
Abstract
In Haiti, routine screening for Chlamydia trachomatis (CT), Neisseria gonorrhoeae (NG), and Trichomonas vaginalis (TV) among pregnant women is not conducted; yet these sexually transmitted infections (STIs) are associated with adverse birth and newborn health outcomes. We aimed to assess the acceptability and feasibility of screening and the prevalence of STIs among pregnant women in Port-au-Prince, Haiti. Pregnant women of at least 18 years of age who attend Haitian Study Group for Kaposi’s sarcoma and Opportunistic Infections (GHESKIO) clinics in Port-au-Prince, Haiti provided self-collected vaginal swab specimens. Laboratory testing was done with Xpert® CT/NG and Xpert® TV. The results of this study showed that of the 322 pregnant women who visited GHESKIO for their regular scheduled appointments, 300 (93.2%) consented for CT, NG, and TV testing. Of those, 107 women (35.7%) tested positive for at least one STI. There were 42 (14.7%) cases of CT, 8 (2.8%) NG, and 83 (29.0%) TV infections. Most infections were treated – 122 of 133 (91.7%). In summary, we found that it was highly acceptable and feasible to implement CT, NG, and TV screening among pregnant women in Port-au-Prince, Haiti. We found high prevalence of STIs among pregnant women, which suggest that STI screening in this population may be warranted.
Introduction
Sexually transmitted infections (STIs) cause a significant global health burden, and cervico-vaginal infections are related to many adverse health outcomes. Although curable, sexually transmitted Trichomonas vaginalis (TV), Chlamydia trachomatis (CT), and Neisseria gonorrhoeae (NG) were responsible for over 350 million new infections worldwide in 2012. 1 A medical history alone is insufficient for the accurate diagnosis of genitourinary tract infections. 2 Many STIs can be asymptomatic and can only be diagnosed with screening tests. 3 Therefore, although the current World Health Organization guidelines recommend syndromic management for STI diagnosis in low- and middle-income countries, 4 syndromic management is unlikely to enhance STI control. 2 The early identification and subsequent treatment of STIs and other genital infections among index patients and their partners are paramount to achieving an effective reduction in the disease burden.
The immunologic response triggered by lower genital tract infections with CT and NG leads to significant inflammation of the cervico-endometrial tissue. 5 Due to infection and the associated chronic inflammatory response, several important sequelae may result from those infections, including pelvic inflammatory disease, ectopic pregnancy, and infertility. 6 TV infection has been associated with a more than 2.7-fold increase in the risk of HIV acquisition,7,8 a 1.3-fold increase in preterm labor and a 4.7-fold increase in pelvic inflammatory disease. 9 STIs such as CT, NG and TV during pregnancy may be associated with increased rates of adverse pregnancy outcomes including neonatal and infant death, preterm birth, low birth weight, and spontaneous abortion.9–12
Although routine screening and treatment for CT, NG and TV infections for pregnant women is done in several high-income countries like the United States, screening is not routinely done in many settings around the world, including Haiti.13–16 Although few recent studies have documented the prevalence of CT, NG, and TV infections in Haiti, two reports estimated that 40% of women in rural areas who were receiving antenatal care and 47% of women in urban areas who were receiving antenatal care had at least one STI.17,18
In Haiti, certain adverse birth outcomes remain high, including neonatal mortality, which was estimated at 25/1000 live births in 2012, and preterm birth was estimated at 14.1/100 live births in 2010.19,20 Improvements in STI diagnosis and treatment may play a role in reducing the high rates of those adverse pregnancy outcomes. The objective of this study was to assess the acceptability and feasibility of the screening of genital CT, NG, and TV infections and to estimate the prevalence of these infections in routine antenatal care in Port-au-Prince, Haiti.
