
Abstract
A 34-year-old man recently diagnosed with advanced human immunodeficiency virus infection (CD4 cell count of 139 cells/mm3), not yet started on antiretroviral medications, presented to hospital with a ten-day history of left leg weakness and difficulty walking. He described a childhood history of chickenpox with previous shingles over his buttock over three years ago. Examination revealed reduced power in the left hip and knee flexors and absent knee and adductor reflexes. Lumbar punctures were performed and polymerase chain reaction (PCR) detected varicella-zoster virus (VZV) DNA. Concurrent serum samples for VZV PCR were negative. The patient was diagnosed with VZV radiculopathy and treated with high-dose intravenous acyclovir. Within two days, neurological signs improved. Previous case reports define VZV radiculopathy by a temporal and geographical relationship with a zoster rash. Our diagnosis was based on a clinical picture of radiculopathy with virological evidence in CSF and confirmed by a dramatic clinical response to treatment. We propose that lumbar puncture and detection of VZV DNA by PCR in the cerebrospinal fluid (CSF) is an invaluable investigation that should be considered in the workup of immunosuppressed patients presenting with a radiculopathy.
Introduction
After primary infection, varicella-zoster virus (VZV) lies dormant in dorsal root ganglia with potential to reactivate in a variety of presentations, commonly as herpes zoster. VZV reactivations can manifest with non-dermatological presentations, including retinal necrosis, cerebellitis and zoster sine herpete. 1 VZV radiculopathy has been described in case series as weakness and sensory loss following a zoster rash in the corresponding dermatome.2–4 In untreated human immunodeficiency virus (HIV), VZV reactivation is common and can result in more severe and disseminated disease. 5 We present the first case report of VZV radiculopathy in HIV in the absence of a recent preceding zoster rash.
Case report
A 34-year-old man presented with a ten-day history of gradual onset of left leg weakness and bilateral thigh pain causing difficulty walking. He had no constitutional symptoms, sensory loss or recent zoster rash. His medical history included untreated HIV-1 (CD4 cell count of 139 cells/mm3 [14%] and HIV viral load 110,929 copies/ml) diagnosed after a pneumococcal pneumonia, untreated latent syphilis (rapid plasma reagin (RPR) 1:128), occult hepatitis B infection (Hepatitis B Virus (HBV)-DNA 37 IU/mL), granuloma annulare and tinea corporis affecting his trunk. He reported a childhood history of chicken pox and two episodes of zoster rash over the buttock over three years ago. He had sex with men and used drugs to enhance sex including intravenous crystal methamphetamine.
Examination disclosed a weak left leg, Medical Research Council (MRC) scale for muscle power was score 2 for hip flexion, 4 for knee flexion and 3 for knee extension. Knee and adductor reflexes were absent on the left. There was left thigh patchy non-dermatomal numbness. Magnetic resonance imaging (MRI) of the spine revealed leptomeningeal enhancement in the cauda equina and lower thoracic cord with no intrinsic spinal cord signal changes and no compression. Lumbar punctures were performed on admission days 2 and 3, both detected VZV DNA by PCR at a low cycle threshold (31) and both were heavily bloodstained (see Table 1 for results). VZV DNA PCR was not detected in either throat swab or plasma. Nerve conduction and electromyography were performed on day 2 of treatment, revealing no abnormality.
