
Abstract
The purpose of this study was to characterise the prevalence and risk factors associated with genital mycoplasmas (Mycoplasma hominis [MH], M. genitalium [MG]) and ureaplasmas (Ureaplasma urealyticum [UU], U. parvum [UP]) in Portuguese women of reproductive age. The cross-sectional study included 612 cervicovaginal self-collected samples from women aged 15–44 years, tested for MH, MG, UU, UP by polymerase chain reaction. Y chromosome (Yc) DNA was detected as a biomarker of recent unprotected sexual intercourse. The prevalences of UU, UP, MH and MG were 28.4% (95% confidence interval [CI] 25.0–32.1), 22.4% (95% CI 19.3–25.9), 8.5% (95% CI 6.5–11.0) and 0.8% (95% CI 0.4–1.9), respectively. Overall, women aged 20–29 years (odds ratio [OR] 1.78; P = 0.010) and the presence of Yc-DNA (OR 2.33; P = 0.038) were associated with an increased risk of UU. Lifetime number of sexual partners was a predictor of UU, UP and MH (OR 2.46; P < 0.001, OR 2.78; P < 0.001 and OR 1.55; P < 0.001, respectively, for more than one versus one partner). The prevalence of MG was low, while UU, UP and MH were common in Portuguese women of reproductive age. The presence of UU, UP and MH was associated with sexual activity (number of sexual partners), although the consequences of its prevalence are not fully understood and should be further investigated.
Introduction
Most sexually active individuals acquire a sexually transmitted infection (STI) at least once in their lives, being involved in the epidemiological chain of infection. 1 Since the majority of STIs are asymptomatic, the identification of urogenital microorganisms associated with a variety of adverse reproductive and neonatal outcomes could be of emerging significance on health.2,3 It is noteworthy the role of genital mycoplasmas and ureaplasmas, which has been a contentious research topic over the past two decades. 3
Genital mycoplasmas and ureaplasmas belong to the Mycoplasmataceae family and Mollicutes class.4,5 They represent a group of atypical wall-less bacteria and are the smallest self-replicating organisms, both in genome size and cellular dimensions.4,5 The introduction of nucleic acid amplification tests (NAATs) has improved the knowledge regarding the epidemiology of these microorganisms and allowed to distinguish between species.3,6 As a result of sexual intercourse, genital mycoplasmas and ureaplasmas can be isolated from the genitourinary tract of both males and females. 7
Genital mycoplasmas and ureaplasmas (UU, UP and MH) have been associated with some symptomatic and asymptomatic genital tract conditions, including cervicitis, bacterial vaginosis (BV) and endometritis. Cervicitis, an acute or chronic inflammation of the uterine cervix, may promote the infection by human immunodeficiency virus and other STIs, including human papillomavirus, by the disruption of epithelial barrier integrity, and subsequent recruitment of inflammatory cells.8–11 They may cause pelvic inflammatory disease, resulting in damage to the fallopian tubes, which may lead to ectopic pregnancy and infertility.12–14 Additionally, there is growing evidence that genital mycoplasma species could contribute to different pregnancy outcomes, including preterm birth and neonatal morbidities.12,15,16 However, it is still under discussion whether UU, UP and MH should be considered pathogens, opportunistic or co-factors associated with genital infections.3,7 Some reports described UU, UP and MH as commensal inhabitants, while others found an association with pathological conditions. 3 Nevertheless, MG is the cause of an emerging STI, with emerging antibiotic resistance. 17 The inconsistent findings could be related to the study design and population, the outcome, the sampling site and device, and the sensitivity and specificity of the detection method (culture or polymerase chain reaction [PCR]). 18
Data regarding the prevalence of genital mycoplasmas and ureaplasmas in the Portuguese population are limited. 19 Considering the impact these microorganisms, infection or colonisation may have on female reproductive health, and the high number of unrecognised infected or colonised individuals, which may function as reservoirs for spreading the infection to other women and men,2,20,21 we must highlight emergent knowledge of the prevalence of genital mycoplasmas and ureaplasmas. Thus, the purpose of this study was to assess the prevalence of UU, UP, MH and MG in Portuguese women of reproductive age and their association with demographic, behavioural data and potential risk factors, using a cervicovaginal self-sampling method.
