
Abstract
Poor mental health may confer worse health outcomes among people living with HIV/AIDS (PLWH). Suicidal behaviors are symptoms of a depressive episode. The goal was to explore characteristics for spatial distribution and risk factors for suicide among PLWH. This study was conducted in Mainland China with the annual newly reported data of PLWH from 2013 to 2018. We compared the spatial distribution differences between the HIV epidemic and suicide mortality and analyzed the global and local spatial analysis of suicide. Further, we explored the possible risk factors of suicide in PLWH by multivariate regression and a decision tree model. High suicide mortality regions in PLWH in China were inconsistent with that of the high prevalence of PLWH, which showed that there was distribution discordance between the HIV epidemic and suicide mortality. Multivariate regression showed that the possible risk factors of PLWH who committed suicide were younger age, with Han nationality, single, having a higher educational level, and homosexual infection route. The decision tree model showed that age was the primary factor. In conclusion, there was a discordance between HIV prevalence and suicide mortality; lower HIV prevalence regions might have higher mortality due to suicide. Concern is merited amongst PLWH with poor mental health.
Introduction
People living with HIV/AIDS (PLWH) are among the groups that most suffer from mental illnesses. 1 Evidence suggests that depression occurs more commonly in HIV-positive individuals and limits significantly the quality of life. 2 Moreover, large psychological studies reported that a depressive episode might induce suicidal thoughts and behaviors. 3 Based on the systematic analysis for the Global Burden of Disease Study 2017, in the range from ages 20 to 50 years, possibly because of the HIV epidemic, there are increases in adult death rates, possibly related to drug use and suicide. 4 Suicidal behaviors comprise a series of actions, including suicidal ideation, suicidal planning and, suicidal attempts. 5 One study Canadian HIV-positive GBMSM (bisexual and other men who have sex with men) reported that 22.3% (150/671) had suicidal ideation and 4.9% (33/671) had suicidal attempts. 6 A prior study surveyed more than 400 PLWH in Canton, China and found that about 32.8% of the PLWH might have suicidal ideation or attempts. 7 At the same time, there is a continually growing number of newly identified PLWH each year in China. At the end of October 2019, the reported cases of PLWH were 958,000. It is imperative to improve the mental health status of PLWH in China with a focus on suicide among PLWH in China.
The Spatial analysis could visualize the geographic heterogeneity and detect the presence and location of a cluster in confined regions. The effective spatial analysis is conducive to know the comprehensive epidemiological scenarios of suicide among PLWH. While, as to our knowledge, most of the spatial descriptions are more focused on the epidemics of HIV or other chronic infectious diseases, there are no reports on the spatial distribution of suicide among PLWH nationally, which might be different from the epidemics of HIV in China.
Besides, sexual transmission has gradually become the dominant route of HIV infection in China 8 where HIV originated among injection drug users (IDUs). HIV incidence and prevalence is higher in MSM (men who have sex with men) than any other high-risk population in China and continues to increase, particularly in larger, urban areas. 9 As change occurs in the sociological structure of PLWH, the sociological factors that lead to suicide in PLWH may also change. Therefore, it is necessary to know the risk factors for suicide among PLWH in China. Previous studies in other countries suggested that sociodemographic factors (e.g., age, gender, and ethnicity), psychological distress or problems (e.g., depressive disorder, generalized anxiety disorder, previously attempted suicide, and family history of suicide attempts) might be risk factors for suicide, and some Chinese studies had suggested that gender, major depressive symptoms, poor social support, family function, and spouse’s HIV status are associated with suicidal ideation in PLWH. However, there remains a lack of studies examining the risk of PLWH who died of suicide in China, and most of the previous studies concentrated on risk factors of suicidal ideation or attempts among PLWH.
The objective of this study is to describe the spatial characteristics among PLWH who died of suicide in China a investigate the prevalence and possible associated risk factors among PLWH who committed suicide within the dataset over the years 2013 to 2018. This is the first stusy to explore the spatial characteristics and the social risk factors among PLWH who died of suicide with nation-wide data. The findings of this study might address the specific needs of HIV treatment and psychological intervention.
Data collection and management
The data used in this article were annual newly reported data (annual newly reported data were the HIV-positive case first being identified during 2013–2018) obtained from the HIV/AIDS case reporting system (CRS) under the National Center for AIDS/STD Control and Prevention of the Chinese Center for Disease Control and Prevention, (China CDC) between January 2013 and December 2018. The CRS was established in 1985 and became online in 2005. All first identified HIV cases were reported to the Web-based systems either by local hospitals or clinics. Demographic characteristics (age, gender, occupation, ethnicity, etc.), HIV related risk behaviors, and routes of transmission (heterosexual/homosexual/IDU/transfusion of blood/other blood cells) were also collected from all the registered PLWH.
The information about the death (date of death and cause of death) of PLWH was also obtained from the CRS, which was reported by local hospitals or local population management departments where PLWH lived in. Major causes of death were classified into three groups: HIV-related death, non-HIV-related death, and unable to determine. According to the cause of death classification standard of the CRS, HIV-related death included the death induced by HIV opportunistic infection, HIV-related tumors (such as Kaposi’s sarcoma), and HIV-related syndrome. And non-HIV-related deaths included death induced by cardiovascular disease, other malignant tumors, respiratory diseases, endocrine nutritional metabolism diseases, digestive system disease, and other unrelated diseases such as drug overdoses, accidents, suicide, and antiviral treatment side effects. If the cause of death did not belong to the categories in the CRS, then it was regarded as unable to determine.
In our study, we used suicide mortality and the proportion of suicide in death as the main outcomes. Suicide mortality among PLWH was estimated by the number of suicides among PLWH within the reported number of PLWH in the same period. The proportion of suicide among PLWH deaths was estimated by the number of suicides among PLWH within the total death number of PLWH in the same period.
Spatial analysis
To identify the residential locations of the reported and dead HIV infection cases, the corresponding national standard geocodes at the province or city level were included in the analysis. Electronic maps were obtained from the China CDC (CCDC). ArcGIS 10.5 software (ESRI Inc., Redlands, CA, USA) was used to create electronic maps, and R studio 1.1.456 software was used to process and analyze the data.
