
Abstract
Male sex workers (MSWs) in Vietnam are at high risk for acquisition and transmission of human immunodeficiency virus (HIV) and other sexually transmitted infections (STIs), yet are extremely disengaged from the healthcare system. This contributes to large numbers of untreated or late-treated infections and increased secondary transmission. We enrolled 995 MSWs in Hanoi and Ho Chi Minh City (HCMC) in a Sexual Health Promotion intervention that included face-to-face delivery of seven content modules, a clinical examination and testing for HIV, syphilis, gonorrhea and Chlamydia. Onsite treatment was provided for STIs, and those who tested positive for HIV were referred to local treatment centers. While 64.6% of participants had never been to a health service and fewer than half (41.2%) had ever been tested for HIV, 67.1% returned for test results. This testing identified 109 (11.0%) participants who were HIV-positive and 312 (31.4%) who tested positive for at least one other STI. Substantive differences were seen in MSWs from different cities, with those from Hanoi more likely to have ever visited a health service (57.8% vs. 24.9%) and to have taken a prior HIV test (54.1% vs. 37.9%) than those in HCMC. Sexual health promotion is a promising approach to engaging MSWs in health services.
Introduction
HIV prevalence remains high in Vietnam, especially among vulnerable populations. While the national prevalence is 0.39%, 1 the rate among men who have sex with men (MSM) is as high as 16% in urban centers such as Hanoi and Ho Chi Minh City (HCMC). 1 Within the overall MSM population, male sex workers (MSWs) are at especially high risk for both the acquisition and transmission of HIV,2–5 and HIV prevalence among MSWs in Vietnam is estimated to be 19.8%. 1 Sexually transmitted infection (STI) rates are similarly high among MSM in Vietnam, and higher still among MSWs. Although most research in this area has focused on injection drug users 6 and female sex workers, 7 Pham and et al. 8 reported high STI rates (6.3%) among MSM in An Giang Province, including syphilis (1.3%), gonorrhea (1.8%) and Chlamydia (3.2%). Colby et al. 9 reported syphilis prevalence of 17.6% among transgender women in Ho Chi Minh City.
Research elsewhere in the world also shows high rates of HIV and STIs among MSWs. Studies show HIV prevalence among MSWs to be 3.7% in England, 10 4.5% in China, 11 5.6% in Israel 12 and 7.3% in Providence, Rhode Island. 13 Higher rates are seen in Peru (30.7%) 14 and in several African countries (as high as 50% in Cote d’Ivoire).15,16 Although STI data are not reported as frequently, prevalences higher than 10% have been reported for syphilis,11,14,17 gonorrhea10,16 and Chlamydia 10 in MSW populations.
It is noteworthy that a substantial proportion of the MSW population have concurrent female sex partners, potentially facilitating epidemiological bridging between high prevalence MSM and the general population.14,18 This may be important for MSWs who have not engaged clinical services, as this subgroup has been shown to have even higher rates of HIV and STIs. 16 Despite these risks, large numbers of MSWs remain untested for STIs and HIV, or test only infrequently or when they are symptomatic. 12
Accordingly, there is an acute need to develop targeted sexual risk reduction programmes for MSWs and to engage them in screening and care. Access to health services, including testing for HIV and other STIs, may identify these infections earlier and potentially decrease their spread into the general population. This paper presents data from a study that implemented a sexual health promotion (SHP) intervention for MSWs in Hanoi and HCMC, Vietnam. Specifically, we describe the prevalence of HIV, syphilis, gonorrhea and Chlamydia, rates of return for test results, and the history of testing and diagnoses for these infections among a large sample of out-of-treatment MSWs.
