
Abstract
Visceral leishmaniasis (VL) is a vector-borne disease caused by Leishmania donovani complex. Post-kala-azar dermal leishmaniasis (PKDL) is a rash that can occur following treatment for VL due to L. donovani species. We describe an unusual case of PKDL occurring during treatment for Leishmania infantum VL in a patient with human immunodeficiency virus-co infection.
Case
A 35-year-old man from Spain with no prior medical history was admitted with reduced consciousness in March 2018, and diagnosed with cerebral toxoplasmosis and human immunodeficiency virus-1 (HIV-1) (CD4 cell count 18 cells/µL and HIV-1 RNA 123,632 copies/mL). Toxoplasmosis treatment was initiated with sulfadiazine, pyrimethamine and folinic acid, and clinical response was confirmed on magnetic resonance imaging on day 14. Antiretroviral therapy (ART) with tenofovir disoproxil fumarate, emtricitabine and raltegravir was commenced on day 20 of his admission. A drug reaction on day 26 led to a switch of sulfadiazine to clindamycin and raltegravir to atazanavir/cobicistat. He was discharged on day 40 with a CD4 cell count of 81 cells/µL and HIV RNA of 21 copies/mL.
Six weeks later, he complained of weight loss, fevers and vomiting. Toxoplasmosis therapy at maintenance dose and ART was ongoing. A full blood count showed white cells of 0.9 × 109/L (neutrophils 0.3 × 109/L), haemoglobin 85 g/L and a normal platelet count. CRP was elevated at 65 mg/L, and CD4 cell count was 51 cells/µL. On examination, his temperature was 38.2°C, he was cachectic with palpable splenomegaly. A computed tomography (CT) scan of his abdomen showed a 16 cm splenomegaly and enlarged para-aortic lymph nodes. A CT-guided lymph node biopsy (Figure 1(a)) and bone marrow biopsy (Figure 1(b)) were performed, revealing Leishmania amastigotes on Giemsa stain, and a diagnosis of visceral leishmaniasis (VL) was made. Polymerase chain reaction (PCR) detected Leishmania donovani/infantum complex on the lymph node tissue.
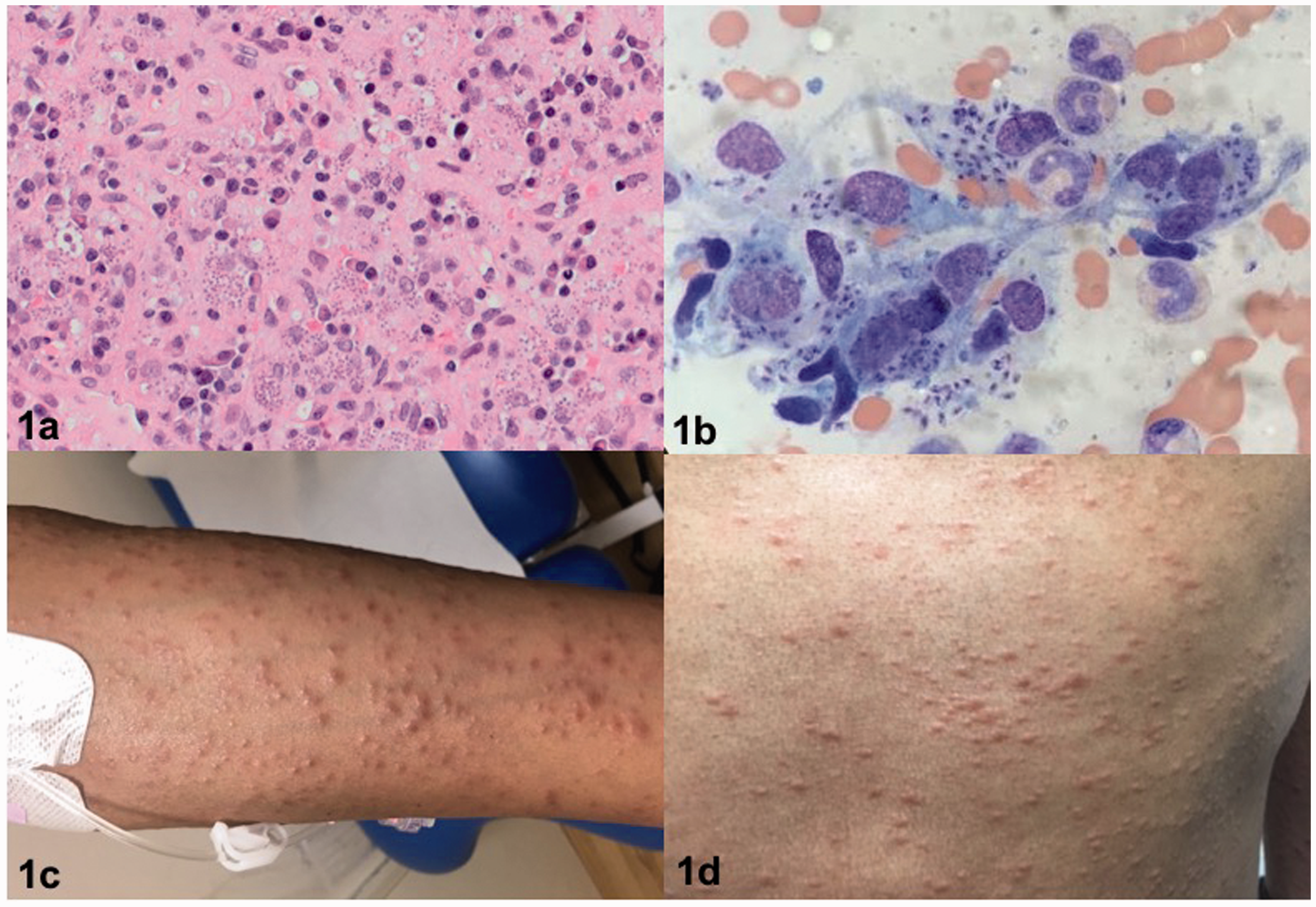
Lymph node biopsy (a) and bone marrow aspirate (b) showing histiocytes filled with Leishmania amastigotes. Patient presented with rash on arm (c) and torso (d).
