
Abstract
Background: The pathogenesis of penile intraepithelial neoplasia (PeIN) is unclear but human papillomavirus (HPV) infection and polymorphisms in human leucocyte antigen (HLA). Objectives: To examine the prevalence of HPV DNA and HLA in PeIN. Methods: Adult Caucasian men with a clinical and histological diagnosis of PeIN, that is, Bowenoid papulosis (BP), Bowen’s disease of penis (BDP) and erythroplasia of Queyrat (EQ) were selected and phenotyped from the clinical records. DNA was extracted from blood and paraffin-embedded sections for HLA and HPV typing, respectively. Human leucocyte antigen allele frequencies were compared with those derived from the UK–based Caucasian population. Results: Seventy-two cases of PeIN (20 BP, 34 BDP and 18 EQ) were studied. Human papillomavirus DNA was identified in 65/72 (90.2%) PeIN; Alphapapillomavirus types were detected in 62/72 (85%) followed by Betapapillomavirus types in 9/72 (12.5%) and cutaneous types in 7/72 (9.7%); HPV16 was the most prevalent genotype at 35/72 (48.6%) followed by HPV33 at 7/72 (9.7%); multiple infections were seen in 18/72 (25%) PeIN. HLA-C*15 (Bonferroni corrected p = 0.049) confers susceptibility to PeIN, whereas HLA-DQA1*01 (corrected p = 0.02) protects against PeIN. HPV16-associated PeIN cases showed no statistically significant association with HLA genotype after multiple corrections. Conclusion: Human papillomavirus is involved in the pathogenesis of PeIN. Immunogenotype may play a role in the pathogenesis of PeIN.
Introduction
The aetiology of penile intraepithelial neoplasia (PeIN) is uncertain, but important factors can be identified. These include environmental factors such as phimosis, smoking (tar metabolites in urine), immunosuppression, male genital lichen sclerosus (MGLSc), human papillomavirus (HPV) infection and immunogenotype.
A high prevalence of HPV DNA has been found in PeIN lesions with HPV16, the most prevalent type detected.1–4 Co-infection with HPV 16 was seen in 88% of lesions and 50% had types 39 or 51 present. HPV8 were found in erythroplasia of Queyrat (EQ). 1 It is probable that different HPV types can result in subtype-specific clinical expression of either EQ, Bowenoid papulosis (BP) or Bowen’s disease of penis (BDP) – and that the common factor is the oncogenic nature of the infecting virus. In most cases, genital HPV infections are transient and asymptomatic with only a small proportion developing persistent infection. Human papillomavirus alone is not thought to lead to neoplastic change, and other cofactors such as smoking, dietary, hormonal factors and immunogenetics are thought to be involved. 5
The human leucocyte antigen (HLA) genes located within the human major histocompatibility complex on the short arm of chromosome 6 (6p21.3) encode molecules that play an important role in regulating T cell responses to viral proteins. Different HLA alleles present different peptides to the immune system, and it is likely that the range of alleles inherited by an individual is significant in determining the outcome of the viral infection. Certain HLA alleles have been associated with susceptibility or protection to HPV infection and related cancer, such as cervical cancer, head and neck cancers and non-melanoma skin cancer. 6 In this study, we examine the prevalence of HPV DNA and HLA in PeIN.
Materials and methods
Ethical considerations
Ethical approval was obtained through the National Health Service (NHS) Research Ethics Service (NRES); NRES Committee London – Riverside, Research Ethics Committee references 07/H0706/58, amendment number 2.2. Research governance was secured from and assured by the Research and Development Department at the Chelsea and Westminster and University College Hospitals London NHS Foundation Trusts.
Patients
Adult men with a clinical and histological diagnosis of PeIN were selected using simple, non-random (sequential) sampling between July 2011 and September 2012 from attendances at the specialized Male Genital Dermatoses Clinics, Chelsea and Westminster and University College Hospitals, London.
