
Abstract
Understanding how HIV is acquired can inform interventions to prevent infection. We constructed a risk profile of 10–24 year olds participating in the 2012 Kenya AIDS Indicator Survey and classified them as perinatally infected if their biological mother was infected with HIV or had died, or if their father was infected with HIV or had died (for those lacking mother’s data). The remaining were classified as sexually infected if they had sex, and the remaining as parenterally infected if they had a blood transfusion. Overall, 84 (1.6%) of the 5298 10–24 year olds tested HIV positive; 9 (11%) were aged 10–14 and 75 (89%) 15–24 years. Five (56%) 10–14 year olds met criteria for perinatal infection; 4 (44%) did not meet perinatal, sexual or parenteral transmission criteria and parental HIV status was not established. Of the 75 HIV-infected, 15 to 24 year olds, 5 (7%) met perinatal transmission, 63 (84%) sexual and 2 (3%) parenteral criteria; 5 (7%) were unclassified. Perinatal transmission likely accounted for 56% and sexual transmission for 84% of infections among 10–14 year olds and 15–24 year olds, respectively. Although our definitions may have introduced some uncertainty, and with the number of infected participants being small, our findings suggest that mixed modes of HIV transmission exist among adolescents and young people.
Keywords
Introduction
The burden of HIV among children, adolescents, and young people remains high with an estimated 1.8 million infected children <15 years and 1.8 million infected adolescents 10–19 years old in 2015; 1 60% of the adolescents living with HIV reside in Eastern and South Africa. 1 Furthermore, in 2015, 15–24 year olds accounted for 34% of the new HIV infections among adults globally and for 37% of the new HIV infections among adults in sub-Saharan Africa. 2 Undiagnosed HIV infection remains a common cause of morbidity and mortality among adolescents in Africa.3–5 The proportion of 15–19 year olds who have been tested and received test results ranges from 2 to 20%, 6 and only 38% of adolescents and adults living with HIV have access to treatment globally.7–9 In Kenya, in 2012, HIV prevalence was 0.6% among 10–14 year olds, 1.0% in 15–19 year olds, and 3.1% in 20–24 year olds, 10 with more females infected than males. 11
Sexual transmission accounts for most of the HIV infections among older adolescents and young adults;12–17 less common are injection drug use or blood transfusion.17,18 Perinatal infection also may contribute to this burden; one-third of perinatally-infected infants are diagnosed in adolescence.5,19–21 In addition, with the increasing availability of treatment even more perinatally-infected children are surviving into adolescence. 22 Understanding how HIV is acquired is necessary to inform interventions to prevent infection in adolescents and young adults.
Using biological and behavioral data from the nationally-representative, population-based 2012 Kenya AIDS Indicator survey (KAIS 2012), we conducted a secondary analysis to evaluate the potential modes of HIV transmission among 10–24 year olds in Kenya.
Methods
The KAIS 2012 was a nationally-representative cross-sectional household survey of persons aged 18 months to 64 years conducted in Kenya from October 2012 to February 2013. 23 Briefly, a two-stage cluster sampling design was used to select household clusters from a national household sampling frame. From each cluster, we randomly selected a sample of 25 households. Approximately half of these households were also selected for a child survey, which included children 18 months to 14 years old.
Trained interviewers interviewed heads of household to collect household characteristics including information of children and adolescents aged 0–17 years residing in the household. This included whether children’s parent(s) were living with or had died of HIV/AIDS. Secondly, we administered separate questionnaires to 10–14 year olds on socio-demographic characteristics, HIV knowledge, HIV testing history, social norms about sex, alcohol and drug use, HIV stigma, and self-reported HIV status. Sexual behaviors were only asked for 12–14 year olds. Thirdly, we administered the main adult questionnaire for persons ≥15 years old that collected socio-demographic characteristics, sexual activity in the past year, number of lifetime sexual partners, HIV testing history, HIV status of spouse or sexual partner(s), blood transfusion history, prior HIV testing, self-reported HIV status, and male circumcision. If the parent or guardian of adolescents aged 10–17 years was also a survey participant, they were asked about the child’s HIV status, HIV care information, and transfusion history. Consenting household members had their HIV test results linked to those of participating adolescents and young adults.
