
Abstract
Not all human papillomavirus (HPV) infections develop into cervical cancer (CC), so it is proposed that other factors may influence this, such as co-infection with Chlamydia trachomatis (CT). To identify the prevalence of co-infection, we included 189 women with suspicion of HPV. Viral typing was performed by carrying out the Roche HP Linear Array test, while CT detection was performed with the COBAS® TaqMan® 48 kit from Roche. Of the 189 women only 184 had an infection with HPV, CT or both: 56.6% were positive for one or several HPV genotypes, and 67.7% for CT. Clinical data showed an association between HPV and CIN I (n = 22; RR = 2.43; 95% CI 1.72–3.43, p < 0.05). CT infection was only associated with cervicitis (n = 40; RR = 1.73; 95% CI 1.34–2.23, p < 0.05). The CT-HPV co-infection rate was 28%. Co-infection revealed an association with CIN I (n = 31, RR= 3.33; 95% CI 2.08–5.34 p < 0.05), CIN III (n = 7; RR = 2.57; 95% CI 1.53–4.31, p < 0.05); and a significant risk of 2.3 (95% CI 1.08–4.90) times higher to develop CC; nevertheless, this risk was not statistically significant. CT/HPV co-infection was associated with the development of a high-grade lesion (CIN III) as well as an important risk for developing CC.
Introduction
Human papillomavirus (HPV) and Chlamydia trachomatis (CT) are two of the most frequent sexually transmitted microorganisms worldwide. Both pathogens are characterized by developing persistent infections and possessing oncogenic properties. 1 It has recently been shown that CT can alter cell survival pathways, cell cycle regulation, repair of DNA damage, and duplication and placement of the centrosome; therefore, CT promotes malignant transformation. 2 HPV infection is recognized as the most frequent cause of the 500,000 cases of uterine cervical cancer (CC) that are reported every year worldwide. 3 In Mexico, the prevalence of HPV in women is estimated at 36%. 4
The Papillomaviridae family typically has five evolutionary groups with different tropism to the epithelium and various clinical characteristics, defined as different genera (α, β, gamma, µ, ν-papillomaviruses).5,6 There are 65 varieties of HPV of the α genus that have been classified as “low-risk” (lrHPV) and more than 14 specific types of “high-risk” (hrHPV) that have been typically associated with the development of cancer. 6 The International Agency for Research on Cancer (IARC) designates genotypes 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, and 59 as carcinogens (group 1); as probable carcinogens (group 2a) to HPV 68; as possible carcinogens (Group 2 b) the genotypes 26, 30, 34, 53, 66, 67, 69, 70, 73, 82, 85, and 97; non-classifiable (group 3) and non-carcinogenic (group 4) genotypes 6, 11, 40, 42, 43, 44, 54, 55, 57, 61, 71, 72, 83, 84, Iso39, 71, 81, and 89/CP6108. 7 , 8
Chlamydia trachomatis is an obligate intracellular bacterium that produces a vast variety of clinical signs in both women and men, infertility being one of the most critical factors. The World Health Organization (WHO) estimates that 131 million new cases of CT are detected annually worldwide. 9 In developed countries, the prevalence of infection by CT is usually 3% to 6%. 10 While in Mexico, it is 4% to 19% according to the population of women who were diagnosed (infertile, sex workers, pregnant adolescents, among others). 11 To date, the percentage of co-infection with CT and HPV reported is 0.7% to 23.5%, in women with CIN and/or CC. 12
It has been reported that CT infections may indirectly influence the progression of CIN and/or CC, caused by HPV. It has been proposed that CT promotes the entry and persistence of high-risk HPV, resulting in chronic inflammation and inhibition of cell apoptosis. 13 Alternatively, some studies report the relationship among CT and cervical lesions, where it has been shown that the prevalence of CT was 47% higher in women with CIN III than in those females with conventional cytology. It has been shown that there is a significant relationship between patients showing high grade CIN and positivity for CT. 14
The purpose of this study was to identify the prevalence of co-infection with HPV genotypes and CT infection in Mexican women with and without cervical intraepithelial neoplasm (CIN).