Human papillomavirus typing
DNA was extracted from archival formalin-fixed and paraffin-embedded tissue by using standard Qiagen protocols, with the addition of the following stringent anti-contamination procedures: extended tissue lysis, a longer elution time and a smaller elution volume. Human papillomavirus typings were performed using Luminex-based platform (HSL-PCR/MPG), two separate commercial reverse hybridization line probe assays and HPV SPF10- DEIA-LiPA25 system, version 1 (based on licenced Innogenetics technology); Labo Biomedical Products, Rijswijk, the Netherlands.6–9 The Alphapapillomavirus genus HPV types tested include HPV 16, HPV18, HPV31, HPV33, HPV35, HPV39, HPV45, HPV51, HPV52, HPV56, HPV58, HPV59, HPV66, HPV68 and HPV70 and low-risk HPV types 6, HPV11, HPV34, HPV40, HPV42–44, HPV53, HPV54 and HPV74. The Betapapillomavirus tested includes HPV5, HPV8, HPV9, HPV12, HPV14, HPV15, HPV17, HPV19, HPV20, HPV21, HPV22, HPV23, HPV24, HPV25, HPV36, HPV37, HPV38, HPV47, HPV49, HPV75, HPV76, HPV80, HPV92, HPV93 and HPV96. Cutaneous genus HPV types include HPV1, HPV2, HPV3, HPV4, HPV7, HPV10, HPV27, HPV29, HPV40, HPV41, HPV43, HPV48, HPV50, HPV57, HPV60, HPV63, HPV65, HPV77, HPV88, HPV91, HPV 94 and HPV95). We have studied all HPV types as an unbiased, comprehensive approach to allow better understanding of the prevalence of HPV in PeIN. Multiple infections are defined as more than one of any of the HPV types.
Human leucocyte antigen tissue typing
DNA was extracted from fresh frozen whole-blood specimens, using standard Qiagen protocols (Qiagen, Crawley, UK) 10 and underwent HLA typing by a validated laboratory (Anthony Nolan Histocompatibility Laboratories, London), using sequence-specific oligonucleotide, probes which were used for HLA typing on a commercial Luminex-based platform (One Lambda LABtype SSO typing, VH Bio, Gateshead, UK). The genes/loci that were tested were HLA-A, -B, -C, -DRB1, -DQB1 and –DQA1. The Allele Frequency Net Database provides online resource for the storage of frequency data on the polymorphisms of several immune-related genes including HLA. 11 The database was used, and specific criteria (e.g. only Caucasian individuals from UK-based populations) were used to match the study population. The population of controls in each HLA gene studied will vary depending on the published reference used as not all references were tested for all loci, that is, Carter database with a sample size of 5024 was used as control for loci HLA-A, -B, -C and –DRB1; Thomson et al. database with a sample size of 537 was used as a control for loci HLA-DQA1 and Doherty et al. database with a sample size of 177 was used as a control for HLA-DQB1.12–14
Statistics
Descriptive and analytical statistics for HPV and HLA data were computed with the use of software programmes: Microsoft Excel and Statistical Package for the Social Sciences, version 20 and Epi Info (Centres for Disease Control and Prevention http://www.cdc.gov/epiinfo/ (downloaded 1 October 2010)). For categorical data, the chi-squared test was utilized together with Yates’ correction for continuity, or Fisher’s exact tests (two-tailed) were used to compare two groups. Advice regarding HLA allele counting and immunophenotypic analysis was provided by the Anthony Nolan Histocompatibility Laboratory. A substantial Bonferroni correction for multiple testing was applied to each HLA analysis, to account for all potential allele comparisons. Corrected p-values of less than 0.05 were regarded as significant.
Results
Seventy-two cases of PeIN (20 BP, 34 BDP and 18 EQ) were studied. The median age at presentation for BP, BDP and EQ was 33.5, 47.5 and 44.5 years, respectively: patients with BP were younger than those with BDP and EQ; 59/72 (81.9%) PeIN patients were uncircumcised at presentation; 16/72 (22.2%) were smokers; 23/72 (31.9%) cases of PeIN had a history of immunodysfunction: 12/72 (16.6%) were HIV-positive (all received combined antiretroviral therapy) and 10/72 (13.9%) had other immunosuppressive disorders.