Statistical analysis
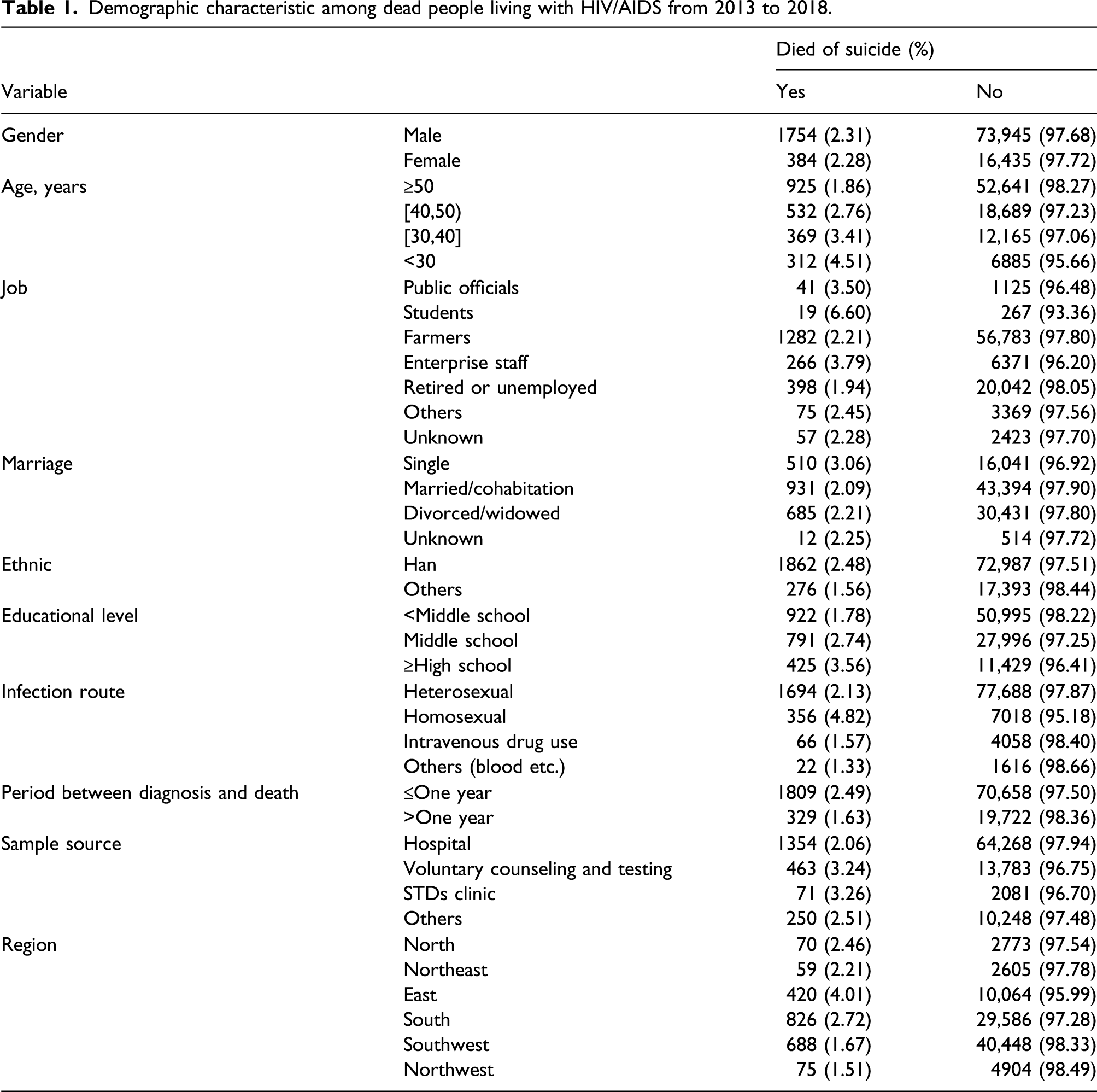
To investigate the presence of factors associated with suicide, we compared social and demographic variables with absolute and relative frequencies (proportions). We analyzed covariates including gender, age (<30, 30–39, 40–49, and ≥50 years old), ethnicity, marital status, occupation, education, HIV transmission route (heterosexual, homosexual, and others), and HIV diagnosis venues (voluntary counseling and testing, hospital, others, and unknown). Univariate and multivariate logistic regression was performed to assess factors associated with suicide. A decision tree model was used to find the most influential variable for factors associated with suicide. Variables with p < 0.05 in univariate analysis were included in the multivariate logistic regression.
General spatial autocorrelation
Assuming the consistent spatial distribution of HIV infection across different cities in China, Moran’s Index (I) was used to measure the patterns (cluster/disperse/random) of distribution of percent of suicide among PLWH throughout the country. Values for Moran’s I ranged from −1 to +1. The pattern of distribution was considered to be clustered if the value of Moran’s I was >0 and Z value was >1.96 or the Moran’s I was <0 and Z value was ≤1.96. Otherwise, the pattern was considered to be random or diverse. 10
Local spatial autocorrelation
The Getis statistics was chosen as the parameter to identify the local clusters in the present study. The meaning of parameters was similar to general Moran’s Index; the Z test was conducted for the Gi parameter. If Z value was >1.96, the local clusters were identified as high-value correlations (statistically significant hotspot, meaning the city had the high percentage of suicide and was surrounded by other cities with a high percentage of suicide as well); and if Z value was ≤1.96, the local clusters can be identified as low-value correlations (statistically significant cold spots, meaning the city had low rates of suicide). Local autocorrelation was conducted at city levels to detect percent of suicide among PLWH hotspots/cold spots among PLWH in China.
Ethical considerations
The data used in this study, from the CRS, and focused on population-level analyses only has been approved by the ethics committee of the NCAIDS, China CDC. Any personal identifiers were removed before data analysis in this study.
Results
Demographic characteristic among dead people living with HIV/AIDS from 2013 to 2018.