Methods
Characteristics of the study
A descriptive cross-sectional study was carried out on endocervical samples obtained between January and December 2015 conducted at the Instituto Nacional de Perinatología Isidro Espinosa de los Reyes in Mexico City, with endocervical samples obtained between January and December 2015. This study was previously approved by the Bioethics Committee of that Institute Reg. No. (499) 212250–3120-10607–01-14. As inclusion criteria, outpatients consecutive to their clinical follow-up, who attended the oncology, gynecology clinics or who were patients of the infertility clinic (areas belonging to the hospital) were selected. We included postnatal and prenatal patients, and patients who had data on a history of HPV infection in recent years whose age range was 15 to 50 years old, who agreed to participate in the study by signing an informed consent, with data suggestive of cervical dysplasia, through colposcopy, and cervical cytology studies by Pap smears. For the identification of the various epithelial lesions, a pathologist identified them by using the classification of cervical intraepithelial neoplasia proposed by Richart (1980), in cervical neoplasms of different grades (CIN I, II, III), CC, cervicitis or leucorrhea. Data were also included in the possible treatment provided to patients.
The exclusion criteria of this study were patients who were being treated with antibiotics and who used intravaginal medications, since these can interfere with the pathogens detection by using the kits for the diagnosis of HPV and CT. Patients who were menstruating or had active vaginal discharge, women with autoimmune diseases, with HIV infections or with some other type of cancer were also excluded from the study.
The variables to be analyzed were: sociodemographic data, such as age, marital status, history of number of sexual partners until 2015, as well as continuous consumption of alcohol, tobacco and drugs; together with the three different degrees of CIN, CC, cervicitis, leucorrhea, and HPV, CT infection or both.
Finally, a follow-up for four years was carried out for HPV + CT + patients by reviewing their clinical record, in order to observe if there was an evolution of the CIN, after detection of the hrHPV genotype (s) and treatment to eliminate CT that concluded in 2015.
Endocervical sampling
The samples were collected during the Pap smear by using an endocervical brush, performing a circular scraping of the cervix. Subsequently, the brush was placed in a sterile tube containing transport medium (BD universal Vitral transport, Becton Dickinson and Company, Sparks, MD USA).
HPV genotyping
DNA purification and amplification, as well as the detection of HPV genotypes from endocervical samples were carried out by managing the commercial kit Linear Array HPV Genotyping Test (Roche Molecular Diagnostics, Branchburg NJ USA), following the manufacturer's instructions. For the amplification of the polymorphic L1 region of the HPV genome, biotinylated oligonucleotides already designed by Roche were used to amplify the DNA of the 37 HPV genotypes identified by this kit. For the detection of HPV genotypes, hybridization was performed on nylon strips provided by the same kit which includes 13 high-risk genotypes (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 68) and 24 low-risk genotypes.
Detection of Chlamydia trachomatis in endocervical samples
The detection of Chlamydia trachomatis was performed by using the real-time PCR technique by using an automated equipment for DNA extraction and amplification, and detection of C. trachomatis, by using DNA kits Amplicor® CT/NG (Roche Molecular Diagnostic, Oklahoma, OK, USA) and COBAS® TaqMan® 48 (Roche), respectively. For this, the manufacturer's instructions were followed. The detection of Chlamydia DNA was performed through the amplification of two fragments of the cryptic plasmid DNA (ORF 1 and ORF 2 region) and a fragment of the ompA gene of the chromosome of the bacterium.
Statistical analysis
The results were analyzed with the SPSS software version 20.0 (IBM Corp. Released 2011. IBM SPSS Statistics for Windows, Version 20.0, Armonk, NY: IBM Corp), by using the Fisher’s exact nonparametric test. The magnitude of the associations between the variables was expressed as relative risk (RR) in a confidence interval (CI) of 95%. A p < 0.05 value of two tails was considered as statistically significant.
