
Abstract
Immediate antiretroviral therapy (ART) for acute HIV infection (AHI) may decrease HIV transmission in high-risk populations. This study evaluated knowledge of AHI and AHI testing program preferences in Lima, Peru through four semi-structured focus groups with high-risk men who have sex with men (MSM) (n = 20) and transgender women (TW) (n = 16). Using content analysis, emergent themes included knowledge of AHI symptoms, AHI transmission potential, and the HIV testing window period, and preferences concerning point of care results. Participants demonstrated low familiarity with the term AHI, but many correctly identified AHI symptoms. However, these symptoms may not motivate testing because they overlap with common viral illnesses and AIDS. Some were aware that infectiousness is highest during AHI, and believe this knowledge would facilitate HIV testing. The shortened window period with AHI testing would encourage testing following high-risk sex. Delayed result notification would not decrease AHI testing demand among MSM, although it might for some TW.
Introduction
Detecting acute HIV infection (AHI) is crucial because viral load is highest during this period,1–3 driving onward transmission. 4 AHI diagnosis and rapid treatment initiation could be especially important in concentrated epidemics, such as in Peru. A modeling study estimated that AHI accounts for 22–29% of onward transmission in Peru, where key populations, including men who have sex with men (MSM) and transgender women (TW), are at significant risk for HIV. 5 AHI testing programs could reduce transmission by facilitating early treatment with antiretroviral therapy (ART),1,6–9 subsequently suppressing viral load10,11 and decreasing high-risk sex.12,13 However, detecting AHI requires use of non-routine tests: nucleic acid amplification testing (NAAT), which detects HIV RNA, and fourth generation immune enzymatic testing, which detects p24 antigen in addition to HIV antibodies. These methods are more expensive than third generation tests but shorten the window period of HIV detection from four weeks to two weeks or less.14–19 It is not clear if populations would be receptive to using these tests after high-risk sex or when experiencing AHI symptoms.
Little available research, mostly from high-income settings, suggests that there is inadequate knowledge about the symptoms and high transmission potential of AHI.8,12,20–22 Knowledge of symptoms is crucial because they could motivate AHI testing following high-risk sex. One of the largest studies about AHI found confusion surrounding the various HIV testing window periods. 21 Lastly, detecting AHI requires delaying result notification by a few days because these expensive assays require pooling samples and de-convoluting the positive pools to reduce costs. 15 It is not known how key populations would perceive this delay and the need to return to receive their results.
While the prevalence of HIV in Peru is <1% nationally, 23 it is above 10% among MSM5,23–26 and up to 30% among TW. 27 Significant research and international funding have targeted these populations.28,29 Nevertheless, inadequate testing and diagnosis remain the largest deficits in the HIV cascade of care. 23 Nearly half of Peruvian MSM in one sample had never been tested for HIV. 30 It is estimated that one-third of transmission occurs among the undiagnosed 5 and 24% of people living with HIV are aware of their serostatus. 23 In a recent study from Lima, the second most important facilitator to HIV testing was lack of condom use, 31 indicating that there is demand for risk-based AHI testing.
To assess this demand and create recommendations for AHI testing programs, we investigated knowledge and attitudes regarding AHI symptoms, AHI transmission potential, testing window periods, and delayed result notification among MSM and TW in Lima. We included TW because they are the most at-risk population in Peru and often worldwide.32,33
Methods
Study team
This research was conducted through a partnership between the Fred Hutchinson Cancer Research Center (FHCRC, Seattle, WA, USA) and two Peruvian non-governmental organizations (NGOs) in Lima: Epicentro and the Asociación Civil Impacta Salud y Educación (IMPACTA). Epicentro provides STD/HIV services, and promotes scientific development and community organization for addressing these issues. IMPACTA researches health and human behavior, especially concerning HIV and the MSM/TW population.
