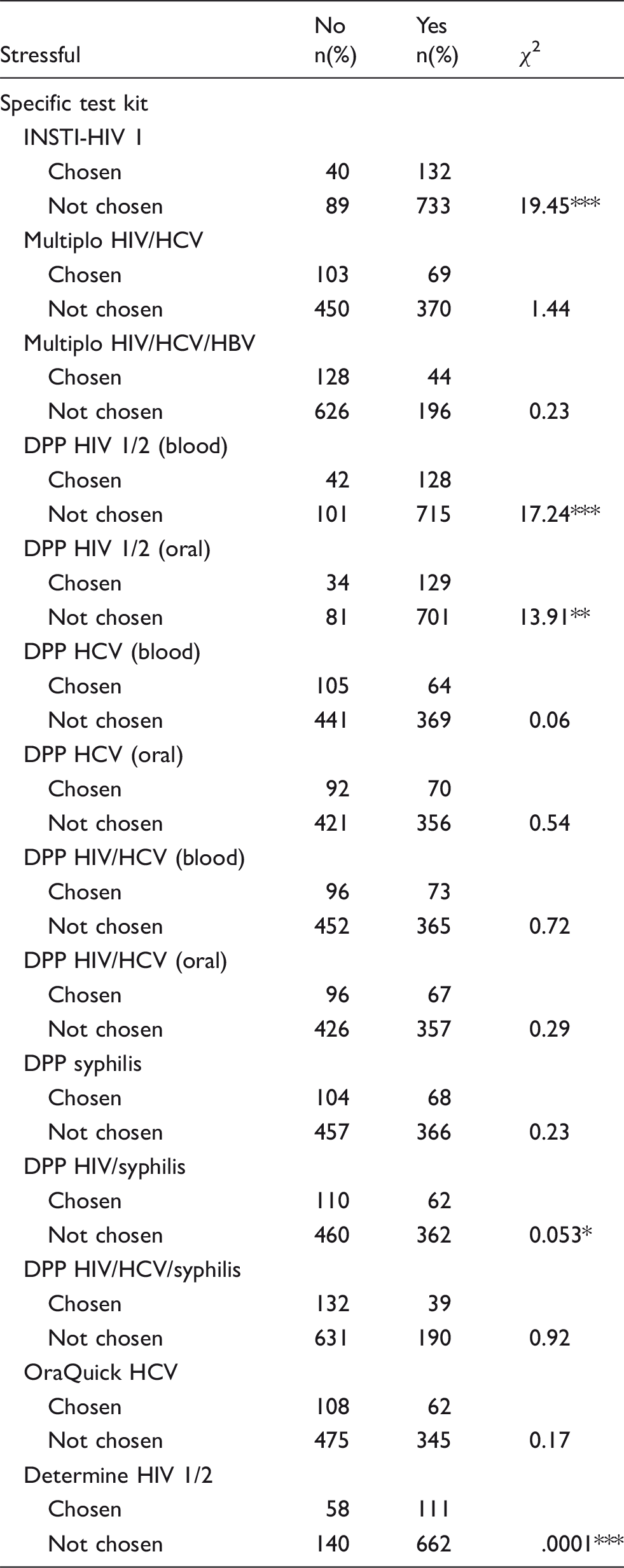
DPP: Dual Path Platform; HBV: hepatitis B virus; HCV: hepatitis C virus; HIV: human immunodeficiency virus.
Note: *p < .05, **p < .01, ***p < .001.
Logistic regression model predicting ‘the idea of getting more than one test was stressful.’