Material and methods
Study population, data collection and ethics statement
This cross-sectional study included 612 Portuguese women of reproductive age (15–44 years). Samples were collected between March 2010 and July 2014. The study was conducted according to the principles of the Helsinki Declaration and approved by the Ethics Committee of University Fernando Pessoa. All participants were volunteers and invited to participate in the study through educational presentations on STIs, with no money or other compensation involved. Written informed consent was obtained from all study participants. Women completed anonymous questionnaires on sociodemographic and behavioural data for epidemiological characterisation. Sexually-active women aged 15–44 years, who were not pregnant, and reported no recent or current vaginal bleeding were eligible for inclusion.
Sample collection and DNA isolation
The cervicovaginal cells were collected by self-sampling using the commercial kit DNA Pap™ Cervical sampler™ (QIAGEN®, Hilden, Germany). Sample processing included the cellular fraction concentration by centrifugation, followed by DNA extraction using the QIAamp DNA Blood Mini Kit (QIAGEN®), following the manufacturer’s instructions. To check the integrity of the DNA extracted from the specimens, a region of 175 base pairs of the cellular beta-globin gene (PCO3/BGII primers, Metabion®) was amplified, as reported in our previous research work. 22
Detection of genital mycoplasmas, ureaplasmas and Y chromosome (Yc)-DNA
PCR amplifications were carried out individually with 1 × PCR buffer, 0.3 µM of each previously described specific primers (MgPa1/MgPa3, 23 RNAH1/RNAH2, 24 UMS57/UMA222 25 and U4/U5, 26 Metabion®), 2.5 mM MgCl2, 0.20 mM deoxynucleotide triphosphates, 1 unit Taq polymerase (KapaTaq, KapaBiosystems®) and 50–100 ng DNA template. Yc PCR amplification was carried out, as previously described by Silva et al. 22 Clinical isolates of MH, MG, UP and UU were used as positive controls. DNA of male blood donors was used as a Yc-positive control. A negative control containing all PCR reagents, except DNA, was added to monitor contamination.
Statistical analysis
Data analysis was performed by the computer software IBM®SPSS® Statistics for Windows (Version 23.0) and GraphPad Prism® (Version 6). To explore the association between age and overall genital mycoplasma and ureaplasma prevalence, age was categorised as previously described. 22 Behavioural variables (age at first sexual intercourse, time after first sexual intercourse, lifetime number of sexual partners and contraceptive use) of participants were also characterised. The mean of years after first sexual intercourse was computed from the difference between the age and the age of first intercourse. Yc-DNA detection was introduced as a measure of recent unprotected intercourse (detectable up to five days after unprotected intercourse).22,27 Chi square and Fisher’s exact tests were used to compare categorical variables, using a 5% level of significance. The univariate analysis was used to estimate the odds ratio (OR) and 95% confidence interval (95% CI) as a measure of association between the explanatory variables. The multivariate logistic analysis was performed considering the variables demonstrating statistical significance in the univariate analysis.
Results
The prevalences of UU, UP, MH and MG were 28.4% (95% CI 25.0–32.1), 22.4% (95% CI 19.3–25.9), 8.5% (95% CI 6.5–11.0) and 0.8% (95% CI 0.4–1.9), respectively (Figure 1). Of 612 women, 35.8% (95% CI 32.1–39.7) were positive for at least one of the genital mycoplasmas and ureaplasmas (data not shown). Two or more of these agents were detected in 5.9% of women (95% CI 4.3–8.0); the concomitant presence of UU and UP was observed in 18.0% (95% CI 15.1–21.2); UU, UP and MH in 3.1% (95% CI 2.0–4.8) and MH and MG in 0.2% (95% CI 0.03–0.9) (Figure 1).
