
Abstract
We aimed to benchmark the quality of care and describe characteristics of patients newly attending the HIV clinic at differing time points over the past 10 years, against the Infectious Disease Society of America HIV/AIDS performance measures. We performed a retrospective analysis of records for patients newly attending the HIV clinic in 2011, 2016 and 2018. There was an increase in male attendees in 2018 and 2016 compared to 2011 (88%, 88% vs. 59% p < .001), viral suppression rates were 97%, 83% and 99% (p < .001), respectively. We observed an increase in patients of South American origin over time. Acquisition risk changed, with increased proportion of MSM (24% in 2011 vs 78% in 2018, p < .001), lower rates of heterosexual (20% in 2018 vs 48% in 2011, p < .001) and IDU transmission (1.5% in 2018 vs 24% in 2011, p < .001). There were lower rates of Chlamydia trachomatis and Neisseria gonorrhoeae testing in 2018 (72%, p < .001), compared to 2016 (84%) and 2011 (83%). Hepatitis B virus vaccination and pneumococcal vaccine rates are declining (p < .001). We demonstrate the changes in both ethnicity and risk of acquisition over time, high rates of antiretroviral therapy prescription and viral suppression, and highlight the importance of health prevention with sexual health screening and vaccination in this population.
Keywords
Background
Since its original description in 1981, there have been colossal advances in the understanding and care of human immunodeficiency virus (HIV) infection. In the West, HIV infection has advanced from an incurable, progressive disease to a treatable, complex chronic disease. Globally, it continues to be a major public health issue with a further 1.7 million individuals acquiring HIV in 2019. 1 Those living with HIV infection without significant co-morbidities and with virologic suppression on antiretroviral therapy (ART) can expect a life expectancy near that of the general population. 2 Care is multifaceted and multidisciplinary. Measurement of quality of care is an essential component to ensuring improved patient-centre care and outcomes. Quality improvement programme reviews should be implemented to identify and amend practice to improve patient care beyond the single focus on HIV viral suppression.
Audit of the standards of HIV care at both individual patient and population levels is essential to drive quality improvement in clinical service provision and in public health outcomes. In 2017, the European Centre for Disease Prevention and Control (ECDC) recommended monitoring a four-stage continuum for Europe; the estimated number of people living with HIV in the population, those diagnosed, those on antiretroviral treatment and those virally suppressed. 3 A national audit was performed in Ireland in 2018 to review these measures which would allow Ireland’s progress to be measured against the UNAIDS 90–90–90 target. 4
HIV Medical Association (HIVMA) performance measures developed in 2007 outlining high priority aspects of care for patients living with HIV, adapted from Ref. 2. ‘Development of national and multi agency HIV care quality measures’.
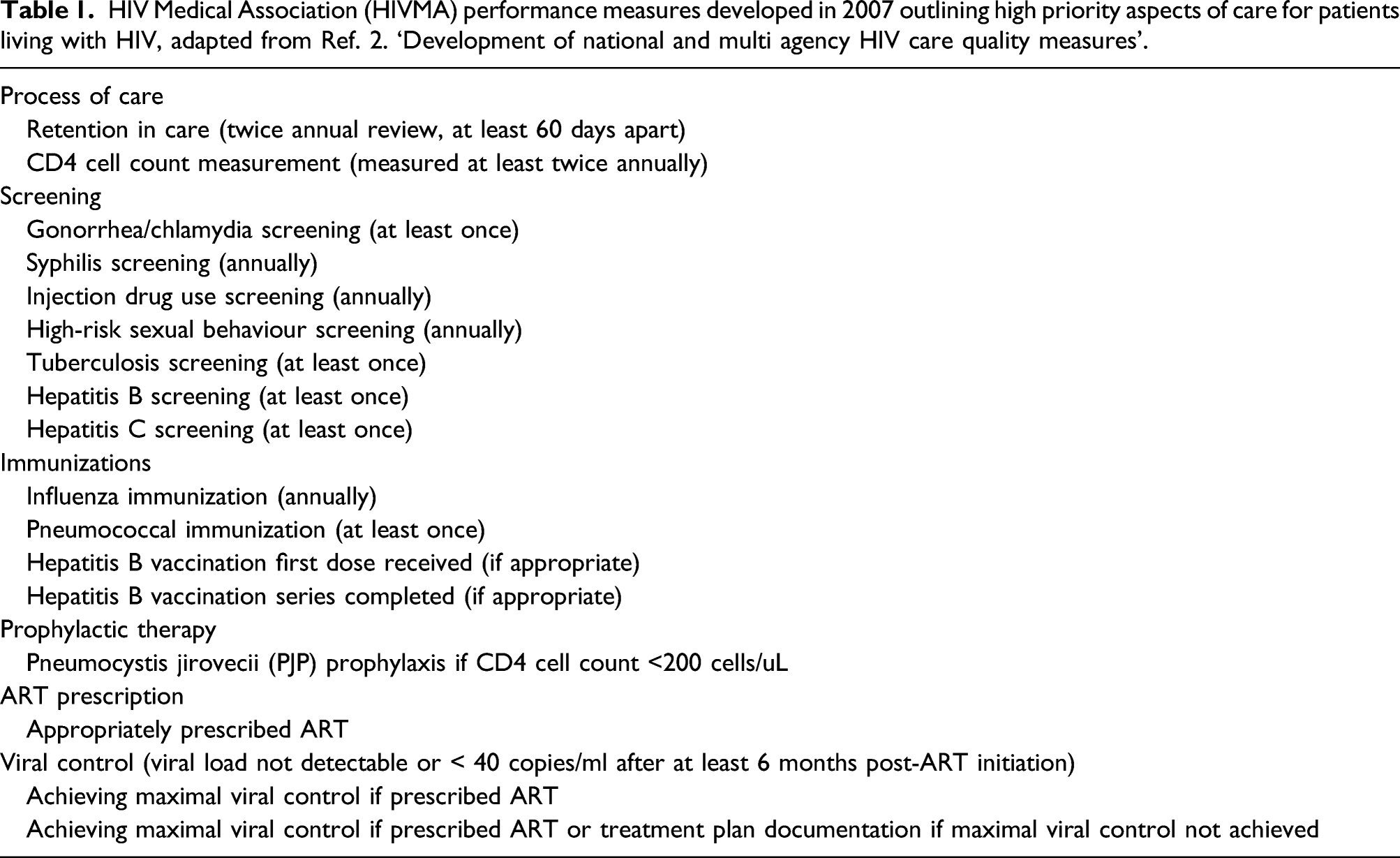
