
Abstract
Chlamydia trachomatis (CT) and Neisseria gonorrhoeae (NG) infections are common among men who have sex with men (MSM). Many oropharyngeal and anorectal infections remain asymptomatic. We aimed to evaluate triple-site screening following PrEP introduction. We enrolled a prospective cohort study including 210 asymptomatic MSM during 2019–2020, analyzed by groups: HIV positive (HIV+), HIV−uninfected using PrEP (HIV−/PrEP+), or HIV-uninfected not using PrEP (HIV−/PrEP−). A self-administered questionnaire captured demographic information and sexual risk-taking behaviors. CT/NG testing results were compared between study groups and predictors of infection were evaluated. We included 59 HIV+, 70 HIV−/PrEP+, and 81 HIV−/PrEP− subjects. 30% (n = 62) of participants tested positive for CT/NG. HIV−/PrEP+ group had highest proportion of infections (n = 33, 47%) followed by HIV−/PrEP− (n = 16, 22%) and HIV+ (n=13, 20%; p < .001). Importantly, 98% (80/82) of pharyngeal/anorectal CT/NG infections were missed in genitourinary tract screening alone. PrEP use and previous syphilis infection were the strongest risk factor for CT/NG. Extra-genital asymptomatic CT/NG infections were prevalent among MSM. These data highlight the importance of routine extra-genital CT/NG testing in asymptomatic sexually active MSM. The study describes the consequences for three-site testing lack of implementation in the PrEP era.
Introduction
Sexually transmitted infections (STIs) are a major public health concern in both resource rich and limited settings. The incidence of STIs has been increasing among certain subpopulations who engage frequent sexual risk-taking behaviors, such as men who have sex with men (MSM) who are living with HIV and those using pre-exposure prophylaxis (PrEP) for HIV.1–4
Chlamydia trachomatis (CT) and Neisseria gonorrhoeae (NG) infections are among the most common venereal pathogens; in the United States (US), diagnoses of CT and NG have increased by 19% and 63%, respectively, from 2014 to 2018. 5 Both CT and NG have major public health implications and can lead to severe clinical sequelae. As both infections are highly transmissible but often asymptomatic, regular CT/NG genitourinary (GU) screening has been a common focus of screening efforts. 5 The immediate goal of screening for STIs is to diagnose and treat infected persons prior to developing clinical disease manifestations and complications, but also to curb community transmission and reinfections by identifying, testing, and treating their sexual partners.
Nevertheless, CT and NG often manifest as isolated (and often asymptomatic) infections of other anatomic sites, including the oropharynx and anal canal. Screening anatomic sites other than urethra/urine may be more impactful since genitourinary CT/NG infections are often symptomatic and therefore more likely to be diagnosed clinically. 6 Recently published US data demonstrated that relying on genitourinary screening alone misses 80% of CT and 77% of NG diagnoses among MSM. 7 Additionally, CT infections are frequently caused by serotypes L1–L3, leading to lymphogranuloma venereum (LGV) but can be asymptomatic in up to 22% of infected persons.8–11
While studies continue to provide evidence supporting extra-genital CT/NG testing, clinical implementation in the US and other countries is still lacking, despite a CDC endorsement for routine triple-site testing. 5 The prevalence of asymptomatic CT/NG infection among Israeli MSM is unknown and triple-site NAAT testing for CT/NG among MSM at high STI risk is not currently standard clinical practice in many countries. PrEP users may be an especially deserving of focus. Despite studies suggesting a higher prevalence of condomless sexual encounters, less than two-thirds of MSM PrEP users have reported consistent CT/NG testing at extra-genital sites.12,13 Moreover, STI testing for PrEP users in the real-world might be much lower than in clinical trials. 14 Therefore, to clarify the risk of asymptomatic CT/NG infection by anatomic site, we prospectively assessed three-site NAAT results among asymptomatic sexually active Israeli MSM, considering HIV serostatus, PrEP use and other sexual risk behaviors.
Methods
Patient recruitment, sample calculation, and collection
We calculated the sample size required to show superiority of combined test of pharyngeal, rectal, and urethral sites versus test of urethral site only. For this calculation, we assumed prevalence rate of 15%, sensitivity of 45% for urine test only, and sensitivity of 90% for three-site testing. We set an alpha = 0.05 (or 2.5% one-sided alpha) and statistical power of 80% for McNemar's test for dichotomous paired variables and determined an optimal sample size of 150. Social media advertisements and flyers were distributed to recruit patients who could register by dedicated website to a designated dates.
HIV-uninfected men not taking PrEP and reporting condom use were included as a comparison group for men reporting unprotected anal intercourse (UAI) at least once within the 90 days prior to enrolling in the study. Additional inclusion criteria included being 18 years or older, not having been screened or receiving antibiotics for STIs in the previous 90 days, and no symptoms suggestive of STI including anal pain and/or symptoms of proctitis, sore throat, or urinary symptoms including urinary discharge.