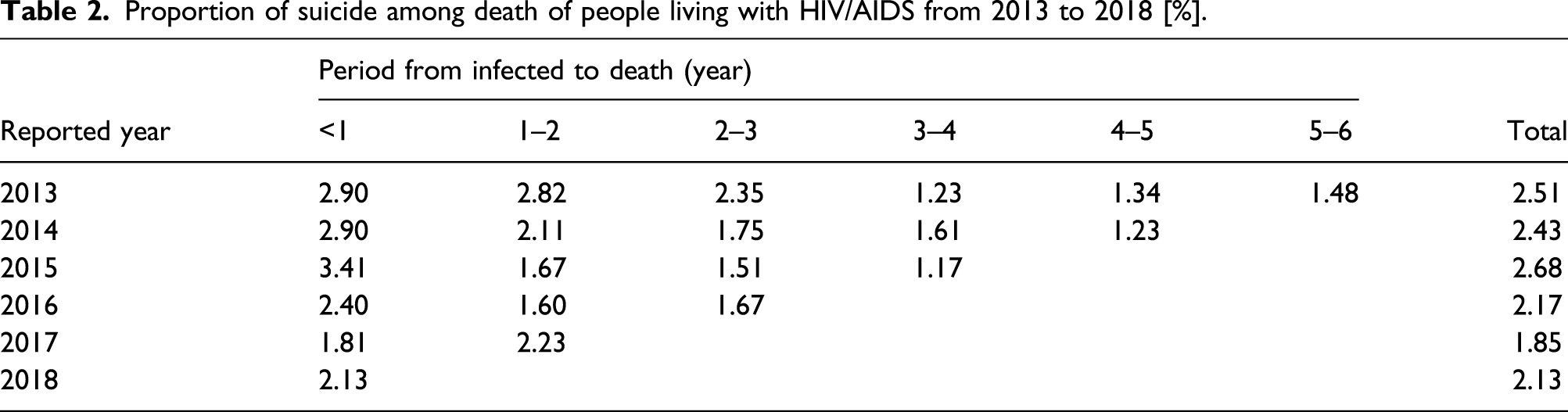
Proportion of suicide among death of people living with HIV/AIDS from 2013 to 2018 [%].
Spatial analysis
Number of report cases and death among people living with HIV/AIDS (PLWH) by province from 2013 to 2018.
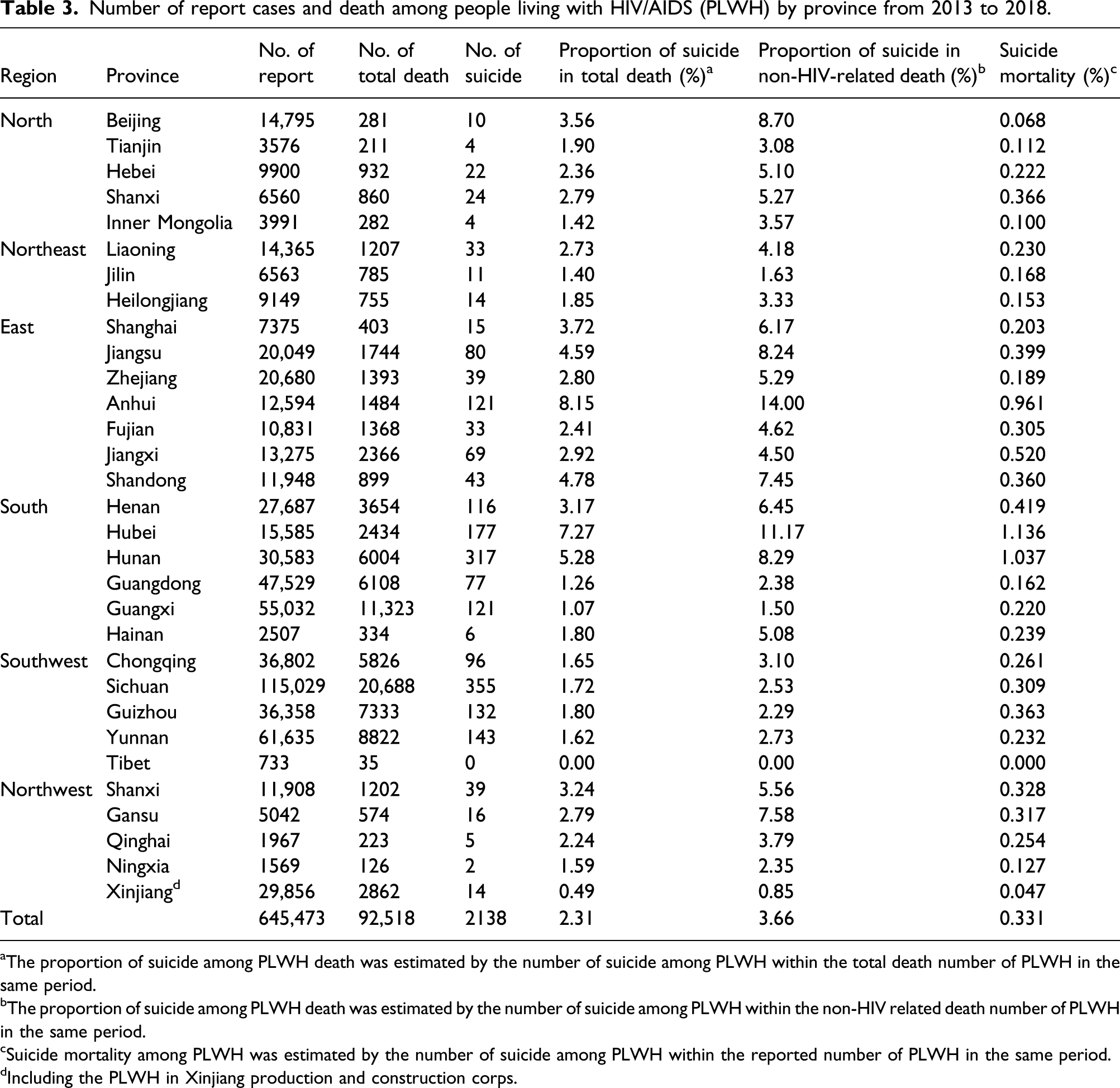
aThe proportion of suicide among PLWH death was estimated by the number of suicide among PLWH within the total death number of PLWH in the same period.
bThe proportion of suicide among PLWH death was estimated by the number of suicide among PLWH within the non-HIV related death number of PLWH in the same period.
cSuicide mortality among PLWH was estimated by the number of suicide among PLWH within the reported number of PLWH in the same period.
dIncluding the PLWH in Xinjiang production and construction corps.
