
Abstract
Chlamydia trachomatis and Neisseria gonorrhoeae constitute major public health problems among women, but the burden of infection in sub-Saharan Africa is poorly documented. We conducted a structured review of the prevalence and incidence of genital, oral and anal C. trachomatis and N. gonorrhoeae infection in women in sub-Saharan Africa. We searched Medline, EMBASE and Web of Science over a 10-year period for studies on epidemiology of genital, oral and anal chlamydial infection and gonorrhoea in women in all countries of sub-Saharan Africa. We assessed geographic and demographic differences in prevalence and incidence of infection; weighted mean prevalence estimates were calculated with a random-effect model. A total of 102 study results were included, with data available for 24/49 of sub-Saharan countries. The weighted prevalence of chlamydial infection was lower among women in community-based studies (3.9%; 95% CI: 2.9–5.1%) than for women recruited at primary healthcare facilities (6.0%; 95% CI: 4.2–8.4%, p < 0.001); the same was observed for gonorrhoea (2.2%; 95% CI: 1.2–4.0% vs. 4.2%; 95% CI: 3.2–5.6%, p < 0.001). Prevalence of Chlamydia among sex workers was 5.5% (95% CI: 4.2–7.3%) and gonorrhoea 7.6% (95% CI: 5.4–11%). Seven studies reported on incidence which varied between 0.75–28 and 2.8–17 per 100 person-years-at-risk for chlamydial infection and gonorrhoea, respectively. Only two studies reported on anal infections and one on oral infection. This overview underscores the considerable incidence and prevalence of genital C. trachomatis and N. gonorrhoeae in women in different settings in sub-Saharan Africa. Better control strategies are warranted to reduce the burden of infection and to prevent long-term complications of these infections.
Keywords
Introduction
Chlamydia trachomatis and Neisseria gonorrhoeae are the most common bacterial sexually transmitted infections (STIs) worldwide. The most recent World Health Organization (WHO) estimates for the African region are an annual incidence (per 100 women) of 2.2 and 5.0 and prevalence (%) of 2.6 and 2.3 for C. trachomatis and N. gonorrhoeae infections in women aged 15–49 years in 2008, respectively. 1 These regional estimates are the highest in the world, and recent modelling analysis classified sub-Saharan Africa as the only region in the high STI incidence/prevalence category.1,2
Women are more likely to be infected than men for several reasons. First, transmission is more effective from men to women due to differences between female and male susceptibility of the genital tract for infection.3,4 Second, gender inequality is especially common in resource-poor settings and places women in a more vulnerable position, e.g. for negotiating condom use or experiencing coercion. 5 Finally, infection in women occurs more frequently without symptoms and is therefore more often left untreated; the majority of these infections in women are asymptomatic.6,7 Women with unrecognized infection have an increased risk for pelvic inflammatory disease with its complications of ectopic pregnancy, tubal infertility and chronic pelvic pain. 8 Furthermore, in addition to epidemiological evidence, it is biologically plausible that these STIs enhance HIV acquisition and might facilitate transmission.9,10 The identification and management of these STIs and other reproductive tract infections were identified as critical components for quality sexual and reproductive health services and have been incorporated into existing services in several countries in Africa.
As microbiological diagnosis of STIs is generally unavailable in low resource settings, the WHO recommends a syndrome-based approach to manage individuals with STI-associated symptoms. The benefits and disadvantages of this syndromic approach are well documented.7,11 An important drawback is that many infections remain untreated as they are asymptomatic whereas overtreatment with resultant unnecessary use of antibiotics also occurs, thereby enhancing risk of antimicrobial resistance.6,12 Although many countries report on the prevalence of syndromes, data about distribution of bacterial STIs in sub-Saharan African countries are generally scattered. Moreover, the currently available overviews focus on a single country or specific populations at risk, e.g. female sex workers.13–15
To our knowledge, there is no recent overview of the distribution of genital C. trachomatis and N. gonorrhoeae in women in sub-Saharan Africa. This structured review aims to inform health policies and STI control strategies for women living in low-resource settings by providing insight into the distribution of genital, oral and anal C. trachomatis and N. gonorrhoeae infections in women over the past 10 years across sub-Saharan Africa.
Methods
Search strategy and selection criteria
We searched for studies that report on the epidemiology of C. trachomatis and N. gonorrhoeae in women in sub-Saharan Africa, using a systematic review approach and report in accordance with the PRISMA guidelines. 16 We used Medline (through PubMed), EMBASE and Web of Science and searched for studies from 1 January 2005 to 31 December 2014 using two different strategies. First, the MeSH-terms and keywords ‘Chlamydia trachomatis’, ‘Chlamydia’, ‘Neisseria gonorrhoeae’ and ‘Gonorrh(o)ea’ combined with ‘sub-Saharan Africa’ or ‘Africa South of the Sahara’ (PubMed) were used. For the second search we used the same words as free text combined with the name of one of the 49 countries in sub-Saharan Africa as per combined definition of the World Health Organization (WHO) and the World Bank.17,18 We did not search conference abstracts or grey literature for additional studies. No language restrictions were applied.
Study selection and eligibility criteria
The following protocol was used to retrieve studies to be included in this review. Reference lists were generated, and titles and abstracts were independently screened by two authors (RPHP and JHD) to identify relevant articles on C. trachomatis and N. gonorrhoeae in women in sub-Saharan Africa (Figure 1). All records identified for further evaluation by at least one of the two authors were checked for duplicates and included for full text screening. The retrieved full text articles were then independently reviewed by two investigators (SPV and JHD) with discordant views resolved by referral to a third investigator (RPHP).