Human leucocyte tissue typing data
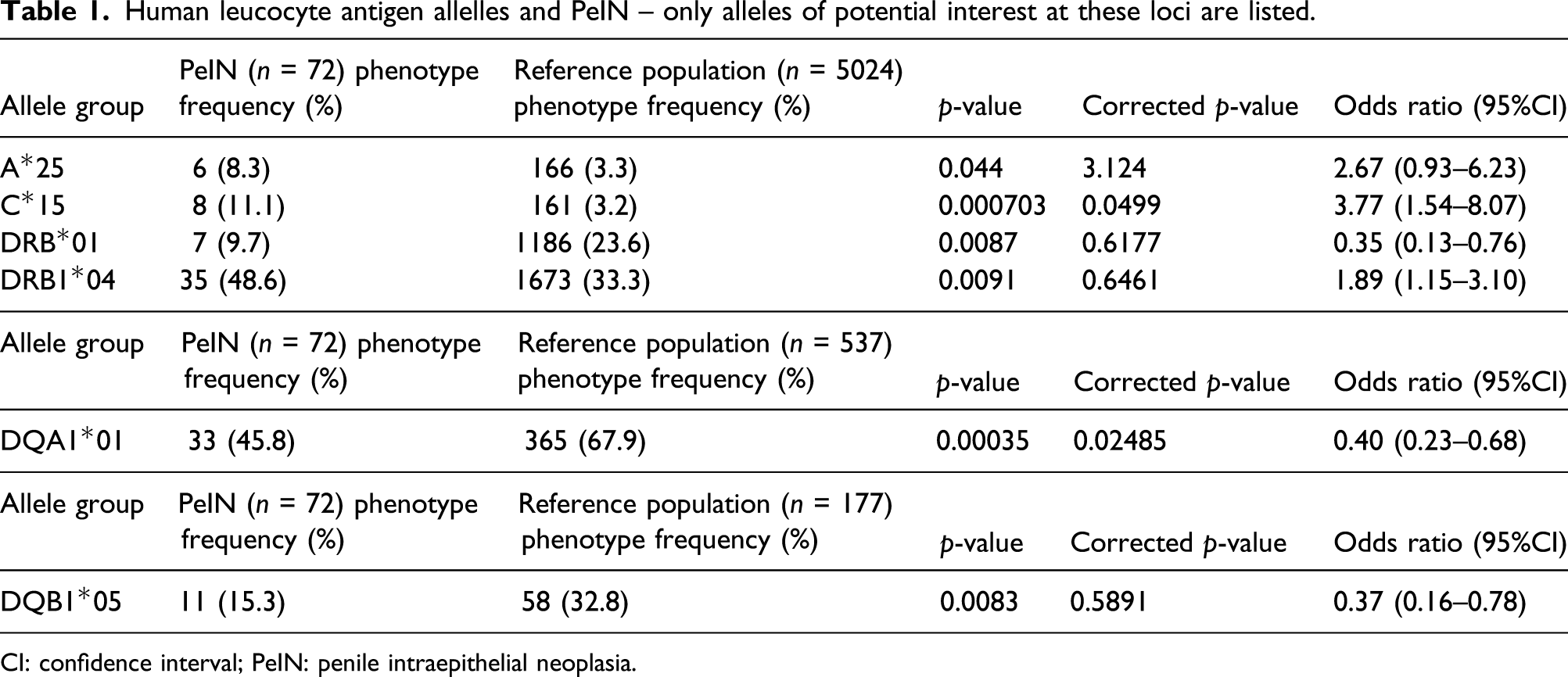
The HLA data were analysed in two ways: PeIN as a whole and subtype analyses. Only those alleles that showed significant differences between the patient and control group that have been investigated are shown (Table 1). PeIN. Compared with the control group, there were no significant differences in the allele frequency in HLA-B. There was a significant increase in frequency of HLA-A*25 (p = 0.044, with Yates’ correction), -DRB1*01 (p = 0.0087, with Yates’ correction) and -DRB1*04 (p = 0.0091, with Yates’ correction), but the statistical significance was lost after Bonferroni correction. Allele HLA-C*15 was statistically significant with Yates’ correction (p = 0.00035) and after Bonferroni correction (p = 0.049) confers increased risk of PeIN. There was a reduced frequency of HLA-DQB1*05 in the patient group significant with Yates’ correction (p = 0.0083). Only allele HLA-DQA1*01 showed statistically significant differences with Yates’ correction (p = 0.00035) and after Bonferroni correction (p = 0.02). Subtypes of PeIN. For BP, allele HLA-A*29 (p = 0.024, with Yates’ correction), -B*44 (p = 0.0035, with Yates’ correction) and -B*56 (p = 0.049, with Yates’ correction) were more frequent in cases than controls; these statistical differences were lost after Bonferroni correction. For BDP, allele HLA-A*25 (p = 0.024, with Yates’ correction) and -C*15 (p = 0.0011, with Yates’ correction) were more frequent than controls but not after