
Abstract
The objective of this study was to describe stakeholders’ perspectives on the acceptability of WeFLASH© (AADISS, Paris, France), a digital smartphone sexually transmitted infection (STI) patient notification (PN) tool to be launched among French HIV pre-exposure prophylaxis users (PrEPers). In Paris, Lyon, and Nice, we conducted 2-hour focus group discussions with PrEPers (n = 21) and community mediators (n = 10), and one-on-one interviews with PrEP-prescribing physicians (n = 5) and HIV/STI management decision-makers (n = 4). Recordings were transcribed. The analysis focused on perceived benefits and risks. Concerning benefits, participants mentioned that WeFLASH© could provide: improved PN and STI screening, by refining the notification of anonymous partners; customized linkage-to-care, by providing users with tailored information on care; and transferable epidemiological data, by filling a need for real-time data. Participants anticipated risks for: privacy and confidentiality and suggested specific security settings to protect users’ identity; sexual behavior and suggested game-like functions to improve the integration of the tool in sexual contexts; and fairness and emphasized the importance of making WeFLASH© accessible to all men who have sex with men. WeFLASH© could facilitate PN for an increasing proportion of anonymous partners met online, and empower users, including notified partners, on questions of confidentiality and consent, access to STI prevention and screening services, and access to data.
Introduction
HIV pre-exposure prophylaxis (PrEP) is mostly used by men who have sex with men (MSM). 1 Health authorities are seeking interventions to manage sexually transmitted infections (STIs) more efficiently2,3 as prevalence increases globally, including among PrEP users, or PrEPers.2,4,5 High STI prevalence among PrEPers is often attributed to higher numbers of sex partners and rates of condomless sex.6,7 Regular screening included in PrEP follow-up may also explain high rates, 8 and make PrEP a tool for STI prevention.4,8 In France, PrEP follow-up is often provided jointly by specialized physicians and community-based mediators attending to PrEPers’ needs for information, sexual health education, and other services, including STI screening every three months. 6
A potential, cost-effective 9 intervention is partner notification (PN), i.e., identifying, notifying, and treating STI patients’ partners3,10 to decrease the STI burden and risks of reinfection and forward transmission in sexual networks. 11 Different PN strategies exist that generally require index patients to know, reveal, or run the risk of exposing their partners’ identity (e.g., a parent finding a letter).3,12 PN indeed raises ethico-legal risks associated with privacy/confidentiality.
There is no single optimal PN strategy for all patients.13–15 Besides recent recommendations, 3 no guideline regulates PN in France as in other countries, like the USA and Canada. 3 In these countries, the necessity to notify partners prevails over medical secrecy although in practice, emphasis is put on index patients’ consent. 3 Few PN trials have been carried out and generally reveal important obstacles, like difficulties in partner identification and follow-up.13–15 For example, a study among Dutch MSM showed that 64% of partners at risk were “unnotifiable,” mainly due to the anonymity of sexual encounters. 16 In a study of a sample of French MSM who reported a past STI, 5 69% notified some of their partners. Among these, most (97%) did it by themselves, although some would prefer PN by a third party (e.g., a coach, care provider; 16%) or a messaging service (34%). 5
Online systems have increased access to PN and placed it in familiar virtual environments.11,12 They include PN-specialized websites: e.g., inSpot (USA; www.inspot.org), Partneralert (Belgium; www.partneralert.be), Let them know (Australia; www.letthemknow.org.au), Checkout (Portugal; www.checkpointlx.com/checkout), Partner Waarschuwing (Holland; www.partnerwaarschuwing.nl), PN systems hosted on gay hookup sites e.g., Online Buddies; www.online-buddies.com (international) and applications (e.g., Don’t Spread It; www.dontspreadit.com (USA). Nevertheless, as offline systems, they require patients to have their partners’ contact information.
WeFLASH©: New smartphone functions and partner notification
Sophisticated smartphone functions like specific-field communication, text/voice messaging, and geo-positioning 17 could benefit PN. Employing these functions, WeFLASH© (AADISS, Paris, France) is a program of online tools currently developed by the AADISS society to facilitate PrEPers’ follow-up in France. To be launched in 2019, WeFLASH© includes an app that sends automatic reminders for routine STI screening and facilitates anonymous PN without relying on users’ exchange of personal information (e.g., phone number, email). Figure 1 presents WeFLASH© user’s pathway from a sexual encounter, to the creation of anonymous links between users, to PN in case of STI exposure.