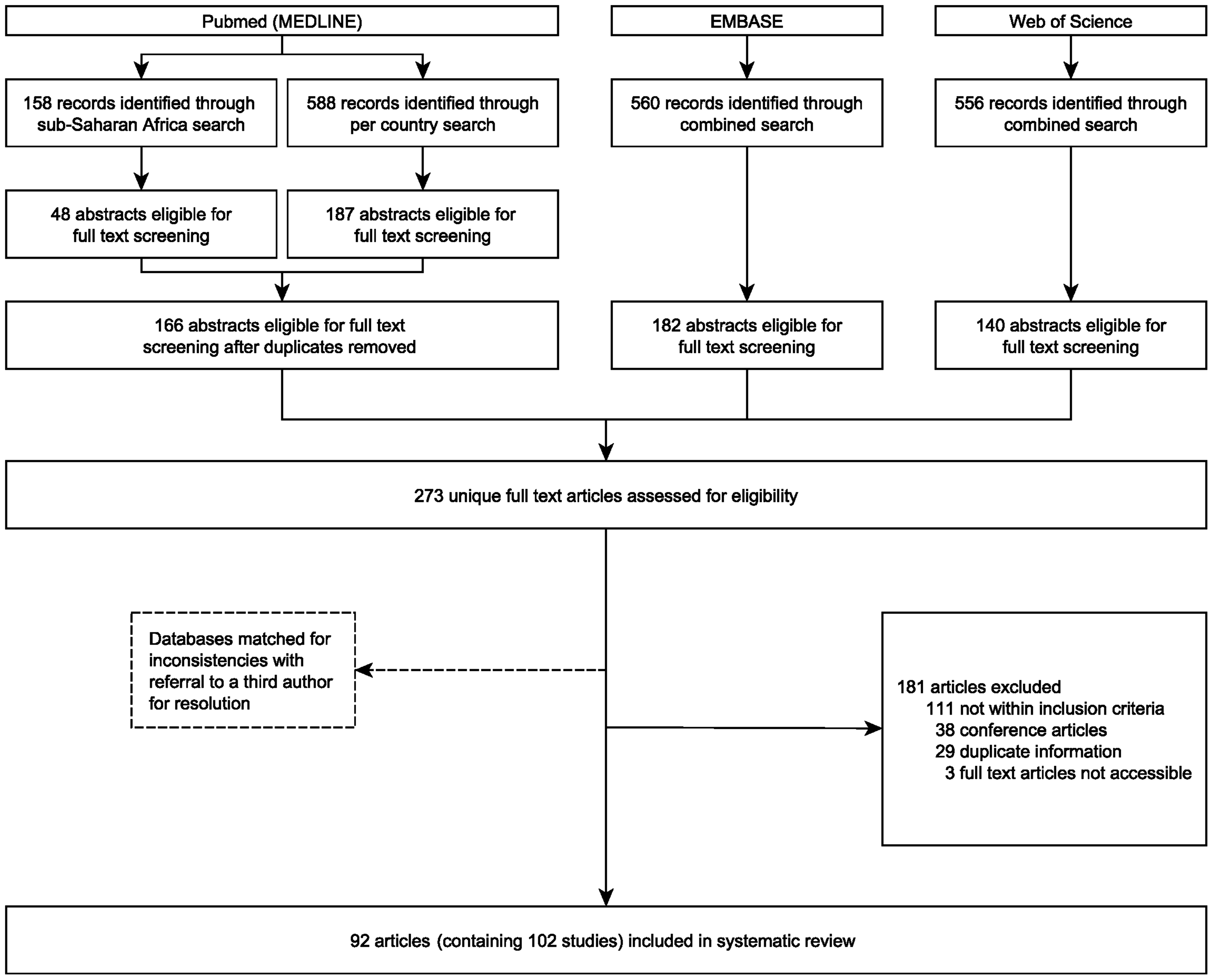
Literature search and selection. Two searches of PubMed were conducted and a combined search was used for EMBASE and Web of Science.
The following inclusion criteria were used: studies reporting on incidence and/or prevalence of C. trachomatis and/or N. gonorrhoeae in a study sample of at least 100 women recruited at one of the following settings: (a) in the general community, (b) at primary healthcare (PHC) facilities (these include: family planning (FP), antenatal care (ANC), PHC clinic, youth clinics, HIV clinic for voluntary counselling and testing (VCT)) or (c) visiting a sexually transmitted diseases (STD) clinic. Furthermore, studies of female commercial sex workers (FSWs) and women working in a bar/bottleshop were evaluated as high-risk groups. No age restriction was applied and the review was limited to genital, anal and oral infections; Chlamydia trachomatis and Neisseria gonorrhoeae infections of other body sites (e.g. eye, joint) were excluded. Studies were only included if one of the following laboratory methods was used: nucleic acid amplification test (NAAT) for C. trachomatis and culture or NAAT for N. gonorrhoeae. Studies were excluded from further analysis based on: study design (review articles, case reports, comments on other researchers’ work, studies using modelling for estimates, and case-control studies without baseline data), study objectives (general microbiology only [e.g. resistance pattern] and ocular infection), specimens used for diagnostic testing (any type other than urine, vaginal, endocervical, oropharyngeal or anorectal swab) and missing information about laboratory method or specimen. Measures of outcome were prevalence (number of women with a positive test divided by total number of women with a test with interpretable result) and incidence (the proportion of all women that were negative at baseline but became infected over a defined period of time) of C. trachomatis and N. gonorrhoeae infection.
In the event that data from one study were reported in two or more publications, we selected the most relevant paper with regard to our objectives. For one study with no differentiation between the prevalence of Chlamydia infection and gonorrhoea and for one study with no differentiation of infection between men and women we contacted the authors for detailed information.19,20 In the case of a study involving multiple countries and/or study populations, available data were split accordingly for analysis and were eligible if each setting or risk group had a population of ≥100 women. Trials were only included if baseline data were presented, as interventions could potentially bias the results.
Data extraction and analysis
Data were independently extracted by two authors (SPV and JHD) using Microsoft Access version 2013 (Microsoft Corporation, Redmond, WA). We extracted the following variables from each article: country, year of publication, setting, population, laboratory material and method, population size (n), HIV prevalence if given, mean or median age if given, and genital, anorectal and oropharyngeal Chlamydia and/or gonorrhoea prevalence/incidence. Both databases were compared for quality of entry with referral of discordant entries to a third author (RPHP) for resolution.
For data analysis, each country was assigned a socioeconomic status, based on the UN Human Development Index (HDI) of 2014: a composite index measuring average achievement in three basic dimensions (life expectancy, education and standard of living) of human development and ranges from very high, to high, to medium and to low. 21 Furthermore, to link our data to the HIV burden in the continent, we used the estimated HIV prevalence among adults (15–49 years) and in sex workers reported by UNAIDS in 2014.22,23
Data were analysed using SPSS version 20.0 (SPSS Inc, Chicago, IL) and R software package 3.3. Overview of C. trachomatis and N. gonorrhoeae prevalence per setting and population was created using maps made by ArcGIS (Esri, Redlands, CA). Per population group the weighted prevalence was calculated with corresponding 95% confidence intervals (CIs) using the random-effect model including statistical analysis of heterogeneity. The association between the prevalence of C. trachomatis and N. gonorrhoeae infection, and between these STIs and estimated HIV prevalence, was plotted using scatter plot (R2 values are provided in the text) and calculated using linear regression analysis.
Funding source statement
There was no relevant sponsor of the study that could have played a role in design, data collection, data analysis, data interpretation, or writing of the report. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Results
We identified 1862 records of which 488 (26%) were potentially relevant. Of these, 215 were duplicates leaving the remaining 273 records for full text screening. We identified 29 publications that were considered duplication of STI data from a single research study; these were excluded from further analysis.11,24–51 After eligibility assessments, 102 study results were included in this analysis, which were published in 92 articles as eight articles had data from two countries and/or study populations and one from three (Figure 1, Table 2 and S1 Table).