Methods
All pregnant women over the age of 18 years who visited the Haitian Study Group for Kaposi’s sarcoma and Opportunistic Infections (GHESKIO) antenatal clinic in Port-au-Prince, Haiti between 26 October 2015 and 14 January 2016 were offered screening for cervico-vaginal CT, NG, and TV infections. GHESKIO is a non-profit organization that works in partnership with the Haitian Government to provide integrated primary care services, including HIV counseling, AIDS care, antenatal care, and management of tuberculosis and STIs. Participants who gave informed consent provided self-collected vaginal swab specimens after verbal instructions provided by GHESKIO healthcare employees. Patients were not offered any incentives for screening. Acceptability was measured by the percentage of patients who consented for participation among those offered testing.
Testing was conducted by study personnel using the FDA-cleared Xpert® CT/NG and Xpert® TV assays (Cepheid, Sunnyvale, CA). The high sensitivity of nucleic acid amplification tests for CT, NG and TV 13 makes them suitable as screening tests particularly because non-invasive specimens like urine and self-collected vaginal swabs can be used. Nucleic acid amplification tests do not require viable organisms and provide convenient specimen processing, allowing use in diverse settings. Several studies have evaluated the utility and performance of self-collected specimens for CT and NG testing. 21 The Xpert® CT/NG and TV assays have test performance equal to other FDA-approved nucleic acid amplification tests in central clinical laboratories. Laboratory testing was done within 72 hours at the GHESKIO central laboratory.
The women returned to GHESKIO within seven days from specimen collection to receive their test results, and free treatment was provided to those who tested positive. Women who tested positive for CT, NG or TV were given 1 dose (1 g) of azithromycin, ceftriaxone 250 mg injection and 1 g of azithromycin, or 1 dose (2 g) of metronidazole, respectively. They were also counseled on how to prevent infection. Feasibility was measured by the percentage of infections that were treated. Women with positive tests were asked to return no earlier than three weeks after treatment for test-of-cure. Women were counseled to bring their partners or refer their partners with a patient referral card to GHESKIO for onsite treatment. Partner-delivered therapy was provided to some women for treatment of CT and TV infections.
Data were collected electronically in secure databases and were analyzed using SAS v9.4 (Cary, NC, USA). Ethical approval was provided by Weill Cornell Medical College, New York, General Institutional Review Board protocol number 15032016010. Ethical approval was also given by the GHESKIO Institutional Review Board.
Results
A total of 322 pregnant women presenting to GHESKIO were screened for participation over a four-month study period. Of the 322 pregnant women who visited GHESKIO for their regular scheduled appointments, 300 (93.2%) participated in the study and were tested for CT, NG and TV. Of those, 286 (95.3%) returned to receive their test results. There were 107 women (35.7%) who tested positive for at least one STI (Figure 1). There were 42 women (14.0%) who tested positive for CT. Of the women who tested positive for CT, 39 (92.9%) were treated. For NG, eight women (2.7%) tested positive, and six (75.0%) returned and received treatment. And lastly, for TV, 83 women (27.7%) tested positive. Of those 83 women, 77 (92.8%) received treatment. Of all of the participants, four were co-infected with all infections tested: NG, CT and TV. Additionally, of the women who tested positive initially, there were 13 partner referrals to GHESKIO who came for treatment.