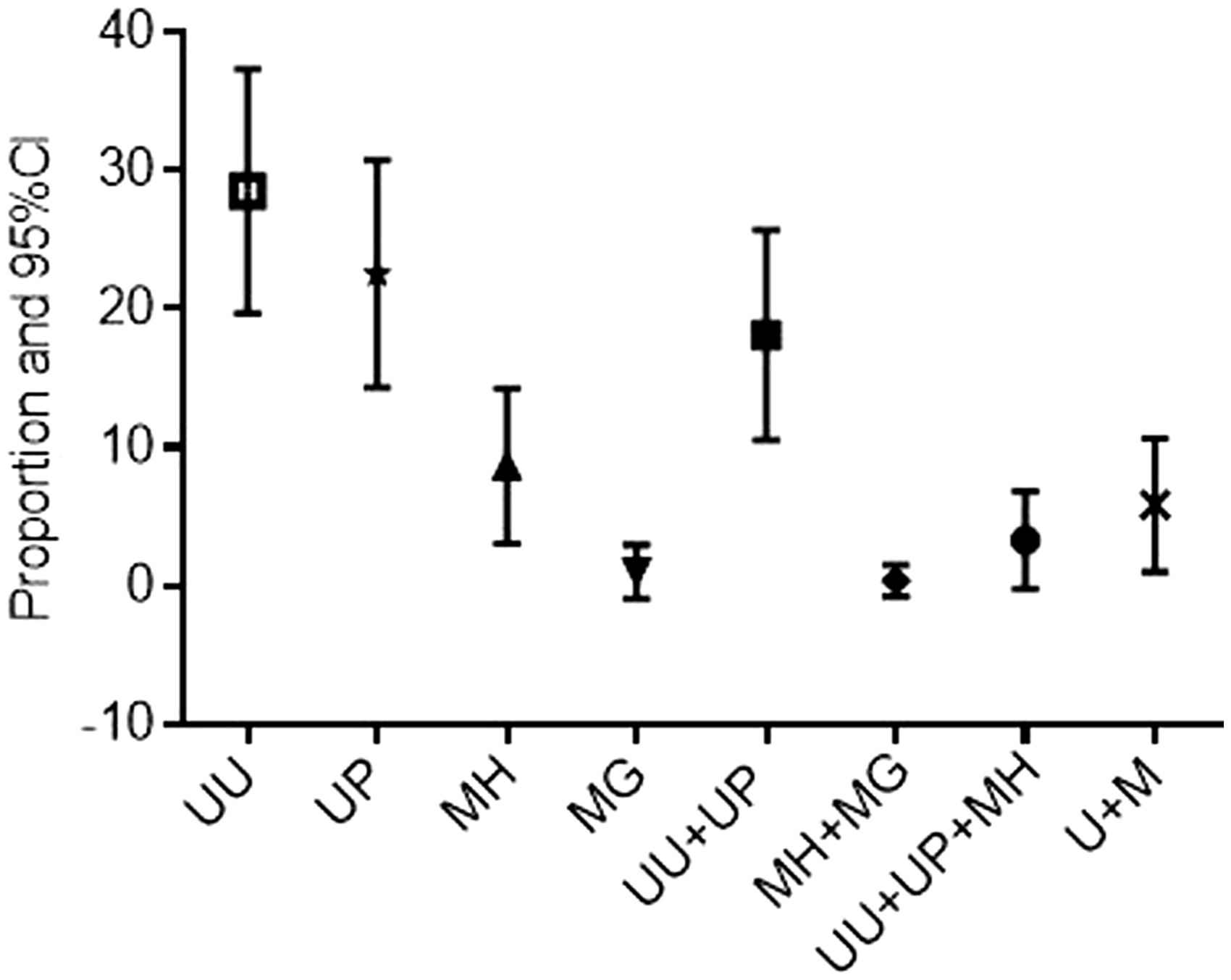
Prevalences and 95% CIs of UU, UP, MH, MG and simultaneous presence of ureaplasmas and mycoplasmas. M: mycoplasmas; MG: M. genitalium; MH: Mycoplasma hominis; U: ureaplasmas; UP: U. parvum; UU: Ureaplasma urealyticum.
Figure 2 shows the age-specific prevalence for genital mycoplasmas and ureaplasmas. UU, UP and MH prevalence was highest in women aged 25–29 years, whereas MG peaked in younger women (18–19 years). The total number of UU (n = 174), UP (n = 137), MH (n = 52) and MG (n = 5) positive samples in each age group was calculated as a percentage considering the total number of women in the study population (n = 612), stratified into groups aged 15–17 years (n = 224), 18–19 years (n = 125), 20–24 years (n = 137), 25–29 years (n = 43), 30–34 years (n = 34) and 35–44 years (n = 49).