Characteristics of studies assessing C. trachomatis and N. gonorrhoeae in sub-Saharan Africa
Prevalence data were available for 24 of the 49 countries in sub-Saharan Africa with wide variation (range: 1–18) in the number of studies that was conducted per country (Figure 2). Among these, seven studies reported on incidence within six countries (Table 3). Data on C. trachomatis were reported in 84 studies and N. gonorrhoeae in 101; 81 (79%) studies reported prevalence data of both infections. Median size of study population was 448 participants (range: 100–6514). Characteristics of 88 studies reporting on prevalence in women recruited in the general community,20,52–69 at PHC settings6,7,19,35,70–104 and FSWs105–124 are described in Table 1. Furthermore, we retrieved 7 studies conducted at the STD clinic72,125–130 and 6 studies targeting bar workers,131–136 bringing the total of studies to 102 as one study included women from both PHC setting and STD clinic. 72
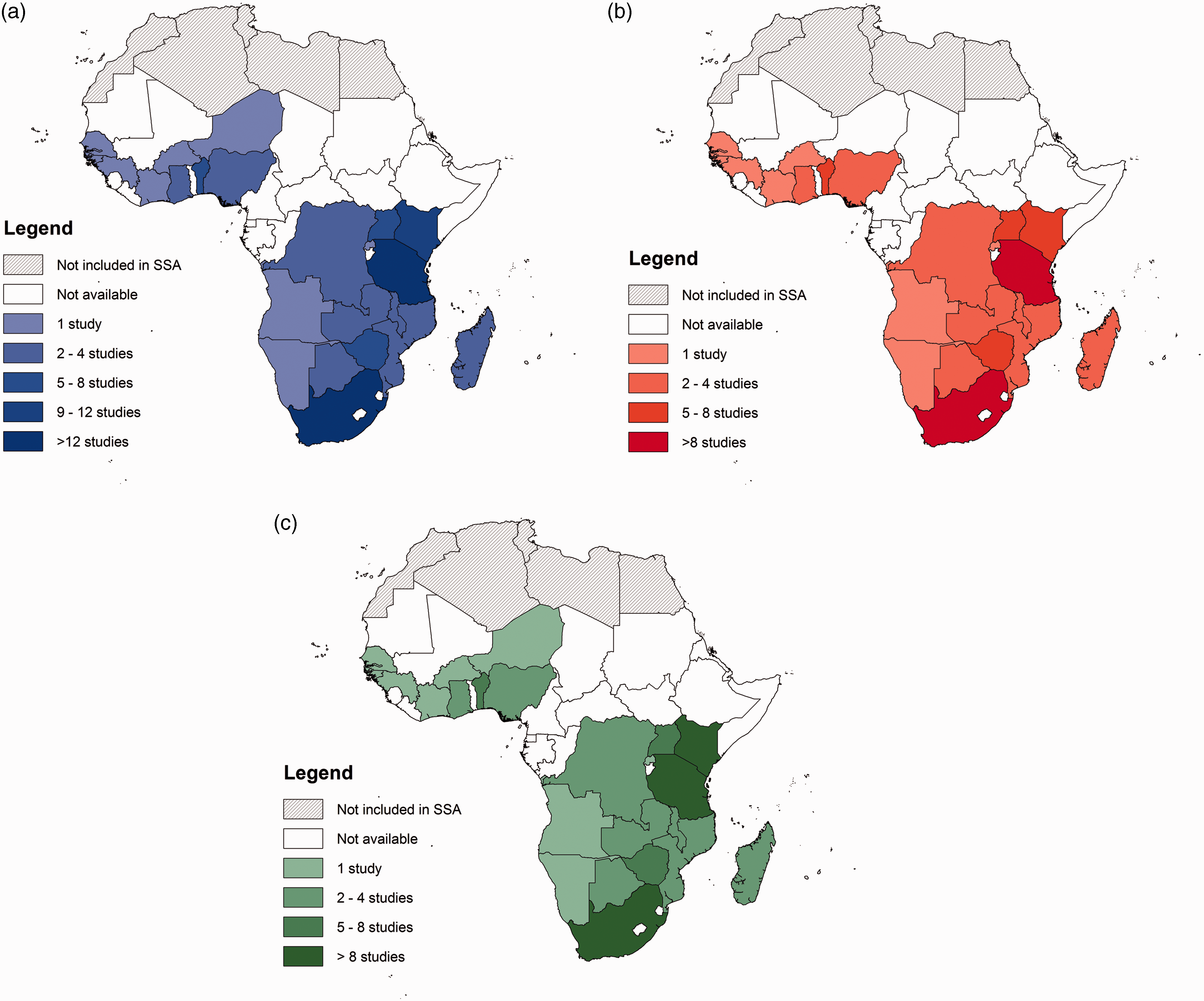
Number of studies reporting on the prevalence of (a) either Chlamydia trachomatis or Neisseria gonorrhoeae, (b) Chlamydia trachomatis and (c) Neisseria gonorrhoeae in women in sub-Saharan Africa as published in the period 2005–2014.
Specifications of studies included in this structured review.