The lead moderator is the founder of Epicentro and a seasoned researcher/advocate for MSM and TW living with HIV. He has facilitated multiple qualitative studies concerning the perspectives of MSM and TW. A senior qualitative researcher with expertise in healthcare utilization among LGBTQ and Spanish-speaking populations further oversaw data collection and analysis to ensure best practices. The assistant moderator and coders underwent intensive two-day training in qualitative methods prior to the study.
Procedures
Template of themes for discussion during focus groups.
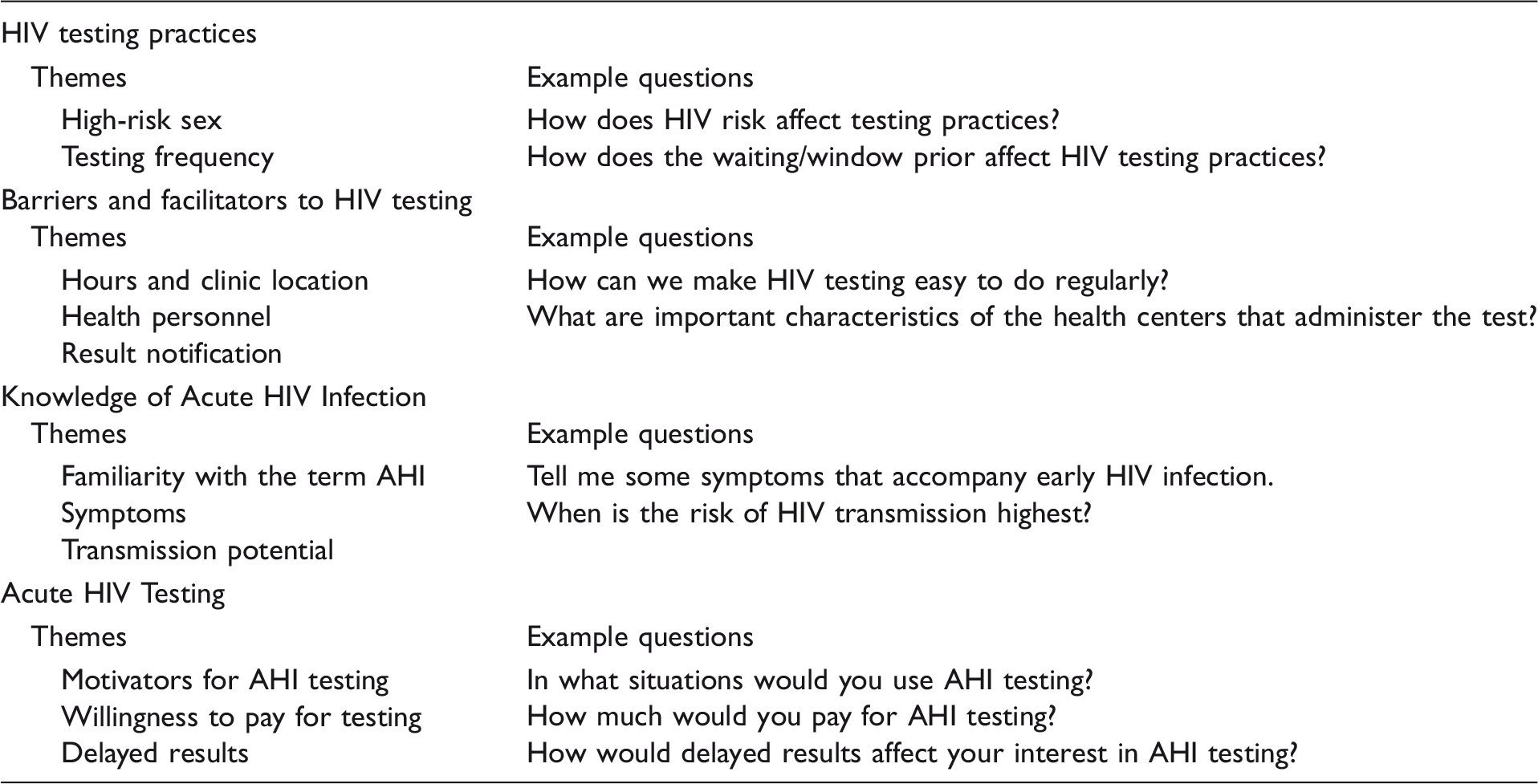
HIV: human immunodeficiency virus; AHI: acute HIV infection.