Blood specimens were tested at the National HIV Reference Laboratory for HIV antibody using Vironostika HIV-1/2 UNIF II plus O Enzyme Immunoassay (bioMérieux SA, Marcy l’Etoile, France) and confirmed using the Murex HIV.1.2.O HIV Enzyme Immunoassay (DiaSorin SpA, Saluggia, Italy). Repeat testing was performed for discordant results, and, if results remained discordant, final results were obtained using polymerase chain reaction (Cobas Amplicor HIV-1 Monitor Test, version 1.5, Roche Molecular Diagnostics, Pleasanton, CA).
This analysis is restricted to adolescents and young adults 10–24 years old with confirmed HIV infection based on survey laboratory results. All analyses were conducted in SAS version 9.3 (SAS Institute Inc., Cary, NC, USA). We categorized respondents into two age groups: 10–14 years and 15–24 years. We classified participants using a hierarchical HIV risk algorithm beginning with putative perinatal transmission. We classified participants as perinatally infected if their biological mother was HIV infected based on laboratory test, if HIV infection was reported, or if their mother had died. If no data were available for the mother, we classified participants as perinatally infected if their biological father was HIV infected based on laboratory test, HIV infection was reported, or if their father had died. Among those without evidence of perinatal transmission, we used self-reported behavioral data to determine risk for sexual transmission. We classified participants as sexually infected if they reported ever having had sex and had had sex with ≥2 lifetime sex partners or, for those with a single lifetime partner, if that partner’s HIV status was positive or unknown. Finally, we classified the remaining participants who did not meet criteria for perinatal or sexual infection as parenterally infected if they had a history of blood transfusion. In this analysis, all counts and percentages were unweighted.
During the survey, verbal permission was obtained from parents or guardians to draw blood from participants who were 18 months to 17 years old and verbal assent from 10–17 year old participants whose parents or guardians consented to their participation. The KAIS 2012 protocol was approved by the Institutional Review Boards of the Kenya Medical Research Institute, the U.S. Centers for Disease Control and Prevention and the University of California, San Francisco.