Cerebrospinal fluid results.
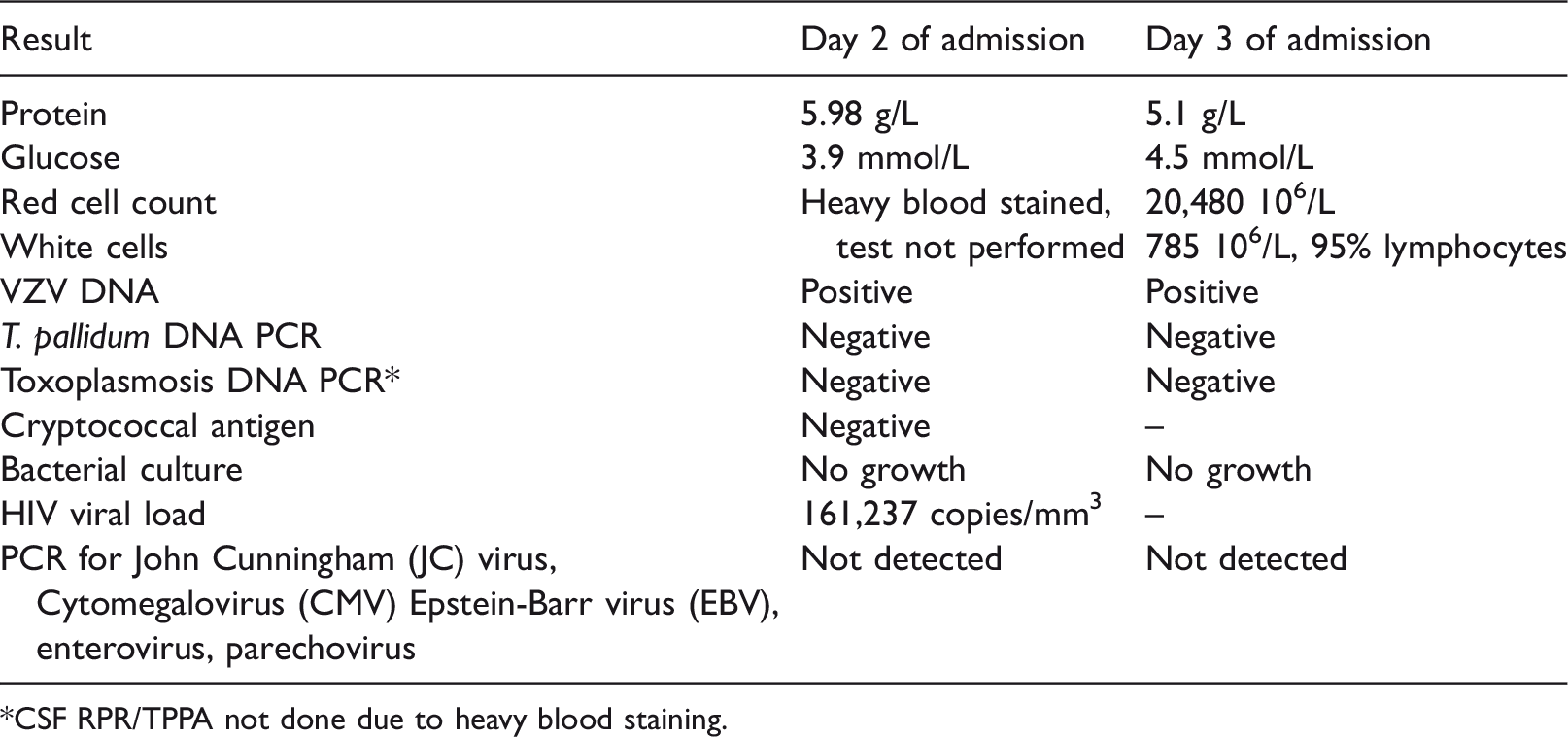
*CSF RPR/TPPA not done due to heavy blood staining.
The patient received intravenous acyclovir 10 mg/kg thrice daily for nine days, followed by one month of high-dose oral valaciclovir. On treatment day 2, there was significant improvement in muscle power from MRC grade 2 to 4. Owing to his history of untreated syphilis and neurological involvement, on day 6 of antiviral therapy he received empirical neurosyphilis treatment (14 days of intramuscular procaine penicillin); however, there was no evidence of Treponema pallidum DNA in CSF samples. Quantitative tests (RPR/Treponema pallidum particle agglutination assay [TPPA]) of the CSF were not analysed because the samples were blood stained.
Following discharge, the patient disengaged from care for five months. On re-attending, his neurological examination was normal (power MRC grade 5) and once daily he was prescribed prophylactic valaciclovir 500 mg OD, co-trimoxazole and initiated on a tenofovir-based antiretroviral therapy (ART) regimen.
Discussion
Previous case reports define VZV radiculopathy by temporal and geographical relationship with a zoster rash together with weakness and electrophysiological evidence.2–4,6 In contrast, we present a case of VZV radiculopathy based on clinical and virological findings. Perhaps in advanced HIV, VZV radiculopathy can present atypically with no preceding zoster rash. This situation has been reported in a patient with haematological malignancy. 7 In our case, electrophysiological testing was performed two days after commencement of acyclovir and subsequent clinical improvement probably accounts for the normal test result.
We report non-specific MRI findings of leptomeningeal enhancement. Previous case series of VZV paresis report a range of MRI findings including normality, increased nerve signal and hyperintensity in the dorsal horns, with nerve enlargement and enhancement being the most common findings.2–4
Our diagnosis was based on the clinical features of radiculopathy, virological evidence of VZV DNA replication within the CSF (in the absence of other pathogens) and dramatic clinical response to acyclovir (within 48 h). Although CSF samples were contaminated with blood, VZV DNA was not detected in plasma suggesting CSF VZV replication. VZV DNA PCR detection in CSF has excellent sensitivity and specificity to active infection8,9; however, this is not exclusive to VZV radiculopathy being commonly found in shingles. Guidelines on VZV CNS disease recommend intravenous acyclovir 10–15 mg/kg thrice daily for up to 14 days. This guidance is based on limited evidence and is not specific to an HIV-positive population. 10 We initiated acyclovir at the recommended intravenous dose for nine days and guided by the clinical response switched to high-dose oral valacyclovir for one month. As these agents are virostatic and require immunological control to suppress VZV, we continued a prophylactic dose until immune reconstruction was achieved with ART.
We report an atypical presentation of VZV radiculopathy in advanced HIV diagnosed by CSF viral PCR, with prompt and full recovery following antiviral therapy. We propose that lumbar puncture and CSF testing for VZV DNA by PCR is an invaluable investigation that should be considered when evaluating immunosuppressed patients presenting with radiculopathy.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.