These measures represent high priority care needs of persons living with HIV (PLWH) but are not without limitation regarding their application. They do not address specific needs related to pregnancy and would not be applicable to a paediatric population. They do not include review of complications of therapy and do not involve screening for co-morbidities. Nonetheless, they have been approved and endorsed by the American Medical Association (AMA), the National Committee for Quality Assurance (NCQA), the Infectious Disease Society of America (IDSA), the HIV Medicine Association (HIVMA) and the Health Resources and Service Administration (HRSA) as a single, aligned set of quality measures to review HIV care and outcomes. Healthcare providers and systems have been encouraged to implement and report on these performance measures. 2
It is important to note that since the publication of the aforementioned guidelines in 2007, the British HIV Association (BHIVA) and the European AIDS Clinical Society (EACS) have published updated guidelines for HIV care. For the purpose of comparison with previously performed audits, we decided to use the HIVMA guidelines so that we could benchmark our results to the same standards.
This study follows two previous audits preformed on the standard of care provided for new patients, both newly diagnosed and new to service, attending the HIV clinic in our department. The first was performed in 2011, and care was re-audited in 2016. The overarching objectives of this study were to firstly, compare clinical outcomes with previously performed audits, and secondly, to describe the impact of a changing patient demographic over the past 10 years and how this has influenced certain care outcomes.
Methods
A retrospective analysis of all newly diagnosed or newly attending patients registered at the HIV Clinic in St James’s Hospital in 2018 was undertaken. Data were collected using the electronic medical records system, anonymised and analysed using excel. Data collected included demographic, laboratory, radiological and treatment data. Patient care was evaluated with reference to the seventeen 2007 HIVMA performance measures, and then compared to the findings of the 2016 audit completed in 2018 (266 patients newly attending the HIV clinic in 2016) and a 2011 audit completed in 2012 (409 patients newly attending the HIV clinic in 2011). Mann–Whitney U test and ANOVA (Kruskal–Wallis test) with Dunn’s post hoc test were used for statistical analysis.
Results
There were 266 PLWH newly registered in the clinic in 2018. A total of 253 patients were included in the audit. Thirteen PLWH were excluded from our study: two died prior to clinic review (one from disseminated TB and the other from severe burns); six were identified through our emergency department viral screening programme and when contacted reported that they were receiving HIV care at a different centre; and five were attending centres outside of Ireland and attended the clinic once for an emergency medication supply. There were clinical notes and laboratory results available on the electronic patient record for 244 of the 253 patients, the remaining nine patients had only laboratory results available for review as their clinical care was provided using paper-based records, in an off-site location.