Results
Of the 189 women with suspicion of infection, only 184 were selected for presenting an infection with HPV, CT, or both pathogens, while five patients had no pathogens detected. 107 (58%) were positive, and 82 were (44.5%) negative for HPV. Regarding CT detection, 128 (69.5%) were positive and 61 (33%) were negative. Of the latter, 51 (28%) showed co-infection (HPV + CT +), 56 (30%) only with HPV, and 77 (42%) only with CT (Table 1). The average age of women positive for HPV was 32.9 years old, while the population of women positive for CT was 35 years old. Women aged 15 to 19 years old accepted a significant relative risk of getting an HPV infection (RR = 2.52, 95% CI 2.05–3.98). Table 1 shows the sociodemographic data of the population with HPV infection, CT infection and HPV+CT+ co-infection, respectively. Regarding marital status, 38.6% were single women, 30.6% married women, and 30.6% in cohabitation.
Sociodemographic data of women testing positive for human papillomavirus, Chlamydia trachomatis and coinfection.
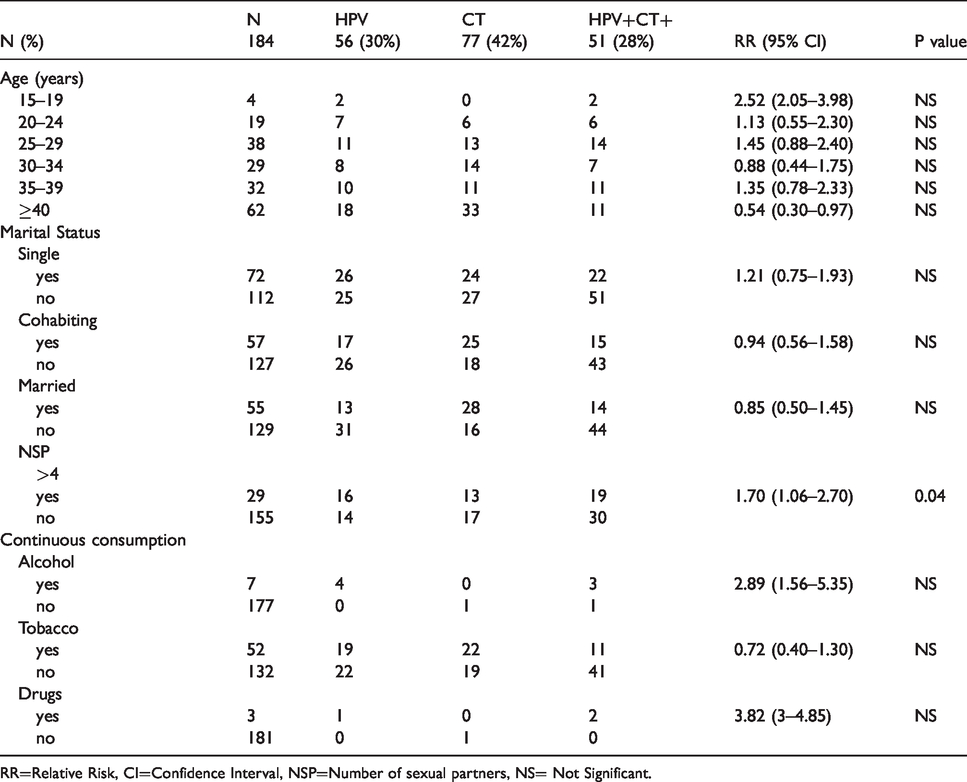
RR=Relative Risk, CI=Confidence Interval, NSP=Number of sexual partners, NS= Not Significant.