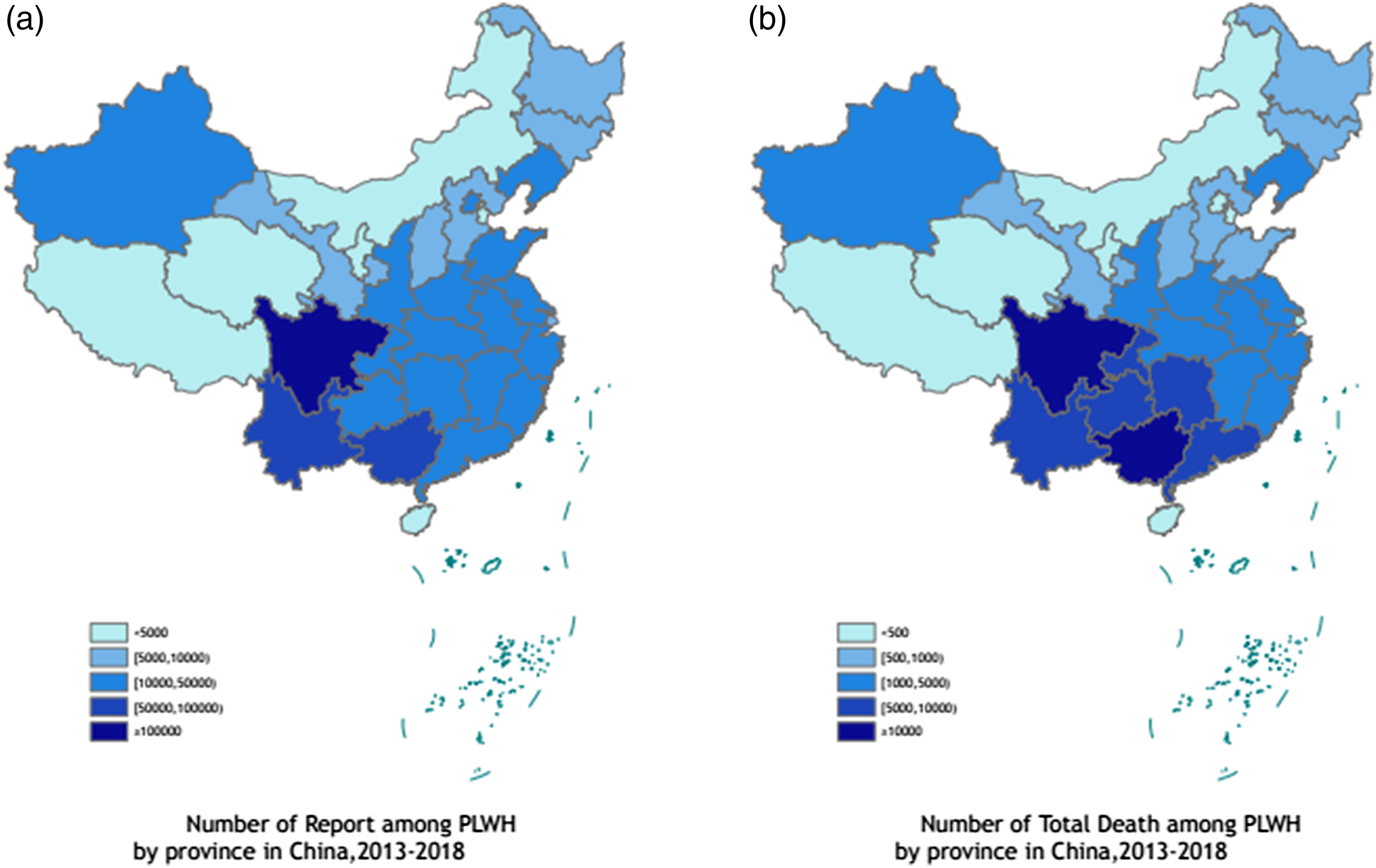
Number of report and death among people living with HIV/AIDS (PLWH) by province in China, 2013–2018. (a) Number of report among PLWH by province in China, 2013–2018. (b) Number of total death among PLWH by province in China, 2013–2018.
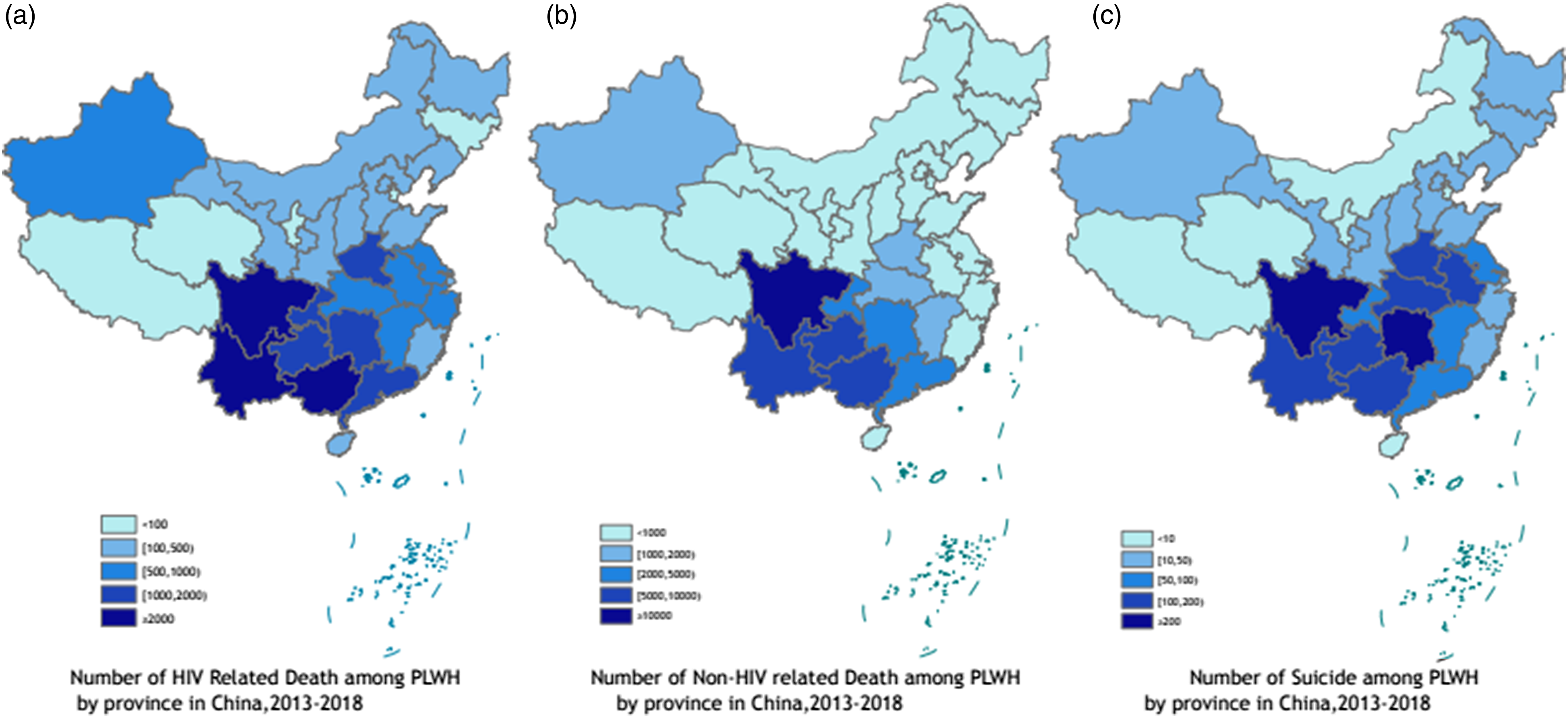
Number of death among people living with HIV/AIDS (PLWH) by province in China, 2013–2018. (a) Number of HIV-related death among PLWH by province in China, 2013–2018. (b) Number of non-HIV-related death among PLWH by province in China, 2013–2018. (c) Number of suicide among PLWH by province in China, 2013–2018.
The geographical distributions of the proportion of suicide in death and suicide mortality were found to be discordant with that of the HIV epidemic in China. Provinces in the southwest of China had a higher prevalence of HIV; regions with a high proportion of suicide in death and suicide mortality were higher in the south or east of China. We