
Abstract
Some syphilis patients do not exhibit an appropriate serological response after treatment despite the absence of any clinical evidence of treatment failure or reinfection. This condition is called “serofast syphilis” or “serological non-response syphilis.” This study explored the incidence of asymptomatic neurosyphilis (ANS) and related factors in 324 asymptomatic patients with serological non-response syphilis. We analyzed descriptive statistics stratified by the presence of asymptomatic neurosyphilis for the basic characteristics of samples. Bivariate analysis was conducted to assess correlations between outcomes and potential predictors. Variables significant in the bivariate analysis (p<0.1) were entered into multivariable logistic regression models. All p-values were two-sided with a significance threshold of p<0.05. The results indicated that 89 of 324 patients had ANS (incidence of 27.5%), and the greatest risk factors were a < fourfold decrease in serum rapid plasma reagin (RPR) titers after treatment and current serum RPR titers >1:32. Our findings suggest that ANS is common among syphilis patients, and patients with a fourfold decrease in serum RPR titers after treatment and current serum RPR titers >1:32 are more likely to develop ANS.
Introduction
The incidence of syphilis has increased worldwide.1,2 It has been reported that approximately 12 million new cases of syphilis occur each year worldwide, and the annual incidence of neurosyphilis varies from 0.16 to 2.1 per 100,000 people. 1
Syphilis is a chronic infectious disease caused by the bacterium Treponema pallidum.1–3 Neurosyphilis is an infection of the central nervous system caused by T. pallidum. Neurosyphilis can occur at any stage of syphilis, and its most common type is asymptomatic neurosyphilis (ANS).2,4–7 ANS is characterized by the presence of one or more cerebrospinal fluid (CSF) abnormalities, such as pleocytosis, elevated protein concentration, or a reactive CSF Venereal Disease Research Laboratory test, in patients with serological evidence of syphilis but no neurological signs or symptoms.5,8 The preferred treatment for syphilis is penicillin G benzathine. 9 An appropriate serological response in syphilis has been defined by the Centers for Disease Control and Prevention as a fourfold or more decline in titers of nontreponemal assays, such as the rapid plasma reagin (RPR) test, which is performed 6-12 months after initiation of the treatment. Approximately 20% of patients with early syphilis do not exhibit an appropriate serological response after treatment despite the absence of any clinical evidence of treatment failure or reinfection. This condition is called “serofast syphilis” or “serological non-response syphilis.”10,11 The occurrence of a persistent infection or neurosyphilis in these patients remains controversial.
In China, the incidence of serofast syphilis is approximately 34.4%, and according to reports, the incidence of ANS in patients with serofast syphilis is approximately 34.6%.11,12 To date, only a limited number of studies have examined the relationship between improper serological response after therapy and risk of neurosyphilis.11–14 As the relationship between improper serological response and neurosyphilis remains unclear, the factors that increase the risk of neurosyphilis in patients with serological non-response syphilis remain unknown.
Thus, this study explored the incidence of ANS in 324 asymptomatic patients with serological non-response syphilis to examine the factors associated with ANS.
Methods
Sample selection
The participants were enrolled in the study from the clinical database of January 2015 to December 2018 of the Beijing Youan Hospital (Beijing, China).The eligibility criteria were 1) age greater than or equal to 18 years, 2) HIV-negative status, and 3) serological non-response syphilis status: defined as a < fourfold decline in nontreponemal antibody titers at ≥ six months after treatment for early syphilis or ≥ 12 months after treatment for late latent syphilis or persistently low positive titers without evidence of treatment failure, even with an initial ≥ fourfold decline.9,10 The eligibility criteria were independently assessed by certified clinicians. 8 Finally, 324 eligible participants were included in the statistical analyses, all of whom underwent lumbar puncture.. Ethical approval was obtained from the Institutional Review Board of Beijing Youan Hospital.
Laboratory methods and demographic data collection
Laboratory analyses, including the RPR (Shanghai Rongsheng Biological Pharmaceutical Co., Ltd, Shanghai, China) and T. pallidum particle agglutination tests (Fujirebio, Tokyo, Japan), were conducted according to manufacturer's instructions. Demographic data, including age, biological gender, ethnicity, and marital status, were collected after diagnosis of syphilis.
Measures
The outcome of interest was the incidence of ANS in Chinese patients with serological non-response syphilis. ANS was indicated by 1) a CSF white blood cell count exceeding 0.005 × 109 cells/L and/or 2) a CSF protein concentration exceeding 0.45 g/L. Additionally, all patients with ANS tested positive for CSF RPR.
Statistical analysis
We conducted descriptive statistical analysis stratified by the presence of ANS for the basic characteristics of samples. Bivariate analysis was conducted to assess correlations between outcomes and potential predictors. Significant variables of the bivariate analysis (p<0.1) were entered into multivariable logistic regression models. All p-values were two-sided with a significance threshold of p<0.05. All analyses were conducted using the IBM SPSS statistics software (version 22.0, IBM Corp, Armonk, NY, USA).