Methods
The study was implemented in both Hanoi and HCMC, Vietnam, from August 2014 through September 2016. The study design, including the SHP intervention, has been described in detail elsewhere. 19 Briefly, using targeted sampling methods 20 in public and semi-public venues in each city, we recruited MSWs for participation in a brief, venue-based, behavioral survey that included reported history of testing and diagnosis for HIV, syphilis, gonorrhea and Chlamydia. Eligibility was restricted to young men, aged 16–29 years old, who self-reported transactional sex with another man at least once in the past 90 days. A randomly-selected subset of MSWs who completed the survey was then recruited for participation in a targeted SHP intervention at our local research sites, which were located in health clinics in each city.
Following informed consent procedures, participants in the clinic-based intervention participated in the second behavioral survey interview, which included the following domains: demographics, substance use, mental health, sexual history, current sexual events (including male and female elective partners, as well as male commercial partners), and health status and utilization of health services.
After completing the interview, participants received the clinic-based SHP intervention, an individual-level intervention consisting of seven modules (Understanding Sexual Health, Sexual Diversity, STI/HIV Transmission, Behavioral Risk Reduction, Substance Use, Stigma Management Skills, and Health Seeking) delivered in a single session by a trained Health Educator. At the conclusion of the SHP intervention, participants received a clinical examination and STI/HIV testing conducted by a study physician who was also trained in the SHP intervention and used the clinical examination as an opportunity to amplify the educational content provided by the Health Educator. Nearly all participants (97.9%) who completed the intervention received testing for HIV, syphilis, gonorrhea and Chlamydia. HIV testing was by venipuncture, with screening by rapid test (Determine HIV 1/2 [Alere, Waltham, Massachusetts, USA] or Genscreen HIV-1/2 [Bio-Rad, Hercules, California, USA]) and confirmation by two additional tests at a public health laboratory following Vietnam Ministry of Health guidelines. Syphilis screening was by rapid plasma reagin (RPR CHARBON, BIOLABO, Maizy, France) with confirmation by Treponema pallidum hemagglutination assay at a reference laboratory. Screening for STIs included oral, anal and penile swabs tested for Chlamydia and gonorrhea using polymerase chain reaction-based commercial test kits (artus CT/NG [Qiagen, Hilden, Germany] or CT/NG [Viet A, Binh Duong, Vietnam]). An appointment to receive test results was scheduled approximately one week later. Treatment was provided onsite for all STIs (immediately for symptomatic STIs and upon receiving test results for STIs that did not display any visible symptoms/signs), and those who tested negative for hepatitis B virus (HBV) antibodies were offered HBV vaccination. Participants who tested positive for HIV were referred to public HIV treatment centers where free antiretroviral therapy was available.
Survey data were collected using iPads running FormHub software (Columbia University, New York, NY, USA), which allowed for immediate upload of completed surveys. Clinical data were entered into online forms using the same software and were stored in study clinics in HCMC. Receipt of surveys and other data were confirmed daily, and provided to U.S. investigators using only unique identification codes. Data were stored on password-protected computers and analyzed using SPSS (version 22, IBM Corporation, Armonk, NY, New York). Between-city differences were analyzed using independent sample t-tests for continuous variables and Chi square (χ2) analyses for categorical data.
Participants were paid the Vietnam equivalent of US$5 in compensation for their time completing the survey interview. However, participants were not paid for clinical testing nor for returning for their STI/HIV test results. Participants provided written informed consent for interviews and biological testing and could refuse to participate in any aspect of the study without penalty. All study procedures were reviewed and approved by Institutional Review Boards in both the U.S. and Vietnam, including a waiver of parental consent for those participants under 18 years of age.
Results
Demographics and sexual partners
A total of 995 MSWs participated in the study; 319 (32.1%) in Hanoi and 676 (67.9%) in HCMC. As required by study eligibility criteria, participants ranged in age from 16 to 29 years old, with a mean age of 22.4 years. Three-quarters (75.9%) were migrants, defined as having been born outside the city in which they were recruited. On average, participants had completed 10.5 years of school, and 17.3% were in school when they were recruited. Nearly half (48.8%) had completed high school, and 10.7% had completed college or university. Nearly all (91.6%) had never married. When asked to describe their gender self-identity, nearly half (49.1%) reported thinking of themselves as men, while 37.0% answered “other” (rather than man, woman, or transgender) and 9.7% were unsure. Fewer than half (45.8%) reported being exclusively attracted to men and 26.9% reported being exclusively attracted to women.