Significant association was demonstrated in those women with HPV and CT co-infection, and the number of sexual partners; a significant relative risk was observed when they had had more than four sexual partners (n = 19; RR = 1.70, 95% CI 1.06–2.70, p < 0.05). The women who regularly drank alcohol (RR = 2.89, 95% CI 1.56–5.35) or used drugs (RR = 3.82, 95% CI 3.0–4.85) showed a substantial, but not significant risk of getting HPV-CT co-infection (Table 1).
Prevalence of co-infection between HPV and CT
The most important type of lesion that is significantly associated with HPV infection was that of CIN I (n = 22; RR= 2.43, 95% CI 1.72–3.43, p < 0.05). Also, we found an important, but not significant risk to CIN III with HPV infection, (n = 3; RR= 1.70, 95% CI 1.04–3.47). The development of condylomas was more common in patients with HPV infection (n = 12; RR= 2.86, 95% CI 2.26–3.63, p < 0.05) (Table 2). CT infection was only significantly associated with the presence of cervicitis (n = 25; RR= 1.73, 95% CI 1.34–2.23, p < 0.05); also in those patients with CT infection, only seven had CINI, three CINII, one CINIII, and one developed CC; in each case there was no association with CT infection (Table 2). In addition, women with co-infection with HPV and CT showed a significant association with development of CIN I (n = 31; RR= 3.33, 95% CI 2.08–5.34, p < 0.05) and CIN III (n = 7; RR= 2.57, 95% CI 1.53–4.31, p < 0.05). Furthermore, a substantial, but not significant risk of 2.3 times greater of having co-infection in patients with CC was demonstrated. In the same way, the HPV+ CT+ patients, had a statistically significant association with the unusual presence of condylomas (n = 19; RR= 3.03, 95% CI 1.99–4.59, p < 0.05) and leucorrhoea (n = 17; RR= 2.36, 95% CI 1.49–3.73, p < 0.05) (Table 2).
Frequency of HPV and Chlamydia trachomatis infection in women with different intraepithelial lesions.
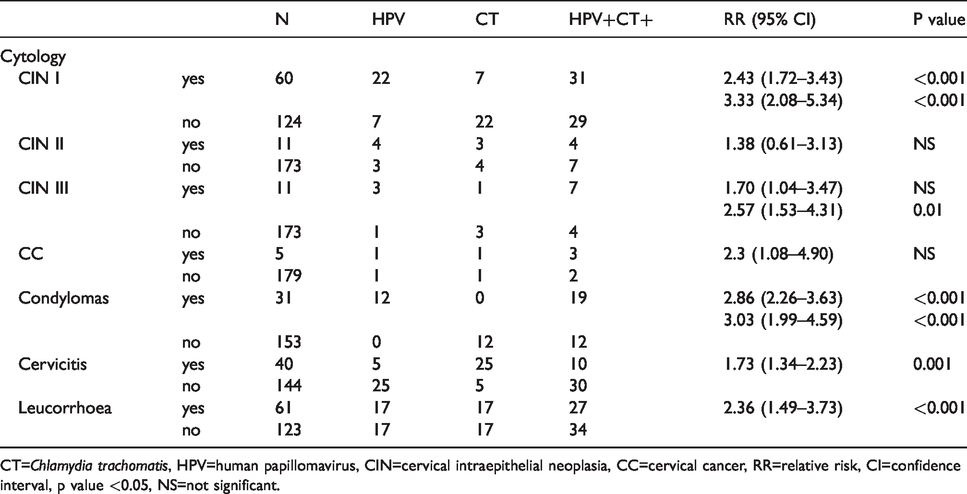
CT=Chlamydia trachomatis, HPV=human papillomavirus, CIN=cervical intraepithelial neoplasia, CC=cervical cancer, RR=relative risk, CI=confidence interval, p value <0.05, NS=not significant.
HPV genotypes and C. trachomatis infection
Of the 107 samples with HPV infection, 42 were high-risk genotypes (hrHPV); 36 were low-risk (lrHPV), and 29 had both genotypes. It is important to note that most patients had more than one HPV genotype. The most frequent hrHPV genotypes were: 59, 16, 52, 66, and 53; while those of lrHPV were: 61, 62, 6, 11, 71, and CP6108.