Results
Sample characteristics
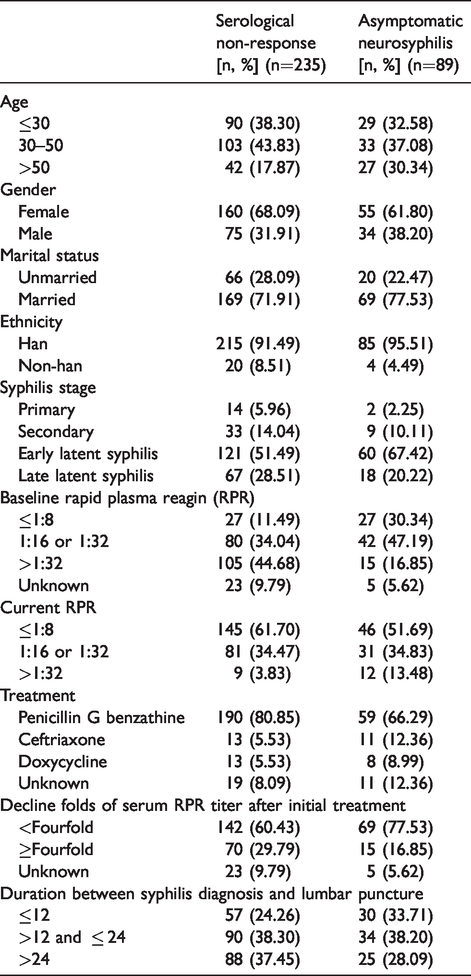
Out of the 324 patients, 27.5% (89/324) were diagnosed with ANS. All patients were previously treated with penicillin G benzathine (2.4 million units IM in a single dose) or ceftriaxone (1-2 g daily either IM or IV for 10-14 days) or doxycycline (100 mg orally twice daily for 14 days), 8 but some of them misplaced their medical treatment records. Therefore, we considered the treatment of such patients as “unknown”. Among the included participants, 42% (136/324) were middle-aged and 66.4% (215/324) were females. Around three quarters were married, and their partners were tested and treated if they were infected. Baseline serum RPR, current serum RPR (when lumbar puncture was undertaken), decline in serum RPR titers after initial treatment, and duration between syphilis diagnosis and lumbar puncture were calculated. We calculated the mean and standard deviation (SD) of the time interval between syphilis diagnosis and lumbar puncture (mean =29.58, SD=21.05). Other detailed information on sample characteristics are included in Table 1.
Characteristics of the included participants.
Factors associated with ANS
Table 2 shows results from the bi-variate and multivariate analyses for factors associated with ANS. Final multi-variable logistic regression model showed that current RPR > 1:32 (aOR=3.461, p=0.031) was significantly associated with higher odds of ANS while a > fourfold decrease in RPR titer after treatment (aOR=0.456, p=0.046) was significantly associated with lower odds of ANS. However, other factors, such as gender, marital status, therapeutic regimen, time interval between syphilis diagnosis and lumbar puncture, were not relevant for ANS development.
Summary of factors associated with ANS in bivariate and multivariate analyses.
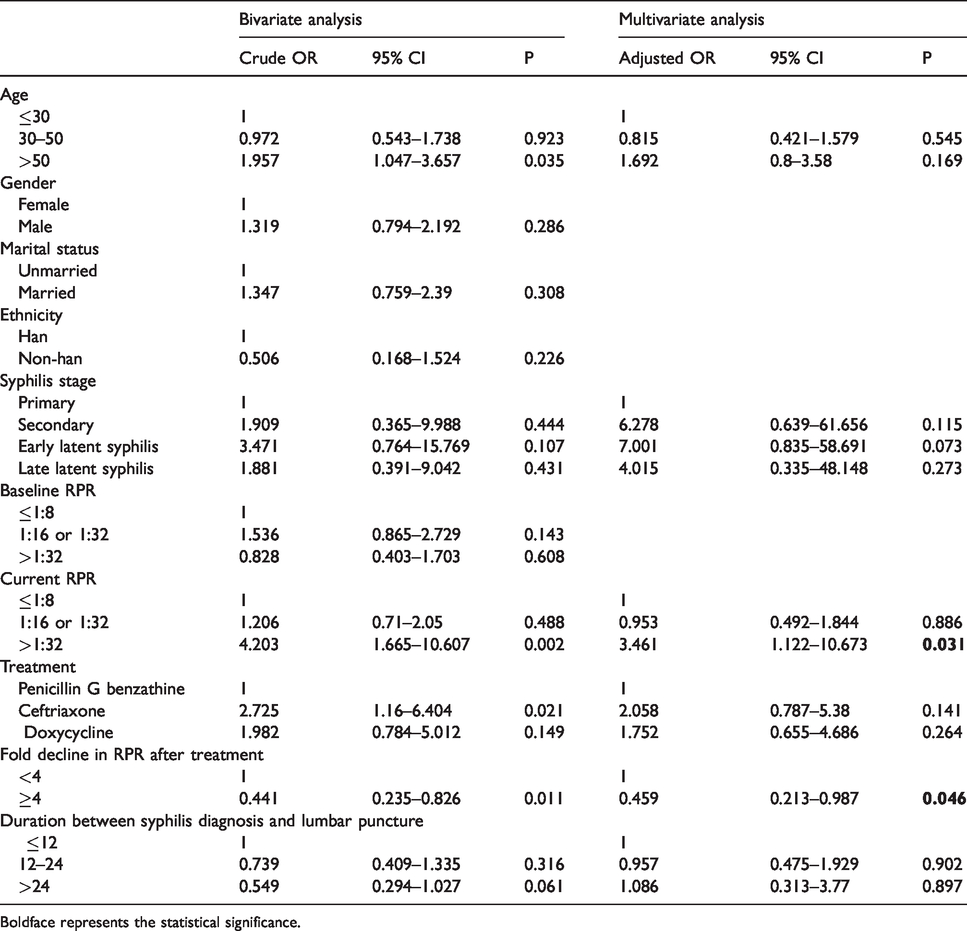
Boldface represents the statistical significance.