Participants were also asked about their sexual partners in the past 30 days. Nearly one-quarter (22.4%) reported having sex with a regular female partner and 6.4% reported paying a female sex worker for sex during this time; 27.9% of participants reported having sex with a male elective partner in the past 30 days. On average, participants reported engaging in 12.7 sex work events (range 1–150) with 10.6 different partners (range: 1–100) in the previous 30 days.
MSWs in Hanoi differed from those in HCMC on most variables tested. They were younger (22.0 vs. 22.5, t = 2.415, p=.016), more likely to be migrants (84.6% vs. 71.7%, χ2 = 19.69, p<.001) and had a higher level of education (11.03 years vs. 9.05 years, t = 4.91, p<.001). They were also more likely to think of themselves as a man (73.9% vs. 37.5%, χ2 = 171.39, p<.001) and less likely to be exclusively attracted to men (29.2% vs. 53.5%, χ2=60.15, p < 001). MSWs in Hanoi were more likely to have had sex with at least one regular female partner (31.9% vs. 18.1%, χ2 = 22.99, p<.001) and at least one female sex worker (11.7% vs. 4.3%, χ2 = 18.87, p<.001) in the last 30 days. There were no differences between cities in the average number of sex work events or sex work clients in the past 30 days. These data can be seen in Table 1.