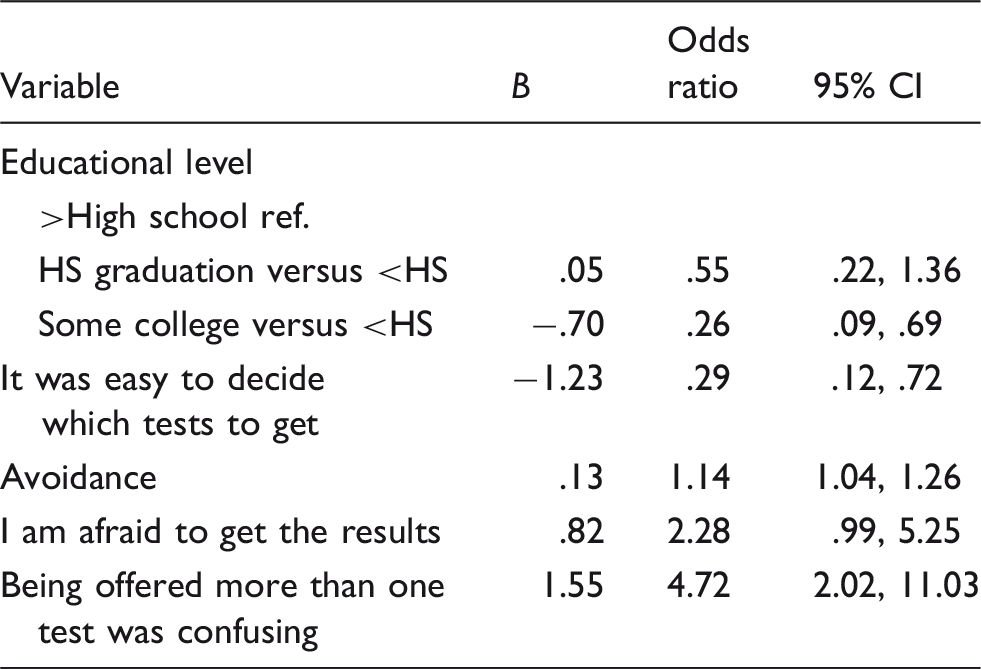
CI: confidence interval; HS: high school.
Logistic regression model predicting ‘getting the results of the rapid tests was stressful.’
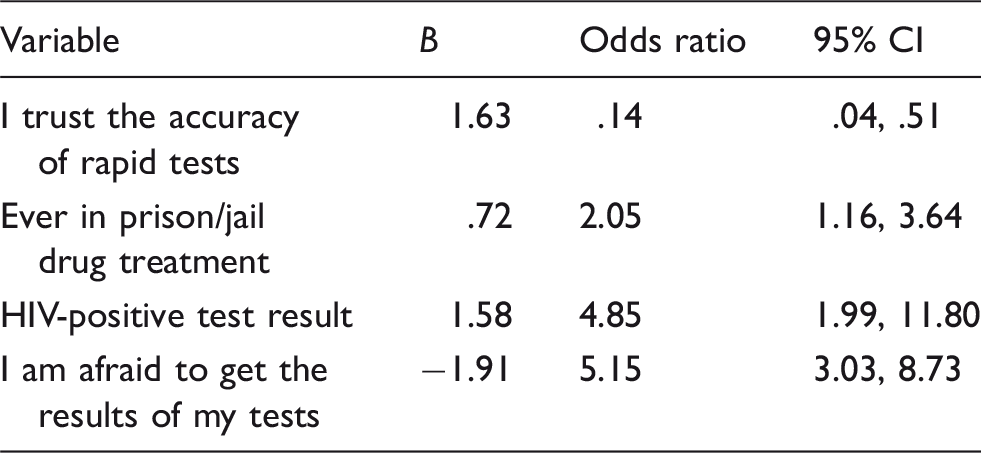
CI: confidence interval
Discussion
This study examined factors associated with stressful POC testing for HIV, hepatitis C, and syphilis, which may be delivered as single or combinations of bundled tests requiring the collection of a single specimen (oral or finger stick) for testing. These tests have demonstrated advantages. Depending upon local health department regulations, a preliminary positive may be immediately confirmed with another POC test and the patient referred for treatment. An additional advantage is that patients do not need to wait one to two weeks to receive test results and providers do not need to expend resources in tracking patients to ensure that laboratory results are delivered. While these advantages have greatly increased both access to HIV and STI testing, as well as facilitated early entry into care for individuals with positive test results, POC rapid testing has not completely reduced the stress of being tested for infections such as HIV.