found that the top five provinces with the highest suicide mortality were Hubei, Hunan, Anhui, Jiangxi, and Henan, where the suicide mortality was 1.14%, 1.04%, 0.96%, 0.52%, and 0.42%, respectively. Also, the top five provinces with the highest proportion of suicide in death were Anhui, Hubei, Hunan, Shandong, and Jiangsu, where the proportion was 8.15%, 7.27%, 5.28%, 4.78%, and 4.59%, respectively (Table 3 and Figure 3). Percentage of death among people living with HIV/AIDS (PLWH) by province in China, 2013–2018 (%). (a) Percentage of suicide in report (suicide mortality) among PLWH by province in China, 2013–2018 (%). (b) Percentage of suicide in total death among PLWH by province in China, 2013–2018 (%). (c) Percentage of non-HIV-related suicide among PLWH by province in China, 2013–2018 (%).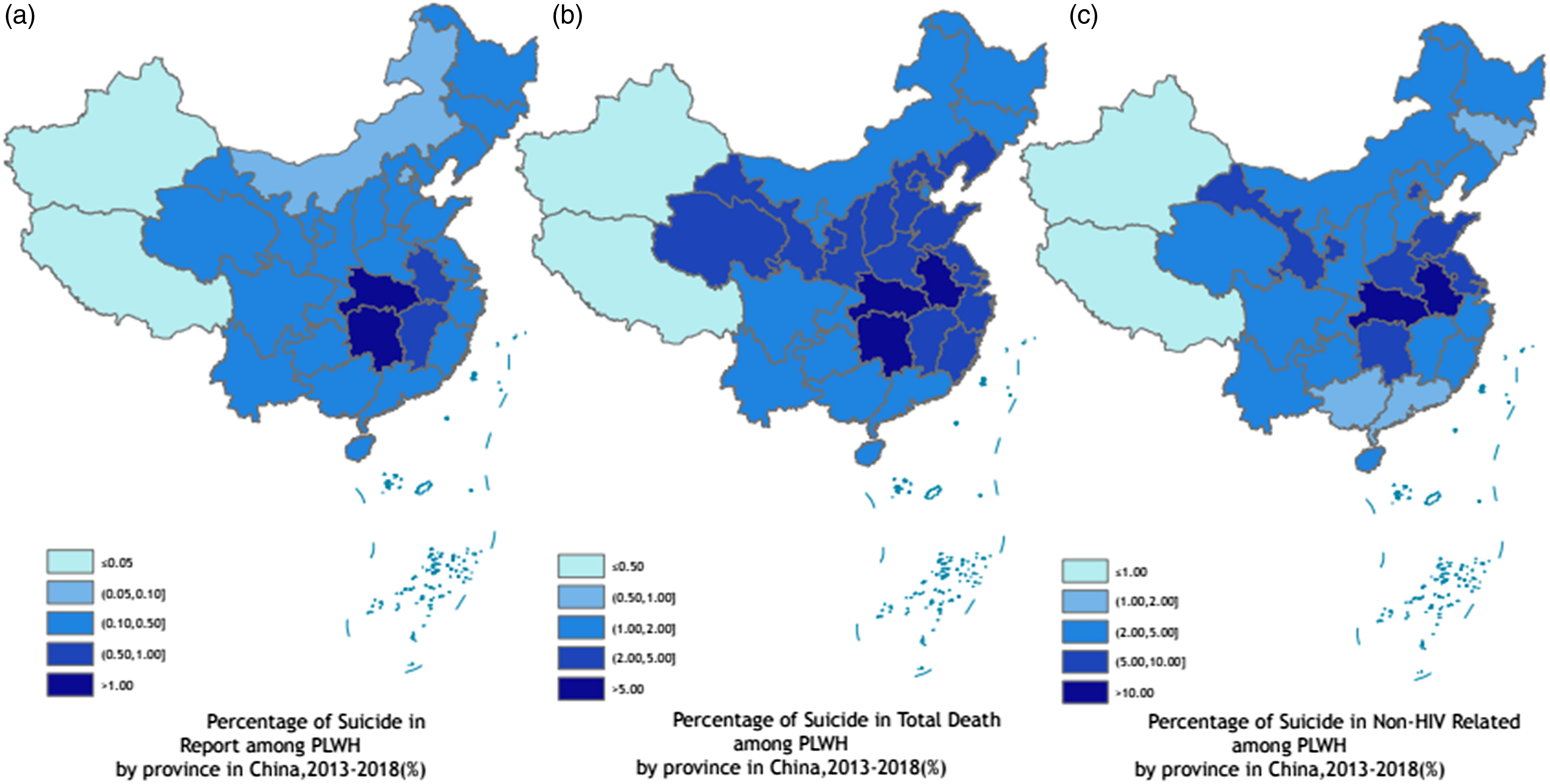