Study population demographics, risk factors, and sexual behavior.
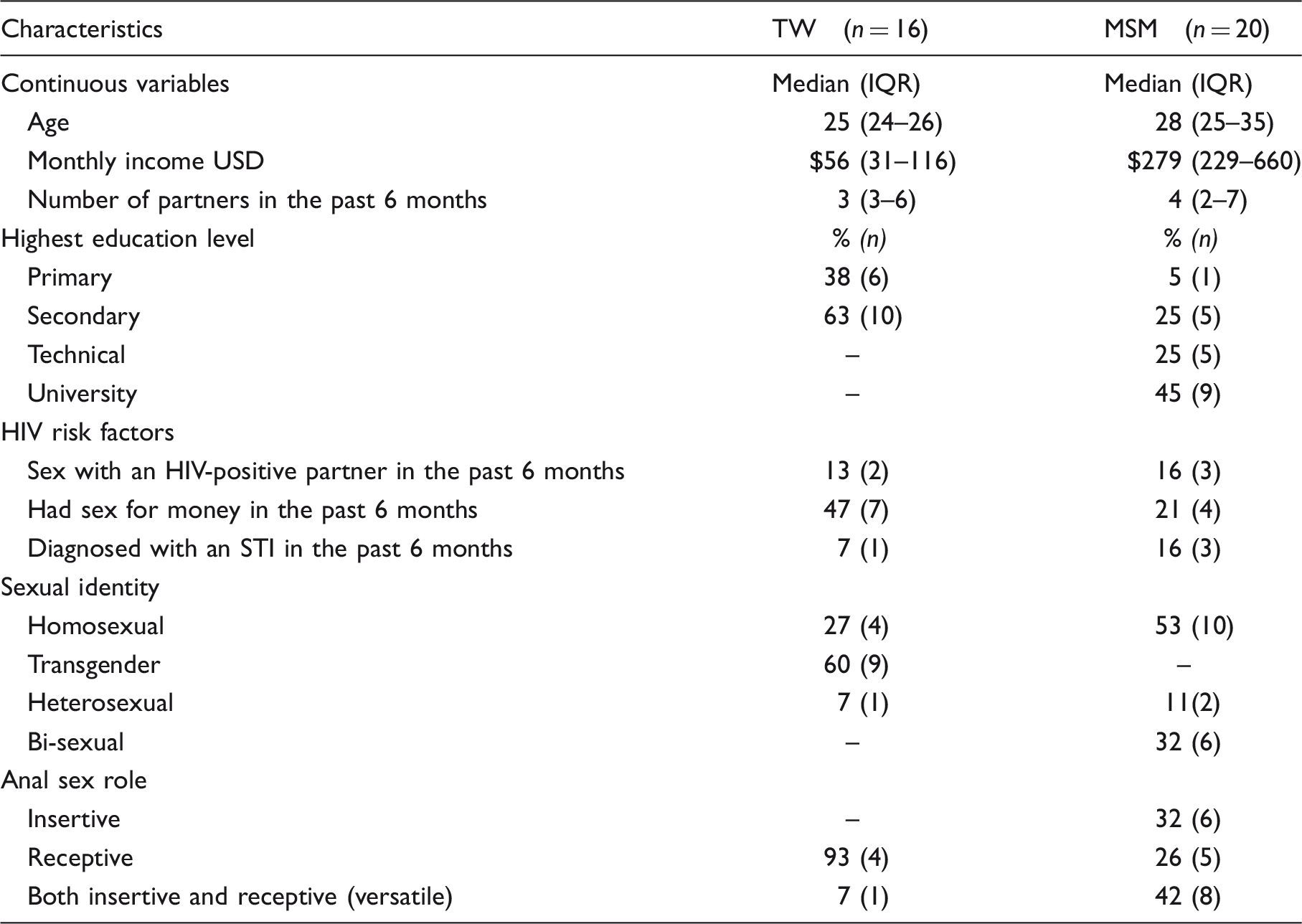
IQR: inter-quartile range; MSM: men who have sex with men; TW: transgender women; USD: United States Dollar; STI: sexually transmitted infection.