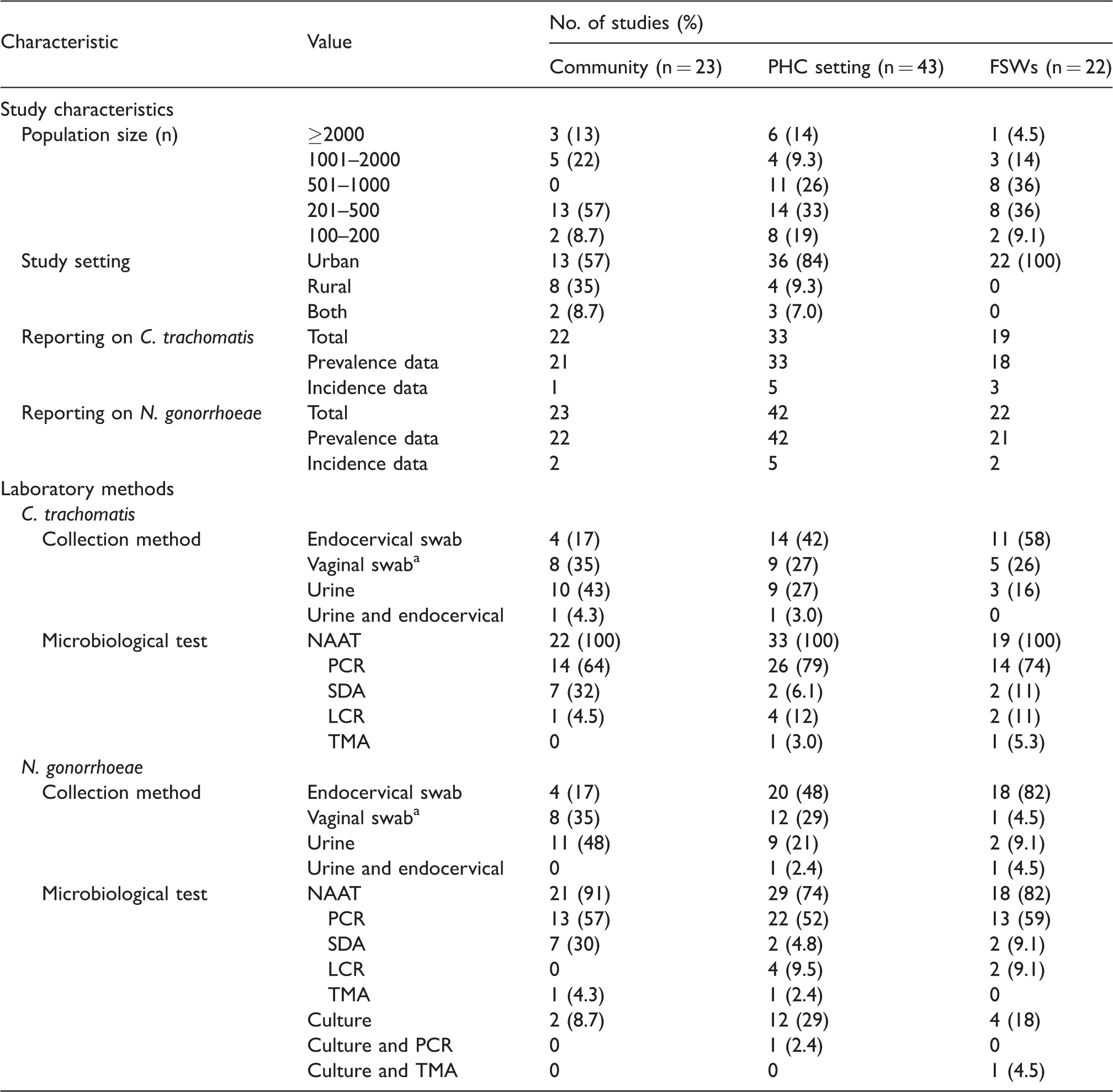
Note: Data of bar workers (n = 6) and women visiting STD clinic (n = 7) are not given in this table, as is one study which included women from both PHC setting and STD clinic.
PHC: primary healthcare setting; FSWs: female sex workers; PCR: polymerase chain reaction; SDA: strand displacement amplification; LCR: ligase chain reaction; TMA: transcription-mediated amplification.
aAmong the 30 studies that tested women with a vaginal swab, 18 (60%) used healthcare-worker collection and in 12 (40%) swabs were self-collected.
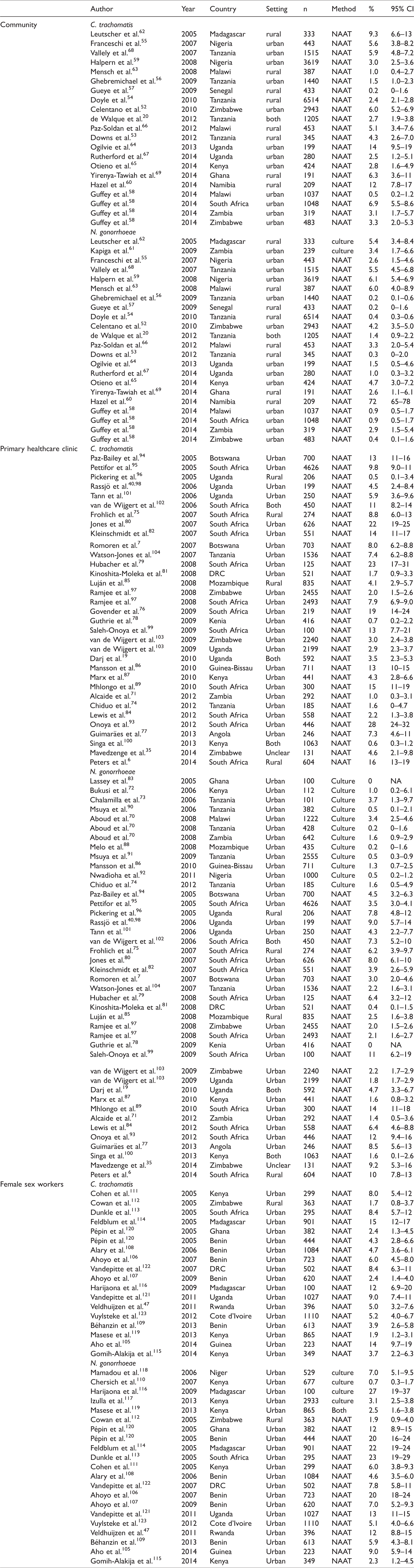
Prevalences of C. trachomatis and N. gonorrhoeae in sub-Saharan Africa.
Incidence per 100 woman years of C. trachomatis or N. gonorrhoeae reported in sub-Saharan Africa from 2005 to 2014.
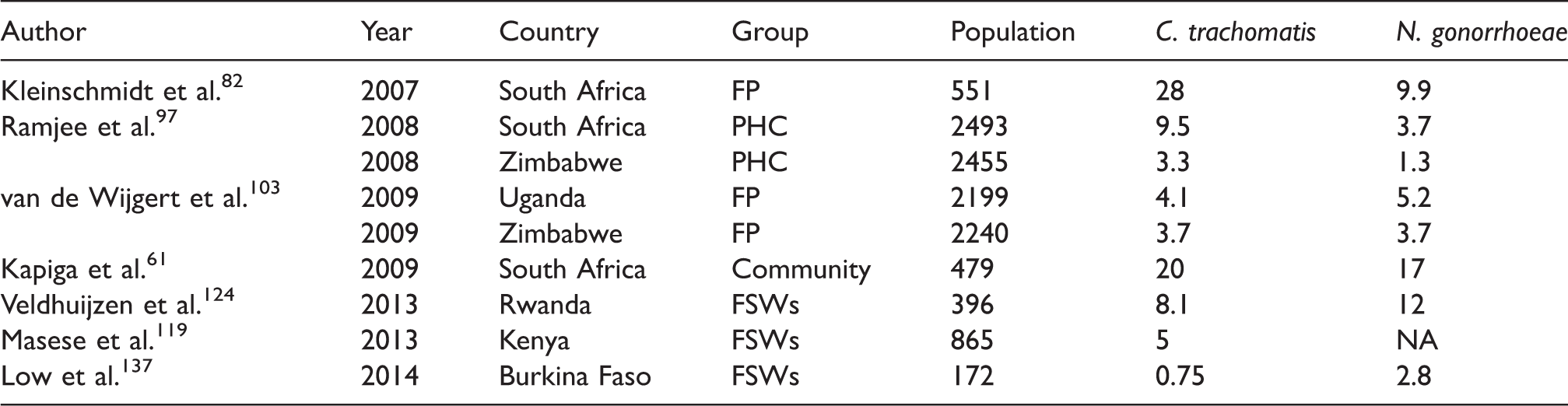
FSWs: female sex workers; FP: family planning; PHC: primary healthcare clinic; NA: not available; DRC: Democratic Republic of Congo.