Demographics and sexual partners.
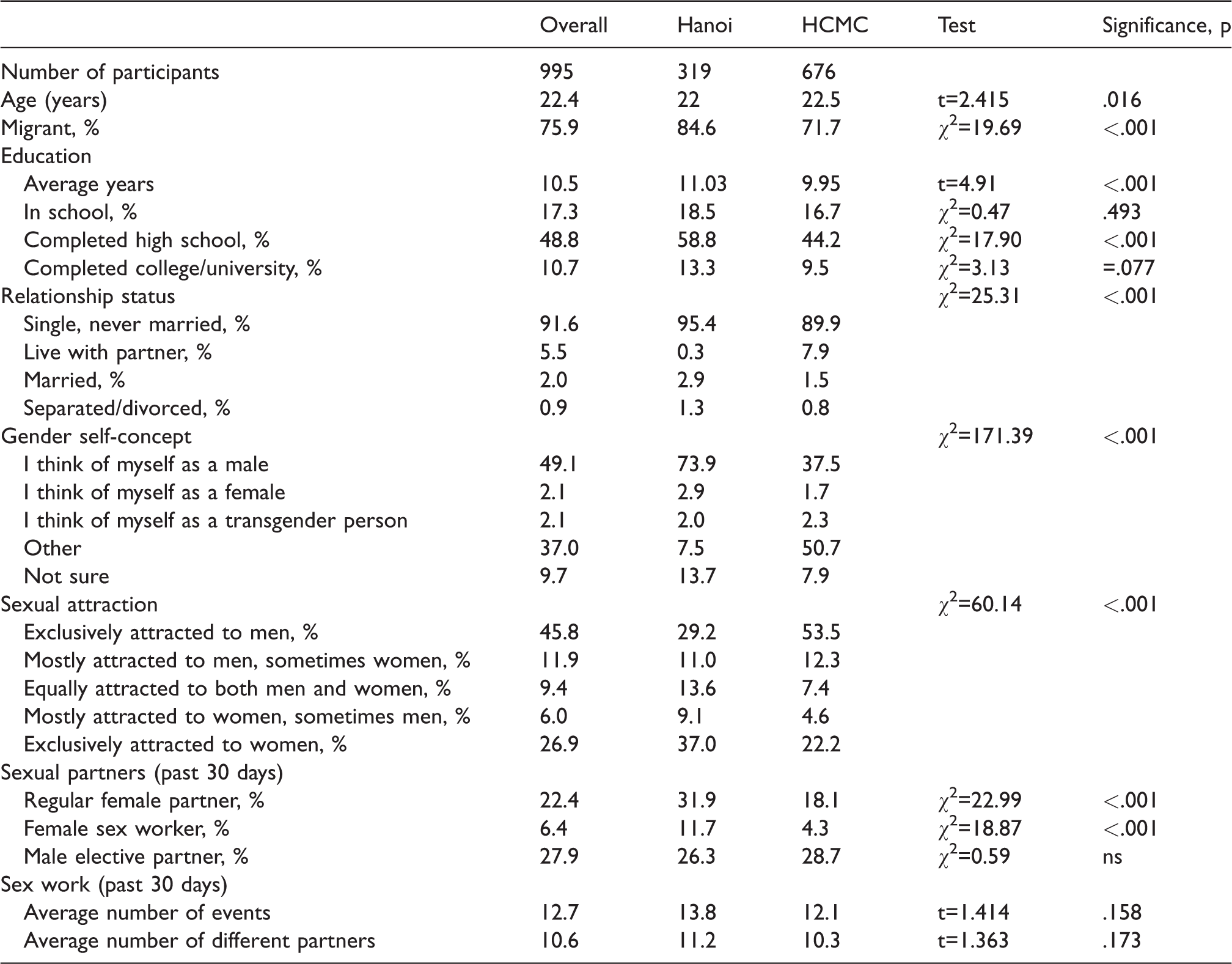
HCMC: Ho Chi Minh City.
Prior exposure to health services and HIV/STI testing
Participants reported limited experience with health services. Two-thirds (64.6%) had never been to a doctor or health service, and only 29.4% had visited a doctor or health service in the past six months. Less than half (41.2%) had ever been tested for HIV, and only six participants (0.6%) had ever tested HIV positive. More than three-quarters (88.2%) had not been tested for an STI in the past 12 months. Low rates of prior STI testing resulted in very low rates of reported lifetime STI diagnoses – 2.9% for syphilis, 2.2% for gonorrhea and 0.3% for Chlamydia.
MSWs in Hanoi were also more likely to have visited a health service, both ever (57.8% vs. 24.9%, χ2=99.43, p<.001) and in the past six months (39.0% vs. 24.8%, χ2=20.05, p<.001) and to have ever taken an HIV test (54.1% vs. 37.9%, χ2=22.40, p<.001) than MSWs in HCMC. The only between-city difference in HIV and STI test results was for syphilis, with higher rates in Hanoi (4.8%) than in HCMC (2.3%) (χ2=4.41, p=.036). These data can be seen in Table 2.
Health service and testing history.