Three groups were convened at a gay-friendly bar in the Central District and one was held at Epicentro. Focus groups were conducted separately among specific populations, meaning no MSM participated in the focus groups attended by TW and vice versa. Each focus group included written and oral informed consent, a brief survey about demographics and sexual behavior, and an explanation of the study’s purpose, including an introduction to AHI testing. The lead moderator used a semi-structured guide to explore themes surrounding HIV testing in general and AHI testing specifically (Table 2). The assistant moderator took notes. The focus groups lasted for less than 2 h. The institutional review boards at IMPACTA and at FHCRC approved these procedures.
Qualitative analysis
Interviews were transcribed in Spanish, checked for accuracy, and uploaded into ATLAS.Ti version 7 (Berlin, Germany). Analysis was conducted in Spanish by three Spanish-speaking authors. The team used a combined deductive and inductive approach to content analysis, wherein themes from previous literature concerning HIV testing were explored and new themes were identified from raw data.
34
During analysis, the team met regularly to review codes and maintain inter-rater reliability. The coders discussed preliminary findings with the larger study team and community partners, who provided feedback on data analysis and interpretation. A summary of this process is provided in Figure 1.
Coding and analysis flow chart.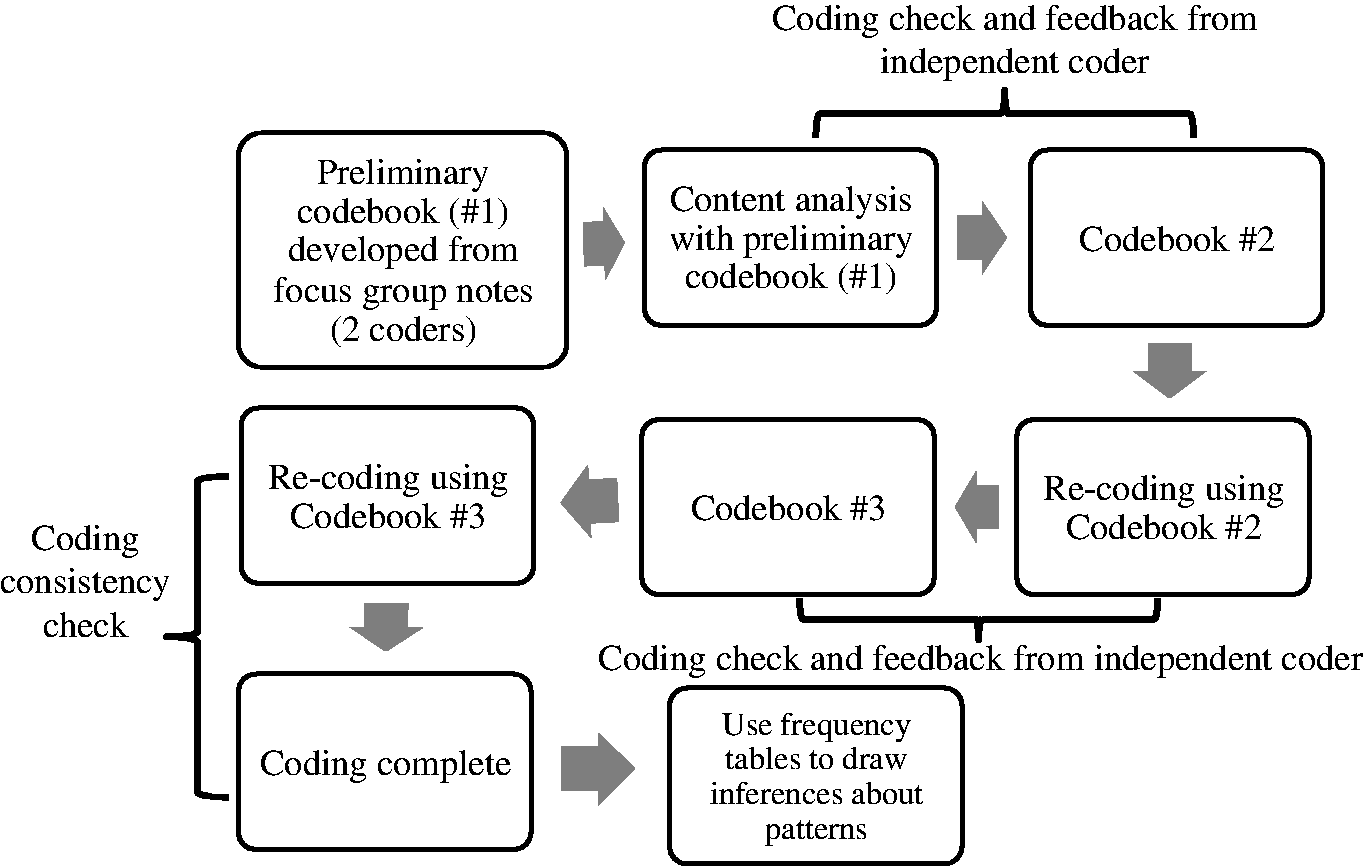
Results
Emergent themes were grouped as follows: (1) knowledge about AHI symptoms; (2) knowledge about AHI transmission potential; (3) knowledge about differences in the testing window period of tests; and (4) preferences concerning the importance of point-of-care (POC) results.
Knowledge about AHI symptoms: ‘Those [symptoms] are precisely what make me take the test …’