Bonferroni correction. There was a reduced frequency of HLA-DQA1*01 in the patient group significant with Yates’ correction (p = 0.013). For EQ, regarding the HLA-B loci, there was a significantly increased frequency of HLA-B*13 (p = 0.0014, with Yates’ correction), -B*40 (p = 0.022, with Yates’ correction) and -B*51 (p = 0.049, with Yates’ correction). Other allele such as HLA-C*15 (p = 0.011; with Yates’ correction) and -DQA1*02 (p = 0.026, with Yates’ correction) were also increased in frequency. None were statistically significant after correction. Human leucocyte antigen allelles and PeIN – only alleles of potential interest at these loci are listed. CI: confidence interval; PeIN: penile intraepithelial neoplasia.
Human papillomavirus typing data
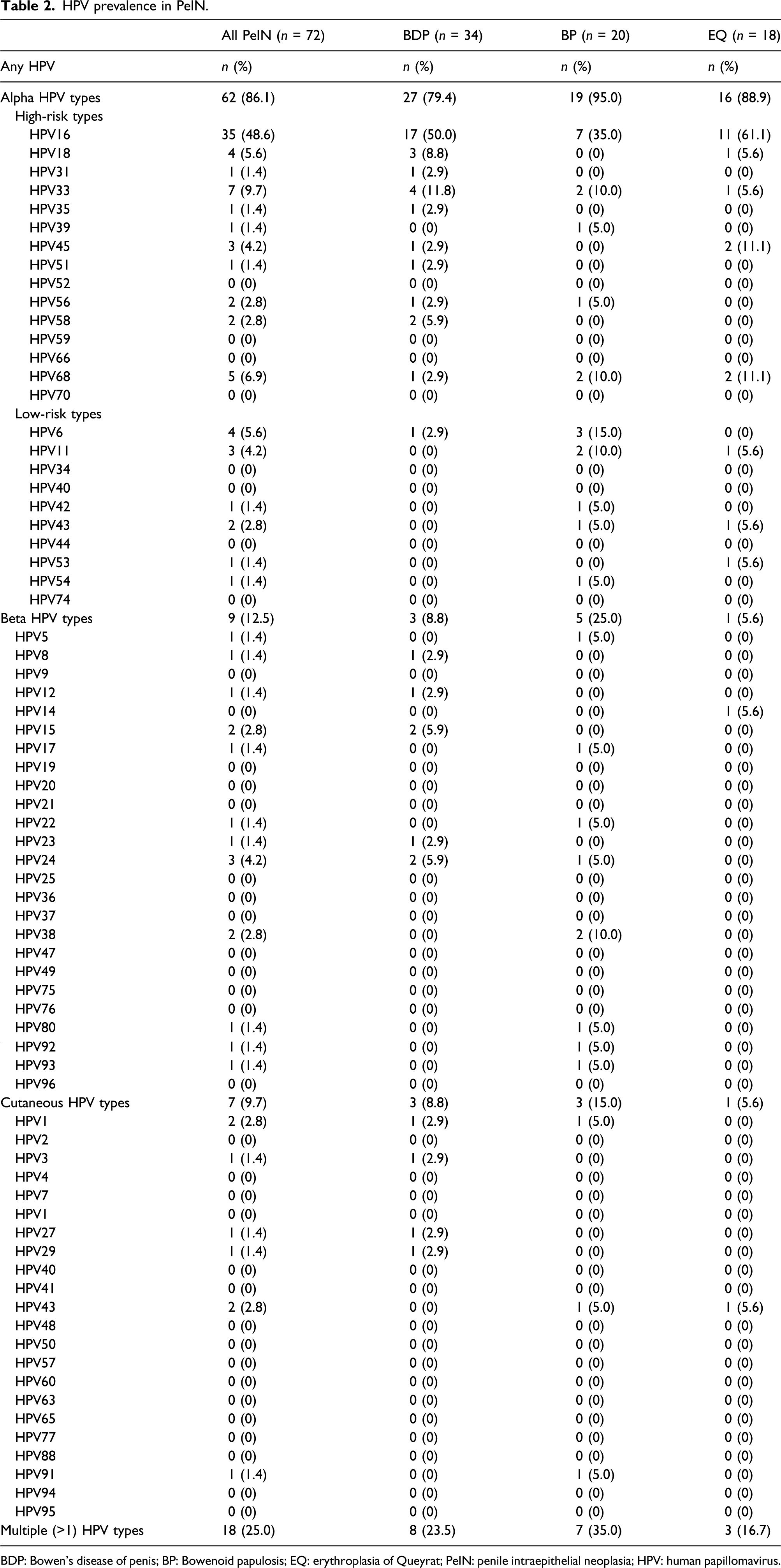
Human papillomavirus results for PeIN have been reported in two ways: (1) PeIN as a whole and (2) subtypes of PeIN. PeIN. Human papillomavirus was detected in 65/72 (90.2%) cases of PeIN. Alphapapillomavirus types were detected in 62/72 (86.1%) followed by Betapapillomavirus types in 9/72 (12.5%) and cutaneous (wart) HPV types in 7/72 (9.7%); HPV16 was the most prevalent genotype at 35/72 (48.6%) followed by HPV33 at 7/72 (9.7%). Multiple infections were seen in 18/72 (25%) PeIN: 8/34 (23.5%) BDP, 7/20 (35%) BP and 3/18 (16.7%) EQ. Male genital lichen sclerosus was seen in 25/72 (34.7%) of PeIN: 5/20 (25%) of BP, 9/34 (26.5%) of BDP and 11/18 (61.1%) of EQ; 19 men with PeIN had neither clinical nor histological