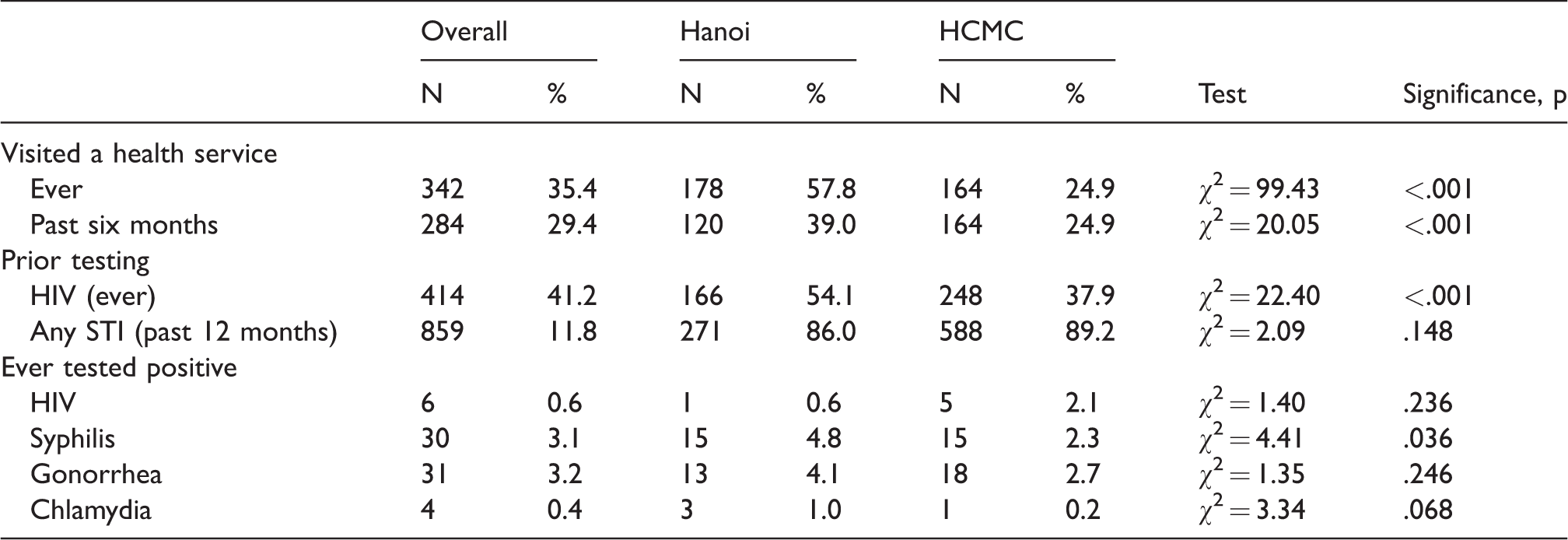
HCMC: Ho Chi Minh City.
HIV/STI status
Overall, 668 (67.1%) of participants returned for their test results. Return rates were higher in HCMC than in Hanoi (71.7% vs. 51.4%, χ2 = 20.31, p<.001). No association was found between returning for test results and having been previously tested for HIV or previously diagnosed with syphilis, gonorrhea or Chlamydia.
Prevalence of HIV and other STIs was relatively high, with 109 participants (11.0%) testing positive for HIV, and 312 (31.4%) testing positive for at least one other STI. For STIs, 166 (16.7%) participants tested positive for syphilis, 104 (10.5%) tested positive for gonorrhea, and 114 (11.5%) tested positive for Chlamydia. Those who had never been tested and/or diagnosed with these infections were of particular interest in this study, and relatively high rates of infection were found in these participants. Among those with no prior HIV testing (n = 548), 10.9% were HIV-positive; while among those who had previously tested negative (n = 431), 8.4% were HIV-positive. A total of 941 participants reported having never tested positive for syphilis in the past; among these participants, 152 (16.2%) tested positive for syphilis at their clinical assessment. For gonorrhea, among those who had never tested positive (n = 948), 10.0% (n = 95) were positive for gonorrhea. For Chlamydia, among those with no prior diagnosis (n = 966), 11.5% tested positive. Thus, intervention participants who had not previously been tested for HIV or diagnosed with an STI were found to have 100 cases of HIV, 152 cases of syphilis, 95 cases of gonorrhea, and 111 cases of Chlamydia that had not previously been diagnosed. These data can be seen in Table 3.
Current HIV/STI infections × prior testing/diagnosis.