Results
Of the 2094 eligible 10–14 year olds, 1661 (80%) were interviewed and 1480 (71%) were tested for HIV. Of these, nine (0.6%) were infected (Table 1). Four (44%) were female. Three (33%) had a mother known to be HIV infected; none reported sexual activity. The mothers of two girls were confirmed to be uninfected, and the HIV status of the mothers of the remaining four was unknown. Of the four whose mothers’ HIV status was unknown, two had infected fathers; the HIV status of the remaining two fathers was unknown. Of the two whose mothers were confirmed to be uninfected, one was 12 years old and the other 14. Therefore, overall, for the nine HIV-infected 10–14 year olds, five (56%) met our criteria for having most likely been infected perinatally. Of the remaining four (44%), two were female. None met our criteria for perinatal, sexual, or parenteral transmission (Figure 1).
Characteristics of HIV-infected adolescents/young adults aged 10–24 years-old, KAIS 2012.
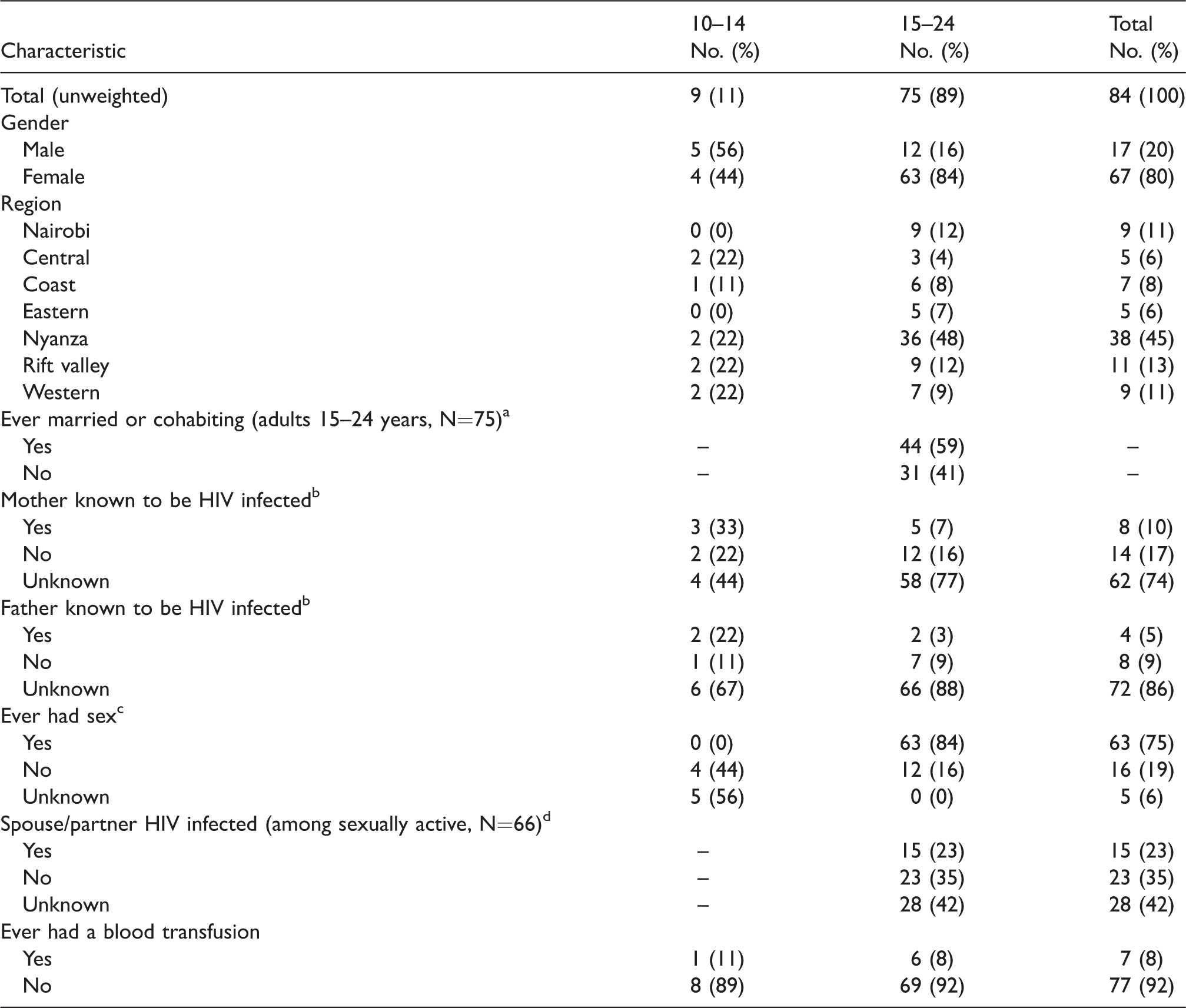
aMarital status only asked for those who were 15–24 years old.
bHIV status of mother/father determined by the HIV test if parent lived in the same household, or through self-report by the head-of-household on the HIV status of the mother and father of adolescents 10–17 years.
cSexual behaviors questions asked to 12–24 year olds only.
dHIV status of spouse/partner determined by HIV test if the spouse/partner lived in the same household and consented to the KAIS blood test, or through self-report by the respondent on their knowledge of the HIV status of the spouse/partner.
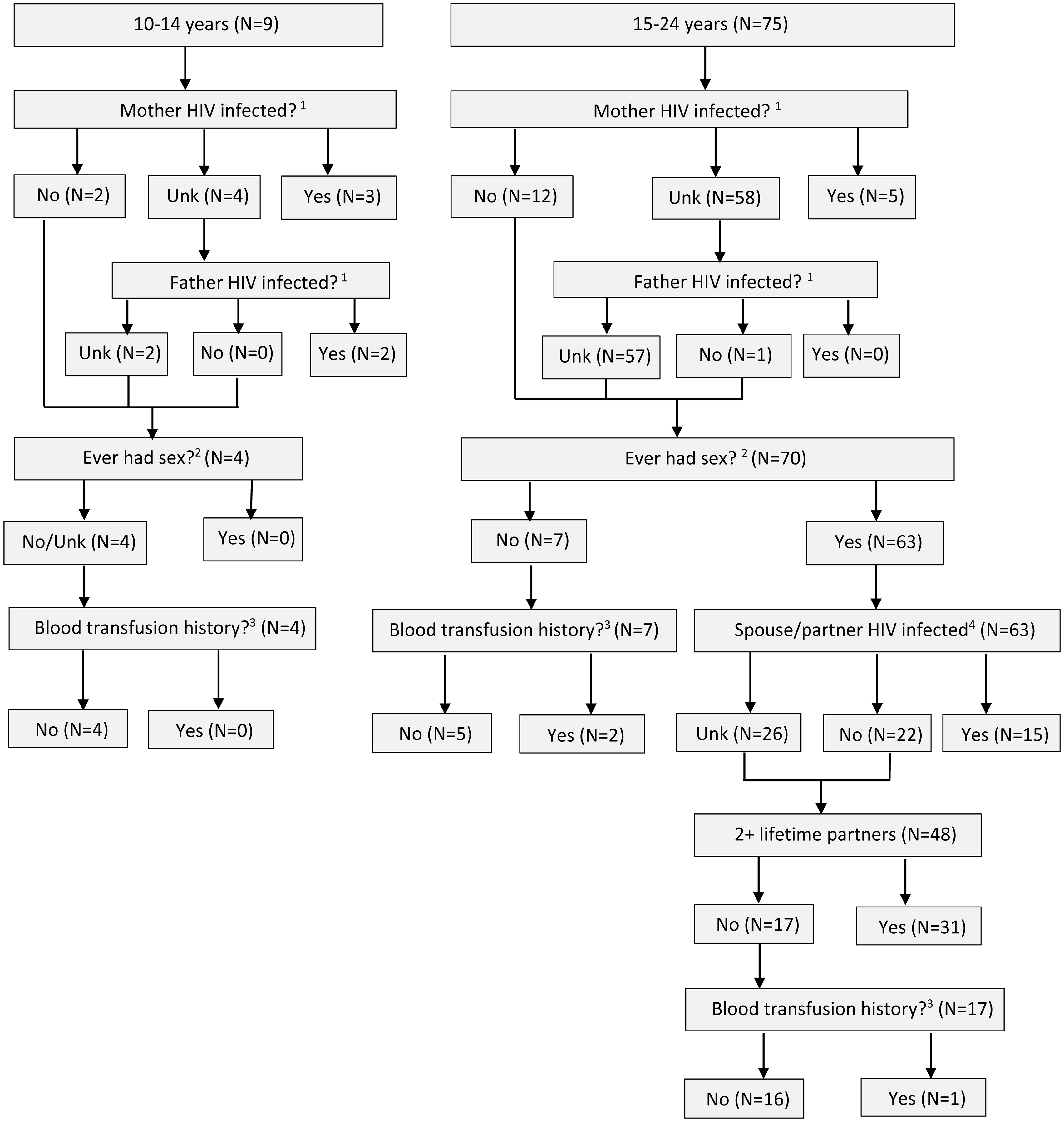
HIV transmission risk of HIV-infected adolescents/young adults aged from 10 to 24 years old (N = 84).Unk: unknown.1The HIV status of the mother and father was determined by the following criteria: a) if the mother/father consented to the KAIS survey and the HIV test was negative, then they were considered uninfected (‘No’); b) if the mother or father consented to the KAIS survey and the HIV test result was positive, or in the event that the