The percentage of hrHPV genotypes that were identified in the different types of intraepithelial lesion were: 39.3% in patients with CIN I (RR = 1.48, 95% CI 1.11–1.96, p < 0.05); 7.5% in patients with CIN II, 9.3% in CIN III, and 3.7% in patients with CC (Table 3).
Percentage of infection by high-risk and low-risk human papillomavirus in women with intraepithelial lesions.

CT=Chlamydia trachomatis, HPV=human papillomavirus, hrHPV=high risk HPV, lrHPV=low risk HPV, CIN=cervical intraepithelial neoplasia, CC=cervical cancer, RR=relative risk, CI=confidence interval, p value <0.05, NS=not significant.
Of the 51 patients co-infected with HPV and CT; 23 had hrHPV, 16 lrHPV, and 12 had both genotypes detected (Table 4). The genotypes of hrHPV that showed co-infection with CT at a higher frequency were: 59, 16, 51, 53, and 66; while in lrHPV genotypes were: 62, 11, and CP6108. An important, but not significant risk was demonstrated in genotypes 18 (RR= 2.06, 95% CI 1.69–2.5), 40 (RR= 2.04, 95% CI 1.68–2.47), 51 (RR= 1.82, 95% CI 1.26–2.63), 69 (RR= 2.06, 95% CI, 1.69–2.5), 81 (RR= 2.06, 95% CI, 1.69–2.5), and co-infection with CT (Table 4).
Frequency of high-risk and low-risk genotypes of human papillomavirus with and without co-infection with Chlamydia trachomatis.
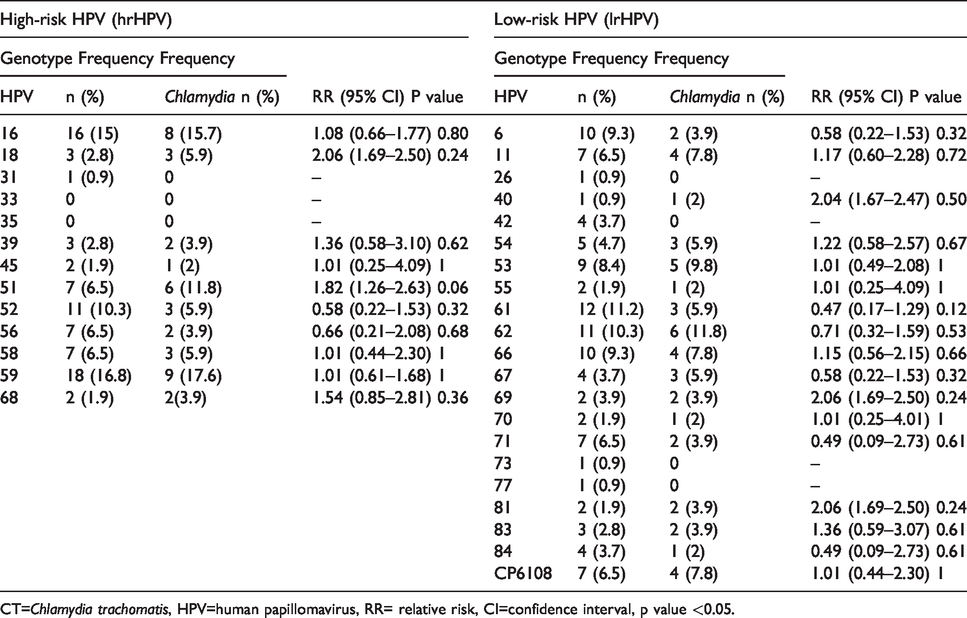
CT=Chlamydia trachomatis, HPV=human papillomavirus, RR= relative risk, CI=confidence interval, p value <0.05.