Chlamydia trachomatis, Neisseria gonorrhoeae, and Trichomonas vaginalis prevalence and the proportion treated among pregnant women in antenatal care in Port-au-Prince, Haiti (N = 300).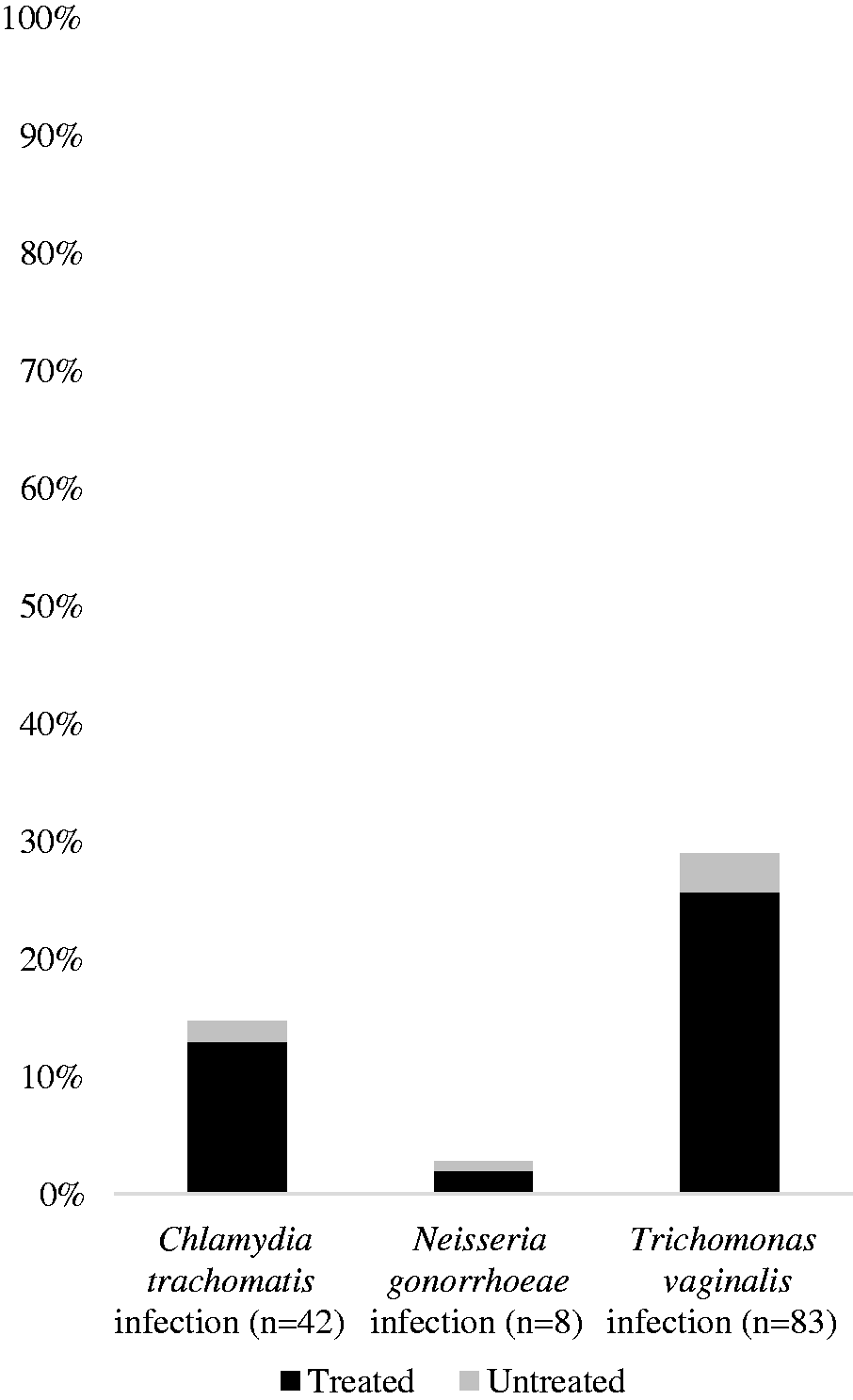
Among the 107 women who tested positive for at least one STI, 83 (77.6%) returned for a test-of-cure. Sixty-two TV-infected women returned for the test-of-cure, of whom 28 (45.2%) tested positive for TV. Five NG-infected women returned for test-of-cure, of whom one (20.0%) was positive. Thirty-two CT-infected women returned for test-of-cure, of whom three (9.4%) tested positive for CT. Those women were retreated.