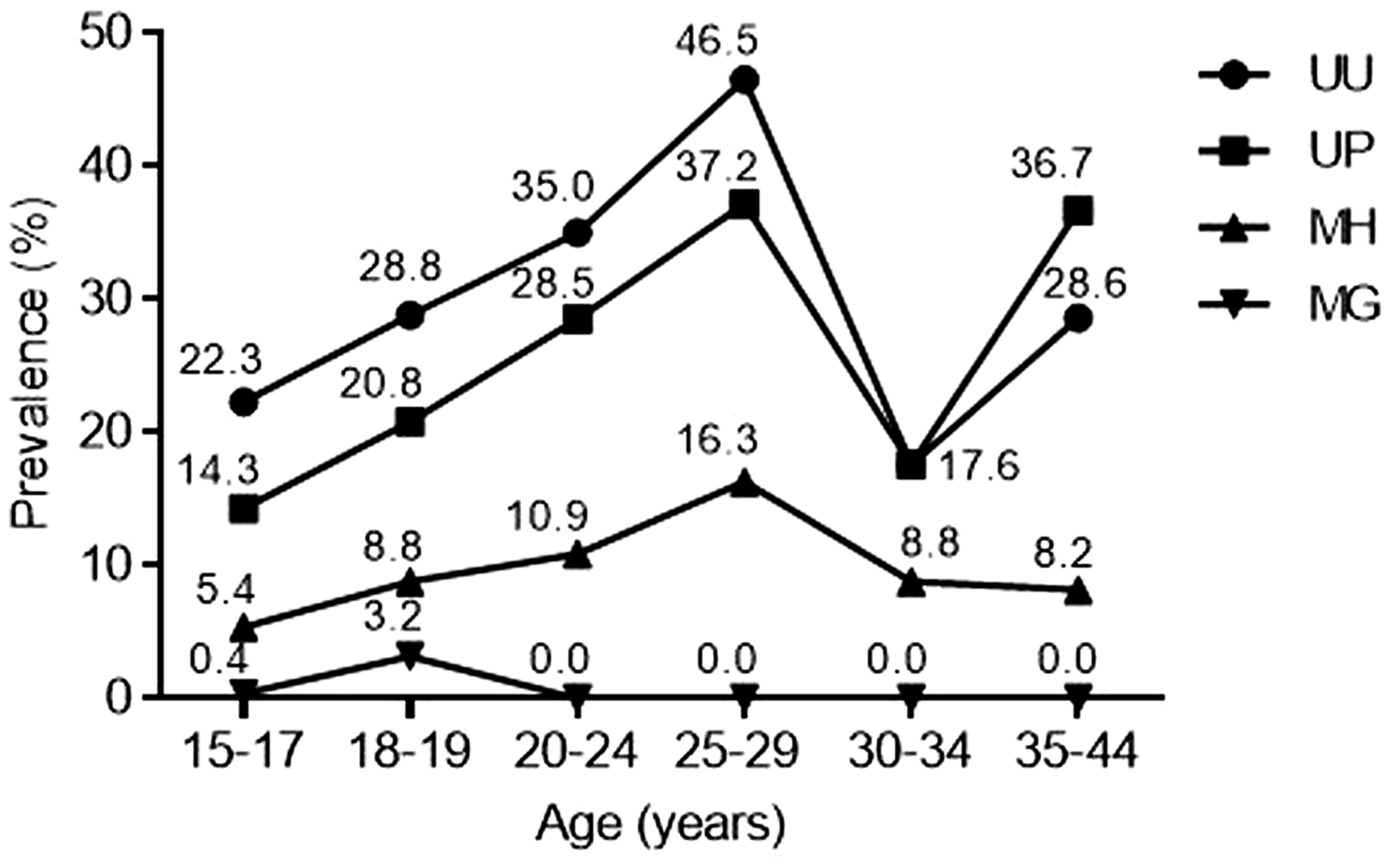
Age-stratified prevalences of Ureaplasma urealyticum (UU), Ureaplasma parvum (UP), Mycoplasma hominis (MH) and Mycoplasma genitalium (MG).