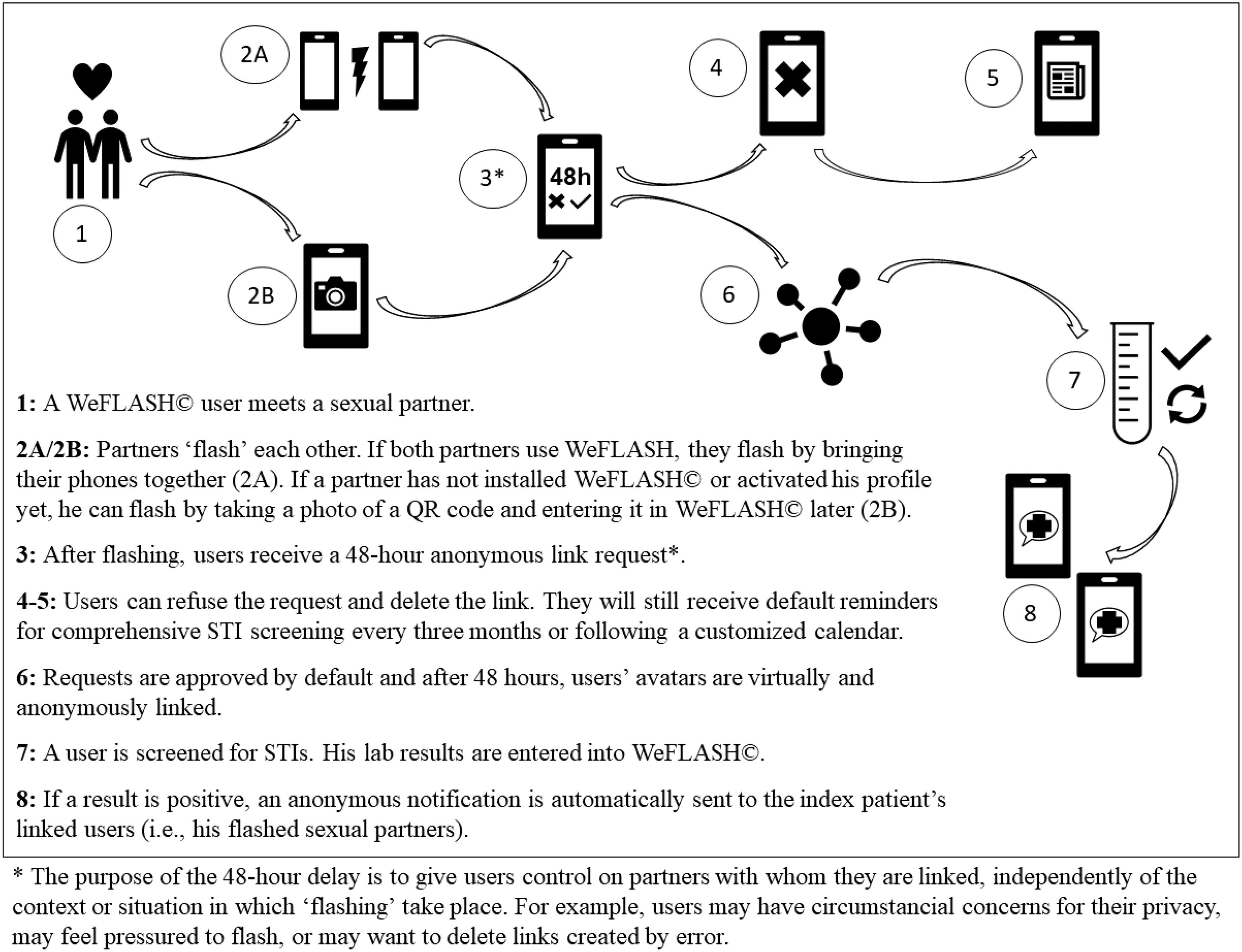
WeFLASH© users’ pathways to “flash” and notify partners.
No app currently exists in France to facilitate PN. It is unclear whether stakeholders, including PrEPers, their care-givers, and decision-makers involved in STI prevention in France, would be receptive to WeFLASH©. Still, the potential benefits, effectiveness and risks of any PN strategy should be examined. Our objective here is to describe key stakeholders’ perspectives on the acceptability of the WeFLASH© PN app.