Despite unfamiliarity with the formal term ‘acute HIV infection,’ participants were familiar with the concept and identified many symptoms of early HIV infection, including fever, fatigue, flu symptoms, nausea/vomiting, diarrhea, headache, stomach ache, sore throat, chills, and lymphadenopathy. They associated AHI with the flu, as one MSM illustrated, ‘I have read that this stage gives you an acute flu, and it has symptoms like chills and fever.’ One TW summarized: ‘[It causes] aches that do not allow you to get up.’
Participants thought AHI symptoms would motivate AHI testing. While discussing symptom awareness, one MSM interjected, ‘Those [symptoms] are precisely what make me take the test … whenever I have a sore throat, get the flu, or a high fever ….’ Another MSM indicated that symptoms already prompt testing, ‘[When you have] a fever, or something else that could be AIDS, and you already [begin] to get scared … this is how you get motivated to go to the health center.’ A TW answered similarly, ‘When [people] have a fever or something, or a recent sickness, they say they’re going to get tested.’
Respondents emphasized that AHI symptoms and the term ‘acute HIV infection’ itself are confused with later stages of HIV. A TW explained, ‘Generally when people have these discomforts they think they have AIDS, but not an acute infection.’ Similarly, an MSM described AHI and its symptoms as ‘when you are in the terminal stage.’ This misunderstanding could be a potential barrier to both AHI and regular HIV testing because it appears to reflect a prevalent misunderstanding among these communities, wherein HIV is commonly equated with death. As one MSM explained, ‘They think that [HIV] is equal to AIDS. They don’t know about the treatments, that there is a time when the virus develops … there is already this stigma that the person who has HIV … is dead.’
The non-specific quality of AHI symptoms could dissuade testing. A TW participant highlighted this concern: ‘… If we put [these symptoms] together … well, [AHI] could be like the common cold.’ An MSM participant reported that this might prevent testing, saying, ‘Obviously anything can cause a fever. Just by getting a fever, a discomfort, a body ache, you do not want to have to go and get tested.’