evidence of MGLSc or HPV. Subtypes of PeIN (Table 2). In BDP, HPV positivity for all tested HPV types was seen in 30/34 (88.2%) cases, and Alphapapillomavirus types were the most prevalent at 27/34 (79.4%) followed by Betapapillomavirus types at 3/34 (8.8%) and cutaneous (wart) type at 3/34 (8.8%). HPV16 is the most prevalent at 17/34 (50%) followed by HPV33 at 4/34 (11.8%) and HPV18 at 3/34 (8.8%). In BP, 19/20 (95%) cases were positive for all tested HPV, and Alphapapillomavirus types were the most prevalent at 19/20 (95%) followed by Betapapillomavirus types at 5/20 (25%) and cutaneous (wart) HPV types at 3/20 (15%). HPV16 is the most prevalent at 7/20 (35%) followed by HPV6 at 3/20 (15%). In EQ, HPV positivity for all tested HPV types was reported in 16/18 (88.9%) cases, and Alphapapillomavirus types were the most prevalent at 16/88 (88.9%) followed by beta type at 1/18 (5.6%) and cutaneous (wart) type at 1/18 (5.6%). HPV16 is the most prevalent at 11/18 (61.1%) followed by HPV 45 at 2/18 (11.1%) and HPV68 or 73 at 2/18 (11.1%). HPV prevalence in PeIN. BDP: Bowen’s disease of penis; BP: Bowenoid papulosis; EQ: erythroplasia of Queyrat; PeIN: penile intraepithelial neoplasia; HPV: human papillomavirus.
Human leucocyte antigen and human papillomavirus interaction data
Subgroup analysis has been performed according to HPV16 infection status because this oncogenic type was the most prevalent genotype seen in this work. Further analyses for other HPV types were not attempted as the numbers were too small.