Methods
Study design
This qualitative study is based on two-hour focus group discussions (FGDs) with MSM PrEPers and community Mediators involved in PrEP follow-ups, and one-on-one interviews with PrEP-prescribing physicians and decision-makers of HIV/STI prevention. FGDs and interviews were conducted between February and July 2018.
All participants received a 10-minute description of the WeFLASH© program beforehand. FGDs and interviews followed semi-structured questionnaires on barriers and facilitators of PrEP follow-up and PN, and preferences and concerns with the WeFLASH© program and PN app. DL conducted all FGDs and interviews with Mediators, and BL conducted interviews with Physicians. JZ or AA were present to observe FGDs and interviews. Participants received no compensation. The study was conducted in the three French cities with the highest number of PrEPers and STI prevalence: Paris, Lyon, and Nice. 18 Approval was obtained from the research ethics board of the Research Institute of the McGill University Health Centre, in Montreal, Canada, where two co-investigators are based. According to French public health legislation, 19 no ethical approval was needed in France.
Study setting and participants
Convenience sampling, a non-probability technique focusing on available groups often employed in qualitative and exploratory studies, 20 was used for PrEPers and mediators. In each city, officials from AIDES, a France-wide association, easily recruited adult MSM who had used PrEP for at least three months and owned a smartphone, and community mediators with an experience of PrEP follow-ups of at least three months. A pilot FGD was conducted in Paris to validate the questionnaire with two PrEPers who were also specialists in relevant fields (a care-provider and an app designer). Then, three other FGDs (one in each city) were conducted with PrEPers (n = 19), and two FGDs were conducted with mediators: one in Paris (n = 4), and one in Nice (n = 6). All FGDs were held at local AIDES offices.
Expert sampling, a purposive, non-probability technique to form a sample based on a particular expertise, 20 was employed for physicians and decision-makers. All physicians approached, and all decision-makers but one, agreed to participate. A total of five physicians were interviewed by BL during an HIV international conference. 21 Physicians practiced in Paris (n = 3), Lyon (n = 1), or Nice (n = 1). Four decision-makers, i.e., directors or managers in organizations promoting HIV/STI prevention, were interviewed in their work offices in Paris, in local organizations (n = 2) and in nation-wide institutions (n = 2).
Data analysis
Recordings of the FGDs and interviews were transcribed. The analysis focused on sections about the PN app. DL reviewed the transcripts to identify and label categories, or “codes,” which were discussed and refined with co-authors. The resulting scheme included perceived benefits of importance to stakeholders, risks and limitations, and solutions to manage them. The scheme was applied to all transcripts using NVivo 11.0 (Melbourne, Australia). DL and BL reviewed reports of the data in each code.
Results
Study participants
Table 1 presents participating PrEPers’ characteristics. Including the pilot FGD, PrEPers’ age ranged between 25 and 60, with an average of 38 years. About half (11/21; 52%) reported having more than 40 partners in the last 12 months; more than a third (8/21; 38%) reported having at least two STIs in the last 12 months; a third (7/21; 33%) reported having used substances during sex; and almost a fifth (4/21; 19%) reported using apps for information about STIs and PrEP.
Socio-demographic and professional description of participating PrEPers in FGDs.

FGD: focus group discussion; PrEP/PrEPer: HIV pre-exposure prophylaxis/HIV pre-exposure prophylaxis user; STI: sexually transmitted infection.
Example of comments from participants concerning the potential benefits and risks or impacts of the WeFLASH© patient notification app.