Patient demographics
Demographics, geographical origin and route of HIV acquisition for new PLWH attending the St James Hospital HIV clinic in 2018, 2016 and 2011.
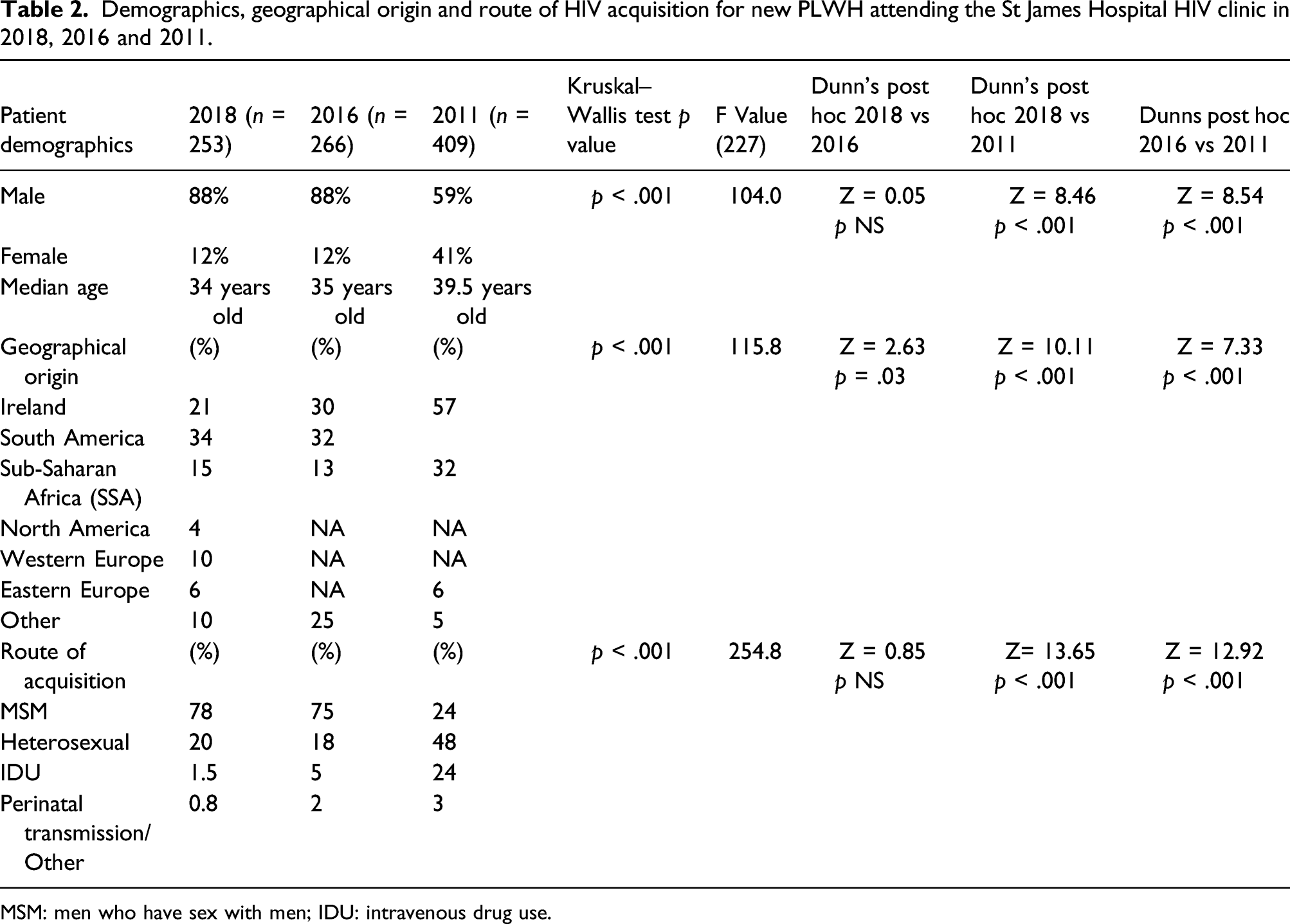
MSM: men who have sex with men; IDU: intravenous drug use.