Additionally, general spatial autocorrelation was conducted for the proportion of suicide and suicide mortality reported between 2013 and 2018, and the Moran’s Index was 18.66 (p < 0.001) and 16.32 (p < 0.001), respectively. Local spatial autocorrelation was conducted by using the same matrix as general spatial autocorrelation at city levels to determine the possible hotspots or cold spots. As Figure 4 shows, in general, hotspots for the proportion of suicide at the city level concentrated in the areas located in the south or east of China, such as Hubei and Shandong province, etc. The cold spots were mainly located in three regions (northeast, northwest, and southwest of China) such as Guangxi and Yunnan province, which was consistent with high HIV prevalence areas of China. The hotspots for suicide mortality at the city level were also concentrated in the areas located in the south and east coast of China, but more concentrated in south central China. While the Cold spots were mainly limited in two areas: northeast and northwest of China. Hotspots and cold spots at city level by year in China, 2013–2018. (a) Hotspots and cold spots of suicide in total death among PLWH at city level in China, 2013–2018. (b) Hotspots and cold spots of suicide in report (suicide mortality) among PLWH at city level in China, 2013–2018.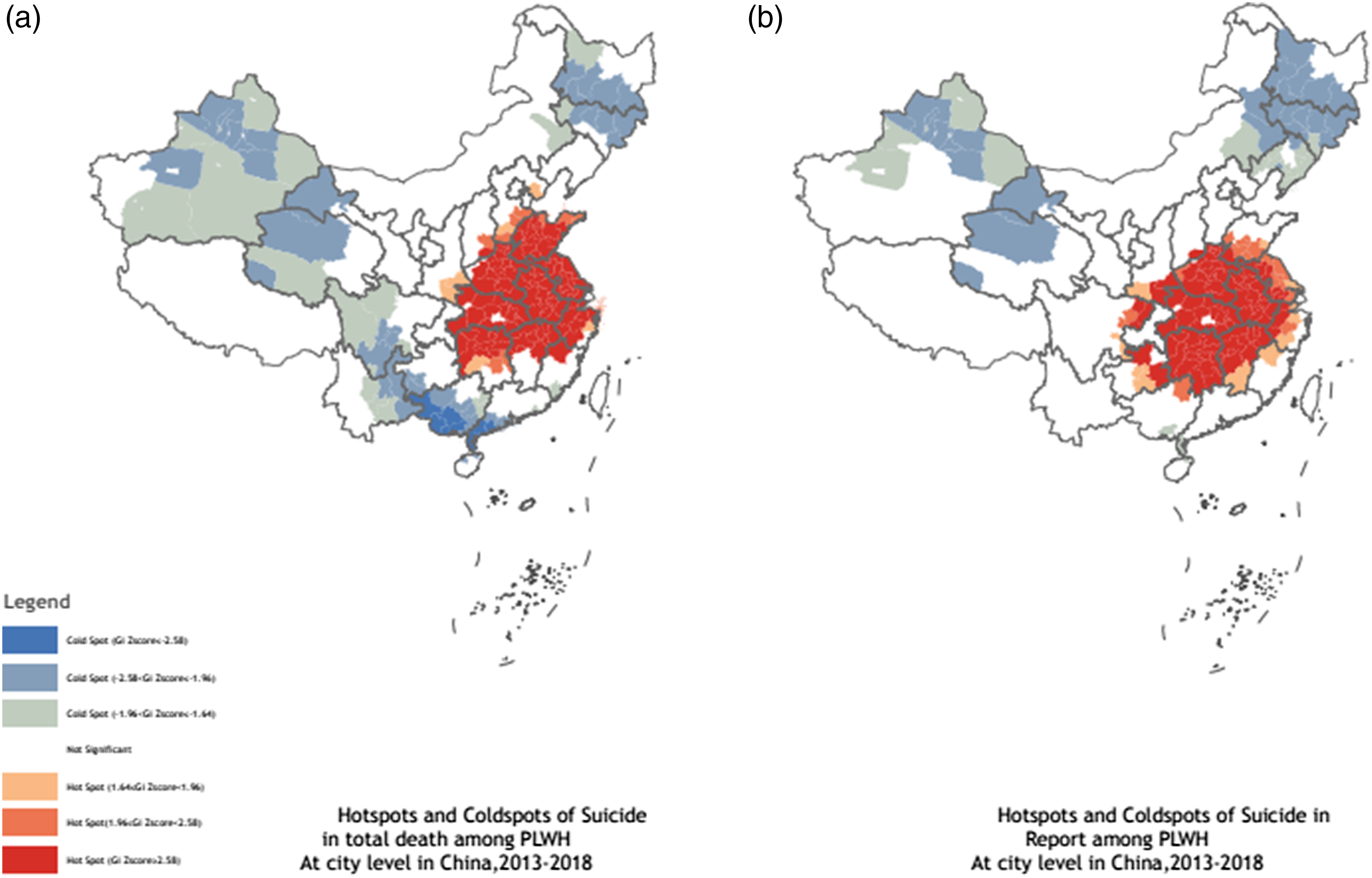
Risk factors for suicide
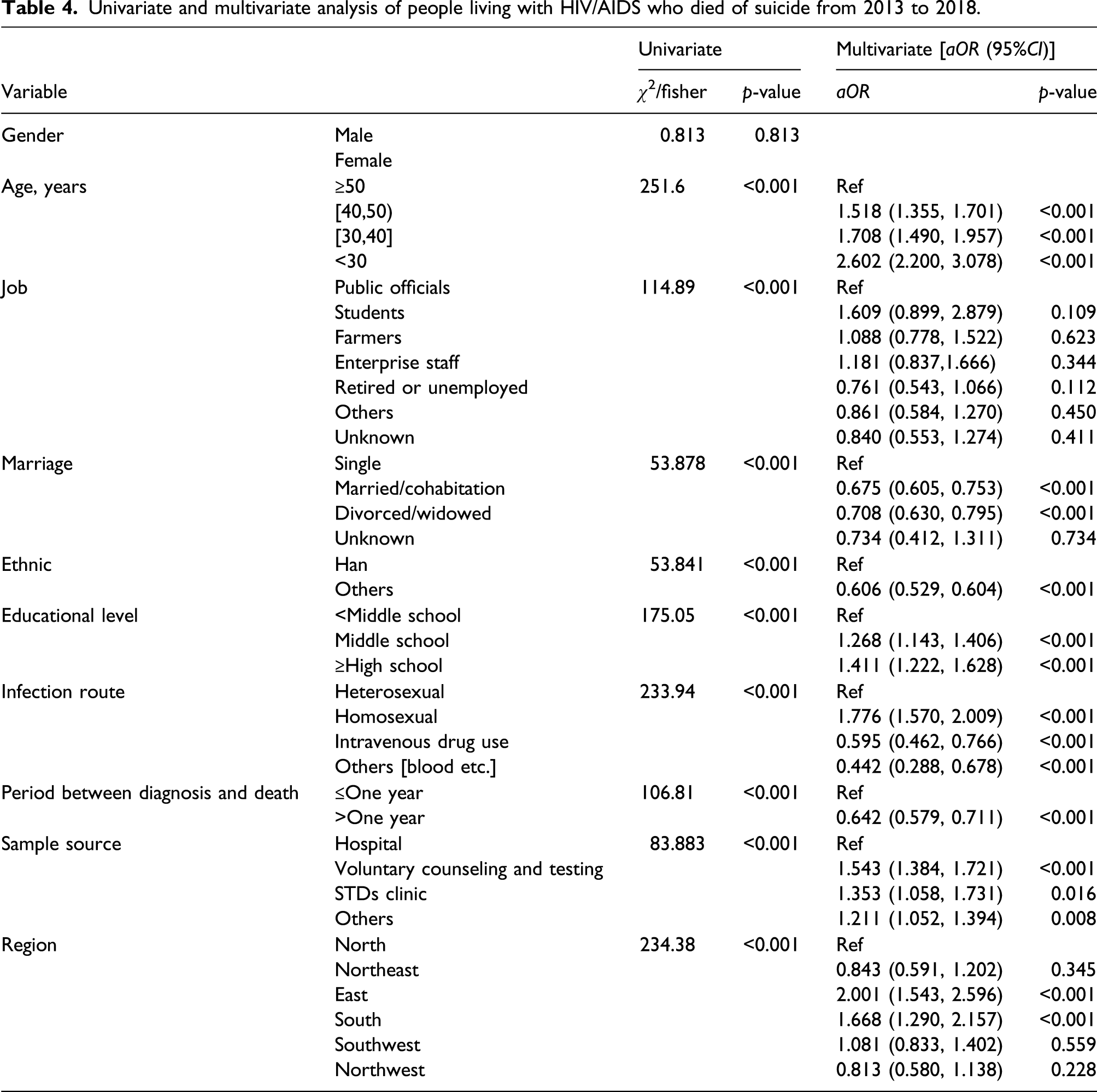
Univariate and multivariate analysis of people living with HIV/AIDS who died of suicide from 2013 to 2018.
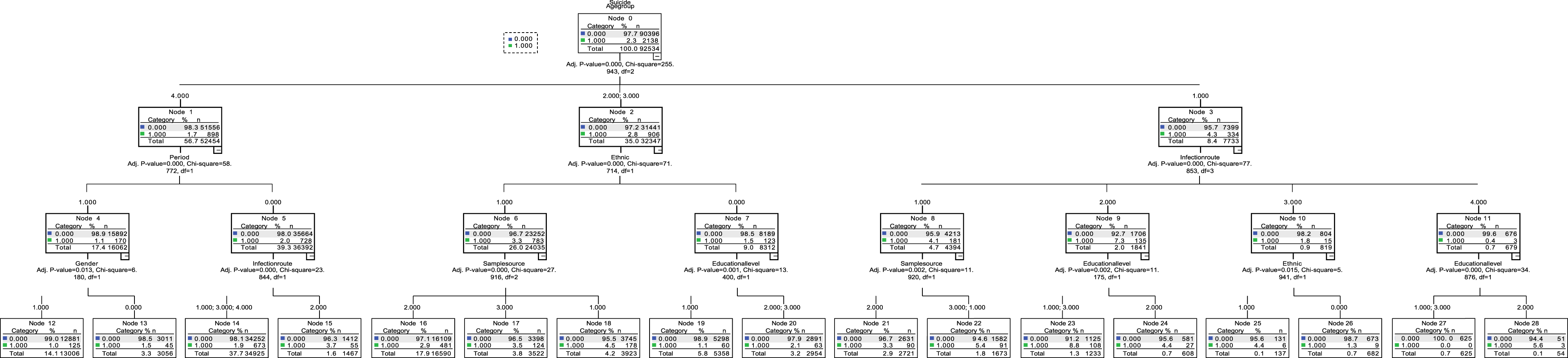
Decision tree model of risk factors of suicide in HIV/AIDS in China, 2013–2018.
Discussion
To our knowledge, most existing studies have focused on suicidal ideation or attempts among PLWH, and thus this was the first study to examine the spatial characteristics and the social risk factors among PLWH who died of suicide in China. Our study involved nationwide annual new report cases of PLWH covering the 31 provinces, municipalities, and autonomous regions of Mainland China from 2013 to 2018.