Demographic and behavioural variables of the study population were stratified by the presence of UU, UP, MH, MG and are shown in Table 1. The mean age was 20.4 ± 6.88 years (15–44 years), and the mean age at first sexual intercourse was 17.6 ± 2.74 years. The mean number of years after the first sexual intercourse was 5.4 ± 5.82 years. Overall, women aged 20–29 years (Figure 2), of younger age at first sexual intercourse (15–18 years), reporting more than one sexual partner, using oral contraceptives, condom users and those with detectable Yc-DNA had the highest prevalences of UU, UP and MH. Contrarily, MG was not identified in Yc-DNA-positive samples (Table 1). The analysis of UU, UP and MH prevalences was performed excluding the Yc-DNA-positive samples (n = 30) and the prevalences of UU, UP and MH were 27.3, 21.3 and 8.2%, respectively. We observed that 8.6, 9.4 and 7.7% of UU, UP and MH detections were attributable to recent unprotected intercourse (last five days). The simultaneous presence of UU and UP, ureaplasmas and MH, and any ureaplasma or mycoplasma was higher in women who reported more than one lifetime sexual partner (31.0, 7.1 and 10.7%, respectively) (data not shown).
Characterisation of UU, UP, MH, MG prevalences according to the study group characteristics of reproductive-age women.
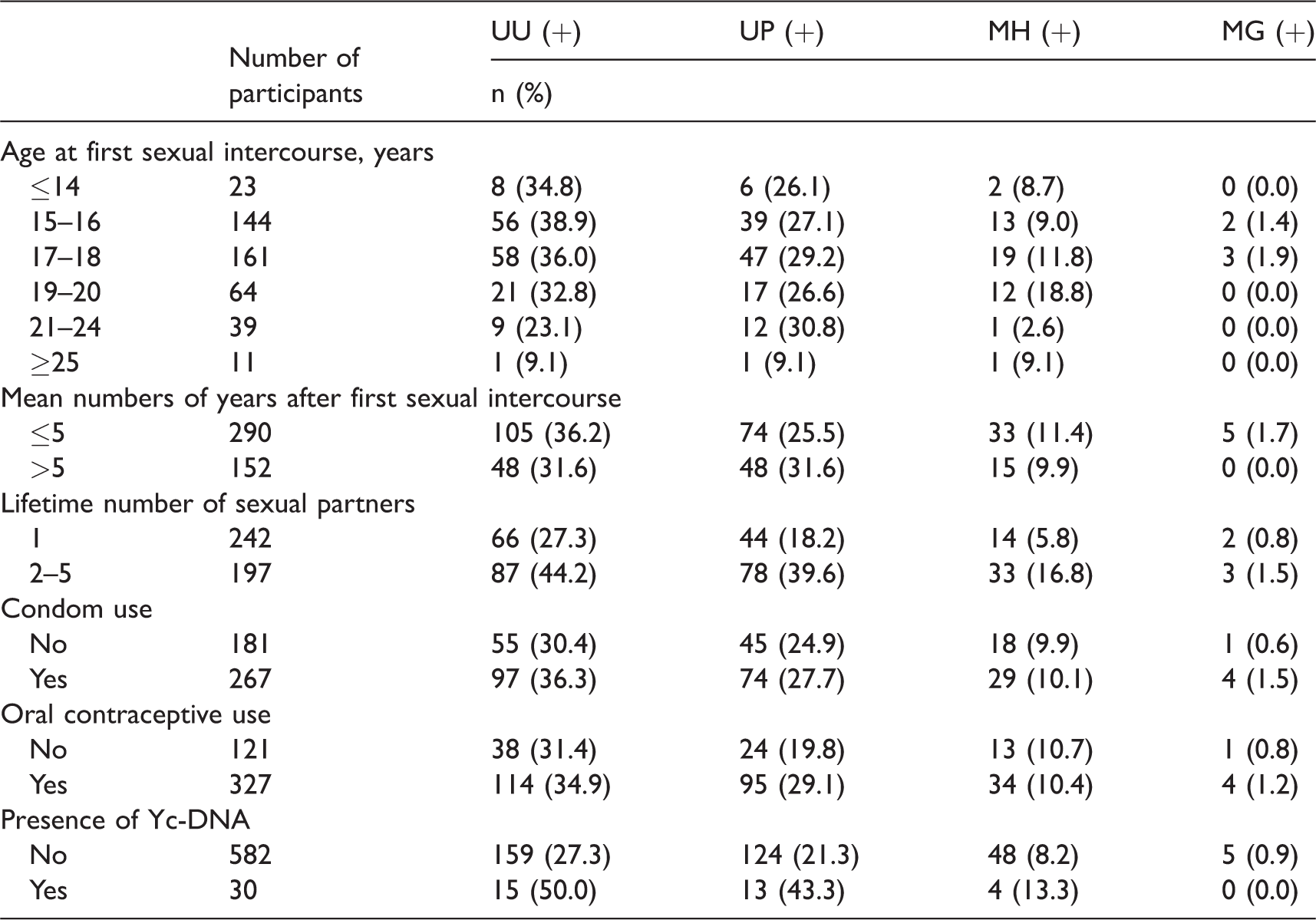
MG: M. genitalium; MH: Mycoplasma hominis; UU: Ureaplasma urealyticum; UP: U. parvum; Yc-DNA: Y chromosome DNA; (+): positive.