Three men could not be categorized into a study group due to missing data and were excluded. Five additional participants were eventually excluded from the analytic cohort due to incomplete outcome data.
The study was approved by the IRB of Tel Aviv Sourasky Medical Centre, Israel. After informed consent, participants were offered self-collected testing including pharyngeal, rectal swabs, and urine specimens were performed. The patients were provided with a thorough explanation about self-specimen collection, including illustrations. We chose self-collection for specimens because of strong supporting data and potential ease for future implementation in clinical settings.5,15 Verbal and written instructions for collection were provided by trained clinic staff. The study participants completed a standardized self-administered questionnaire assessing sociodemographics, sexual behavior, drug use, and current use of PrEP.
Rapid PCR test
Testing swabs (rectal, pharyngeal, and urine samples as indicated) were collected and stored according to manufacturer instructions. Samples were tested on-site using the GeneXpert (Cepheid, Sunnyvale, CA, USA) assay. Specimens were placed into a Cepheid swab transport reagent tube and the GeneXpert CT/NG cartridge was then used to purify, concentrate, detect, and identify targeted nucleic acid sequences by the GeneXpert instrument.
Although being used in various clinics, self-collection of pharyngeal and rectal swabs for the Xpert CT/NG assay has not been reviewed by any regulatory authority.
Sequencing of positive chlamydia results
Molecular genotyping of CT was performed at the Chlamydia National Reference Laboratory in Israel. DNA was extracted from the various samples using MagNA Pure Compact Instrument (Roche). Multi-locus sequence typing (MLST) of five CT hypervariable genes and the outer membrane protein A (ompA) genotyping were performed. 16 Molecular serotyping was determined by blast analysis of the ompA sequence.
Statistical analysis
We first compared participant characteristics by study group, testing for differences using t-tests for age and chi-square or Fisher’s exact test for categorical variables, as appropriate. We then calculated the prevalence of CT and NG results by study group and anatomic site. Using these results, we also calculated the proportion of infections that would