
Abstract
Background
Pre-exposure prophylaxis (PrEP) is an effective means of HIV prevention for men who have sex with men (MSM), a key population whose engagement is crucial for achieving effective public health outcomes. An optimal service model would be important in planning the implementation of PrEP in places where such service has not been established.
Methods
A qualitative study was conducted to delineate the attributes of an optimal PrEP service model for MSM in Hong Kong, a city where no formal PrEP programs existed. Twenty purposively sampled MSM who were enrollees of two pilot PrEP projects participated in the semi-structured interviews promoting story-telling. The coded data were thematically analyzed following Grounded Theory approach, focusing on uncovering a typology of the essential attributes of an optimal PrEP service model, and the reasons for such preferences.
Results
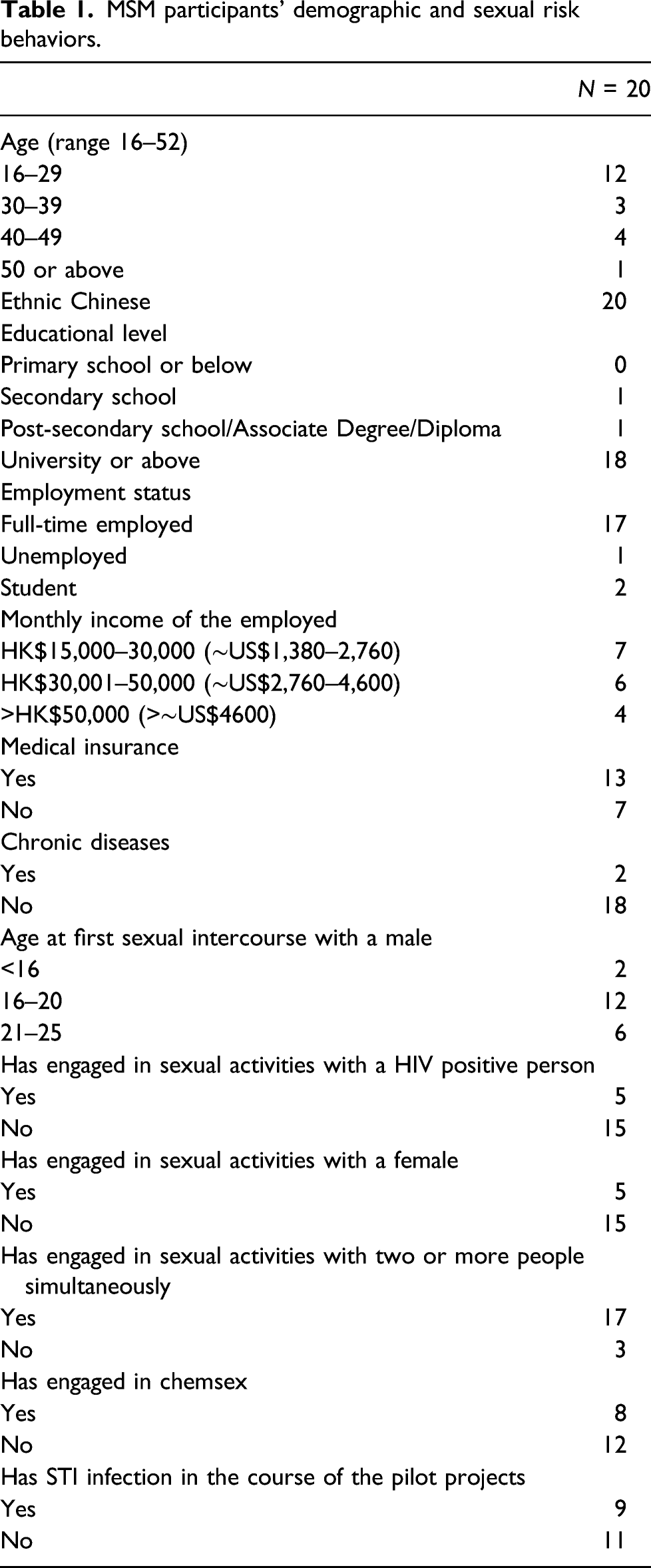
Participating MSM were all ethnic Chinese and aged 26 to 52 years. All had received PrEP from pilot projects in conjunction with periodic screening of sexually transmitted infections (STI), HIV antibody, and plasma creatinine. Four major themes emerged as regards the attributes of a preferred PrEP service: (i) comprehensiveness of HIV/STI and safety monitoring; (ii) convenient unitary service; (iii) stigma-free PrEP access and protecting confidentiality; and (iv) affordable price. Whereas regular provision of PrEP was acceptable to MSM, unaffordability and related stigma were the anticipated challenges for potential service providers.