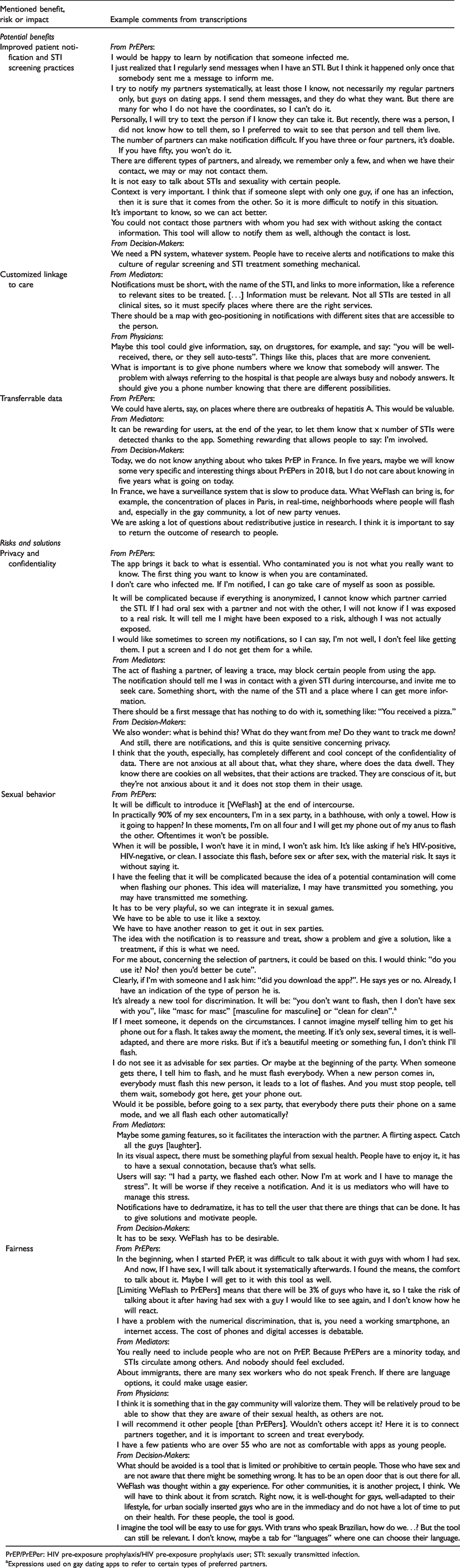
PrEP/PrEPer: HIV pre-exposure prophylaxis/HIV pre-exposure prophylaxis user; STI: sexually transmitted infection.
Expressions used on gay dating apps to refer to certain types of preferred partners.
Also, eight out of ten mediators were men. The length of their practice as mediators ranged from 6 to 74 months (average of 31 months). All but one mediator had worked with more than 100 PrEPers. All physicians specialized in infectious diseases, each having over ten years in HIV clinical practice, and four out of five were men. Half (2/4) of decision-makers were women, and three out of four had over ten years of experience in sexual health and STI/HIV prevention.
Table 2 provides illustrative comments from participants concerning perceived potential benefits and risks of WeFLASH(c).
Potential benefits of WeFLASH©
During FGDs and interviews, participants discussed three benefits the WeFLASH© PN app would have: improved PN and STI screening practices, customized linkage-to-care, and transferable data. Participants sometimes made suggestions for the app to realize these benefits.
Improved PN and STI screening practices
For decision-makers and PrEPers, WeFLASH© would improve PN and screening practices, which they consensually considered as important benefits. Referring to an alleged lack of PN interventions in France, decision-makers argued that a PN app would fill a need for targeted screening by notifying STI-exposed people and bring them into care.
PrEPers appreciated that WeFLASH© would inform them when to be tested and notify them in case of STI exposure. PrEPers explained that they were rarely notified by partners and currently felt limited in their capacity to notify their partners. They regularly attempted to notify their partners, mostly by using smartphones (dating apps, private messaging/social media, or phone calls), or talking directly to the person. Still, existing strategies were difficult to implement if one had too many partners, anonymous sex encounters, or concerns for partners’ reactions or for being identified as an index patient.
PrEPers considered that WeFLASH© would help notify anonymous partners met on dating apps, given that they would feel comfortable discussing the app with them and were likely to carry their phone when meeting them.
Customized linkage to care
Physicians and mediators valued how WeFLASH© could provide users with customized information on care and sexual health services. They suggested that notifications include geo-positioned references to convenient services in terms of services, location, and schedule.
Transferable data
Decision-makers and PrEPers appreciated WeFLASH©’s capacity to compile and exchange real-time data. For decision-makers, WeFLASH© could meet needs for epidemiological data on STI outbreaks and users’ sexual networks, behaviors, STI outbreaks, and treatments, necessary to design effective and timely prevention campaigns. Decision-makers, mediators, and PrEPers suggested the use of messaging functions to transfer findings back to users, including statistics on personal use and prevention messages.