Discussion
The results indicated that 89 of 324 patients had ANS (incidence of 27.5%), and the most significant risk factors were a less than fourfold decrease in serum RPR titers after treatment and current serum RPR titers >1:32.
Studies have documented the incidence of neurosyphilis at different stages of syphilis (primary, secondary, and latent) or among various populations (HIV-negative, HIV-positive), and risk factors for neurosyphilis in HIV-negative and/or HIV-positive patients with syphilis have been described.13,14 ANS is a type of neurosyphilis15,16 whose diagnosis depends on the patient's medical history and laboratory examinations.5,13 ANS is difficult to diagnose, and only a limited number of studies have examined its incidence and associated factors. However, these studies have yielded inconclusive results. Thus, the associated factors remain largely unknown. Some studies demonstrated that the serological non-response state was common in syphilis with an incidence rate of 35.2%–44.4%. A certain relationship exists between ANS and the serofast state, and it has been reported that the incidence of ANS among patients with serofast syphilis in China is 34.6%. 11 However, the factors linking ANS to the serofast or serological non-response state require further investigation. Our results indicated that 89 of 324 serological non-response syphilis patients (27.5%) had ANS, and this incidence rate exceeded that of patients with latent syphilis (13.5%) or syphilis at any stage (13.5%), indicating that ANS is common among patients with serological non-response syphilis. In contrast, the incidence was lower than previously reported (34.6%). 11 The difference in results of the two studies may be attributed to the small sample size of our study. ANS among patients with serofast syphilis should be given more attention by clinicians. If there is no requirement for lumbar puncture, identification of relevant risk factors is clinically significant and should be conducted.
The most common finding in ANS patients was an abnormal CSF white blood cell (WBC) count, occurring in 84.27% of the 89 patients. This was consistent with the frequent occurrence of CSF WBC count abnormalities in serological non-response neurosyphilis patients. Thus, an abnormal CSF WBC count had a high diagnostic value for both ANS and neurosyphilis.
Our results indicated that patients with serological non-response syphilis and a serum RPR titer ≥ 1:32 had a high risk of ANS, which is inconsistent with a previous report. 11 Several studies have used a ≥ fourfold decline in six months as a serological cure criterion for treatment. However, in our study, 26.2% (85/324) patients experienced a ≥ fourfold decline in serum RPR titers after treatment, but 17.65% (15/85) of them developed ANS, indicating that this criterion may be inappropriate for determining serological cure. Our results indicated that patients with serum RPR titers ≥ 1:32 had a 3.45-fold higher risk of ANS, and those with a ≥ fourfold decrease in serum RPR titers after treatment were less likely to develop ANS. Conversely, age and gender had no correlation with the occurrence of ANS, which was different from that of HIV-positive patients. 14 Although the incidence of ANS in patients aged > 50 years was higher than that in other age groups, the difference was not statistically significant. Furthermore, the incidence of ANS was higher in males (45.3%) than in females (35.4%), but the difference was not statistically significant.
This study had several limitations. Owing to the small sample size, statistical power might be insufficient to identify significant results of some factors. Additionally, the study was retrospective, and a lack of multi-centered research data could have led to potential bias in the results. Other confounding factors may have also affected the results. Several studies17,18 have reported that the Treponema pallidum particle agglutination assay titer and concentration of CXCL-13 in CSF are factors associated with neurosyphilis. However, our study did not evaluate these factors. In future studies, we will aim to incorporate these markers. In addition, although we compared the time interval between syphilis diagnosis and lumbar puncture, we could not determine the time at which the serum RPR titers changed relative to the time of development of neurosyphilis.
Patients with a < fourfold decrease in serum RPR titers after treatment and current serum RPR titers of > 1:32 are more likely to develop ANS. These patients should receive recommendations to undergo lumbar puncture and neurosyphilis treatment to prevent the development of asymptomatic neurosyphilis. Our findings can guide clinicians to a certain degree to identify ANS in patients with serofast syphilis.
Footnotes
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Beijing Hospitals Authority Youth Program (QML20181701) and the National 13th Five-Year Grand Program on Key Infectious Disease Control (2017ZX10202101-004-001).