Conclusions
The qualitative assessment of MSM’s preference for PrEP service delivery has yielded important information on the many facets of a desirable service model.
Keywords
Introduction
The efficacy of pre-exposure prophylaxis (PrEP) for preventing HIV transmission has been well-established in clinical studies.1–4 In real-world settings, providing PrEP as part of a combination package of HIV prevention services in San Francisco in the US, 5 Australia, 6 and London in the UK 7 has created impacts in significantly minimizing HIV transmission. The unprecedented increase in efforts of PrEP implementation is evidenced not only by its extensive rollout in Western countries, but the accelerated development of pilot programs targeting key populations in Southeast Asia. 8 Following recommendation by World Health Organization (WHO), national guidelines of PrEP implementation were in place in 35 countries by 2018. 9 Despite global recognition of the effectiveness of PrEP, its uptake has remained suboptimal with no more than one million people worldwide taking PrEP as of 2020. 10
Globally, men who have sex with men (MSM) are at higher risk of HIV transmission, but their uptake of PrEP has remained variable. High awareness of PrEP was not paralleled by a high degree of willingness to take PrEP.11–15 As in many places in the world, MSM constitute the key vulnerable population with high risk of HIV infection in Hong Kong. In 2019, MSM accounted for 69% of all reported new infections among males. 16 In the absence of any regular PrEP program in the public service, only 3.5% of MSM interviewed in a territory-wide survey in Hong Kong had ever accessed PrEP. 17 In the planning of PrEP for MSM, the implementation challenges include not just the local health system’s characteristics but also the acceptability of the service. Offering PrEP as part of a comprehensive HIV prevention strategy that included ongoing risk reduction counseling was reported to moderate risk compensation. 18 In accessing PrEP, cost has been shown to have significant implications on one’s decisions to use. 19 Inequity of access was a deterrent to effective provision of PrEP, as shown in Northern and Central England, suggesting the need to outreach segments of populations with specific demographics. 20 One characteristic of delivery models that is likely to affect its success is “decentralization of services” via mobile service and peer-led community-delivered services, which was particularly effective in suburb areas. 21 Moreover, ease of accessing services and convenience of medication collection have been found to be associated with substantial interest in PrEP. 22 Whereas the insights generated by previous literature are crucial, the community’s perspective is needed to address relevant attributes of a PrEP service model that appeals to the users, so as to meet their needs and preferences. A qualitative study was conducted by interviewing MSM participants of two pilot PrEP projects in Hong Kong to assess their preferences in real-world context by drawing their experiences of PrEP access.
Methods
Study design
Qualitative approaches in healthcare studies enable researchers to depict voices of what they mean for an individual, adding richer knowledge with meaningful data, 23 which could support strategies for increasing PrEP uptake. Story-telling through semi-structured interviews allows investigation of live experiences that offers insights for phenomena in a specific context, 24 providing reflections from the vulnerable community. 25 This study was conducted on purposively sampled MSM who had taken part in two pilot PrEP projects in Hong Kong, a city where PrEP services have not yet been established. We adopted a qualitative approach to make an in-depth inquiry about how and why PrEP users had perceived PrEP delivery, with the objective of eliciting perspectives and meanings in response to open-ended questions. An emphasis was placed on storytelling, which is a powerful tool to communicate data-rich accounts of their sexual health needs and to share lessons from participation in the pilot projects. The interviews were conducted by the first author. Face-to-face individual interviews in Chinese took place at the meeting room of our Research Centre, located separately from the Pilot PrEP Clinic and with participants’ privacy protected. Anonymity was maintained throughout the interviews.