Geographical origin is changing, with a trend towards diversity, as outlined in Table 2. In 2018, we saw fewer new Irish-born PLWH in the clinic compared to previous years (21% in 2018, 30% in 2016 vs 57% in 2011 p = < .001), with fewer PLWH from sub-Saharan Africa (SSA) too (15% in 2018, 13% in 2016 vs 32% in 2011 p = < .001). The largest percentage of new PLWH in 2018 was of South American origin (34%).
In 2018, the mode of HIV acquisition was predominately sexual transmission among men who have sex with men (MSM) at 78%, with an additional 20% of cases reporting a heterosexual acquisition risk. Few PLWH were infected as a consequence of injection drug use (1.5%) and 0.8% of PLWH acquired infection from vertical transmission. In 2016, these figures were similar (Table 2). In 2011, however, we saw a higher proportion of intravenous drug use (IDU)-related acquisition risk (24%), lower MSM acquisition (24%) and higher heterosexual transmission (48%, p < .001).
Summary of results of standards of care provided to new patients attending the HIV clinic in 2018, 2016 and 2011.
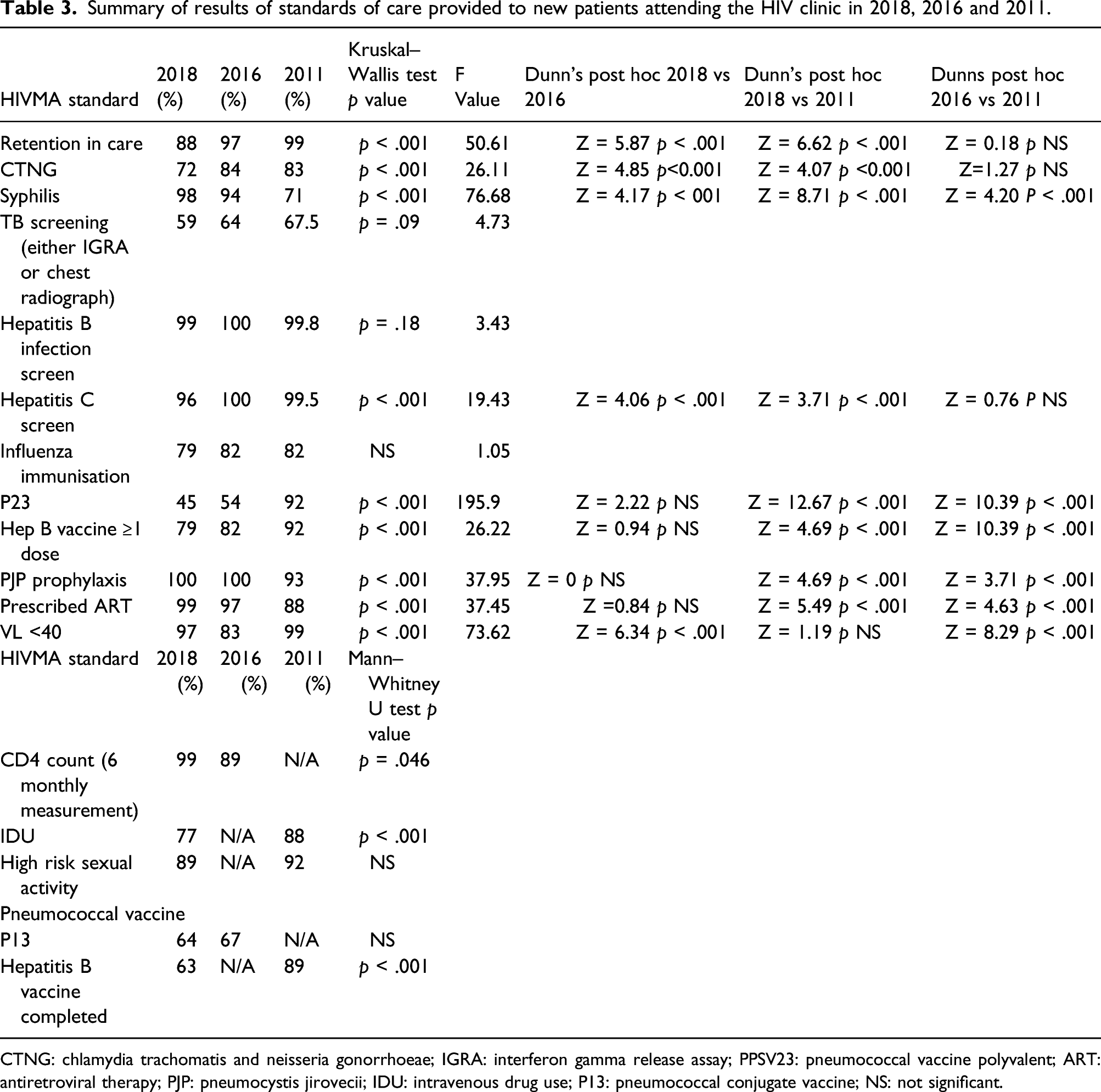
CTNG: chlamydia trachomatis and neisseria gonorrhoeae; IGRA: interferon gamma release assay; PPSV23: pneumococcal vaccine polyvalent; ART: antiretroviral therapy; PJP: pneumocystis jirovecii; IDU: intravenous drug use; P13: pneumococcal conjugate vaccine; NS: not significant.