have been missed under potential testing permutations (i.e., urine alone, urine plus anorectal, and three sites.) Predictors of any STI positivity were then evaluated, testing for differences between those who had any positive test to those who did not using chi-square or Fisher’s exact tests. We then included all participant characteristics (sociodemographic variables, drug use, and sexual behaviors) in a multivariable logistic regression model predicting STI positivity, where our primary measure of interest was the study group. We used multiple imputation methods to account for missing data in the multivariable model. Last, we compared CT serotype proportions by anatomic site. All analyses were conducted using SAS version 9.3 (SAS Corporation, Cary, NC).
Results
Characteristics by study group.
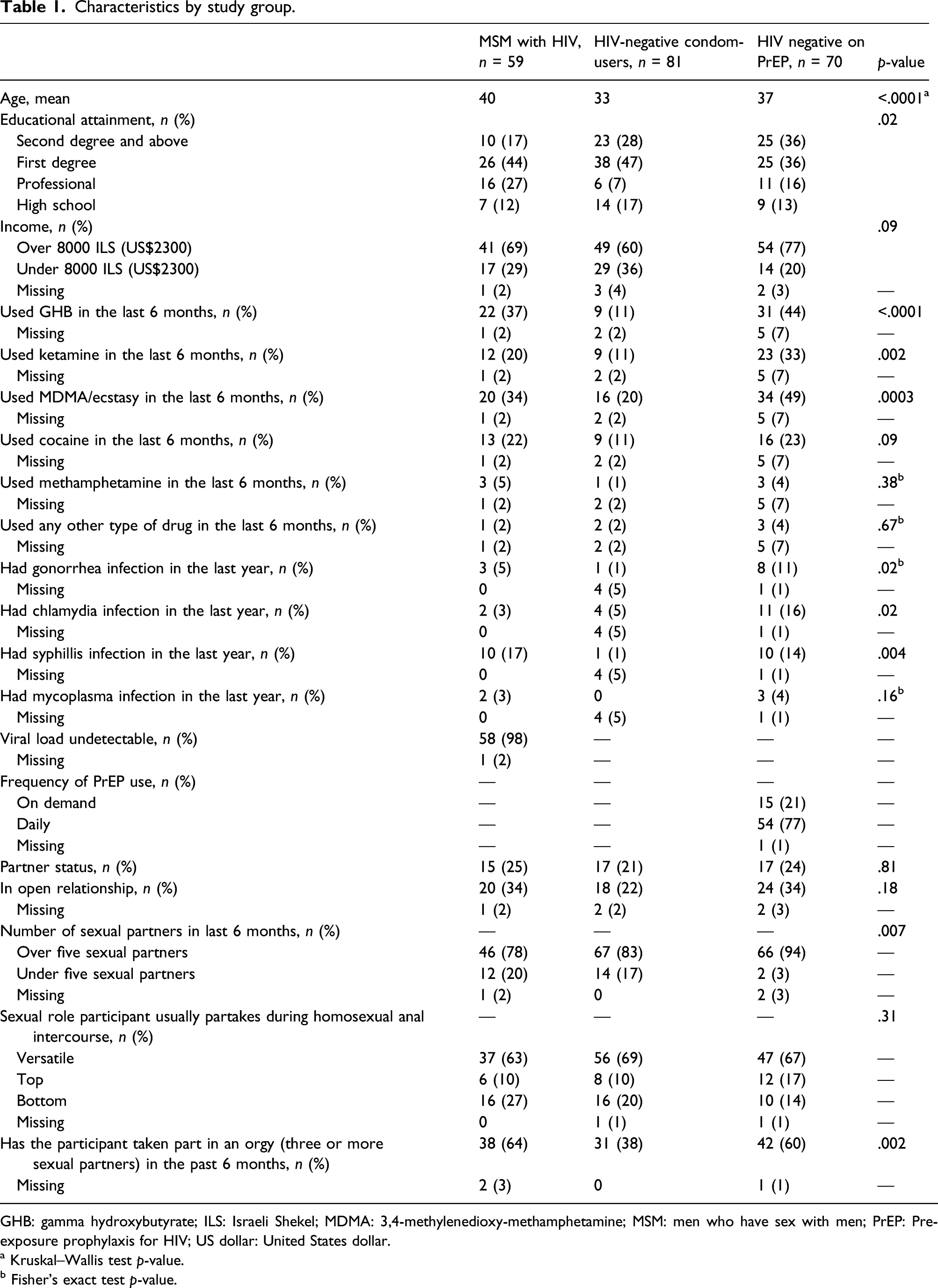
GHB: gamma hydroxybutyrate; ILS: Israeli Shekel; MDMA: 3,4-methylenedioxy-methamphetamine; MSM: men who have sex with men; PrEP: Pre-exposure prophylaxis for HIV; US dollar: United States dollar.
a Kruskal–Wallis test p-value.
b Fisher's exact test p-value.
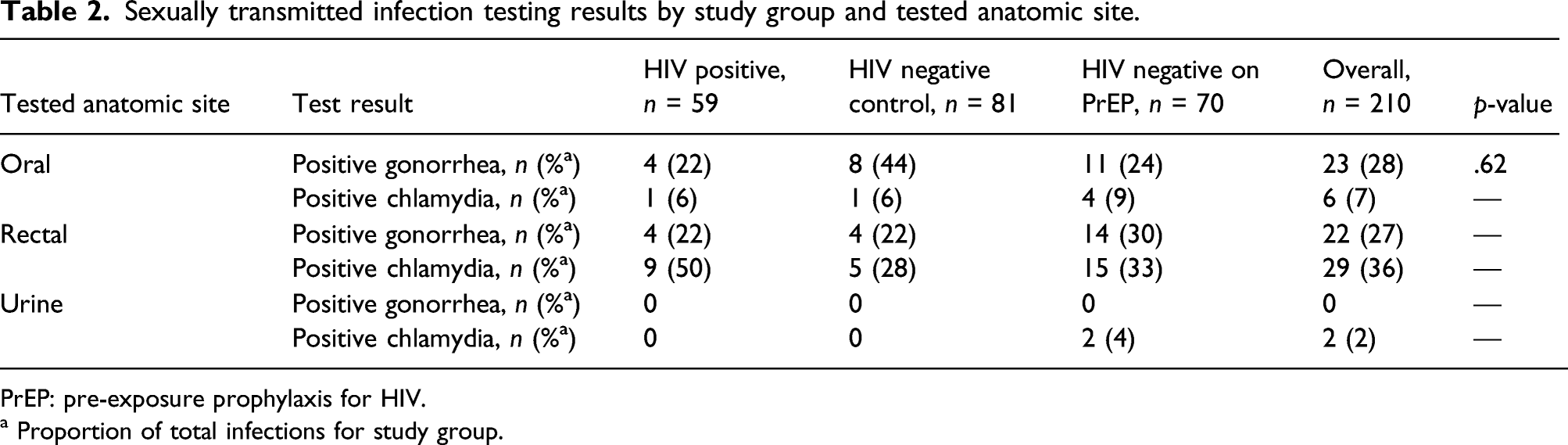
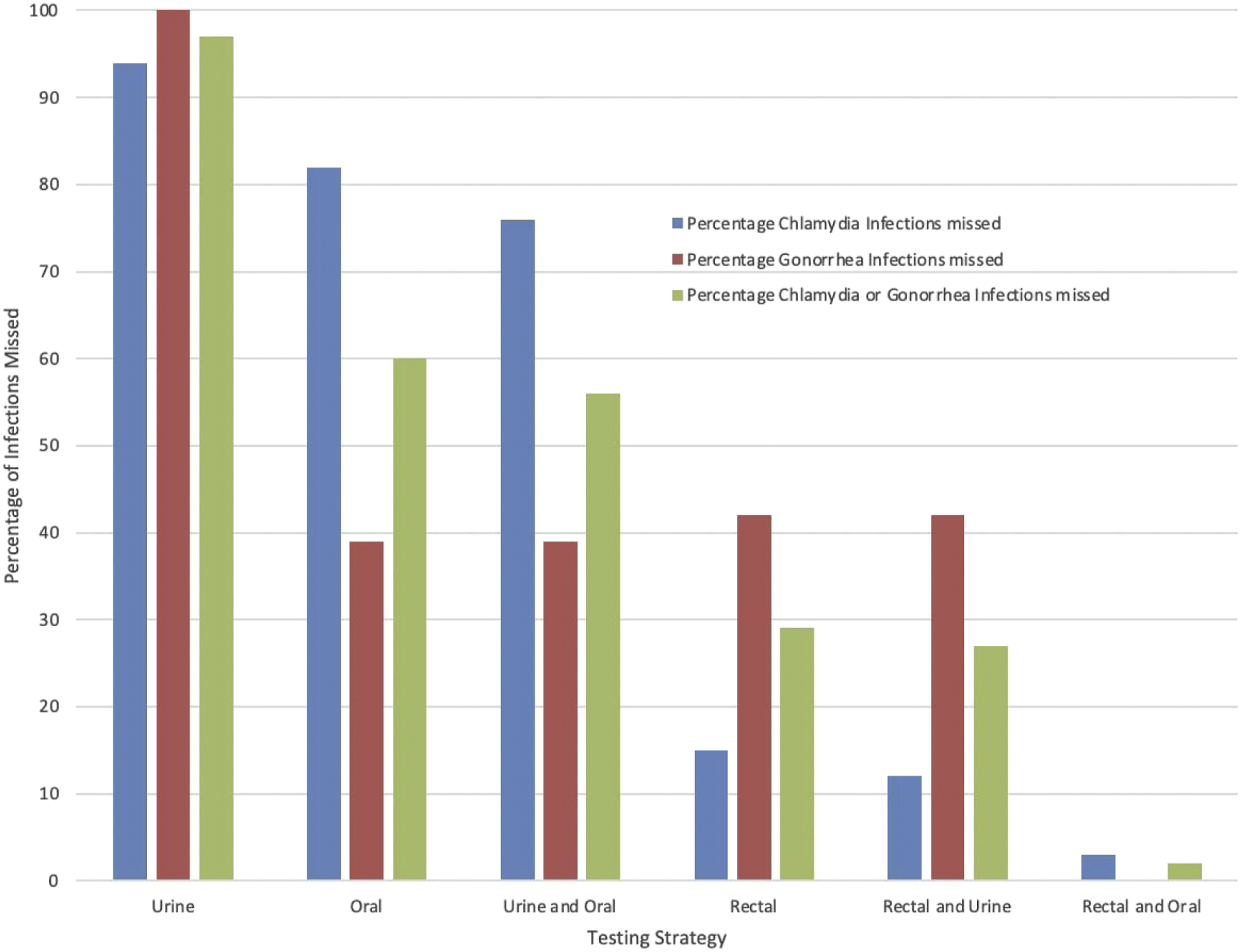