Participants and recruitment
Twenty MSM who had enrolled in one of the two pilot projects that provided co-formulated tenofovir disoproxil fumarate 300 mg and emtricitabine 200 mg (TDF/FTC) for PrEP in Hong Kong were recruited. All participating MSM were HIV antibody negative, HBsAg negative and had an eGFR of >60/mL/min/1.73 m2. They met the inclusion criteria of (i) history of unprotected anal sex in the preceding 6 months; (ii) negative HIV antibody within the last 3 months; and at least one of the following in the preceding 6 months: (iii) history of sexually transmitted infection (STI) diagnosis(es); (iv) having sex partner(s) who were living with HIV or people with unknown HIV status; (v) having more than one sex partner; and (vi) history of sexualized use of drug (chemsex). The first project offered partially self-financed TDF/FTC for daily PrEP (n = 71); the logistical procedure of which has been described elsewhere. 26 The second project was a cross-over study (n = 119) involving the prescription of free daily followed by on-demand PrEP and vice versa each for a period of 16 weeks. 27 During the on-demand phase, participants took two tablets of TDF/FTC 2–24 h before sex followed by one tablet each at 24 and 48 h afterwards, referenced from the regimen for the IPERGAY study. 28 In the course of the two pilot projects, participants were regularly monitored with point-of-care (POC) and laboratory tests for HIV infection (4th generation HIV antibody tests), plasma creatinine and STI, the latter including syphilis serology, Chlamydia trachomatis (CT), and Neisseria gonorrhoeae (NG) nucleic acid tests (NAT).
Data collection
A semi-structured interview guide was designed based on a review of related literature18,19 before the commencement of the study. It consisted of a list of sub-topics to address MSM’s experience of PrEP use during the pilot projects, namely: (i) motivations for PrEP and risk perception; (ii) potential sexual behavioral change following PrEP use; and (iii) preferences of PrEP delivery models, their acceptability and future engagement in PrEP services. Participants were encouraged to draw from their experiences with the current PrEP projects to suggest the characteristics of components required for a PrEP service and the reasons for their preferences. Questions relating to the location of the clinic, setting, appointment scheduling, quality of communication with physicians, views towards sample collection technique and testing frequency, and anticipated challenges to PrEP use including cost of medication were inquired. Probes were made when clarifications were needed to increase the depth of knowledge. Interviews each lasting 45–90 min were audio-taped. Each participant received a HK$100 (∼US$13) supermarket coupon as a token of appreciation. Data collection continued until saturation was reached by interviewing 20 participants. Ethical approval for this study has been obtained from the Joint Chinese University of Hong Kong – New Territories East Cluster (CUHK-NTEC) Clinical Research Ethics Committee (CREC Ref. No.: 2016.470)
Data collation and Analysis
Audios were fully transcribed in Chinese for coding, and selected quotes representing identified themes were then translated to English at a later stage. A coding framework was first established by engaging our Research Team members to independently code the first four transcripts (20% of total transcripts) that involved a reiterative reading and coding of text with inductive and deductive codes. The agreed coding framework reaching intercoder reliability was then applied on the remaining transcripts, using NVivo 12 qualitative data analysis software. The coded data were thematically analyzed following Grounded Theory approach, 29 focusing on uncovering a typology of the essential attributes of an optimal PrEP service model, and the reasons for such preferences. Findings were reviewed by Research Team members—to appraise, discuss, and reach consensus with the themes generated.