mother/father did not consent to the KAIS test or was not a resident in the household, but the head of household reported in the household interview that the parent was infected or had died from HIV/AIDS, they were considered infected (‘Yes’); or c) if the parent did not test or was not in the household and no other information was available about an illness or death from HIV/AIDS, then their HIV status was considered ‘Unknown’.2Sexual histories were available only for adolescents/young adults 12–24 years. Therefore, ‘ever had sex’ was classified as ‘unknown’ for adolescents under 12 years.3Blood transfusion histories were determined by self-report during interview.4The HIV status of the spouse/partner was determined by KAIS HIV test result (if the spouse/partner resided in the household and consented), or by self-reported knowledge of the HIV status of their spouse or sexual partner.
Of the 5708 eligible 15–24 year olds, 4546 (80%) were interviewed and 3818 (67%) were tested; 75 (2%) were infected. Of these, 63 (84%) were female, 44 (59%) had ever been married or cohabitated, 63 (84%) had ever had sex, and 15 (23%) had a known HIV-infected sexual partner (Table 1). Twenty-six (41%) had no information on the HIV status of their sexual partners. Of the 75 HIV-infected 15–24 year olds, five (7%) met our criteria as having been most likely infected perinatally as all five had an HIV-infected mother. Twelve (16%) had mothers who were known to be HIV uninfected, and 58 (77%) had mothers whose HIV infection status was unknown. Of these 58, one had an HIV-uninfected father, and the HIV status of the remaining 57 fathers was unknown. Overall, 63 (84%) of 15–24 year olds met our criteria for having been most likely infected sexually; 15 (24%) had sex with a known HIV-infected partner, 31 (49%) had ≥2 lifetime, and for the remaining 17 (27%) who had reported having had sex with a single partner whose HIV status was unknown. Of the seven 15–24 year olds who did not meet our criteria for perinatal or sexual transmission, two (3%) had received blood transfusions and met our criteria for having been most likely infected parenterally. The remaining five (7%) did not fall into any of the modes of transmission categories (Figure 1).