Overall, endocervical swabs were the most frequently used for laboratory detection of C. trachomatis (44% of studies) and N. gonorrhoeae (49%), followed by vaginal swab (29% and 26%). Overall, we did not observe a difference in prevalence between studies using urine (26%) versus endocervical or vaginal swabs for specimen collection for the detection of C. trachomatis (median 5.1% vs. 5.9%, p = 0.29). Polymerase chain reaction (PCR) was the most frequently used method for detection (75% and 54%), followed by strand displacement amplification (SDA) for Chlamydia (14%) and culture for gonorrhoea (23%). For N. gonorrhoeae infections in women, we observed an overall difference in median prevalence between culture (1.6%) and NAAT (4.7%) methods for detection of infection (p = 0.001). We observed this difference for studies that recruited women at PHC settings (p < 0.001), but not for studies assessing the community (p = 0.31) or FSWs (p = 0.59) as only a few (2/23 and 4/21) used culture.
Prevalence of C. trachomatis and N. gonorrhoeae in the community-based studies
Prevalence of C. trachomatis and N. gonorrhoeae in women recruited in community-based studies varied across sub-Saharan Africa (Figures 3(a) and 4(a)) and is summarized in Table 2. Highest prevalences of C. trachomatis and N. gonorrhoeae was observed in Northwestern Namibia where in one study 29/209 (12%) and 150/209 (72%) of women living in 28 rural villages in Kaokoland were infected, respectively. 60 The weighted prevalence for C. trachomatis was 3.9% (95% CI; 2.9–5.1%; I2 = 95%) and for N. gonorrhoeae 2.2% (95% CI; 1.2–4.0%) in sub-Saharan Africa. When excluding the study from Hazel et al. 60 because of outlier high N. gonorrhoeae prevalence (72%), the weighted prevalence was 1.9% (95% CI; 1.3–2.8%; I2 = 95%) among 23850 women.
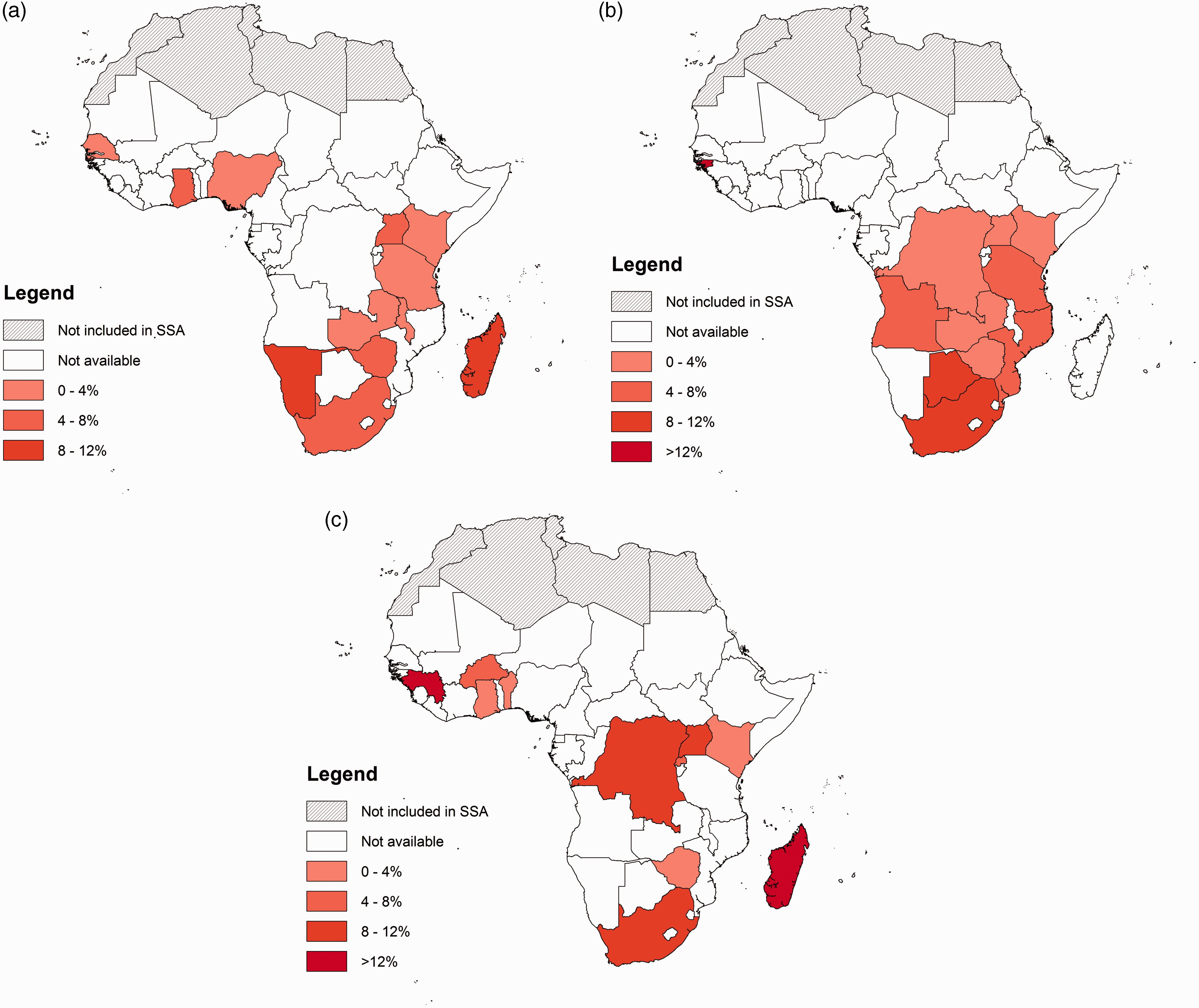
Prevalence of Chlamydia trachomatis reported (a) in general community settings, (b) in PHC settings and (c) among FSWs in sub-Saharan Africa. For community settings, we observed data in 21 studies in 12 countries with no studies reporting prevalence higher than 12%; for PHC settings, we observed data in 33 studies in 11 countries and for FSWs, we observed data in 18 studies in 11 countries.
