
Abstract
Pharyngeal testing for Neisseria gonorrhoeae (gonorrhoea) in heterosexual men is not currently recommended in UK guidelines; however, it was being undertaken in a service in the North East of England for those presenting with urethral infection or as contacts of gonorrhoea. This service evaluation was performed to see if this practice should continue, or cease in line with national recommendations. The results revealed that 10% of contacts were positive in the pharynx only. Had this test not been performed, it would have left these patients without any treatment, as the current guidelines now discourage epidemiological treatment of contacts. Twenty-seven per cent of all heterosexual men diagnosed with urethral infection also had oropharyngeal gonorrhoea, with implications for persistent infection, had testing not been performed followed by a test of cure.
Keywords
Introduction
Pharyngeal testing of gonorrhoea in heterosexual men used to be recommended in UK national guidelines in men with urethral gonococcal infection (suspected on urethral microscopy or laboratory confirmation) and those presenting as contacts of gonorrhoea. This changed in 2011 1 when pharyngeal testing in men was no longer recommended; no reason was given for this, and it was not mentioned in the ‘Changes since 2005 Guideline’ section at the start of the guideline. As this change was not highlighted, a level 3 service in North East England continued this practice. Current UK guidelines now state that extragenital testing should be ‘guided by an assessment of risk and symptoms’ in people who are not women or men who have sex with men (MSM). 2 Following this oversight being highlighted, a service evaluation was undertaken to assess if the practice should continue, or stop in-line with national recommendations. Rectal swabs have never been performed in heterosexual men in this service.
Methods
The service sees approximately 2600 heterosexual men per year and is situated in a major city. The prevalence of gonorrhoea in the local population is 75 per 100,000, with an overall increase in the North East of 23% between 2014 and 2018. 3 The local database (Lilie) was searched for all men with a diagnostic code for gonorrhoea (B) or contact of gonorrhoea (PNG) between 1 August 2016 and 31 July 2018, as these were the only heterosexual men who should have had a pharyngeal swab (following local guidelines). Patients’ sexual orientation was self-reported. There is a local code, M, denoting MSM, and these were excluded from analysis. Electronic medical notes were then reviewed, sexuality was confirmed, and it was recorded whether a pharyngeal swab had been taken; the pharyngeal swab result; and the proportion of contacts that were positive for gonorrhoea. The assay used to test the swabs was the Cobas® 4800 CT/NG Test (Roche Molecular Systems, Branchburg, NJ, USA), which is a nucleic acid amplification test (NAAT).
Results
A total of 232 heterosexual men were coded as B or PNG; 131 men had a diagnosis of gonorrhoea in the urethra, either through microscopy or asymptomatic screening (excluding those presenting as contacts). In these patients, 80.9% (106/131) then had a pharyngeal swab performed, and 33% (35/106) of these pharyngeal swabs were positive for gonorrhoea (see Table 1). One patient had failed treatment and remained positive on the NAAT in the pharynx, despite clearing the urethral infection.
Summary of results.
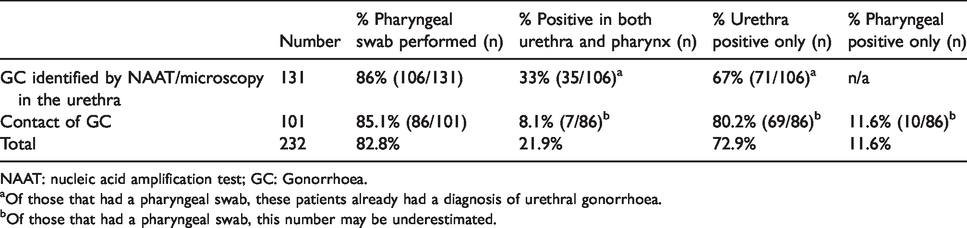
NAAT: nucleic acid amplification test; GC: Gonorrhoea.
Of those that had a pharyngeal swab, these patients already had a diagnosis of urethral gonorrhoea.
Of those that had a pharyngeal swab, this number may be underestimated.
