
Abstract
Cerebrospinal fluid (CSF) escape phenomenon is widely studied and documented in HIV-1. However, hardly anything is known about progressive neurologic disease in otherwise well-controlled HIV-2 infection. We present a case of neurosymptomatic CSF escape in HIV-2 infection from India.
Introduction
Neurosymptomatic cerebrospinal fluid (CSF) escape is a condition where neurological signs and symptoms along with dissociation between CSF and plasma human immunodeficiency virus (HIV) concentrations are seen in patients on antiretroviral therapy (ART). 1 Almost all the reported cases of CSF escape1,2 are in patients infected with HIV-1.
Globally almost 90% of HIV cases comprise of HIV-1. Isolated or dual infections with HIV-2 remain restricted to certain regions such as Western Africa and India. 3 HIV encephalitis has been documented in HIV-2 cases not on ART or failing on ART.4,5 However, hardly anything is known about progressive neurologic disease in otherwise well-controlled HIV-2 infection.
We present a case of neurosymptomatic CSF escape in HIV-2 infection from India.
Case details
In September 2013, a 71-year-old married woman presented with complaints of weakness and multiple aphthous ulcers. She gave a history of recurrent diarrhea for a couple of years. She was diagnosed with HIV-2 infection. She originated from a district in Western Maharashtra, India. Her husband was seronegative for HIV-1 or-2. She had a history of blood transfusion in 1988. There was no past history of any opportunistic infections or any other comorbidity such as diabetes mellitus, hypertension, or hypo/hyperthyroidism. The nadir CD4 cell count at the start of ART was 488 cells/mm3 and CD4% was 26%. Hepatitis B and Venereal Disease Research Laboratory tests were negative; chest radiograph and ultrasonography of the abdomen revealed no pathology. The initial treatment regimen was a combination of two nucleoside reverse transcriptase inhibitors (NRTIs) and a boosted protease inhibitor (PI) – zidovudine + lamivudine + lopinavir/ritonavir. Table 1 summarizes the subsequent CD4 cell count after initiation of ART. At that time, HIV-2 viral load testing was not available in India.
Follow-up immune-virological investigations in an HIV-2-infected patient, from initiation of first-line ART until diagnosis of CSF escape.

CSF: cerebrospinal fluid.
In March 2016, she complained of delusions and hallucinations for which she was initiated on haloperidol. She was also prescribed simvastatin. Magnetic resonance imaging (MRI) of the brain at that time showed cerebral atrophy appropriate for her age. She improved with the treatment. In April 2017, she was hospitalized for complaints of giddiness, loss of balance, disorientation, tremulousness, and fear of the unknown. MRI brain showed scattered foci of hyperintensities in the bilateral periventricular white matter, centrum semiovale, and corona radiata on T2WI and FLAIR images, dilated ventricular systems, widened cerebral cortical sulci, and basal cisterns suggestive of cerebral atrophy (Figure 1). Suspecting CSF escape phenomenon in this case, we obtained CSF for examination, which showed marginally elevated proteins (65 mg/dl), normal glucose level (77 mg/dl), 400 red blood cells, and total nucleated cell count of 10, all lymphocytes. Simultaneous plasma glucose was 119 mg/dl. No organisms were seen on Gram stain and Ziehl–Neelsen stain. India ink test was negative for cryptococcal infection. Plasma viral load by real time polymerase chain reaction assay for HIV-2 (in-house test), which by this time had become available in India, was found to be below 100 copies/ml (the cutoff value for the test). Viral load in CSF was found to be 1995 copies/ml. This confirmed our suspicion of CSF escape. Due to unavailability of genotypic drug resistance testing for HIV-2, the treatment was changed empirically. Anticipating resistance to the NRTI backbone and lopinavir, the second-line regimen was constructed using an integrase inhibitor combined with a PI with a higher genetic barrier. In April 2017, her ART was switched to dolutegravir (50 mg) once a day and darunavir/ritonavir (600 mg/100 mg) twice a day. After initiating the new regimen, the patient felt better within a week and her symptoms of giddiness, loss of balance, disorientation, tremulousness, and fear of the unknown rapidly disappeared. During a follow-up visit in May 2017, she reported that her symptoms had completely subsided. The CD4 and VL after switch to second-line ART have yet not been done.