Nearly one-third (62, 30%) of the cohort was diagnosed with either asymptomatic CT or NG. The majority of infections were anorectal (51, 62%); only 2.5% (n = 2) were urethral infections identified from urine testing. The HIV−/PrEP+ group had the highest proportion of participants with infections (33, 47%) followed by HIV−/PrEP− (16, 22%) and HIV+ (13, 20%; p < .001). Rectal CT/NG infections were the most common infection site in all three patient groups (72% of HIV+, 50% of HIV−/PrEP−, and 62% of HIV−/PrEP+) (Figure 1, Table 2). Importantly, 97.5% (80/82) of CT/NG infections overall would not have been detected had testing been limited to urethral screening (Figure 2). Proportion of positive sexually transmitted infection tests by study group and anatomic testing site. Sexually transmitted infection testing results by study group and tested anatomic site. PrEP: pre-exposure prophylaxis for HIV. a Proportion of total infections for study group. Proportion of gonorrhoeae or chlamydia infections missed based on anatomic sites tested.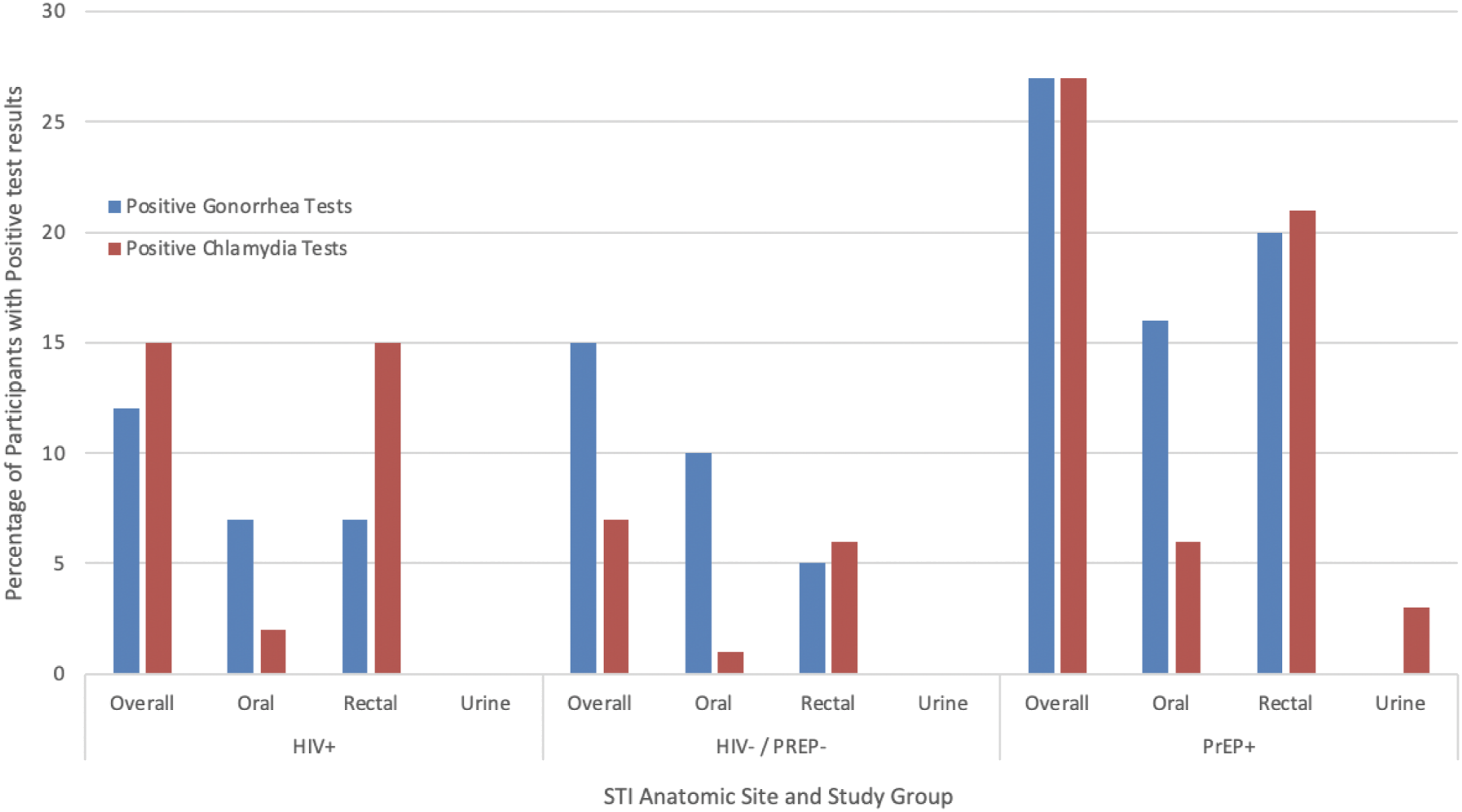
Comparison of participant characteristics by sexually transmitted infection diagnosis.