Increased frequencies of HLA-C*15, -DQA1*02 and -DQA1*03 were observed in all HPV16-infected PeIN cases compared with controls, and this was statistically significant (p = 0.0011, 0.0016 and 0.047, respectively). However, the significance was lost following Bonferroni adjustment (corrected p = 0.073, 0.11 and 3.1, respectively).
Discussion
There are currently limited published data on the distribution of HLA and its association with HPV in PeIN. Our work describes a population of PeIN studied virologically and has deployed novel, validated molecular HPV typing techniques capable of detecting a broad spectrum of HPV types -73 in all non-genital cutaneous (wart), genital and beta HPVs.
A high prevalence of MGLSc (61.1%) in EQ was reported in our study consistent with previous findings. 15 It may be that uncircumcised men with preputial dermatoses are exposed to a local carcinogenic influence such as chronic inflammation or other environmental or excreted carcinogens (as in smokers). Some authors have observed that warty or basaloid undifferentiated PeIN is occasionally encountered on a background of MGLSc. 16 The association between MGLSc and differentiated variants of PeIN has been controversial with most recent studies supporting the association16,17 whilst others do not.18,19 Despite these seemingly contradictory data, there are undoubtedly a significant number of bona fide cases of squamous cell carcinoma of penis arising on a background of LSc, highlighting the importance of maintaining a high level of vigilance particularly in cases of atypical hyperkeratotic lesions associated with MGLSc.
In previous work, HPV has been detected in between 6 and 100% of PeIN lesions.1–4,20 The variation in reported prevalence is likely due to differences in the HPV DNA detection method used and the number and types of HPV tested. Genital types have been always the only HPV subtypes studied with HPV16, the most prevalent type detected.2–4 The prevalence of multiple infections was between 4.3 and 15%.2,20 Our results are consistent with, and strengthen, these previous findings: the overall prevalence of HPV in PeIN in this study was 90.2%. HPV16 was the most prevalent HPV type detected in this work similar to many published studies.2–4 Multiple infections were seen in 25% of PeIN in this study, and this is higher than the published rate between 4.3 and 15%. In our cohort of PeIN with immunodysfunction, high positivity of HPV was seen in 19/23 (82%). HIV patients constituted at least half of the immunocompromised PeIN at 12/23 (52%), among which 9/12 (75%) were positive for HPV.
Several HPV types have been identified in BDP: HPV2, HPV16, HPV18 and HPV34, among which type 16 occurs most frequently.21–23 Our work is the largest cohort of BDP examined for HPV. Our work has shown that HPV16 is the most prevalent at 17/34 (50%). The molecular work has also shown a high prevalence of HPV compared with clinical or histological evidence of HPV in BDP.
Several HPV types have been previously identified in BP: HPV1, HPV2, HPV16, HPV18, HPV31, HPV39 and HPV67, amongst which HPV16 is the most prevalent subtype reported.21,23 Our work constitutes the largest cohort of BP studied. We have also detected a high prevalence of HPV16 consistent with published data. The high positivity of HPV in BP in our work affirms the defining feature of BP to be HPV infection and shows that the molecular positivity is more useful than clinical history and histological sensitivity.
The published literature on HPV typing in EQ is limited. HPV8 coinfection has been implicated in the pathogenesis of EQ in eight patients. 1 Coinfection with HPV16 was seen in 7/8 (88%) of lesions and 4/4 (50%) had types 39 or 51 present. HPV16 and HPV18 were detected in EQ and BDP. 2 HPV16 was detected in several case reports of EQ but absent in some cases. 24 Our work constitutes the largest cohort of EQ to be studied for HPV. Our results are consistent with previously published papers in that HPV16 is the most prevalent subtype seen. The high positivity for HPV is also seen in this molecular investigation compared with clinical or histological evidence of HPV in EQ. Our work has also shown a high prevalence of MGLSc associated with EQ. All these factors might explain the perceived higher risk of squamous carcinogenesis in EQ than those of BDP and BP.