Considering UU, UP, MH and MG-positive samples, 96.4, 95.5, 96.1 and 100.0%, respectively, were related to women reporting no history of STIs (data not shown). In the total population (N = 612), 95.1% confirmed no history of STIs.
In univariate analysis, UU was significantly associated with women aged 20–24 years (OR 1.88, 95% CI 1.17–3.01; P = 0.008) and 25–29 years (OR 3.03, 95% CI 1.54–5.95; P < 0.001) and having more than one lifetime sexual partner (OR 2.11, 95% CI 1.42–3.14; P < 0.001). The following factors were associated with UP: age of 20–24 years (OR 2.39, 95% CI 1.41–4.04; P = 0.001), 25–29 years (OR 3.56, 95% CI 1.73–7.32; P < 0.001) and 35–44 years (OR 3.49, 95% CI 1.75–6.96; P < 0.001), and having more than one lifetime sexual partner (OR 2.95, 95% CI 1.91–4.55; P < 0.001). MH was significantly associated with being 25–29 years old (OR 3.44, 95% CI 1.27–9.31; P = 0.011) and having more than one lifetime sexual partner (OR 3.28, 95% CI 1.70–6.32; P < 0.001). An association was also found between Yc-DNA and ureaplasmas (UU: OR 2.66, 95% CI 1.27–5.57; P = 0.007 and UP: OR 2.82, 95% CI 1.34–5.97; P = 0.005). UU, UP and MH were not statistically associated with age at first sexual intercourse and the contraceptive type (oral contraceptives or condom use). Because of the low prevalence of MG, the analysis was not performed.
Variables demonstrating statistical significance in the univariate analysis were entered in sequence into the multivariate analysis. The association between UU and women aged 20–29 years (OR 1.78, 95% CI 1.15–2.76; P = 0.010), having more than one sexual partner (OR 2.46, 95% CI 1.60–3.78; P < 0.001) and Yc-DNA (OR 2.33, 95% CI 1.05–5.17; P = 0.038) remained statistically significant in the multivariate analysis. Also, the association between UP, MH and having more than one sexual partner (OR 2.78, 95% CI 1.77–4.37; P < 0.001 and OR 1.55, 95% CI 1.79–7.06; P < 0.001, respectively) remained significant.
Discussion
The vaginal microbiome contains a multitude of microbial species, including genital mycoplasmas and ureaplasmas.3,18 Studies on the prevalence of genital mycoplasmas and ureaplasmas are limited, which could be related to the controversy of infection or colonisation by these microorganisms. 20 To the best of our knowledge, we report for the first time the prevalence of genital mycoplasmas and ureaplasmas in Portuguese women of reproductive age, using a cervicovaginal self-sampling method.