Discussion
We found that 12% of all the 10–24 year olds who participated in KAIS 2012 had an HIV-infected mother or father, suggesting they were most likely infected perinatally and had survived to adolescence or young adulthood. However, for three quarters, the mode of transmission was likely sexual. Overall, similar to previous reports, most infections were among women.24,25 Overall, 56% of HIV-infected 10–14 year olds had a risk for perinatal HIV transmission compared to only 7% of the HIV-infected 15–24 year olds. However, perinatal HIV transmission for this group may have been under ascertained considering that none of the four 10–14 year olds for whom we were unable to assign a potential risk reported being sexually active and none had a blood transfusion. These findings corroborate other studies from countries with generalized epidemics that have shown that there is a substantial number of HIV-infected children who are infected perinatally and survive into adolescence undiagnosed.12–14 Although we cannot draw definitive conclusions due to the small number of HIV-infected 10–14 year olds, our findings highlight a need to further explore modes of HIV transmission in this age group.
We also found that sexual transmission likely accounts for the majority of HIV transmission among older age groups. These findings are similar to other studies where sexual transmission is the major mode of infection among older adolescents and young adults. 26 Among sexually-active 15–24 year olds in our study, more than one third did not know the HIV status of their sexual partners. If these sexual partners are uninfected, the HIV-infected adolescents and young adults pose a risk of transmitting HIV to them. On the other hand, if these partners were infected, they were likely the sources of infection for our study participants. Both scenarios underscore the importance of diagnosis and disclosure of HIV status as a crucial step in the prevention of HIV infection among young people.27,28
This study has limitations. Due to the small number of HIV-infected 10–24 year olds, some of the estimates are potentially imprecise, and the unweighted analyses we have presented are only applicable to infected participants in our sample. Therefore, our estimates cannot be generalized to the broader Kenyan population. Also, not all parents or sexual partners of infected 10–24 year olds were tested for HIV; therefore, the HIV status of infected parents and sexual partners is based on self-report alone and may be underreported given the stigma associated with HIV/AIDS or because of lack of awareness of their parents’ or partners’ HIV status. Since sexual information was not collected among 10–11 year olds, we could not assess sexual risk among this age group. Finally, there were a number of assumptions made in constructing the algorithm for assigning mode of HIV transmission, and we can only infer the most likely mode of transmission. Our algorithm, thus, may have misclassified the actual mode of HIV transmission of infected participants.
In conclusion, we found that among 10–14 year olds, perinatal transmission likely accounted for more than half of HIV infections; we found no apparent risk in the remainder of 10–14 year olds, but we could not exclude perinatal transmission or unreported sexual activity. Sexual transmission accounted for the large majority of infections among 15–24 year olds, but there were a small number in this group who were likely infected perinatally. Given the small numbers of HIV-infected adolescents, interpretation of our findings should be done with caution. Despite the limitations in this study, our findings suggest that mixed modes of HIV transmission exist among adolescents and young people in Kenya. Thus, while scaling up prevention of perinatal transmission of HIV is critical, it will not eliminate a large proportion of infections for adolescents and young people in Kenya. Targeted interventions for adolescents and young adults should include promotion of condoms and disclosure of HIV status to prevent sexual transmission, HIV testing with immediate linkage to care and treatment, and close monitoring on treatment to ensure that high levels of adherence, viral suppression, and survival can be achieved for this population.
Footnotes
Authors’ contributions
BN, TK and GR designed the study design, analyzed and interpreted the data, and wrote the manuscript. AK interpreted the data and, revised the manuscript. MM, AM, and JW revised the final manuscript. All authors approved the final version of the manuscript.
Acknowledgments
We thank the KAIS 2012 study team for data collection and all the children and families that participated in this survey.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: KAIS 2012 was made possible through financial support from the U.S. President's Emergency Plan for AIDS Relief (PEPFAR) through CDC and USAID, Joint United Nations Team on HIV/AIDS, JICA, Global Fund and the World Bank. The authors received no financial support for authorship and publication of this article.