Potential impacts, risks, and suggested solutions
Participants perceived potential impacts on, or risks for, their privacy and confidentiality, their sexual behavior, and fairness. In some cases, they made suggestions on ways to manage or minimize these risks.
Privacy and confidentiality
Decision-makers commented that concerns for privacy may dissuade some people from using the app. However, they added that several commonly used apps (e.g., social media) could raise similar concerns, and hence did not consider it as an important problem.
Mediators’ main concerns were that notified partners could suspect or identify index patients. They thus suggested short notifications emphasizing the necessity to receive care, with no details on index patients’ identity or circumstances of exposure. However, PrEPers recognized that they then may have difficulties assessing the seriousness of detail-less, anonymous notifications.
PrEPers and mediators were concerned that if another person saw a WeFLASH© notification on their phone, this person could identify them as app users and as potentially exposed to STIs. PrEPers and mediators suggested app settings to receive notifications at a preferred time, or to receive coded notifications on trivial, STI-unrelated topics with secured links to the information on STI exposure.
Sexual behavior
For some PrEPers, WeFLASH© could influence their choice of partners, especially on dating apps: they may prefer meeting WeFLASH© users, as an implied indication of safe sexual behavior and an assurance of being notified in case of STI exposure. Yet other PrEPers feared that such a criterion for choosing partners would become a form of discrimination among MSM.
PrEPers also perceived WeFLASH© as unfit for use in sex venues (e.g., bathhouses or sex parties), where one cannot carry a phone. They suggested: using WeFLASH© on a discreet, easy-to-carry device, such as a smartwatch, instead of a phone; adding a function to automatically flash all app users in close range; or installing “flashing terminals” in the entrance of sex venues.
PrEPers were also unsure about how/when to talk about WeFLASH© with their partners (before, during, or after sex). Some PrEPers were concerned that discussing WeFLASH© with intimate or committed partners would damage spontaneity or trust in the relationship, given the stigma associated with STIs. As a solution, they suggested the integration of playful sounds, animations, or game-like features to flashing. Also, PrEPers and mediators discussed how the app could induce associations with the anticipation or reception of notifications. They recommended reassuring language in the wording of notifications.
Fairness
Participants commented on WeFLASH©’s capacity to be used by people from different backgrounds and communities. PrEPers thought that it was a good idea to first launch the app among PrEPers, given their perceived high-risk level, health awareness, and self-perceived skills to discuss sexual health. For decision-makers, WeFLASH© is well-designed for digitally-connected MSM living in urban areas, who compose most of the current pool of PrEPers in France. Participants from all groups mentioned that WeFLASH© may give PrEPers pride, as “ambassadors” of an app to prevent STIs and improve collective sexual health.
Still, all participants also thought that WeFLASH© should be quickly expanded to all MSM independently of PrEP use. For PrEPers and mediators, a more inclusive implementation would mean more partners to flash, increasing WeFLASH©’s benefits and decreasing risks of judgment or rejection. For physicians, it would prevent stereotypes of users as high-risk people and would reach more STI-vulnerable networks. For decision-makers, it would increase the quality of app-generated epidemiological data.
Nevertheless, participants expressed doubts that WeFLASH© would reach all MSM. PrEPers and mediators mentioned potential linguistic barriers; PrEPers saw the cost of smartphone and data connections as prohibitive for certain people; and physicians commented that apps were often difficult to use for older people.
Discussion
This qualitative study describes stakeholder groups’ perspectives on the acceptability of a French PN app allowing users to create virtual links and receive automatic and anonymous notifications in case of STI-exposure. In Paris, Lyon, and Nice we conducted FGDs with PrEPers and community-based mediators, and semi-structured interviews with PrEP-prescribing physicians and decision-makers, i.e., high officials in organizations dedicated to the management of HIV/STI prevention.
Participants found WeFLASH© an acceptable tool. Anticipated benefits were modulated by group affiliation. PrEPers and decision-makers found that the app was well-designed to notify partners met anonymously on dating apps, which compose an increasing portion of MSM’s partners and are the most difficult to notify.5,14 They appreciated the possibility of generating/transferring real-time data that could help PrEPers adapt their behavior and lower their risk of exposure, and help decision-makers understand epidemics and design appropriate prevention campaigns or policy. Care-givers, including physicians and mediators, emphasized the improved access to and delivery of sexual health services. 2 Similar to the conclusions of a review of PN strategies, 22 they suggested the addition of adapted information in notifications for more efficient linkage-to-care, especially for out-of-care people.