Considering genital colonisation as a source of these microorganisms, genital ureaplasmas may be detected in the cervical or vaginal samples of 40–80% of sexually mature and asymptomatic women, MH in 20–50% and MG in 0–5%, 3 although some heterogeneity results from the detection method, i.e. culture or NAATs. The prevalences of MG and MH found in our study were similar to other studies.28–33 In young women, the prevalence of MG infection has been estimated to be 1% and is between that of Neisseria gonorrhoeae and Chlamydia trachomatis infections. 34 Prevalence of UP was lower, and in contrary, prevalence of UU was higher, than that reported by other authors.12,31,33,35 Nevertheless, we should take into account the highly variable sensitivity of detection assays (even considering NAATs), the sampling method and the number of participants, which may also vary across the studies.
The prevalence of UU, UP and MH increased with age, mainly in the 20–24 and 25–29 age groups, whereas the highest MG prevalence was observed in younger women (18–19 years) as previously reported.30,31,35,36 Furthermore, we observed a second peak of UU and UP prevalence in women aged 35–44 years. These results might be multifactorial, resulting from cohort effect (small group size), the interplay of sexual behaviour during the middle age (both for men and women), hormonal contraceptive use, and the rate of BV, among others.37,38
The results of this study agree with those reported by other authors, considering the number of sexual partners.3,30,39 In our study, more than two sexual partners were reported by 51.2 and 79.1% of women in the age groups 20–24 and 25–29 years, respectively, and among women with more than five years of sexual activity (65.8%) (data not shown). These results are supported by the highest prevalences of UU, UP and MH being found in the same age groups. After puberty, colonisation with MH and ureaplasmas occurs from sexual contact7,40 and colonisation increases with the number of different sexual partners. 41 Sexually-mature individuals without sexual contact are infrequently colonised. 3 Moreover, it has been suggested that the prevalence of an STI increases by 10% with each additional sexual partner.20,21
In the study setting, the type of contraception (condoms or oral contraceptives) use was not related to any of the detected mycoplasmas or ureaplasmas, although nearly 60% of women, mainly in the age group 20–29 years, reported the use of condoms. These results could be linked to the inconsistent or non-use of condoms, measured by self-reports, which are susceptible to under- or over-reporting bias.42,43 Additionally, women reporting the use of condoms may not be aware of their correct use, with impact on reproductive health, thereby enhancing the probability of transmission of STIs to susceptible partner(s).42,43 Consistent use of condoms was not related to the infection and/or colonisation by genital microorganisms. The interchange of microorganisms from a woman’s vagina, oral and rectal microorganisms between partners and partner’s sexual contact(s) is acknowledged as a normal process among sexually-active individuals. 44 On the other hand, condom and spermicides may be associated with vaginal flora shifts, and consequently, may predispose women to genital infections, decrease vaginal Lactobacillus and increase colonisation of other bacterial communities, 45 including UU, UP and MH, which may be considered a part of the BV spectrum.
The mean time after sexual intercourse was not related to any of genital mycoplasmas and ureaplasmas, suggesting that infection or colonisation does not depend on the timing of sexual activity. However, Yc-DNA detection was associated with ureaplasmas. This result may be related to recent/current sexual transmission of ureaplasmas, as cervicovaginal samples from women at high risk of STIs have frequently been found to contain traces of semen. 22 Our results also showed that 8.6, 9.4 and 7.7% of UU, UP and MH detections were found in women who recently had unprotected intercourse, respectively. A recent study by Malagon et al. 46 indicates that a substantial proportion of HPV DNA detections may be depositions due to recent unprotected intercourse since they found that 14.1% of HPV DNA detections in genital samples were owing to vaginal sex in the past seven days. The proportion of colonised women is greater than men, suggesting an increased female susceptibility. 3 Furthermore, males and females are colonised more frequently by ureaplasmas than MH. 3 Since most STIs in men are subclinical, they act as asymptomatic carriers and function as reservoirs and vectors. 47 Additionally, phages may potentially be introduced into a healthy vagina through sexual activity, causing lysis of the native Lactobacillus strains with consequently overgrowth of other bacteria, which may have a similar effect to BV, or ultimately, be one of the complex interactions of multiple factors which causes BV. 48 Yc DNA have been shown to be a valid semen biomarker in cervicovaginal samples. The protocol used in this study allows the detection of semen residues in the lower female genital tract for up to five days after sexual intercourse. 27 The detection of Yc-DNA in the cellular fraction of cervicovaginal secretions after unprotected penovaginal intercourse by PCR is both specific and sensitive. 27