Discussion
Cervical intraepithelial neoplasia (CIN), is an abnormal growth of squamous cells of the cervix, one of its main precursors is HPV infection. However, there are also other factors that can influence the development of these lesions; 15 there is co-infection with other microorganisms, such as the Herpesviridae family (cytomegalovirus, Epstein-Barr, and herpes simplex type 2) or Chlamydia trachomatis, although, by themselves, these microorganisms could develop CIN. 12 However, in this investigation the presence of these viruses was not analyzed, only the detection of CT was carried out. The prevalence of HPV infection in patients studied with CIN was 32%, a higher percentage than that reported by Madaan et al., in 2019, 16 who mentioned that the prevalence of HPV in patients with abnormal cervical cytology was 21.1%, where those who had high grade CIN (1.1%) had 100% positive HPV, while 41.1% were low grade CIN.
Currently, studies have been carried out internationally on co-infection between HPV and CT (HPV-CT), it has been reported that the worldwide prevalence is between 4–59%.1,12 In the present study, the percentage was 47.7% (51/107), therefore it is within the ranges published worldwide; while Conde-Ferráez et al., 17 in 2019, reported a prevalence of 6.3% (4/63) in women of Morelos state, Mexico. This not rare, Panatto et al., 18 in 2015, reported a prevalence of 14.6% in Italian women (15/103), likewise, a similar prevalence was found by Saraceni et al., 19 in 2014, were 60% (32/53) in women in the same country.
Recently, it has been reported that CT infections may indirectly influence the progression of CIN and/or CC, caused by HPV. Alternatively, some studies report the relationship between CT and cervical lesions, where it has been shown that the prevalence of CT was 47% in women with high grade CIN than in those with normal cytology; it has been shown that there is a significant relationship between patients showing high-grade CIN and positivity for CT. 14 In the present study, we demonstrated an association between CIN I and CIN III and the co-infection between HPV and CT, as well as an important risk of CC with HPV-CT co-infection. Some studies that relate CC with CT, report a possible association, as in the study conducted by Wallin et al., 20 where they observed that 118 women who developed cervical cancer after having had a normal Pap smear, had a prevalence of CT infection of 8%. Their results show that the risk of contracting CC in patients with previous infections of CT, adjusted for HPV co-infections was 17.1%, for which they suggested an association between both pathogens. The association with CC or CIN could be due to what some researchers, such as Safaeian et al., 13 proposed, where a CT infection promotes the entry and persistence of high-risk HPV, because of chronic inflammation and inhibition of cell apoptosis that causes bacteria inside the cell, so that co-infection could exacerbate the clinical picture of patients. Furthermore, Paula et al., 21 reported that 17.1% of women infected with CT had some type of high- or low-grade lesions, so CT solely could play some role in the formation of CIN.
In order to know if the patients increased the degree of CIN after the identification of the hrHPV genotype(s) and having been treated with azithromycin (specific treatment for CT infection), it was decided to carry out their follow-up on the development of their lesions during a period between 2016 and 2019. The results obtained showed that only two patients continued with CIN I data until 2019, while the rest of the patients who had shown some type of CIN did not progress to a greater degree (data not shown). This is because the hospital doctors removed, by cervical cone surgery, the damaged area, such as CIN II and III, in addition to continuously monitoring patients after the high-grade lesion was detected. It is also important to note that the majority of patients with CIN I regress spontaneously as Arends et al., tell us, where they mention that 50–60% of the lesions diagnosed as CIN I will regress spontaneously; if clinicians intervene at such an early phase of the process it may result in the unnecessary treatment of women who are at little or no risk of developing carcinoma. 15
Several studies have reported that high-risk sexual behavior contributes significantly to an elevated incidence of HPV infection and other STIs. Ryser et al., in 2017, 22 suggested that sexual behavior has achieved an increase in HPV exposure in recent years, which in turn is associated with the incidence of intraepithelial lesions and cancer in the United States. So that, significant changes in sexual risks, such as early coitarche, where they reported a growth of 11% since 2010, and a prevalence of HPV 60% higher in women aged 20 to 29 years old than in older females, were also associated with sexual behavior. There was moreover an increase of more than five sexual partners in young women since 2000, which in turn was associated with the presence of HPV and CC. In the present study, we observed an association between HPV+CT+ co-infection in those women with more than four sexual partners, which suggests that sexual behavior is related to the increased risk of these infections. 22 In this study, the prevalence of CT infection was 70%, a high percentage for that reported in Mexico, however, it is a population that had not been previously investigated. Despite the above, this percentage is lower than the one reported by Liu et al., 23 in 2015, who described that 91% of women infected with CT showed HPV genotype infection.