Discussion
We provided screening for genital CT, NG, and TV infections for 300 pregnant women in routine antenatal care in Port-au-Prince, Haiti. We found that STI screening in antenatal care was acceptable with most, over 90%, of antenatal patients consenting to STI testing at their antenatal visit. Screening led to the identification of prevalent CT, NG and TV infections; and over a third of participants tested positive for at least one of the three STIs tested. We found high STI prevalence among this population with almost 15% testing positive for CT, an infection known to be associated with serious adverse outcomes in pregnancy.10,12 NG infections were identified in over 2% of participants. TV infection was the most prevalent STI identified in this study with over a quarter of participants testing positive. Infection with TV, a motile protozoan, is the most common, non-viral STI worldwide. 1 Of those infections identified, a very high proportion, over 90%, were treated making screening during antenatal care an effective way to both identify and treat STIs in pregnancy. Some participants with STIs did not return for treatment even after follow-up phone calls were made.
Test-of-cure visits were conducted approximately three weeks after treatment. Some participants continued to test positive even after following adequate treatment. Most striking is that almost half of those treated for TV had a positive TV test-of-cure result. Molecular tests detect nucleic acid from organisms whether they are alive or not. However, that means that treated individuals may continue to test positive using a molecular test after treatment beyond the period of infectivity. In addition, there is emerging evidence of metronidazole-resistant TV globally 22 and this could be another explanation for the high positive TV rates at the test-of-cure; however, we were unable to explore these possibilities in the present study. Further research is needed to determine the time to organism clearance to inform appropriate timing for test-of-cure; however, some evidence suggests that nucleic acid-based tests for NG infection will be negative at 7 to 14 days after treatment 23 and over 85% of women will be negative for TV and CT nucleic acid after 21 days of treatment. 24 We were unable to determine if the high positivity rate for TV at test of cure was due to the Xpert® TV assay detecting nucleic acid from dead TV organisms, treatment failure or reinfection.
Many nucleic acid amplification tests have been optimized for use with several specimen types including non-invasive specimens like urine and patient self-collected specimens (such as vaginal and rectal swabs). 21 An additional advantage of nucleic acid amplification tests is the advent of multiplex assays, such as the Xpert® CT/NG assay used in this study that simultaneously detected multiple targets to diagnose multiple pathogens. Those factors make the nucleic acid amplification tests ideal for a range of settings.
This study was not without limitations. Participants were those visiting GHESKIO centres, a non-governmental clinical setting in Port-au-Prince, Haiti and therefore may not be representative of participants in other settings. Additionally, the moderate sample size and short duration of this study did not provide sufficient power and observation time to look at the impact of testing on pregnancy outcomes or to provide highly precise estimates of prevalence. Despite those limitations, our intervention was able to identify the prevalent CT, NG and TV infections that would have likely gone untreated in the absence of testing.
Screening for STIs in pregnancy provides an opportunity to improve health outcomes of women and infants.10,12 This study is comparable to similar pilot studies in Botswana and Peru that have demonstrated the acceptability and feasibility of clinic-based screening for STIs among pregnant women.25,26
STI testing and treatment in antenatal care are acceptable, feasible and have led to the treatment of prevalent infections at GHESKIO centers in Port-au-Prince, Haiti. Further, the high prevalence of STIs found in our sample provides support for efforts to increase screening and treatment in order to reduce the disease burden of STIs and subsequent adverse health outcomes among pregnant women and infants.
Footnotes
Acknowledgements
The testing supplies were donated by Cepheid Inc. (Sunnyvale, CA).
Authors’ contributions
CCB provided oversight of the study, conducted the analysis, and wrote the manuscript. PM assisted with study implementation, data collection, data analysis. OO oversaw the study and laboratory-based processes. JWP, DB and JDK oversaw and conceived of the study. AW assisted with the data analysis and provided critical review. All co-authors provided review of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: CCB acknowledges funding from NIDA T32 DA023356 and NIDA R01 DA037773-01A1.