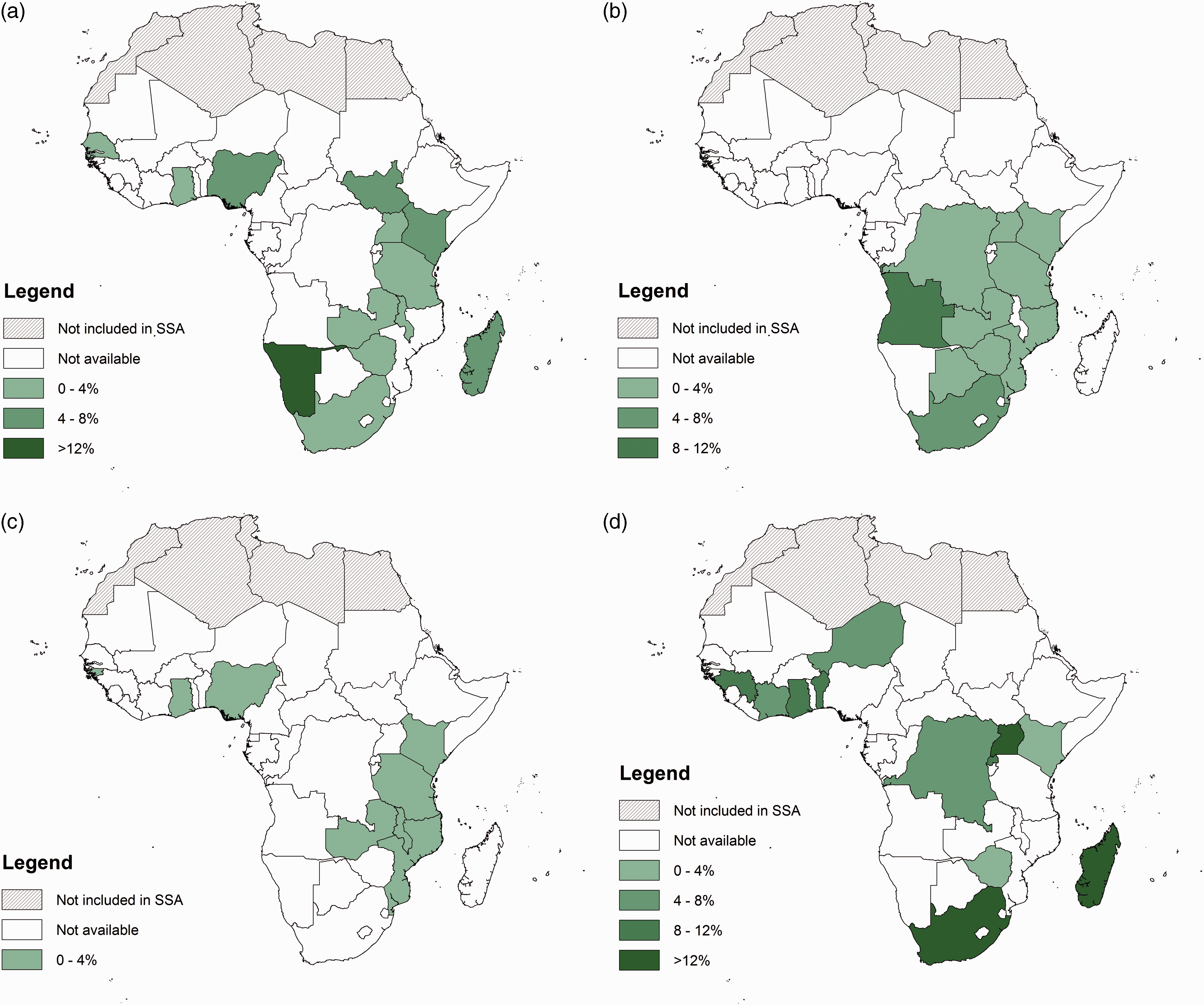
Prevalence of Neisseria gonorrhoeae reported (a) in general community settings, (b and c) in PHC settings and (d) among FSWs in sub-Saharan Africa. For community settings, we observed data in 22 studies in 12 countries with no studies reporting prevalence between 8 and 12%; for PHC settings, we observed data detected by NAAT (b) in 30 studies in 10 countries and by culture (c) in 12 studies in 8 countries and for FSWs, we observed data in 21 studies in 12 countries.
The prevalence of infection was different for the rural compared to the urban setting. For C. trachomatis, the prevalence was 3.0% (n = 8865) in the rural and 4.2% (n = 13,750) in the urban setting (p < 0.001) whereas for N. gonorrhoeae; 1.0% (8656) versus 3.6% (13989) prevalence was observed, respectively (p < 0.001). In addition to studies conducted at the community level, prevalence of 25% (144/569) for chlamydial infection and 19% (108/568) for gonorrhoea was reported among 569 young women (median age 19 years) from randomly selected high schools in rural coastal Kwazulu-Natal.
Prevalence of C. trachomatis and N. gonorrhoeae in women recruited at PHC settings
Thirty-three studies reported on prevalence of C. trachomatis and 42 for N. gonorrhoeae in women attending PHC facilities; 12/42 (29%) used culture and 29/42 (69%) used NAAT as the detection method (Table 2). Data of women recruited at PHC settings were based on the recruitment of women at primary healthcare clinics (14 studies); ANC clinics (12 studies); FP clinics (8 studies); youth clinics (5 studies) and HIV clinics (4 studies). South Africa had the highest number (13) of studies reporting on prevalence of chlamydial infection with a mean of 11% (median 14%; range, 2.2–28%) (Figures 3(b) and 4(b)). For C. trachomatis, we observed a weighted prevalence of 6.0% (95% CI; 4.2–8.4%; I2 = 98%) and for N. gonorrhoeae a weighted prevalence of 1·0% (95% CI; 0.6–1.8%; I2 = 76%) detected by culture and 4.2% (95% CI; 3.2–5.6%; I2 = 94%) by NAAT.