For participants, a balance should be achieved between privacy and effectiveness. Accordingly, anonymous notifications with little detail of the circumstances of STI exposure may increase users’ sense of privacy but have limited effectiveness if users do not feel concerned, a finding that echoes a study of PN from notified partners’ perspectives. 23 PrEPers and decision-makers gave less importance to privacy in their comments than other participants, maybe because they anticipate more benefits from the transfers of information. However, a study showed that although app users are generally ready to divulge personal information if they receive benefits in return, they still expect security for their privacy and data, especially when health-related information is concerned. 24 Physicians and mediators were more concerned with privacy, maybe because professional secrecy importantly defines their professional activity. Indeed, French legal frameworks used to examine PN include professional secrecy and rights to information, privacy, confidentiality, and consent. 3 Hence confidentiality and privacy should not be taken lightly.
Notwithstanding, with WeFLASH©, professional secrecy is not threatened because care providers are not notifying partners themselves. Also, in existing online and offline PN strategies, notified partners passively receive notifications. 11 With WeFLASH©, all users are empowered: all must technically consent to install the app, flash their partners, maintain links with flashed partners’ avatars, and send and receive notifications. Still, PrEPers suggested additional measures to increase users’ sense of security and privacy: providing clear information in several languages on security settings, and allowing users to decide when and how they want to be notified.
Besides privacy, perceived risks mainly affected sexual behavior and fairness. Any health intervention is constituted of several apparently trivial practices that are nevertheless ethically sensitive given their impacts on individuals' rights, lifestyles, and justice. 25 Participants mentioned they could use WeFLASH© to “sort” partners, a potential form of discrimination similar to “serosorting” (i.e., choosing partners in function of their HIV status or PrEP use), already present in gay communities. 26 They suggested innovative functions to alleviate associated risks and make the app more adapted to users’ contexts, including reassuring notifications offering tailored information on adapted and accessible care and playful items to reduce stress and facilitate integration in sexual contexts. Participants also suggested making WeFLASH© available to all MSM to reduce stereotypes of PrEPers as risk-taking 27 and respond to increasing prevalence rates of STIs among MSM. 2
WeFLASH© is not appropriate for all MSM, in all sexual contexts. For instance, participants anticipated potential difficulties to use the app with committed partners, whom they preferred to notify directly, as well as linguistic, financial, and generational barriers. They also saw obstacles in sex venues/parties, although a recent study on PN in France found high rates of PN for MSM who attend sex parties. 5 Individuals choose different PN strategies based on their values, practices, relationship types, and the information they have on their partner.3,28 While WeFLASH© is an innovative and important addition to the field of PN, several PN strategies should be presented to index patients, with explanations of their respective advantages, limits, and implications, so patients can make informed decisions. 3
This study’s limitations include its small sample size. Still, considering exploratory data from all stakeholder groups, data saturation was achieved, as no new data sufficiently stood out to justify additional FGDs or interviews. This suggests that these results may be transferable to similar contexts. Still, as WeFLASH© is implemented, mixed (qualitative/quantitative) methods data collection from a more representative sample of PrEPers, should be used to document more comprehensively users’ STI and PN experiences, including their dating and sexual contexts (e.g., use of dating apps, sex in bathhouses); history and frequency of STI screening; and strategies employed when notifying partners and being notified. Finally, one person was responsible most data collection activities and for conducting the analyses, which could have biased our results. Nevertheless, observers were present during FGDs and interviews, and analyses and results were regularly discussed with other investigators for validation.
Conclusion
Consulting key stakeholders to assess the acceptability of WeFLASH© provided important feedback for its design, and improved our understanding of PrEPers’ practical concerns with PN. This study highlights the value of stakeholders’ perspective and feedback in the design and development of new health and prevention technologies. A complementary study should be conducted on the implementation of WeFLASH© in real-world context.
Footnotes
Acknowledgments
The WeFLASH program is developed by the AADISS society and supported by the AIDES France association.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: BL holds a Canadian Institutes of Health Research Strategy for Patient-Oriented Research Mentorship Chair in Innovative Clinical Trials, and DL is a research assistant in this Mentorship Chair (#383427).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.