He commenced 4 mg/kg of intravenous liposomal amphotericin B (LAB) for 10 doses (days 1–5, 10, 17, 24, 31 and 38) as per UK guidelines, 1 with rapid clinical recovery. However, on presentation for the sixth dose of LAB he had an asymptomatic papular rash over his torso, arms, thighs and face (Figure 1(c) and (d)), which progressed over the next week. A skin biopsy demonstrated dermal granulomas containing Leishmania amastigotes. Specialist opinion was that this rash would be consistent with post-kala-azar dermal leishmaniasis (PKDL). After 10 doses of LAB, the rash was persistent and CD4 cell count remained low (91 cells/µL). A decision was made to prolong LAB therapy, given on alternate weeks. After 16 doses of LAB, therapy was stopped due to a deterioration in renal function. Alternative therapy with miltefosine was considered, but repeat skin biopsy demonstrated no Leishmania amastigotes. Subsequently, he has remained well, and the rash has continued to improve at >6 months post LAB. His current CD4 cell count is 265 cells/µL with an undetectable HIV viral load.
Discussion
VL is a vector-borne disease caused by the protozoan L. donovani complex (L. infantum or L. donovani species). L. donovani VL typically occurs in South Asia and East Africa, whereas L. infantum VL typically occurs in the Mediterranean, the Middle East and Brazil. There is usually an insidious onset of symptoms including fever, weight loss and hepatosplenomegaly or splenomegaly which may be massive. PKDL is a rash which can occur following treatment for L. donovani VL. In Sudan, PKDL occurs shortly after treatment in up to 50–60% of patients, and in India it occurs months to years after VL in 5–10% of patients. 2
People living with HIV (PLWH) have an increased risk of VL, a poorer response to treatment and an increased risk of relapse.3,4 Most cases are caused by reactivation of a latent infection which manifests after immunosuppression, 5 although it has rarely been reported in association with immune reconstitution inflammatory syndrome (IRIS). 6 Signs and symptoms are similar to those in the immunocompetent host, but other organs not usually affected can be involved, including the lungs and gastrointestinal tract. 5
Skin lesions have been described in patients with HIV-VL co-infection, and Leishmania amastigotes have been detected in healthy looking skin. 7 There are few reports of PKDL with L. infantum in PLWH,8–10 and in some patients, PKDL can occur while the patient is still on treatment for VL; this is sometimes termed ‘para-kala-azar dermal leishmaniasis’. 11
The optimum management of VL with HIV co-infection is not known. The World Health Organization recommends LAB as first line at a dose of 40 mg/kg over 10 doses. 12 Combination therapy with miltefosine may be more efficacious but evidence is limited. 13 The risk of relapse is high before immune reconstitution is achieved, so some experts recommend secondary prophylaxis, although the duration of treatment, when this should be started and with which agents, is unclear. 14
There are limited data on the management of PKDL, particularly with HIV co-infection. 2 The penetration of anti-leishmanial drugs into the skin is uncertain, and parasites may persist despite appropriate treatment. This may be enhanced in PLWH, and skin lesions may act as a source for relapse. 11 It can also be difficult to measure response to treatment as the rash may persist beyond parasitological cure. 2
Conclusion
In this case, we suggest that VL developed as an unmasking IRIS phenomenon. The dermatological manifestation is very unusual, developing during VL treatment, and being caused by L. infantum species. There is little evidence on the most appropriate treatment in these patients. This patient responded well to a prolonged course of LAB, but the risk of relapse remains a possibility and we continue to monitor closely.
Footnotes
Acknowledgements
We would like to thank the patient for giving his consent for us to publish this case report and these images. We would also like to thank all members of staff involved in this patient’s care.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.