Prevalence of C. trachomatis and N. gonorrhoeae among FSWs and Bar workers
Among FSWs, highest prevalence was reported in Madagascar (14%) and Guinea (14%) for C. trachomatis infection, and in South Africa (23%), Madagascar (22%) and Uganda (13%) for infection with N. gonorrhoeae (Figures 3(c) and 4(d)). Lowest prevalence was observed in Ghana (2.4%) for chlamydial infection and in Zimbabwe (1.9%) for gonorrhoea. We observed a weighted prevalence of 5.5% (95% CI; 4.2–7.3%; I2 = 93%) for chlamydial infection and 7.6% (95% CI; 5.4–11%; I2 = 98%) for gonorrhoea. In addition, studies reporting on prevalence of STIs in bar workers were mainly conducted in Tanzania. Four studies, all from Tanzania, reported on prevalence of chlamydial infection (range, 6.0–13%) which gave a weighted mean of 9.0% (95% CI; 6.4–13). For gonorrhoea, six studies reported on prevalence of gonorrhoea (range, 0.9%–7.9%) with a weighted mean of 4.8% (95% CI; 2.0–11), including one study in Ghana with reported prevalence of 0.9% and the remainder from Tanzania.
Comparison of prevalences of infection between different settings
A higher weighted prevalence of C. trachomatis infection was observed at PHC settings (6.3%) as compared to women recruited in the community (3.9%; p < 0.001) The same difference was observed for N. gonorrhoeae infection with a weighted prevalence of 4.3% at PHC facilities and 1.9% among women in the general community (p < 0.001) The difference remained when excluding the study from Namibia as potential outlier with 72% prevalence.
In addition, weighted mean prevalence among women recruited at STD clinics was higher compared to women recruited at PHC settings for both chlamydial infection (8.8%; 95% CI: 3.5–14%, p < 0.001) and gonorrhoea (7.7%, 95% CI: 4.0–14%, p < 0.001) based on five and seven studies, respectively. The observed prevalence among FSWs (5.5% and 7.6%) was lower compared to the weighted prevalence among women recruited at PHC settings for chlamydial infection (p = 0.004) but higher for gonorrhoea (p < 0.001) and higher compared to women recruited in the community for both chlamydial infection and gonorrhoea (p < 0.001).
Incidence of C. trachomatis and N. gonorrhoeae infections
Seven studies reported on incidence estimates of C. trachomatis or N. gonorrhoeae infections in sub-Saharan Africa between 2005 and 2014 (Table 3). The highest incidences of chlamydial infection (range, 0.75–28/100 person-years at risk [PYAR]) and gonorrhoea (range, 2.8–17/100 PYAR) were observed in South Africa among a family planning clinic in 2007 and among the general community in 2009, respectively.
Factors associated with prevalence of infection at population level
We used linear regression to compare all studies (n = 75) reporting on prevalence of both genital C. trachomatis and N. gonorrhoeae detected by NAAT and observed a relation (p < 0.0001, R2=0.23) between the prevalences of these two infections in sub-Saharan Africa.
Mean age of participants in studies was not associated with C. trachomatis (p = 0.69) and N. gonorrhoeae (NAAT-based, p = 0.99) infection.
A higher HDI index was associated (p = 0.035, R2=0.41) with higher prevalence of C. trachomatis infection and borderline (p = 0.078, R2=0.31) with higher prevalence of N. gonorrhoeae infection among women recruited at community level per country, but not associated with women recruited at PHC settings. After stratification for setting; we observed no association in the rural setting for HDI index with C. trachomatis (p = 0.51) and N. gonorrhoeae (p = 0.75) infection, but an association in the urban setting for both chlamydial infection (p = 0.027; R2=0.58) and gonorrhoea (p = 0.018; R2=0.64) with higher HDI was observed among the community-based studies.
We did not observe an association of genital C. trachomatis infection and HIV prevalence as reported in the different studies (n = 44, p = 0.70), but we did observe an association of N. gonorrhoeae infection (detected by NAAT) with reported HIV prevalence (n = 40, p < 0.0001, R2=0.38).
There was no relation of HIV prevalence estimates among adults (reported by UNAIDS) with prevalence of C. trachomatis and N. gonorrhoeae at community level and at PHC settings per country. Furthermore, there was no association of HIV prevalence estimates among FSWs (reported by UNAIDS) with C. trachomatis and N. gonorrhoeae infection.
Oral and anal infections
Two studies reported on anal infections among African women. Rutherford et al. 67 observed of 0% prevalence for anorectal chlamydial infection and 0.45% for anorectal gonorrhoea (detected by PCR) among 280 women in Uganda. No data were reported on receptive anal intercourse (RAI) and fellatio in this study. A study from South Africa showed prevalences of 7.1% and 0.2%, and 2.5% and 0% for anorectal and oropharyngeal Chlamydia and gonorrhoea (detected by PCR), respectively, among 604 women. RAI was reported by 26 of these women (4.6%), and fellatio by 80 women (14%). Neither practice was associated with genital or rectal infection in that study.
Discussion
This review summarizes data from 102 studies reporting on the epidemiology of C. trachomatis and N. gonorrhoeae in women, in diverse settings and populations, in sub-Saharan Africa from 2005 to 2014. These studies were all conducted in countries with a moderate to high HIV prevalence and show that these bacterial STIs are common among women.
We observed a considerable difference in the number of studies conducted in each sub-Saharan country with the majority of studies conducted in South Africa (18%), Tanzania (17%) and Kenya (12%). Furthermore, the publications that we identified only represented approximately half of all sub-Saharan African countries; there were no data points for a considerable number of countries. The limited attention paid to the epidemiology of chlamydial infection and gonorrhoea in sub-Saharan African countries is further reflected by a total of only seven studies reporting on incidence estimates of C. trachomatis or N. gonorrhoeae infections between 2005 and 2014. However, although we included several databases in this analysis, we cannot rule out existence of (unpublished) reports on STI prevalence or incidence.
The weighted prevalence of chlamydial infection and gonorrhoea for women recruited in their community (3.9% and 2.2%) is in line with the WHO 2005 estimates (3.9% and 2.1%) published in 2008 based on modelling, although prevalence varied noticeably among sub-Saharan African countries. The subsequent WHO 2008 estimates published in 2012 for C. trachomatis infection are lower (2.6%) than observed in our study, but in a similar range for N. gonorrhoeae (2.3%).1,138 The most recent WHO estimates published in 2015 are similar for chlamydia (3.7%), but lower for gonorrhoea (1.7%). 139 However, we observed an higher weighted prevalence among women recruited at PHC settings in sub-Saharan Africa (6.3% and 4.3%) as compared to WHO estimates and results from community-based studies. There could be several reasons for this observed difference. First, publication bias might have occurred as studies that observe relatively high prevalence are more likely to be published, contributing to a higher prevalence in our analysis. Second, the WHO uses case-reporting surveillance systems in many countries which might underestimate the burden of asymptomatic infections. Although the WHO estimates are adjusted for unreported and undiagnosed cases, the question remains to what extent it should be adjusted, especially in case of C. trachomatis infections. Third, women with symptomatic STIs may be more likely to visit healthcare facilities for care than those without symptoms. Finally, our analyses included studies until 2014 whereas the estimates of the WHO are calculated over an earlier reference period.