A total of 101 men presented as contacts of gonorrhoea, with an overall positivity rate of 35.6% (36/101) (urethral and/or pharyngeal). A pharyngeal swab was performed in 85.1% (86/101) of patients, with 19.8% (17/86) being positive; 58.8% (10/17) of these patients were only positive in the pharynx; this represented 11.6% (10/86) of all pharyngeal swabs taken, 9.9% (10/101) of all contacts and 27.7% (10/36) of all positive gonorrhoea diagnoses in those presenting as contact of infection (see Table 1).
Overall, 22.4% (52/232) in both groups (urethral infection and/or presenting as contact), and 26.8% (42/157) of those with urethral infection, had oropharyngeal infection.
Discussion
Current national guidelines do not make any recommendations that heterosexual men should have pharyngeal swabs taken, unless they have a resistant strain isolated from the urethra, or it is suspected they acquired the infection in the Asia-Pacific region. 2 In this review, had the pharyngeal swabs not been taken, one in ten of all contacts would have gone undiagnosed, and in all heterosexual men with urethral infection, over one in four would have been unaware they had pharyngeal gonococcal infection. Had all in this review had a pharyngeal swab performed, these results may have been even higher.
The Cobas® 4800 CT/NG Test was the assay used to test the swabs. This assay has a specificity of 100% and a sensitivity of 99.7%. 4 It should be noted that this test has not been validated for use within the European Economic Area (EEA) for testing at extra-genital sites, but has been internally validated in the laboratory and found to be suitable.
One patient (who only had a pharyngeal swab taken at his test of cure) failed treatment and remained positive in the pharynx by NAAT; unfortunately it could not be cultured. The urethral infection had cleared at test of cure. The infection in his oropharynx could have led to onward transmission, highlighting the need to ensure any oropharyngeal infection is identified and then cleared. It is well documented that oropharyngeal infection is more difficult to treat5–8 and the national guidelines emphasise that those with oropharyngeal infection have a test of cure. Latest changes in the UK national recommendations state that epidemiological treatment is no longer routine 2 ; therefore, had those presenting as contacts not been tested at the pharynx, they would be unaware and untreated, with missed opportunities for partner notification and prevention of onward transmission.
In recent years, there is a strong body of evidence for gonorrhoea transmission through kissing, and through the orogenital and ororectal route.9–12 Some researchers have specifically looked at heterosexual men, finding up to 89% of contacts of gonorrhoea having solitary oropharyngeal infection, 13 and 36% of all heterosexual men found positive for gonorrhoea, were only infected in the oropharyrnx. 14 The majority of research has been performed in MSM, but the principals remain the same if the urogenital route of transmission is removed. These data were not specifically collected from this cohort of patients. The bacterial load in saliva has been found to be no different from that in the pharynx, regardless of culture positivity or negativity, 15 meaning that heterosexual men have the same risk for acquiring oropharyngeal gonorrhoea as MSM and women. A study published in 2018 identified a ‘sexual network’ in Australia. 16 It found that there was a disproportionately high incidence of oropharyngeal gonorrhoea in the absence of urogenital infection. There was a similar strain found in the pharynx of two people, separated in the network by two other participants, strongly suggesting that these infections were transmitted within the network as opposed to sexual contact with others.
As with any study, there are limitations to this service evaluation. Firstly, no specific behavioural data were collected from this cohort of patients, such as rimming or kissing. Also, we have to assume that the patients are being truthful when they state that they have had no sexual contact with men. The assay used, although internally validated as reliable, is not approved within the EEA for testing specimens from extragenital sites. None of the pharyngeal swabs taken for culture were positive. On one hand, this may not be surprising, given that gonorrhoea culture of the pharynx is only around 50% sensitive,17–19 but it cannot be ruled out that some of these tests could be false positive results.
This service evaluation showed that pharyngeal testing in heterosexual men presenting as contacts of gonorrhoea, or positive for gonorrhoea in the urethra, is warranted and we plan to continue our current practice.
Footnotes
Acknowledgments
We wish to thank Dr Andrew Berrington, Consultant Microbiologist, Sunderland Hospital, for his advice and review of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.