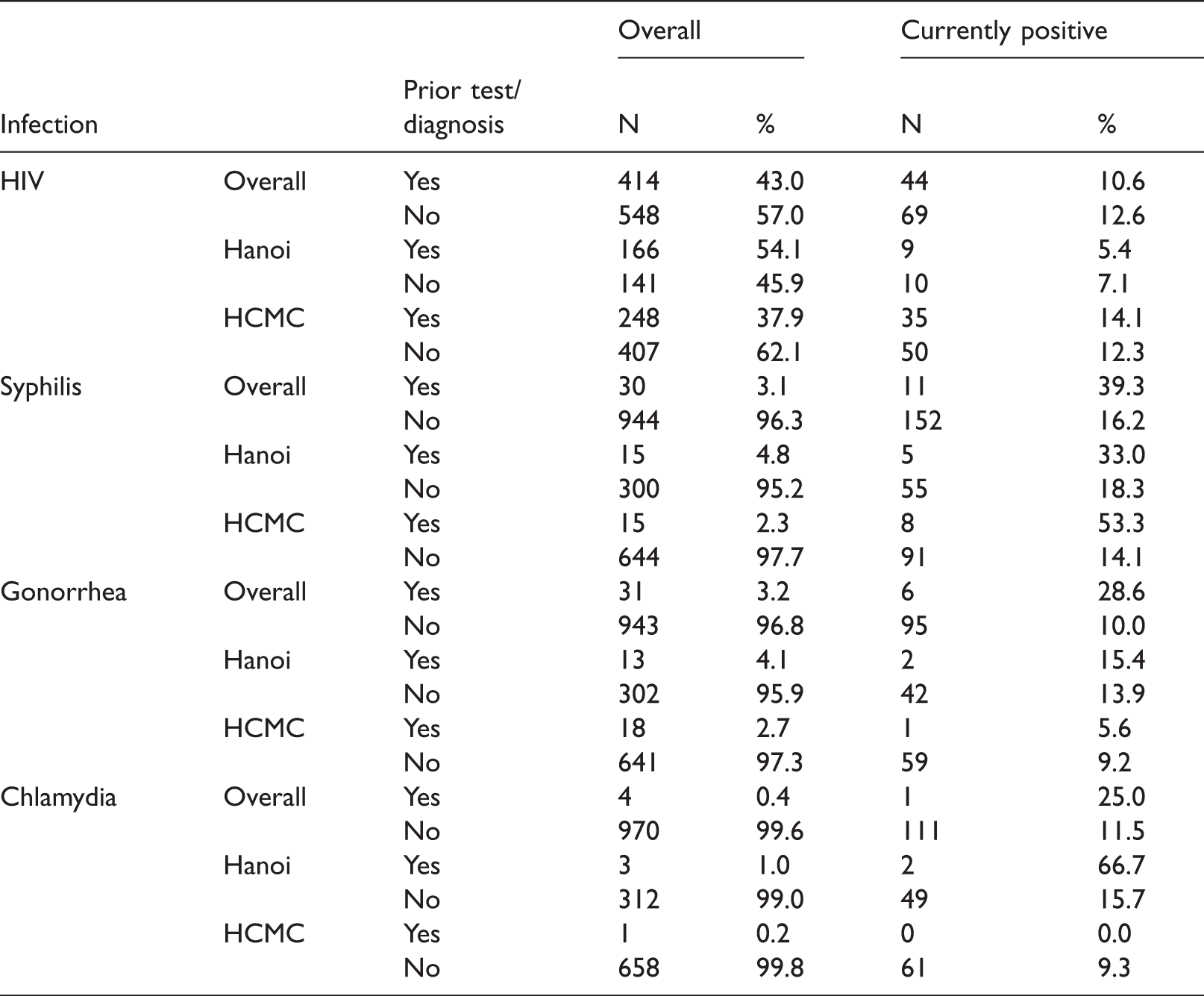
HCMC: Ho Chi Minh City.
Discussion
This study illustrated the benefits of engaging MSWs in testing and treatment for HIV and other STIs. Participation in the SHP intervention, which included both a clinical assessment and laboratory testing for HIV and other STIs, resulted in identification of a large number of infections, which were then either treated onsite (in the case of STIs) or referred to public clinics for treatment and monitoring (in the case of HIV). These infections were identified among participants who had very limited engagement in the healthcare system and profoundly low rates of prior testing.