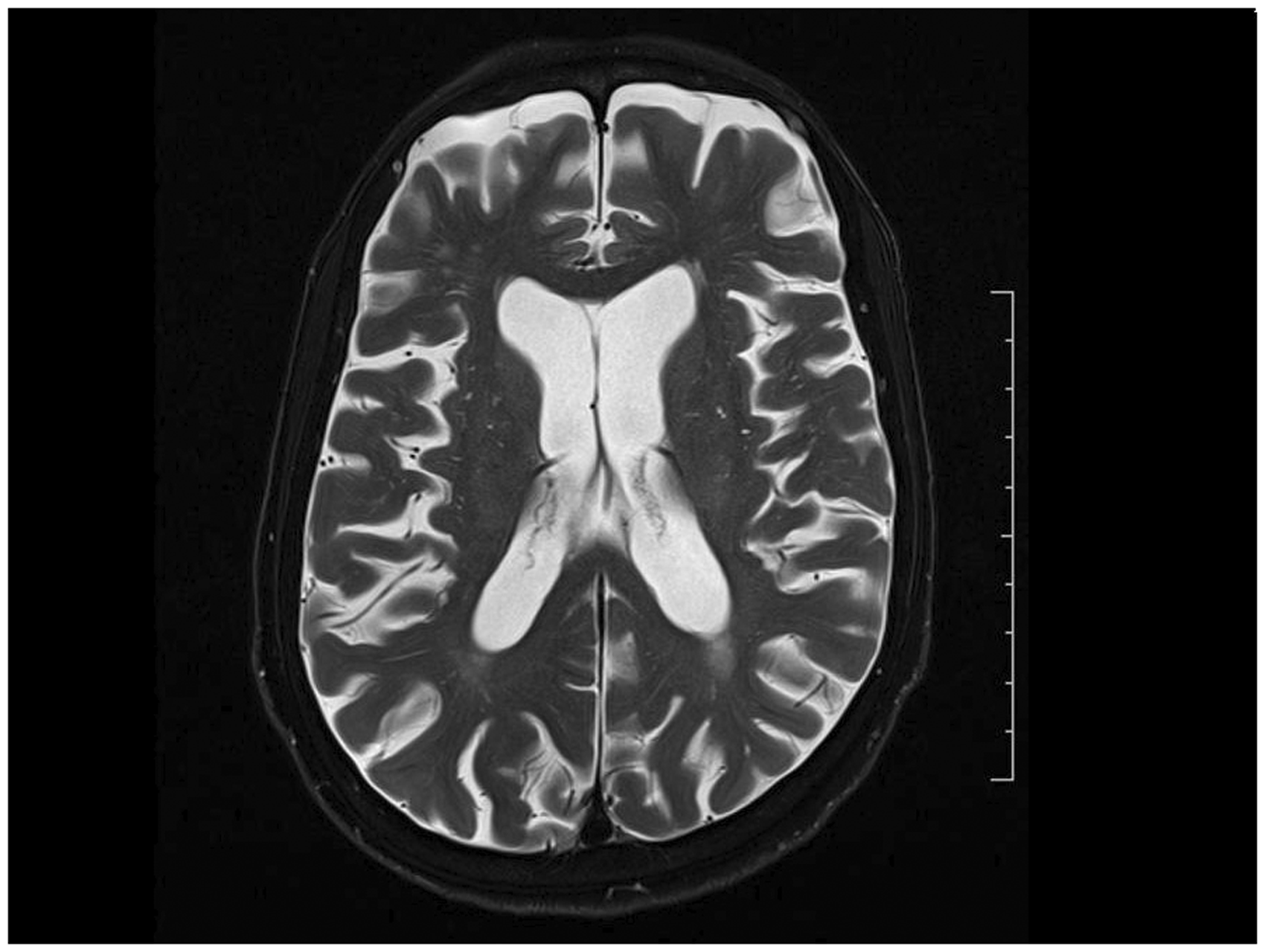
MRI brain. Image shows atrophy, mild ventricular dilatation, and periventricular white matter lesions.
Discussion
The CSF escape phenomenon has been widely studied and reported so far in HIV-1 infection but not in HIV-2 infection. Evolving evidence indicates that trajectory of disease progression in HIV-2 is similar to HIV-1, albeit at a slower rate.6,7 The clinical presentation and absence of any other opportunistic pathology seen in our case raised the suspicion of CSF escape. The MRI picture was reminiscent of other cases reported in the literature. 1 An additional feature was cerebral atrophy, which could be age related or as reported in one case of HIV-1. 8 The disassociation in plasma and CSF viral load counts confirmed our diagnosis of CSF escape. This was further endorsed by the rapid recovery of CNS symptoms seen after switching to new ART regimen.
To the best of our knowledge, this is the first documented case of HIV-2 CSF escape from India and probably globally. The present case had long-standing HIV-2 infection and had achieved sustained immune recovery with ART. In the absence of any specific literature for HIV-2, we looked for possible risk factors for neurosymptomatic CSF escape based on the available literature on HIV-1. 9 Our case rated low on most of the risk factors. The patient had excellent ART adherence. Her first-line regimen contained two antiretroviral medicines with good CNS penetration and the CNS penetration-effectiveness score of her ART using the 2010 version developed by Letendre 10 was 9.
There might be an increasing number of HIV-2 cases with prolonged ART exposure. Until now, for want of laboratory assays for HIV-2 viral load, immunological monitoring has been the mainstay of HIV-2 management in resource-limited settings. It is possible that many of the neurosymptomatic cases which may have had CSF escape were missed. As in case of HIV-1, treatment monitoring of HIV-2 needs to shift to virological monitoring. CSF escape should be considered as one of the differential diagnoses in all neurosymptomatic HIV-2 cases on ART.
Footnotes
Authors’ contribution
VK and RK were involved in clinical management of the reported case. RP prepared the manuscript. VK and RK provided valuable inputs in refining the manuscript draft. All the authors read and approved final manuscript draft.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.