Surprisingly, we observed a lower prevalence (5.5%) of C. trachomatis infection among FSWs and a higher prevalence of N. gonorrhoeae (7.6%) as compared to women recruited at PHC settings, but similar to women in community-based studies. Successful prevention programmes aimed at this specific population have been reported in some countries, including Ghana and Benin, resulting in decreased prevalence of these bacterial STIs.109,140 On the other hand, selection bias may have played a role in these studies. Sex workers constitute a key population and it may not be easy to recruit self-identified sex workers into a research study. It is not unthinkable that sex workers engaging in the highest risk behaviour for contracting STIs were not included in these studies.
The prevalence of C. trachomatis was higher, but associated with increased N. gonorrhoeae prevalence in all studies. The WHO prevalence estimates also suggest higher C. trachomatis infection in both 2005 and 2008, although chlamydial infection is suggested to show a decreasing trend over time while gonorrhoea is increasing. The strong associations observed in our analysis could contribute to better surveillance as it could facilitate prediction of burden of both STIs in settings where only one of these infections can be measured.
N. gonorrhoeae prevalence was associated with a higher HIV prevalence among women overall in studies included in our analysis, but for C. trachomatis we did not observe this relationship. Furthermore, at country-level, neither infection was associated with HIV prevalence as reported by UNAIDS (for adults) among women recruited at the diverse settings. Although it is biologically plausible that both infections enhance HIV acquisition and transmission there are several reasons that could explain the observed lack of association. First, the data retrieved from studies are fairly heterogeneous as study population (and size), country and location varied, which could have weakened the relation. Second, we used most recent UNAIDS HIV estimates while study year of many studies was prior to this date. Third, successful HIV prevention programmes have succeeded in decreasing the prevalence of C. trachomatis and N. gonorrhoeae.109,140 A last important reason could be the potential difference in timeline as one could have become infected with HIV years ago and have recently become infected or reinfected with C. trachomatis or N. gonorrhoeae.
Prevalence of chlamydial infection and gonorrhoea at community level was higher in sub-Saharan African countries with relatively higher reported HDI (by UNDP). We did not observe the same association for studies of women recruited in PHC settings. Despite the fact that poverty is associated with increased vulnerability for STIs in general, the observation may also suggest that sexual risk behaviour may be higher in areas in Africa of relatively higher socio-economic status, for example through increased alcohol use. Another explanation could be that these results are reflecting that countries with higher HDI (e.g. South Africa) have better resources to educate women at risk for STIs at the community level and mobilize women with symptoms or as part of partner notification to be tested. On the other hand, exposure to specific public health programmes may possibly have affected this association, for example mass treatment of trachoma in some of the countries ranking relatively low on HDI.
There are very limited data on oral and anal infections in African women; only one study observed considerable anorectal prevalence of C. trachomatis and N. gonorrhoeae among women visiting a PHC clinic. Recent studies from Europe show treatment of anal C. trachomatis and N. gonorrhoeae in women will likely reduce transmission of these STIs.141,142 As there are limited data available, more research is warranted to determine the role and burden of these infections in sub-Saharan Africa.
In line with literature we observed higher prevalence of N. gonorrhoeae among women recruited at PHC settings by using NAAT as the detection method compared to culture. This may be explained by logistic and operational challenges in culturing N. gonorrhoeae, the bacterial frailty and the known higher sensitivity of molecular assays.143–145 This observation has implications for STI control programmes in these settings. Given lower performance of culture compared to molecular techniques, studies and health policies using culture are likely to underestimate the burden of STIs.
This study has several limitations. First, there was considerable heterogeneity of publications included in this analysis. Study design, sample size, sampling strategy, laboratory method and specimen type used varied substantially across the included studies. Each of these studies has its own limitations and risk of bias; the sampling strategy (e.g. convenience sampling) used in some studies may have accounted for some of the outliers. By using clear inclusion criteria and calculating prevalence estimates per population group we tried to limit this limitation. However, heterogeneity of studies should be taken into account when interpreting our results. A second limitation was the availability of studies per country within sub-Saharan Africa as only half of the countries had one or more studies available. Local variations in sexual behaviour might result in differences between countries in sub-Saharan Africa that could not be identified due to a limited number of countries with sufficient data. Third, we did not include conference abstracts and grey literature in this evaluation which may have affected the breadth of our search. Also, our search may have missed a few studies with STI data embedded as part of a different objective, e.g. HIV clinical trial, neither can we rule out the existence of unpublished country-level data. A further possible limitation is that settings where chlamydial infection and gonorrhoea are regarded as public health concerns, and thus more effectively integrated in healthcare provision, are potentially more likely to be targeted by epidemiological studies. Likewise, more studies were conducted in urban than in rural settings. Finally, publication bias may have occurred in favour of high-prevalence studies resulting in an overestimation of weighted prevalence in our analysis
The WHO states that an important obstacle to provision of services for control of STIs at the decision-making level is that policy-makers give low priority to control of STIs, which is potentially aggravated by the stigmatization and prejudice associated with these infections and limited awareness of the importance of their impact on health and economic development. 146 Although STIs other than HIV are not named in either the Millennium Development Goals or the new Sustainable Development Goals, they have important global health priorities on their own, but their impact is unrecognized. 147
The Disease Control Priorities Project (DCPP) considered the diagnosis and treatment of STIs as a neglected low-cost opportunity to improve health in sub-Saharan Africa. 148 However, many countries fail to provide suitable education and services to populations at risk for STIs. 146 In order to overcome these obstacles enhanced surveillance of STIs is required in sub-Saharan Africa in order to stronger advocate the importance of STI control and facilitate the integration of STI control measures in existing reproductive health programmes.
Brief conclusions
C. trachomatis and N. gonorrhoeae constitute a major public health problem among women, but the burden of infection in sub-Saharan Africa is poorly documented. Our overview underlines a relevant prevalence of genital C. trachomatis and N. gonorrhoeae in women in diverse settings in sub-Saharan Africa with geographic differences. Only a few studies reported on oral and anal infections. Enhanced surveillance of STIs is required and better control strategies are warranted to reduce the burden of infection and prevent long-term complications of these infections.
Supplemental Material
Supplemental material for Genital Chlamydia trachomatis and Neisseria gonorrhoeae infections among women in sub-Saharan Africa: A structured review
Supplemental material for Genital Chlamydia trachomatis and Neisseria gonorrhoeae infections among women in sub-Saharan Africa: A structured review by Jan Henk Dubbink,Stephan P Verweij,Helen E Struthers,Sander Ouburg,James A McIntyre,Servaas A Morré andRemco PH Peters in International Journal of STD & AIDS
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.