Results
MSM participants’ demographic and sexual risk behaviors.
Theme 1: Comprehensiveness of HIV/STI (sexually transmitted infection) screening and safety monitoring
Almost all MSM participants expressed their positive attitudes toward the provision of HIV/STI testing in conjunction with PrEP prescription. Some described that the comprehensiveness of testing was most beneficial in giving them a greater sense of “extra protection” and for their “peace of mind.” Many elaborated on the necessity to receive HIV and STI testing in circumstances of increased risk of exposure, such as “unsafe sex,” and the scenarios of having sex with a person living with HIV without definitely knowing his HIV status. “I had fun with someone who later told me that he got AIDS,” one MSM reported. Several participants described receiving a HIV negative result has “convinced” them that PrEP was effective and justifiable to continue, and many regarded that regular monitoring was acceptable. A majority noted the needs to monitor “potential side-effects,” for example decreased eGFR. Some took regular testing as a strategy allowing timely treatment than being “too late when you feel something goes wrong.” Overall, the frequency of attending clinic every 1–3 months was perceived to be within the acceptable range. “I’m taking the tests more regularly and thus I feel I’m so much healthier than before!” as several reported.
Theme 2: Convenient unitary service
The majority spoke about the convenience of PrEP access as a significant factor contributing to their satisfaction. The pilot projects were viewed as a “unitary service” with the provision of PrEP medication in conjunction with the aforementioned testing procedures (Theme 1). Some specified the need for one-stop service in the same clinic, and regarded it “troublesome” to collect the pills separately from the pharmacy. Some identified the need for real-time actionable results, with the presence of physicians who supported linkage to care and treatment. “I get tested, with testing results generated immediately, then having physicians explain the conditions,” one MSM reported. The majority felt most confident when knowing physicians were taking the leading role, as one explained, “Seeing physician must precede the prescription of PrEP, because after all, the drug may have side effects.” Some highly valued the ease with self-collection of samples for testing STI at the clinic by “reading instructions along with illustrations posted on the wall,” and some regarded taking one’s own samples, without eroding their privacy, was clearly preferred.
Theme 3: Stigma-free PrEP access and protecting confidentiality
A stigma-free service protecting confidentiality was preferred by most MSM, but exactly how and where PrEP should be implemented was met with mixed opinions. Some described their concerns that an integration of PrEP in the routine HIV services would lead to the labeling of PrEP users as “HIV infected patients.” One explained, “…because people, generally holding negative views towards HIV, would take on a distorted view if it’s placed within the HIV Treatment Centre.” Some anticipated public hostility to people utilizing designated PrEP service. As one explained, “I think having a separate delivery mode for PrEP is inappropriate, because it’s like having everyone go to a designated place, and that would turn out like a Drug Abuse Clinic, so any person getting in there is for the drug…” A few anticipated the capacity of a standalone delivery model in providing linkage to HIV care and dealing with the psychological burden should a PrEP user become diagnosed with HIV infection. “Then he needs to go through everything again from assessment to everything else that would lead to repeated conversations (with (healthcare workers) HCW) and very likely, adding to a further burden to the client who’s already burdened,” explained another participant. Others remarked that they had no preference for any particular PrEP delivery model as long as its delivery site would not compromise their privacy, such as “not located in busy spot,” and establishing steps to protect privacy in waiting area. As one explained, “…because at the end of the day...homosexual identity is not something that I can tell others, in addition to the sexual behaviors I’ve engaged in.” The potential of gay-friendly NGOs, where “higher level of privacy” was maintained, in delivering PrEP was acknowledged. Others expressed concerns about PrEP access “…for someone who really doesn't want to disclose one’s sexual identity, one tends to be more reluctant to visit or show up at these places” because their attendance would equate to acknowledgment of homosexuality.