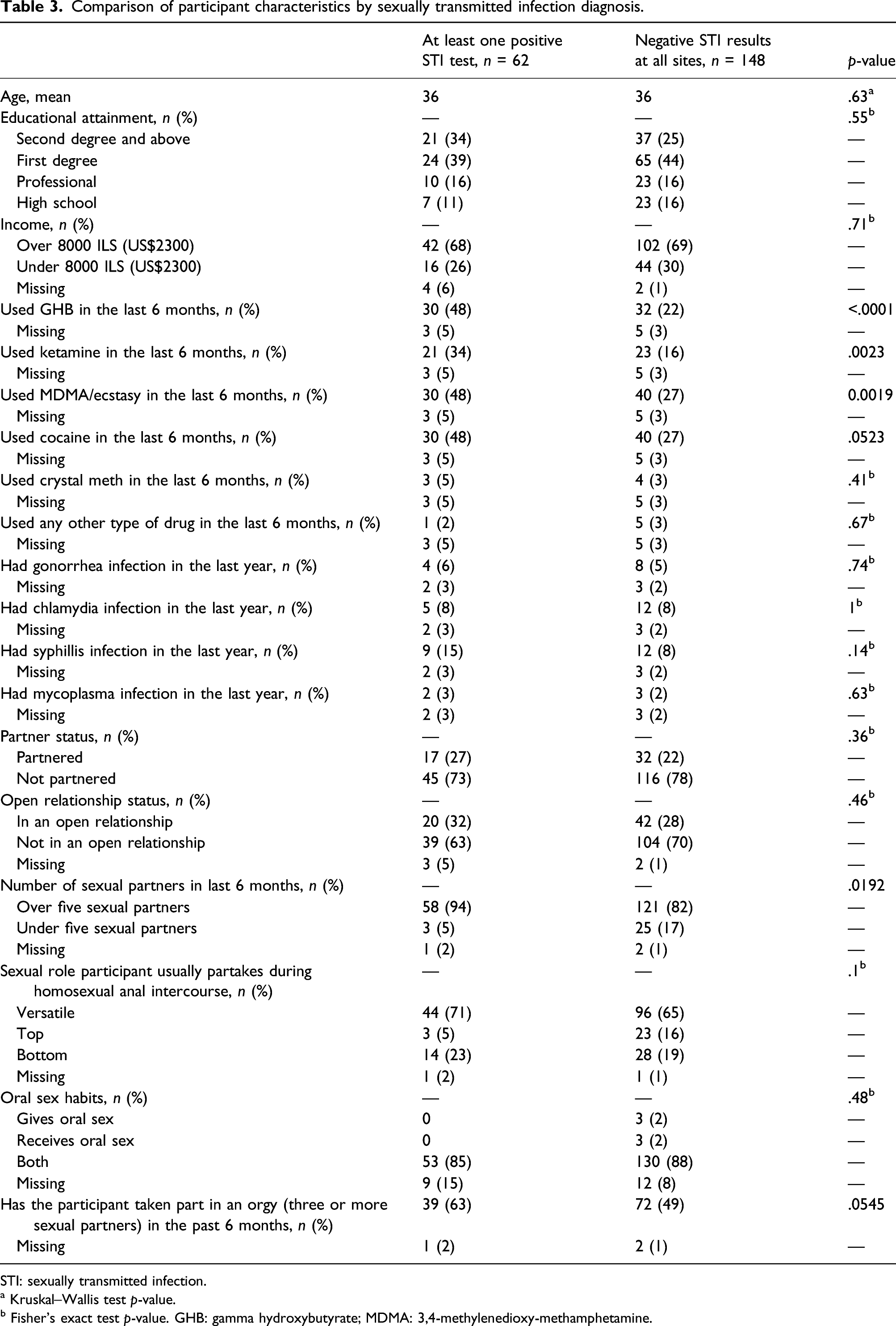
STI: sexually transmitted infection.
a Kruskal–Wallis test p-value.
b Fisher's exact test p-value. GHB: gamma hydroxybutyrate; MDMA: 3,4-methylenedioxy-methamphetamine.
Adjusted logistic regression model predicting asymptomatic sexually transmitted infection.
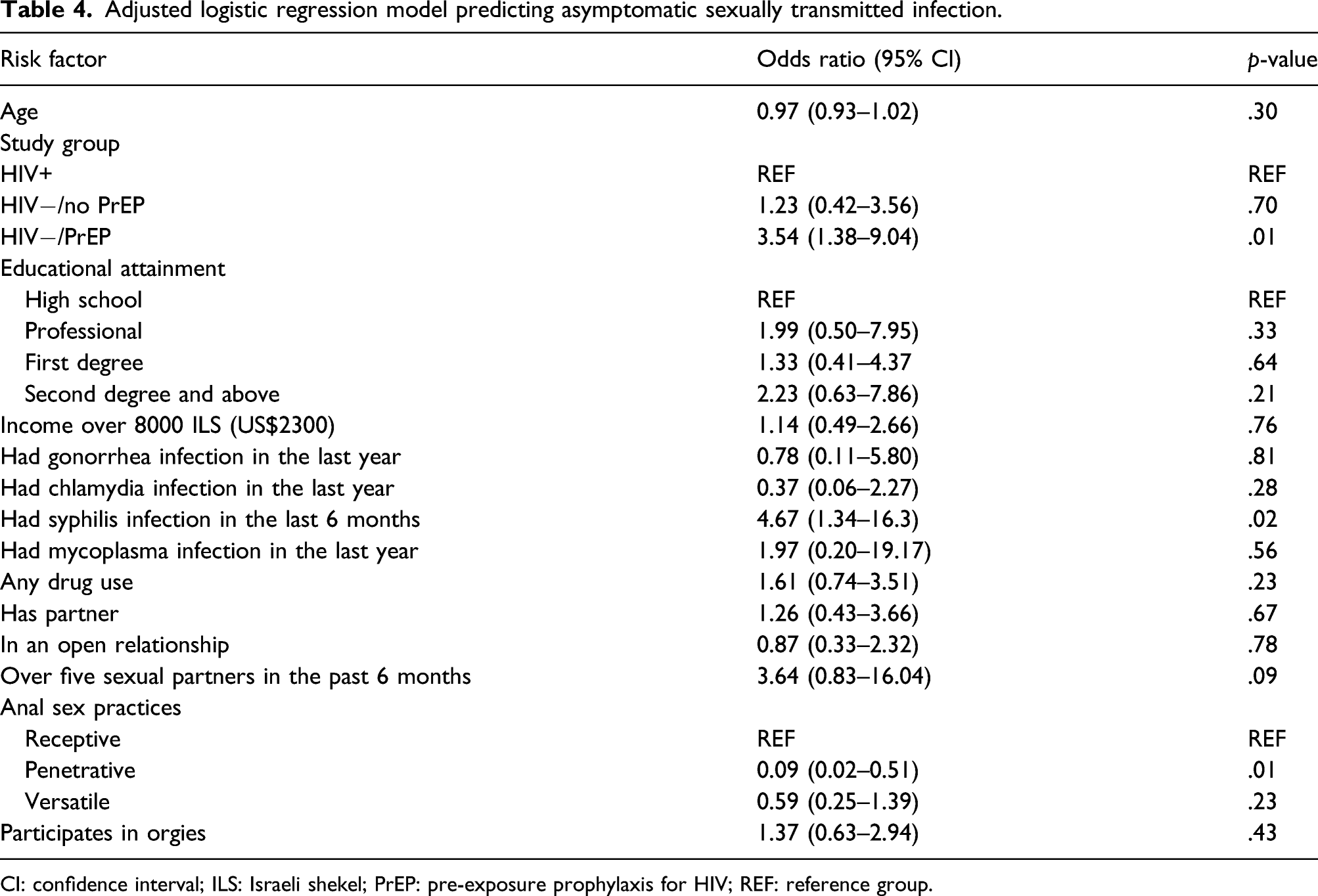
CI: confidence interval; ILS: Israeli shekel; PrEP: pre-exposure prophylaxis for HIV; REF: reference group.
Chlamydia serotypes by anatomic testing site.
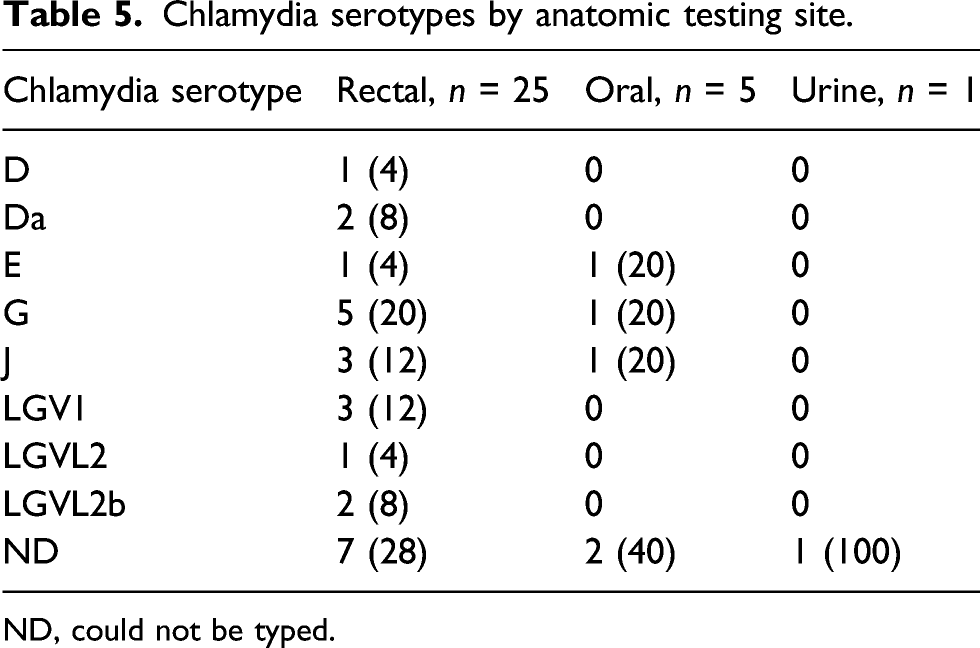
ND, could not be typed.
Discussion
This prospective, single-center study evaluated the prevalence of asymptomatic infections among Israeli MSM undergoing self-collected three-site NAAT for NG and CT. When comparing risk groups, significantly more infections were found among HIV-uninfected PrEP users; 98% of the infections would have been missed by stand-alone GU testing; almost half of the participants in that group tested positive for either NG or CT in at least one of the sampled anatomic sites. The vast majority of infections were detected in non-urethral samples, suggesting that urine-based STI screening alone may have limited value.