Vaginal microbial communities undergo significant fluctuations at various stages in women’s lives (namely in birth, childhood, adolescence, reproductive age and menopause), directly linked to oestrogen levels. In women of reproductive age, the oestrogen cycling stimulates thickening of the vaginal epithelium, and the Lactobacillus-dominated vaginal microbiota maintains a low vaginal pH (<4.5). 49 Vaginal dysbiosis occasionally causes symptomatic conditions. 50 The most common and best studied clinical condition characterised by vaginal dysbiosis is BV, which is associated with almost non-existent vaginal inflammation. 50 Several studies have demonstrated that BV is accompanied by alterations in the vaginal microenvironment, high vaginal pH, decrease of Lactobacillus species and greater abundance of other bacterial communities (Gardnerella vaginalis, Prevotella spp., Mobiluncus spp., UU and MH), and fungi (Candida albicans).49,51–54
Molecular biological methods are promising tools to supersede conventional microbiological identification, 35 and have allowed for detection of a range of fastidious agents, whose aetiologic roles in genital infections need to be further investigated. 12 Moreover, we may consider the role of self-sampling as an alternative method to improve the detection of STIs,55,56 although dependent on the population’s knowledge about STIs. 57
Testing for genital mycoplasmas and ureaplasmas in reproductive-age women is important since these microorganisms, depending on circumstances, could be pathogenic. 2 MG is the cause of an emerging STI, which has been receiving increasing attention in recent years, in part by the recognition of its association with male and female reproductive tract disease syndromes, and also by the increasing spread of antibiotic resistance. 17 It is important to estimate, in reproductive-age women, the prevalence of genital mycoplasmas and ureaplasmas (i) to improve the efficacy of empirical treatment for genitourinary infections,12,28,35,51 and (ii) to avoid complications in pregnancy (including postpartum endometritis, preterm labour, premature rupture of membranes and neonatal infections).2,20,21
There are some limitations and risk of data bias in the present study. Information about recent antibiotic treatment was not addressed in the self-administered questionnaire, which may increase the risk of data bias in the prevalence of the detected ureaplasmas and mycoplasmas. However, in healthy women the bias is reduced as the use of antibiotics would be infrequent and limited to respiratory and urinary infections, mainly with beta-lactams, which are not effective against mycoplasmas and ureaplasmas. Reporting bias and validity estimation of self-reports is a major problem in sexual behaviour research. The variables ‘age at first sexual intercourse’, ‘lifetime number of sexual partners’, ‘condom use’ and ‘oral contraceptive use’ are related to aspects of sexual behaviour that women may feel sensitive about, or be uninformed about, and some participants may not answer these questions accurately. In reproductive-age women, the study of BV-associated species (by real-time PCR for quantification of the microorganisms involved) would help clarify whether or not UU, UP and MH may be considered STIs or a part of the BV spectrum.
Conclusion
Our results suggest that genital UU, UP and MH are common, whereas MG is rare in Portuguese women of reproductive age, particularly in women aged <30 years. Multiple sexual partners were associated with a high detection rate of UU, UP and MH, suggesting transmission by sexual contact. The presence of Yc-DNA was associated with the presence of UU. However, no statistical association was found between MG and sexual variables, which may be related to the sample size. Testing for genital infections in reproductive-age women is of great significance, to identify the simultaneous presence of different microorganisms and to inform appropriate management in specific situations (pregnancy). Further studies are needed for better clarification of the clinical significance of these microorganisms on acquisition of other STIs and their impact on obstetric outcomes.
Footnotes
Acknowledgements
The authors thank all the volunteer women who participated in this study. ALT is a postdoctoral fellow from FCT – Fundação para a Ciência e Tecnologia (SFRH/BPD/111114/2015). The authors are grateful to the Research Center of the Portuguese Oncology Institute of Porto (project no. PI86-CI-IPOP-66–2017).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Liga Portuguesa Contra o Cancro- Núcleo Regional do Norte (Portuguese League Against Cancer), FP-ENAS- CEBIMEB of University Fernando Pessoa, CNPq; FEDER funds through the Programa Operacional Factores de Competitividade-COMPETE and Portuguese funds through FCT – Fundação para a Ciência e a Tecnologia, under the project UID/Multi/04546/2013.