Knowledge about AHI transmission potential: ‘That’s when the disease starts, when it peaks’
Many participants were unaware of the high transmission potential during AHI. One participant demonstrated this when asked to describe when infectiousness is highest: ‘[I have] an idea more or less, [it is] when you are in the terminal stage.’ However, other MSM reported some knowledge about it: ‘It’s the beginning stage, but when it’s more likely to spread [to others], like the virus is expanding throughout your body.’ A TW thought it is easier to transmit the virus during AHI ‘because the virus is beginning to gain strength.’ Transmission risk emerged as a facilitator for behavior change following diagnosis: Moderator: … What were saying about how you can take this test earlier? TW Participant: Yes, you’re not waiting 3 months or 6 months, because some people wait too long and then they don’t go, but if it is within one week then one would go … it’s good, because people who take the rapid test will be alerted … if you’re sick, you’re going to be … they are going to have to be careful.
Knowledge about differences in testing window periods: ‘We go to the doctor after we wait three months’
Participants were aware of the false-negative window period of HIV antibody tests. They said they would not seek testing after high-risk sex because of the window period, which they estimated to be three months. As exemplified by this MSM: ‘The three-month wait has an effect … let’s say I had high-risk sex yesterday … if I wanted to take the test … four months may pass … and I never go to take [the test].’
Participants were enthusiastic about the shortened window period of AHI testing. One MSM suggested using AHI testing after condom failures: ‘Possibly [you would get tested] after a night of heavy drinking, the condom comes off or you have sex without a condom.’ The TW participants were similarly frustrated with the window period and excited about AHI testing. A TW respondent noted: When you [get tested after] three months, and you have [had unprotected sex] in the past two weeks, then you need to wait three months for your test. But I would like to go the morning after my [sexual] relations.
Preferences on the timing of result delivery: ‘It’s a test that you do today and after two days you can pick it up’
Although AHI testing shortens the false-negative window period, the tests are not yet POC and samples must be pooled, tested, de-convoluted, and confirmed, which delay result notification by two days or more. During the focus groups, each participant was asked to choose between AHI testing with delayed results versus POC testing with a longer window period. MSM unanimously preferred AHI testing, as one summarized, ‘If you can wait a month for your results, you can wait two days.’
Conversely, many TW preferred AHI testing, as one TW exclaimed, ‘I think that the travestis are going to love this program … [Because although] you have to wait two days, it will tell you the truth.’ However, others insisted on POC delivery: ‘I want to know the same time, the same day after one or two hours … But if they say you need to wait two or three days, I would lose interest.’ This need for POC results was described in the context of work schedules and fear. One TW reported, ‘As we [sex workers] work at night, we get up later in the morning. Tiredness prevents you from doing many things.’
Discussion
Although opinions vary about the proportion of new infections attributable to AHI, it is likely that it plays an important role, especially in concentrated epidemics, such as in Peru. 35 There is a need to investigate how to implement successful AHI testing programs in Peru’s public health system, which provides most of the country’s HIV/AIDS care. 26 A recent pilot testing program implementing NAAT in Lima increased HIV case identification by 8.0% among MSM and 5.3% overall. 36 While introducing these programs could detect additional infections, identifying needs and preferences of the target population is critical to develop health promotion programs that increase uptake of the services (e.g. education about AHI symptoms; stigma reduction around testing).
Our participants were aware of some AHI symptoms and thought others would seek healthcare for a flu-like illness. In a previous study in Lima, people who had been tested for HIV were more likely to engage in HIV risk behaviors such as transactional sex, problem drinking, and sex with greater numbers of partners, compared to those who had never been tested. 31 Thus the Ministry of Health (MoH) guidelines for regular testing, every three to six months, 37 may be creating a false sense of security and contributing to onward transmission. 31
The participants highlighted the potential to confuse AHI symptoms with AIDS. This could impede AHI testing in Lima, where a ‘fear of a positive result’ 30 and viewing HIV as a ‘death sentence’ 38 are barriers to testing. Although AIDS-related deaths are decreasing in Peru, 29 these fears may not be unfounded because the national provision of ART has been imperfect.26,29 Understanding the factors impeding HIV testing is crucial because nearly 70% of participants with HIV in Lima were unaware of their positive serostatus. 39 This is often attributed to high testing-related stigma. 23 Education about AHI and the provision of AHI testing could ultimately reduce fear and stigma about HIV/AIDS, if early infection was marketed as an opportune time to initiate treatment, especially considering the high infectious potential. Like US studies, our participants were uninformed about the high transmission potential during AHI.20–22 Such understanding is critical because some MSM would change their behavior following AHI diagnosis to prevent onward HIV transmission in other studies, 13 and our participants predicted that others would as well.