In addition to the value of identifying and treating these infections in study participants, the intervention may have prevented additional infections, as untreated STIs can be transmitted to sex partners and facilitate additional infection with both STIs and HIV.21,22 MSWs in this study reported high rates of sexual concurrency and complex patterns of sexual partnering, including sex with elective male and female partners, potentially representing an epidemiological bridge between risk networks. While we do not have data on whether study participants changed their sexual practices, or received additional HIV and STI testing in the months following participation in the intervention, we do know that they gained awareness of STI symptoms, 23 a positive experience of sexual healthcare (which was a key aim of the intervention, and is illustrated by high post-intervention ratings 19 ) and successful treatment for their infections at the time of the intervention.
Substantial differences were seen between MSWs in the two cities. MSWs in Hanoi were in some ways more isolated, as they were younger and more likely to be migrants, suggesting limited social support. On the other hand, MSWs in Hanoi were also more likely to have visited a health service as well as more likely to have previously been tested for HIV, suggesting greater, albeit limited, access to sexual healthcare. These differences likely reflect the underlying differences in the MSW environment in each city. Hanoi is a smaller city, and the seat of the national government, and sex work venues tend to be fairly small. HCMC, on the other hand, is a much larger, sprawling city, with a large number of venues in which male sex work takes place. While these between-city differences were the reason we selected these two cities for the study, additional work is needed to determine the specific impacts these environments have on sexual practices, disease transmission, and engagement with health services. Nevertheless, the SHP intervention was effective at engaging MSWs in both cities.
There were a number of limitations that should be considered when interpreting these findings. First, as with most studies of MSWs, it is impossible to determine whether study participants were representative of MSWs in Hanoi or HCMC, or Vietnam as a whole, and therefore generalizability of these findings cannot be assumed. Second, data on prior HIV and STI testing and diagnoses were obtained via self-report, and therefore cannot be verified. Unfortunately, for a population that is not engaged in healthcare, and that only accesses treatment services when symptoms are prominent and interfere with their ability to have sex, verification of this information is not possible. Finally, although the intervention had a strong impact at the time of participation, the study procedures did not include ongoing follow-up of participants, and therefore we cannot determine whether the intervention resulted in improved subsequent access to sexual healthcare. While some study participants did return to the study clinics for further testing after completing the intervention, suggesting that healthcare engagement persisted for at least some participants, this information was not collected systematically from all participants, and thus it is difficult to draw conclusions regarding ongoing healthcare engagement. Finally, slightly more than one-third of participants did not return for their test results, and our return rates were especially low in Hanoi. We noted low return rates at the start of the project and introduced longer clinic hours and greater outreach contact with participants, which resulted in improved return rates of nearly 70% during the final months of the project.
SHP is a promising approach to improve engagement with health services for those most vulnerable to acquiring and transmitting HIV and other STIs. Our intervention identified a substantial number of previously unidentified infections in MSWs, a population with low rates of prior testing for HIV, syphilis, gonorrhea and Chlamydia. Expanding the use of health promotion in general – and SHP in particular – to include MSM, female sex workers and injection drug users has great potential to reduce the spread of HIV and STIs in Vietnam, ultimately slowing the HIV epidemic and likely leading to additional benefits deriving from increased access to health services.
Conclusions
MSWs in Vietnam are at heightened risk for the acquisition and transmission of HIV and other STIs. They are also profoundly disengaged from the healthcare system, resulting in higher rates of untreated infection and delayed treatment. An SHP intervention was effective at engaging MSWs in Hanoi and HCMC in testing, treatment and referral for HIV, syphilis, gonorrhea and Chlamydia.
Footnotes
Acknowledgments
We wish to thank the young men who generously participated in this study, as well as the Health Educators, Research Interviewers, and Study Physicians in each city. Data are available via request to the lead author.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research reported in this paper was supported by a grant from the U.S. National Institute on Drug Abuse (NIDA, R01DA033673, L. Goldsamt, PI).