Currently, HPV16 and 18 continue to be the most prevalent worldwide. Despite the above, the prevalence of other genotypes has been increasing. Reports in this regard mention that the most frequent are genotypes 58, 51, 52, and 53; 4 , 24 in that study it was shown that HPV59, HPV16, and HPV 52 were the most prevalent. The most frequent low-risk genotypes worldwide are 6 and 11; in this study, both the presence of these genotypes and genotypes 61, 62, 71, and CP6108 were confirmed. Chironna et al., in 2010, 25 have reported that genotypes 61, 62, and CP6108 show a prevalence of 10.7%, 8.4%, and 7.9%, respectively, in Italian women, and that these genotypes were also associated with the presence of low-grade intraepithelial lesions. In this study, 12.1% of women exclusively infected with lrHPV developed CIN l, confirming the role of these genotypes in the formation of low-grade lesions.
Recent studies have shown an increased risk of HPV infection in women with a previous CT infection; it is likely that Chlamydia causes local inflammation leading to the development of a significant damage to the epithelial tissue, which can cause women to be more susceptible to HPV infections, regardless of the genotype. 19
Furthermore, it is known that CT increases susceptibility to HPV by producing microabrasions and alterations between the bonds of epithelial cells, damaging the mucosal barrier and allowing HPV to enter, which could aggravate the clinical framework of the lesion.
Regarding HPV-CT co-infection, Seraceni et al., reported that the genotypes HPV16, HPV59, and HPV53 (high-risk) presented a co-infection with CT in 12%, 20%, and 21%, respectively. In our study 28% of the women presented co-infection, the most prevalent HPV genotypes were 59 with 17.6%, 16 with 15.7%, 51 with 11.8%, and 53 with 9.8%. It is important to mention that in the present study it was not possible to report a significant association due to the small number of positive samples for each type of HPV. Despite the aforementioned, it is reported that genotype 51 had a major relative risk, but not significant 1.8 times higher for coinfection with CT, a similar fact was found for genotypes 18, 40, 69, and 81.
Conclusion
In addition, an important association was found between high-grade lesions such as CIN III and HPV-CT co-infection, suggesting that co-infection could contribute to the development of high-grade lesions.
Footnotes
Authors’ contributions
M.A.E.T., F.M.G.I and G.C.E. designed the study; M.A.E.T., M.L.H., M.R.E.G., F.M.G.I and G.C.E analyzed and interpreted the data and results; M.A.E.T., F.M.G.I and G.C.E gave a major contribution to the writing of the manuscript.
Acknowledgments
M.A.E.T., received grant-aided support from “Consejo Nacional de Ciencia y Tecnología” (CONACyT, México), while G.C.E, F.M.G.I, M.R.E.G, and E.R.M received support from the “Sistema Nacional de Investigadores (SNI)” from CONACyT, Mexico. G.C.E and E.R.M received support from Estímulos al Desempeño en Investigación, Comisión y Fomento de Actividades Académicas (Instituto Politécnico Nacional). This study was funded by Secretaría de Investigación y Posgrado del Instituto Politécnico Nacional (SIP 20194936, 20200675). The authors are also grateful to Sofia Mulia for correcting the style of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.