The suicide mortality of PLWH in this study (331/100,000) was considerably higher than the findings from the review of suicide in HIV negative people (95/100,000). 11 This finding was consistent with studies among PLWH focused on suicidal ideation in China; a review in 2018 showed that the rate of suicidal ideation (12%–78%) was higher in PLWH than that in the general population (2.6%–25.4%). 12 The possible reason was that PLWH had to face significant impacts on physical health, such as immune system deterioration, and various psychological disorders, such as social discrimination, depression and anxiety, etc.13–15
This was the first study to determine spatial characteristics among PLWH who died of suicide, with the national data in China. We found that the high suicide mortality regions were inconsistent with that of the high prevalence of PLWH in China, which showed that there was a distribution difference between HIV prevalence and suicide mortality. The regions had higher HIV prevalence but a lower proportion of suicide located in Southern and Southwestern China (including Yunnan/Sichuan province, and Guangxi Zhuang Autonomous Region). These areas were the initial places of the HIV epidemic in China. 16 These regions were the first regions to implement a series of care policies for PLWH and standardize the voluntary HIV testing or counseling services. These provinces took the lead in Antiretroviral Therapy (ART) for HIV, building the standardized, scientific, and legal management of prevention and treatment work. 17 The majority of HIV infections in the early phase of the epidemic were among drug users in these regions, then to flourish to all provinces, due to the sharing of injection equipment and following unsafe sexual behaviors.18,19 With the lower educational level, ethnic minorities or foreign-born women supported themselves’ lives or those of their families through commercial sex. 16 So, With comprehensive policies for PLWH and a higher prevalence of HIV, the stigma or discrimination might be relatively low, leading to the observation that suicide mortality was lower in these regions.
In addition, The Top three provinces of suicide mortality were Anhui, Hubei, and Hunan, located in the east and south of China. The possible reason might be the high percent of homosexual transmission and mental disorders among PLWH in these provinces. The proportion of HIV cases due to homosexual contact were 22% in Anhui from 2013 to 2018 in this study, and another study in Anhui reported that 31% HIV-positive MSM had suicidal ideation. 20 HIV-positive MSM were suffering double pressure from both stigma of homosexuality and HIV infection so may be more vulnerable.21,22 A study of 370 PLWH in Hunan showed that 42.2% of the participants had homosexual orientation, and the prevalence of depression and anxiety among them was 40.3% (PHQ-9 ≥ 10 points) and 30.5% (GAD-7 ≥ 10 points), respectively. 23 At the same time, the proportion of students in the total PLWH increased from 5.8% in 2008 to 18.3% in 2016, and male homosexual behavior was the main way of transmission in HIV infection among students.24,25 College students were reported to have high levels of suicidal ideation, planning, and attempts.26,27 Hubei’s capital city, Wuhan, is the city with the largest number of universities in China. Large numbers of students or highly educated people in these areas may have contributed to higher suicide mortality. On the other hand, although HIV-positive MSM also comprised a large percent in coastal areas of China such as Jiangsu or Shanghai, these regions had more open minds or greater inclusion for MSM than Hubei or other two regions. So, HIV-positive MSM had to face much more psychological pressure, which leads to high suicide mortality, in Anhui, Hubei, etc., as non-coastal provinces. In summary, although HIV prevalence was not the highest in the east or south of China, we still need to pay attention to the psychological status or stigma of PLWH in these low HIV prevalence places. Public health efforts should aim to destigmatize HIV and mental illness and develop tailored suicide prevention programs among PLWH.
We found some risk factors of suicide in PLWH, which were being younger age, with Han nationality, single, higher educational level, and homosexual infection route. The possible explanations were, first, the suicide rate among college students in China was higher than in other groups of the same age because of competition in school. 28 And, a report in Shanghai in 2015 found 88% of the 92 HIV positive students was caused by homosexual transmission 29 ; another study on college students in 2019 reported that suicidal ideation in the sexual minority (including MSM) was significantly higher than other students. 30 As for the observation PLWH with higher educational levels tended to commit suicide, the proportion of PLWH with higher socioeconomic status such as MSM is increasing in China.
We also found that single PLWH were more likely to commit suicide. A prior study in HIV negative people showed that being unmarried may increase the vulnerability to negative consequences of stressful life events 31 and this increased the feelings of loneliness, hopelessness, worry about the future, and led to reduced social support. 32 For single PLWH, besides the pressures mentioned before, they may have had to face the pressures from that they were afraid of transmitting to their future spouse or their parents’ push them to get married, especially in MSM who did not “come out of the closet.”
Another risk factor for committing suicide was acquiring infection by the homosexual transmission route. In A review of mental health among MSM in China reported varying prevalence of lifetime suicide attempt in Chinese MSM from 4.6% 33 to 12.6%, 34 compared to an estimated 0.8% prevalence of suicide attempts in the general Chinese population. 35 For HIV-positive MSM, the prevalence of suicidal ideation has been documented to be between 10.6% 35 and as high as 26.0%. 34 Also, a study showed that suicidal ideation or attempts also resulted from the failure of being unaccepted by mainstream society in HIV-positive MSM. 21 Similarly, one study in Guangzhou told that the possible reason was the influence of traditional beliefs, so MSM tended to suffer from social stress or perceived stigma. 6
There were some limitations in our study. First, reporting bias as the data qualities relied on routine disease surveillance. HIV case and cause of death reporting were recorded by local hospitals or the CDC, and diagnostic facilities in different regions might affect the quality of data. Second, most of the behavior data were self-reported, which might lead to memory bias and social desirability bias. For example, some MSM might obscure their experience of homosexual behaviors to keep from exposing their sexual orientations, which might lead to reporting wrong transmission routes in the system. Third, the lack of temporal trends analysis, prevented us from studying the potential changes in suicide mortality over time.
In conclusion, there was an inconsistency between HIV prevalence and suicide mortality, which means that high suicide mortality regions were inconsistent with that of the high prevalence of PLWH in China. Besides, We found social risk factors of suicide in PLWH, including being students, single, having a higher educational level, and homosexual infection route. Specific intervention strategies on mental or behavioral health for PLWH in different regions and with different characteristics to decrease the mental-related burden of disease in this high-risk population.
Footnotes
Acknowledgements
We thank all provincial and city-level AIDS directors and their colleagues for the human immunodeficiency virus reporting system.
Author note
To analyze characteristics of geographical distribution and risk factors on people living with HIV/AIDS (PLWH) who committed suicide.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors: No reported conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the article have been disclosed.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.