HIV disease control
In 2018, 48% of patients had a detectable viral load (VL) on initial presentation and 12% had a CD4+ T cell count <200cells/mm3 with 100% of these patients appropriately prescribed pneumocystis pneumonia (PJP) prophylaxis. This high rate of PJP prophylaxis prescribing was consistent in 2016 and 2011 (Table 3).
99% of the 2018 cohort were prescribed antiretroviral therapy (two patients were identified as elite controllers with successful viral suppression without ART therapy), compared to 88% in 2011. Successful viral suppression, defined as most recent HIV RNA not detected or <40 copies/ml at time of data collection, was achieved in 97% of patients (nine who were not retained in care for repeat VL testing are excluded from this calculation). This outcome was improved from 2016 when 83% of patients achieved viral suppression (p < .001). In 2011, 99% of ART-treated PLWH attained VL suppression.
Sexual health and recreational drug use
In 2018, 72% of patients had baseline Chlamydia trachomatis (CT) and Neisseria gonorrhoeae (NG) screening. There were higher rates of CT and NG testing in 2016 (84%) and 2011 (83%, p < .001). Syphilis screening with syphilis antibody testing was performed in 98% of patients in 2018 on initial presentation. 94% of patients had syphilis antibody testing in 2016, and in 2011, 71% of patients were screened (p < .001). High risk sexual behaviour screening was similar in 2018 and 2011 (p not significant), although assessment for recreational drug use was lower (77% in 2018 vs 88% in 2011, p < .001) (Table 3).
Tuberculosis screening
Tuberculosis (TB) screening in the 2018 patient group was performed with either a chest radiograph in 53% of patients or interferon gamma release assay (IGRA) in 26%, and 43% of patients had both. On further analysis of the 2018 group (243/253 patients assessed), a higher proportion of patients newly diagnosed with HIV infection who attended our clinic for their first review had a chest radiograph (67 of 93, 72%) compared with newly transferred patients (77 of 149, 51.68%, p = .0021). 15% (10/67) of these newly diagnosed patients had abnormal chest x rays, and of those, 20% (2/10) were subsequently diagnosed with TB.
In the newly HIV diagnosed patient group (93 patients), 40% had an IGRA, and this was positive in 8% (n = 3) of tests. Subsequently, two of these patients were diagnosed with active TB disease.
Of the 149 patients (61%) with known HIV infection who transferred care from a different centre, 26 patients (17%) had an IGRA test performed or documented previous IGRA result. In this group, 18% of (3/17) IGRA’s performed at our clinic were positive (one patient was previously treated for latent TB, and two patients were diagnosed with latent TB following this screening).
Immunity and vaccinations
Hepatitis B virus (HBV) screening rates were ≥99% throughout the three time-points. In 2018, 79% of non-immune patients received ≥one dose HBV vaccination and 62% of patients completed the vaccination course with at least three doses. Completion rates for HBV vaccination were 82% in 2016 and 92% in 2011.
Influenza vaccination was administered to 79–82% of patients over the three time-points.
The present recommended pneumococcal vaccination course includes pneumococcal conjugate vaccine (PCV13) followed by pneumococcal polysaccharide vaccine (PPSV23). 5 In the 2018 cohort, only 43% of patients successfully completed this course, receiving PCV13 before PPSV23, an additional 0.8% received these two vaccines in reverse order. 12% of patients were given pneumococcal vaccination with only PCV13 and 2% received only the PPSV23 vaccine. Use of the PCV13 vaccine was not recommended for adults with HIV in 2011 when vaccination uptake with PPSV23 alone was 92%.