Similar to American college MSM, 22 our participants were aware that conventional antibody-based tests miss early infections, although many overestimated the window period to be three months, when it is closer to 21–28 days with the third generation immunoassays commonly used in Peru. 17 It is not clear if this gap in knowledge is due to inadequacies in HIV counseling or the lack of uptake of educational material in Peru, and this issue deserves further exploration. For example, a recent campaign, ‘Hazte la prueba,’ does not clarify between the limitations of the window periods of rapid and ELISA testing methods. 40 The most recent counseling guidelines from the MoH from 2009 do recognize the window period and the importance of explaining it and the different stages of HIV to patients. However, they do not outline the duration of the window periods or provide detailed information on AHI infectiousness. They generally recommend patients to return for repeat testing after three months if they suspect they were tested during a window period. 41
MSM preferred AHI testing with delayed results to POC testing with a longer window period, while many TW preferred POC tests due to sex-worker schedules and fear/stigma. Similarly, in Guatemala City, TW were more interested in attending a health clinic that catered to the difficult schedule inherent of sex work. 42 HIV testing programs should accommodate the burdens of this population because sex work is the main economic activity of TW in Lima, 32 and therefore likely an important driver of the epidemic. The development of cheaper (∼$15) POC NAAT could address their concerns. 43
Our findings are limited by the fact that the facilitators did not educate the participants about the duration of the window period of third generation HIV tests, because of time constraints and the fact that they could have been using rapid testing, which often has a longer window period. Therefore, participants could have compared AHI testing with a perceived window period that is longer than it is in reality. As some participants were recruited through Epicentro community events, the study may disproportionately reflect the opinions of individuals obtaining care through NGOs.
Conclusions
We report demand for AHI testing among high-risk MSM and TW, and have identified that these populations may use symptoms and high-risk sex as facilitators to AHI testing. Our findings that the symptoms of AHI may be confused with those of AIDS implies that AHI testing programs should clarify the differences between different stages of HIV, avoid fear-inducing/stigmatized messages, emphasize that early diagnosis is not a death sentence due to ART, and connect the high transmission potential of AHI with concerns for infecting others. Such approaches will both enhance the success of AHI testing programs and increase linkage to care for initiation of ART following diagnosis. Although AHI testing could reduce transmission, neither AHI testing nor less-sensitive testing methods (e.g. ELISA, rapid-testing) can be implemented successfully without improved education about the HIV testing modalities and window periods among providers and laypeople, especially in Peru. We also found that TW may not prefer AHI testing due to their preference for POC results. As TW are most afflicted by HIV in Peru, further research is needed to design programs to address their needs, whether by working around their schedules or directly seeking them out for result delivery. Our study highlights the importance of educational programs targeting providers and populations, suggesting the need for further improvement of educational resources for AHI and general HIV testing.
Footnotes
Acknowledgements
We would like to acknowledge the research staff at IMPACTA and Epicentro, Yesika Magallanes RN, and Cinthia Surhaces, who made this research possible. We would like to thank Dr James Dobbins for his efforts reviewing and editing this manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was received from the National Institutes on Drug Abuse (NIDA) under grant number R01 DA032106. YM received support under grant numbers K01CA193918.
Supplementary data
For those who are interested in accessing these data, please email Dr Ann Duerr at aduerr@fredhutch.org to obtain research proposal instructions and transcripts.