Human papillomavirus is prevalent and infection with it can be difficult to assess. In contrast to other viral infections where the exposure can be documented by a reliable laboratory marker such as virus-specific IgG antibody, a similar marker for HPV exposure does not exist. The roles of beta and cutaneous (wart) types in PeIN are not known as there have been no previous published studies to elucidate this. The significance of multiple HPV subtypes is not fully understood, and the potential role of different detected HPVs as carcinogens or coinfectors has not been explored. 25 It is conceivable that some of these HPV types could be background passenger, rather than driver, HPV.
Another factor that has complicated interpretation of the role of HPV in PeIN is the absence of agreement and lack of consistency and accuracy in the definition and classification of premalignant penile lesions, clinically and histologically. It is difficult to correlate our findings of HPV in PeIN with some of the published literature because the HPV typing techniques and classification of PeIN have varied considerably. In this work, the HPV status has been correlated with the clinical morphology. The most recent consensus from The Royal College of Pathologists advocates (a) the preferential use of the term ‘PeIN’ and (b) its subdivision histologically into differentiated and undifferentiated types. 26 This was not the consensus at the inception of our work so HPV prevalence and subtype analysis have not been correlated directly with the two histological types of PeIN, but the histological type can be inferred from the association with either GLSc or HPV. The majority of the cases studied most likely had undifferentiated PeIN because they were HPV-associated. The HPV negative cases most likely had differentiated PeIN associated with GLSc. Clearly, there are a number of cases with both HPV and GLSc. It is not unreasonable clinically to believe that men with clinical, histological and virological evidence of both GLSc- and HPV-related PeIN are at higher risk of penile squamous cell carcinoma.
This is the first work to investigate host immunogenetics in PeIN. In our work, HLA-C*15 (corrected p = 0.049) appears to confer susceptibility to PeIN, whereas HLA-DQA1*01 (corrected p = 0.02) appears to protect against PeIN. The significance of these is yet to be defined in larger cohort of PeIN. HLA-C*03:03 was found to increase the risk of developing cervical intraepihealial neoplasia (CIN)-2/3, whereas HLA-C*01 was found to confer a protective effect. 27 Although such associations have not been seen here, a limitation is the relatively small number of patients, but PeIN is much less common than CIN so harder to study in number.
Subgroup analyses were performed according to HPV 16 status in this work. Our attention has been drawn to several alleles of potential importance: both HLA-DRB1*07 and -DQB1*05 increase risk of HPV16-infected EQ cases, whereas -DQB1*03 predispose to HPV16-infected BDP cases. Comparable evidence of HPV16 specificity has been seen in CIN and vulvar intraepithelial neoplasia.28,29
As previously discussed, genital HPV infection is extremely common. However, only a small fraction of infections would appear to progress to persistent disease and cancer, suggesting that other determinants contribute to the pathogenesis. One potential cofactor may be the host cellular immune response to HPV infection, mediated by HLA-restricted T lymphocytes. The HLA haplotype of an individual may lead to clearance or predispose to persistence of HPV infection. 30 The exact nature and mechanism whereby host gene products regulating HPV oncogene expression and preventing HPV-induced cell immortalization remain elusive. While certain alleles have a documented detrimental effect on HPV infection, some HLA alleles have a protective role. 31 Human leucocyte antigen typing therefore might be a useful surrogate for immunophenotypic susceptibility and prognostication.
In summary, HPV was identified in 90.2% PeIN. Significant (p < 0.05) HLA associations were (i) susceptibility to PeIN – specifically HPV16-positive PeIN (HLA-C*15, -DQA1*02 and –DQA1*03) and (ii) protection against PeIN (HLA-DQA1*01). The HLA associations and their implications discussed above must remain speculative given the small number of HPV16-positive subjects and the large number of statistical tests performed. The number of subjects analysed is too small to draw any definite conclusions. We are currently collecting additional data in increasing numbers of patients. This is particularly important given the current effort to improve our understanding of the immunophenotypic factors associated with penile precancer and cancer in the development of HPV vaccination and its deployment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Skin Treatment and Research Trust (START) and Sir John Fisher Foundation.