Discussion
This study aimed to describe the standard of care delivered to newly diagnosed or newly attending PLWH registering at a large urban centre in 2018 and to compare these findings with those from prior audits undertaken in the same centre over a seven-year period. We observed a shift in multiple demographic variables of our cohorts over time. In 2018, most patients newly diagnosed or newly attending were men, and this was associated with an increase in MSM risk for HIV acquisition and a reduction in heterosexual risk over time, as described. This shift in profile of PLWH correlates with the increase in patients migrating from South America, where high rates of MSM transmission are described 6 and a reduction in PLHW migrating from SSA where HIV transmission is predominantly heterosexual. 7 Geographical origin provides context for individualised care given the epidemiological variation in factors including rates of tuberculosis infection, 8 syphilis infection, 9 glucose-6-phosphate dehydrogenase deficiency 10 and differences in HLA B5701 genetics. 11 Although not all these measures were included in the study, they highlight the importance of considering patients’ geographical origin and its context in patient care.
Improved access to needle exchange facilities and drug counselling and treatment services is reflected in the falling rates of IDU-related risk of acquisition. This change in risk associated with IDU impacts on co-morbidities and screening recommendations throughout care. 11
The median age of new PLWH attending the clinic was lower over time. HIV screening has become more widespread over the past decade, in keeping with UNAIDS 90–90–90 targets. 4 In the hospital in which the study was conducted, blood-borne viral screening is performed on all patients attending the Emergency Department on an opt out basis since 2015. 12
There was an increase in ART prescribing, correlating with changing international guidance recommending antiretroviral treatment be initiated for all patients living with HIV, irrespective of CD4 count. 13
There are areas where quality of care improved; CD4 count measurement increased and syphilis screening levels improved. Throughout the three time-points, there were high rates of use of PJP prophylaxis and hepatitis B and hepatitis C viral screening.
TB screening rates are low and declining. BHIVA guidelines advocate clinical assessment for active TB in all newly diagnosed PLWH, as well as latent TB assessment in those from high risk areas. 14 EACS guidelines, recommend TB screening appropriate to risk, advising consideration of ethnic origin, CD4 count and ART use. 13 A significant proportion of patients screened for TB had a positive result; but only 40% of newly diagnosed patients were assessed for TB with IGRA in 2018, suggesting TB may be under diagnosed in the cohort. Screening was performed even less in the transferred patient group with comparison to the new patient group who attended the OPD for their first clinical review post-HIV diagnosis. Of the 51% in the transferred group who were screened, there were cases pick-up of previous TB exposure, with 18% IGRA positive. This highlights the need for reinforcement of screening in this group as well as in those newly diagnosed.
Widespread use of ART has been effective in attaining viral load suppression, and PLWH have excellent rates of regular CD4 count measurement. The success of HIV care however cannot be based on ART prescribing and viral load suppression rates alone. A focus on preventative interventions including sexual health screening, as endorsed by BHIVA 14 and EACS 13 guidelines, is an essential aspect of holistic care in PLWH. TB screening and completion of vaccinations are known to reduce these infections in this vulnerable population. Delivery of comprehensive, person-centred, evidence-based care is critical, particularly in the era of patients living longer and successfully ageing with HIV. 15
There are several limitations to this study. As the data were collected at different time-points, there were variations in some aspects of data collection. For example, IDU and high risk sexual activity screening were not assessed in 2016, and CD4 count measurement was not assessed in 2011. Vaccination records in 2018 were collected using patients electronic record and may exclude vaccinations prescribed on paper charts or vaccinations provided in primary care, driven by increasing numbers of PLWH accessing primary care and the increasing delivery of vaccinations in pharmacies and GP practices. At this time, Ireland does not have a unique patient vaccine identification number or electronic passport, impacting on the ability to track vaccination delivery across multiple health systems and locations. Of note, EACS 13 and BHIVA 14 have published more comprehensive, updated guidelines on HIV care, and we have used the HIVMA 2007 guidelines in order to compare the quality of care provided across the three audits. A further limitation given the retrospective nature of this study, we were unable to distinguish patients newly diagnosed with HIV and those who have transferred their care from a different setting, with the exception of the 2018 TB data above.
Conclusion
This study chronicles the changing demographic in patients attending the HIV Clinic over the past 10 years, with a shift in geographical origin and HIV acquisition risk factors observed. There were several strengths in the quality of care provided to PLWH attending our centre. The study has highlighted the need for a renewed focus on health prevention in the domains of sexual health, TB screening and vaccination. With a growing and ageing patient cohort, there is a necessity for continuous evaluation of service provision and a quality-improvement framework to focus on interventions and improve patient outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.