The current study found several factors associated with POC rapid test stress both before and after administration of the tests. Low educational attainment is associated with a stressful testing experience and higher levels of education appear to mitigate against stressful testing. Being a current or former IDU, and ever having traded sex for drugs were both associated with a stressful testing experience. Impulsivity as measured by the subscales of the BIS was significantly associated with both pre- and posttest stress. All of the subscale scores (motor, attentional, nonplanning) were significantly associated with stress at both time points. We hypothesize that impulsive individuals may have chosen tests without considering that they would then be receiving multiple, and possibly positive, test results.
An individual’s perception of risk for HIV has been reported previously as being associated with agreeing to be tested with the standard HIV test requiring one- to two-week turnaround time. 18 The time lag between being tested and receiving the results of the test is greatly truncated with rapid POC testing. This study found that when individuals are provided with a choice of which POC tests to undergo, they are significantly less likely to choose single HIV POC rapid tests. However, once they have chosen tests to undergo, the single HIV POC rapid tests were negatively associated with pretest stress. This could be because individuals who fear the results they may receive from an HIV test simply did not choose an HIV test, while those who chose the HIV tests knew or were confident in what those test results would be, therefore they were not stressed about it. POC tests that bundled HIV with one or more other infections (HCV, syphilis) were not associated with pre- or posttest stress. It is possible that the novelty associated with multiple POC tests reduced stress in some way, perhaps because the participants simply did not understand the multiple tests. Other studies have reported high satisfaction with rapid POC testing for combined HIV and syphilis testing7,8 as well as HIV rapid POC tests.5,6 However, those studies did not measure the stress associated with receiving rapid test results for more than one test. More research is needed to understand how multiple POC rapid tests affect participants’ stressful testing experiences as a stressful experience and satisfaction with the testing process are not mutually exclusive.
One coping mechanism for dealing with stressful situations is avoidance. With standard testing, avoidance is accomplished by not returning to receive the test results. Avoidance may manifest differently under rapid POC testing. Previous studies have shown that individuals high on avoidant coping will choose the regular HIV test over a rapid test, knowing they can postpone getting test results due to laboratory processing time. 20 HIV pretest counseling may not completely mitigate against the stress of POC rapid testing. Findings from this study indicate that, if given a choice, participants will avoid those tests which they personally find stressful (i.e. rapid HIV tests). However, for those who chose them, the rapid HIV tests were inversely associated with pretest stress. None of the POC tests were associated with pre- or posttest stress in the multivariate models. However, receiving an HIV-positive test result was associated with posttest stress. For those individuals who chose an HIV test, either as a single test or as part of a combination test, getting a positive test result was stressful. These individuals are most likely to be those who did not know or suspect that they were HIV-positive as they could have avoided the HIV tests altogether at test choice.
Frequently, the test counselor may experience stress on their own behalf, knowing they may need to deliver a positive test result within a few minutes of specimen collection. 45 Like the patients, HIV test counselors no longer have from one to two weeks to prepare for the delivery of an HIV-positive test result. Hood et al. 46 noted that test counselors providing POC testing in drug treatment facilities were fearful that clients told of HIV-positive test results would become suicidal or act out in other ways. Staff training was necessary to counteract these perceptions. Offering POC testing for pregnant women using a combination test for syphilis, hepatitis B, and HIV in an international setting also required significant staff training to overcome fear of delivering positive test results. 10
There are some limitations to the current study that must be noted. The pretest stress question specifically asked about multiple tests. While the majority of POC tests were combination/bundled tests, some were single tests. This study did not separate out the stress from waiting for results from a single test versus the bundled tests. This is an area for future research, especially given that the technology is moving in the direction of offering bundled tests with one blood spot specimen. Testing stress perception may vary depending on the number and types of tests being conducted in a POC setting and the implications of positive test results.
This study also did not assess test counselor stress associated with delivery of multiple positive test results. All test counselors received extensive training on the meaning of the various negative and positive test results they were delivering, but it is possible that their stress levels for providing multiple positive test results to clients could have influenced the stress levels of participants. Further research is needed to identify how counselor stress can be reduced in POC settings. Finally, this study took place in a large urban city in Southern California. Results may not be generalizable to non-U.S. settings or low-resource environments where much of the rapid POC testing occurs.
In conclusion, this study reported on the stressful testing experience for clients in a study of multiple POC tests for HIV, syphilis, and HCV.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.