Our finding of high proportions of CT/NG infections in non-urethral sites is supported by previous studies.17–19 One retrospective analysis of asymptomatic MSM visiting an urban STI clinic in San Francisco indicated that 83.8% of CT/NG infections would have been missed by standalone GU screening. 18 A study from Germany found that by testing participants only for urogenital STIs, 27.7% of infections would have been identified, however, this study included symptomatic subjects and Mycoplasma genitalium infections. 3 These studies and the current analysis provide support that multi-site testing should be considered as a standard-of-care for STI screening for sexually active MSM.
MSM being treated with PrEP may be a particularly high-risk group in need of special attention. We found that PrEP use was a strong independent predictor of asymptomatic STI, and likely represented more frequent sexual activity and lack of use of STI precautionary measures. Increases in high-risk behaviors after initiating PrEP and an increase in condomless sex have been previously described. 3 Furthermore, study participants in our cohort's PrEP group reported more frequent recreational drug use, a factor likely exacerbating sexual risk-taking. These findings corroborate a recent meta-analysis demonstrating that MSM using PrEP were 25.3 times more likely to acquire NG, 11.2 times more likely to acquire CT, and 44.6 times more likely to acquire syphilis compared to MSM not using PrEP. 2 Also similar to our findings, a multicenter study of MSM in Germany 19 found that using PrEP, having higher numbers of sex partners, having condomless sex as well as using party drugs were independent risk factors for being tested positive for at least one STI. Therefore, initiating and/or studying interventions to address STI risk for PrEP users are warranted to mitigate major complications such as LGV or growing antimicrobial resistance, as has emerged for NG.
Typing CT infections for serovars L1–3 which cause LGV is clinically important, as it may lead to treatment modification, albeit not often routinely performed. Our study exclusively recruited asymptomatic MSM and showed that approximately one-third of anorectal CT specimens were caused by an LGV serovar with the majority of LGV diagnoses among HIV-infected MSM (66%) while only 16% were among PrEP users. Similar findings were seen in a case series from France where most LGV cases were identified among HIV-positive MSM. 20 Another French cohort study of HIV-uninfected MSM using PrEP found that 18.7% of anorectal CT specimens tested positive for LGV serovars and nearly a third of cases were asymptomatic. 21 These data emphasize the potential need for chlamydia serotyping and LGV testing in HIV-infected MSM and support a possible role for empiric treatment for LGV in asymptomatic anorectal CT infections when serotyping is not available. 5,21
A strength of our study was the prospective collection of data from a unique population of high-risk MSM. We included important behavior and sexual risks in our data collection to help identify specific risks associated with STI incidence. Although the results support the need for triple-site NAAT testing in sexually active MSM, we acknowledge several potential limitations. First, our study was from a single center and the majority of the patients had similar demographic profiles, so results may not be generalizable to other populations with divergent STI incidence rates. In addition, we used self-collected specimens which may have affected sample quality. However, accuracy of self-taken specimens for diagnosis of STIs from both pharyngeal and rectal sites in asymptomatic patients has been assessed in several studies and compared favorably to clinician-collected samples.22,23
This study highlights the importance of extra-genital testing for CT\NG among sexually active MSM while also emphasizing the limitations of lone urine-based STI screening. STI rates in the US have been markedly increasing, reaching an all-time high in 2018 and marking the fifth consecutive year of increases for CT and NG. 24 The FDA approval of extra-genital screening in 2019 25 was a crucial step for improving the screening of asymptomatic patients. However, the COVID-19 pandemic has had a worldwide impact on the availability of STI PCR testing due to reallocation of resources for COVID-19 testing. These competing priorities (rising STI incidence and limited PCR resources) suggest that novel strategies for testing, such as the pooling of three-site tests or limiting the use of urine-based testing, combined with prevention efforts, are needed. Furthermore, the substantial burden of asymptomatic STIs in PrEP users suggests that possible advocacy for barrier protection, enhanced surveillance with every 3 months screening and/or other strategies to mitigate STI burden should be considered in this group.
Our study found a substantial prevalence of CT and NG infections in Israeli MSM with the highest proportion of infections among PrEP users. STI screening strategies for asymptomatic MSM, particularly those on PrEP, should include extra-genital sites.
Footnotes
Acknowledgments
We are grateful to Cepheid for the provision of Xpert CT/NG cartridges for this study.
Author contributions
Shlomo Pilo, Ministry of Health, National Public Health Laboratory, Tel Aviv, Israel. For analyzing the samples for Lymphogranuloma venereum. All authors contributed to drafting and revising the text and all authors approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the IRB of Tel Aviv Sourasky Medical center, Israel.