Participants expressed that the non-judgmental attitude of medical staff towards MSM was treasured. The approachability of medical professionals had promoted effective physician-patient communication, as one reported, “I’m comfortable with the physicians here and I can candidly respond though these questions are very personal and sensitive!” Inability to achieve patient respect in the PrEP service context was a concern, as recalled by an MSM commenting on services previously received, “Those (medical staff) from the government service were so snappy. They’re very rude...they see us as “sinners” or “promiscuous people!” These participants, suggested that “…increasing training for HCW, regarding (physician-patient) communication, is needed if the government intend to initiate PrEP service in the future.”
Theme 4: Affordable price
Lower price (approximately one-third of market price via the first pilot project) and free PrEP (via the second pilot project) were considered acceptable means for PrEP access by all MSM participants, while acknowledging the support of funding source for these projects. As one MSM noted, “I believe that a pill costing HK$188 is not affordable for most people of my age, or any Hong Kong people with a similar financial background as mine.” Others voiced that the role of the government in delivering PrEP at affordable price was a critical component of successful implementation, which required strategies of “regulation of market price,” and “provision of subsidy.” Without funding for future research-based PrEP programs or government support for regular PrEP services, the most cited alternative was traveling overseas, for example, to Bangkok for purchasing generic TDF/FTC pills at a much cheaper price despite the uncertainty of the availability of regular monitoring. As one reported, “I think I’ll go get it in Thailand, where testing for the first time seems available, but not including regular monitoring afterwards…”
Discussion
Based on MSM’s experiences in the pilot PrEP projects, four major themes were uncovered in our study that reflected important attributes of PrEP service models in Hong Kong: (i) comprehensiveness of HIV/STI testing and safety monitoring; (ii) convenient unitary service; (iii) Stigma-free PrEP access and protecting confidentiality; and (iv) affordable price. The preference for incorporating regular testing in PrEP services was different from published studies which reported that regular monitoring was considered troublesome by PrEP users.30,31 Our study instead highlighted MSM’s recognition of HIV and STI risk as well as protection from adverse effects from antiretrovirals. MSM diagnosed with STI were referred to specialist services for treatment while those tested negative felt safe in their sexual relationships. Instead of tedious sampling and laboratory testing, the application of simple POC methodology and self-sampling for STI screening and eGFR monitoring might have led to the favorable attitude of MSM participants in our study.
Central to participants’ experience in PrEP was their appreciation of the role of clinic physicians in providing appropriate professional advice on sexual health, health monitoring, and risk reduction consultations. In particular, MSM appraised the soft skills of PrEP clinic staff as effective communicators, contrasting their unfavorable experiences with stigmatized attitudes from HCW. However, this can only occur when HCW are equipped with the skills to engage clients to discuss about sexual behaviors.32–36 Some doctors were very cautious in prescribing PrEP because of concerns about possible emergence of drug resistance34–36 and considered it crucial to monitoring PrEP users vigorously. 34 Their views of the inevitable occurrence of risk compensation32–36 created challenges in promoting PrEP provision. Negative attitudes of HCW toward PrEP could adversely affect their communication with potential PrEP users 37 or even their own decisions to prescribe PrEP. 38 Depriving eligible MSM from PrEP access because of the anticipated risks of fueling STI infections may not be in the best public health interest. 39 Studies in different nations, such as the US,35,40 Canada, 35 Kenya, 41 and Belgium 42 demonstrated the importance of capacity development for HCW to enhance PrEP delivery to achieve successful scale up. Our findings lend weight to the non-judgmental attitudes of HCW as one of the major components of an effective PrEP service.
Views of MSM on the precise mode of PrEP service delivery in Hong Kong were divided. A universal factor was a preference for facilities that could be stigma-free. Integrating PrEP in the routine HIV services in the public sector was valued for its capacity to provide continuum of HIV care from prevention through treatment. There was however the perceived stigma of being inadvertently labeled as a person living with HIV. The stigma attached to one’s “HIV status” has persisted within healthcare setting/institution, and the fear of negative reaction from the public. This highlighted the irony of not preferring PrEP service to be associated with HIV infected people, which demonstrates the nested nature of AIDS/HIV stigma. On the other hand, the delivery of PrEP through designated specialized services may lead to another form of dual stigma—being identified as MSM as well as that of “promiscuity” attached to PrEP. Our results are consistent with previous literature demonstrating stigma as a salient barrier that could undermine PrEP access. 43
One most prominent theme of our findings was the affordability of PrEP, which was in line with that of the other studies reported in countries and regions in Europe, 44 Asia,44,45 and North America.38,46 Guidelines on PrEP promulgated by WHO have highlighted that equitable access will contribute to reducing health disparity gap. 47 In Hong Kong, the current price of the medication per month is around HK$6000 (∼US$770), 48 and up to $8000-$10,000 (∼US$1025–1280) if check-ups and monitoring are included as in the private sector, 49 which are generally unaffordable. Our MSM participants expressed concerns about cost burden locally, and their preference for making overseas travels for generic PrEP or purchasing online despite their awareness of the insufficiency of health monitoring. In the development of a PrEP service, it is crucial that this is affordable for eligible persons, as sustainability is important for a preventive measure that needs to be adopted over an extended period of time. The ultimate cost to PrEP users and the society would vary with the adopted regimen, mode of funding and that of the operation. While this current study captured the attributes of optimal PrEP service for MSM, there are notable hesitancy issues, such as low risk perception, 50 concern of side effects,51–53 and non-adherence to daily regimen, 50,54 which may not be addressed even with an optimal service model. Wider community education is needed to promote awareness of not just PrEP users and health service providers.
This study carried several limitations. The findings generated were based on the analyses from a small number of MSM recruited from a Pilot PrEP Clinic located in a teaching hospital in Hong Kong where PrEP was delivered through time-limited studies. Extrapolation of the results to the whole of Hong Kong or other places must be cautioned. There were potential biases of views of MSM who had been motivated to join pilot projects in the first place. To minimize biases, the interviews were conducted by the first author, who was independent and had not been involved in the implementation of either pilot projects from which participants were recruited. The dataset was subsequently de-identified before proceeding with the analysis process. Unlike quantitative research, this qualitative study has not been organized to seek to produce generalizability, but rather to yield data-driven insights on how PrEP services are preferred to be delivered. We believe our study produces practical knowledge, and is relevant to the way that PrEP-related health services are to be developed.
In conclusion, our qualitative assessment of MSM’s preference for PrEP service delivery has yielded important information on the many facets of a desirable service model. There are major challenges of the anticipated PrEP-related stigma, the importance of equipping HCW with cultural competence and acceptance, and the need for affordable PrEP services.
Footnotes
Acknowledgements
We would like to acknowledge for all the participants who contributed to our in-depth interviews, and research assistants and PhD students, who transcribed the interviews.
Conflicts of interest/Competing interests
The authors have no conflicts of interest to declare that are relevant to the content of this article.
Funding
This work was supported by Council for the AIDS Trust Fund (Grant number: MSS321R)
Ethics approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Joint Chinese University of Hong Kong – New Territories East Cluster (CUHK-NTEC) Clinical Research Ethics Committee approved this study.
Consent to participate
Written informed consent was obtained from all individual participants included in the study.
Consent for publication
We give consent for this manuscript to be published.
Availability of data and material
The datasets generated during and/or analyzed during the current study are not publicly available as the disclosure of detailed personal information could compromise the privacy of research participants.
Code availability
Not applicable.
Authors’ contributions
JYCL designed the qualitative methodology. JYCL conducted interviews and processed data. JYCL, NSW, and SSL conducted analysis and data interpretation. JYCL wrote the first draft of the manuscript. NSW, KCKL, THK, GCYL, DPCC, and SSL critically revised the manuscript. SSL conceived ideas and supervised the study. THK managed procedural arrangement. All authors reviewed and approved the final version.