
Abstract
A large number of countries are being confronted with twin epidemics of increasing STI incidence and antimicrobial resistance (AMR). This has led to calls to intensify STI screening of high STI prevalence populations. The available evidence suggests that this will have little impact on STI prevalence but a significant deleterious effect on AMR. We suggest that this call to intensify STI screening is one of the several errors that stem from the way that the STI-field has been dominated by a biomedical individualistic conceptual framework. This framework views STIs as obligate pathogens that can and should be eradicated by intensive seek-and-destroy activities. We evaluate five types of evidence that suggest that a multi-level, socio-ecological framework would provide a more accurate portrayal of the important determinants of STI prevalence and AMR spread. By incorporating concepts such as limiting STI screening to scenarios with clear evidence of net-benefit and considering ‘antimicrobial footprint’ thresholds, this framework would be more likely to result in a better balance between targeting STI prevalence whilst minimizing the risk of AMR emerging.
Keywords
Background
All disciplines operate within a conceptual framework. This conceptual framework determines how we structure our ideas to bring facts together in a way that they form a coherent whole.1,2 An optimal theory of the determinants of STI prevalence should thus provide an accurate portrayal of all the important determinants in a way that illustrates the interrelationships, the relative importance of the various determinants and facilitates proportionate and effective responses. 2 If the theory privileges certain causes over others, then it should be replaced by a theory which does not do this.2,3 In this viewpoint, we argue that evidence that has emerged over the past few decades suggests the need for the STI field to transition from a predominantly biomedical individualist to a more explicitly eco-social conceptual framework. This argument is not new.4–6 Rather our viewpoint focuses on five types of recently published evidence that further expose the limitations of the biomedical individualist approach. In particular, we focus on how the biomedical individualist approach has resulted in massive and harmful levels of antimicrobial consumption in key populations. We then examine positive evidence of how an eco-social framework would provide a more complete framework for STI epidemiology and help reverse this excessive antimicrobial consumption.
The STI-treatment-can-eliminate-STIs era of STI control (a brief history)
A particularly dramatic transition in conceptual frameworks in the health sciences was the switch from miasma- to germ theory in the 19th century
2
Microbes were identified as being responsible for specific diseases and later found to be susceptible to antimicrobial therapy.
7
Syphilis was, for example, found to be caused by a specific spirochaete, Treponema pallidum, which was in turn found to be susceptible to antimicrobials such as penicillin. If syphilis infections could be detected early and treated, then onward transmission could be halted, and the disease controlled or even eradicated.
8
Widespread testing and treatment were indeed thought to have played an important role in the decline in the incidence of syphilis incidence in the post-World War II period in numerous regions around the world.8–10 Other bacterial STIs such as chlamydia, gonorrhoea and chancroid were similarly found to be caused by specific bacterial species that could be cured with specific antibiotic therapies. The successes of this approach resulted in this intensive STI screening/treatment paradigm dominating the STI control field up to the contemporary period.11,12 One foundational principle of this conceptual framework was that if STI screening, diagnosis and treatment was intensive enough, then STIs could be eliminated or near-eliminated (Figure 1, Table 1).
13
A corollary to this theory was that discrepancies in STI prevalence between populations could be largely explained by differences in the availability of efficacious STI services.
12
Chesson et al., for example, argued that ‘to a large extent, inadequacies in health service provision and health care seeking are responsible for the high levels of STIs and the high rates of complications and sequelae in low and middle-income countries’.
12
Likewise, the increasing incidence of STIs in many countries around the world over the last two decades are seen as requiring intensification of this seek-and-destroy approach (screen for STIs as broadly as possible and eradicate STIs in those testing positive)14,15 As an example, screening for STIs such as chlamydia/gonorrhoea in MSM, particularly in HIV preexposure prophylaxis (PrEP) cohorts, has been intensified in numerous guidelines8,16 In a similar vein, the World Health Organisation (WHO) has published a plan to reduce the incidence of gonorrhoea, chlamydia and syphilis by 90% by the year 2030 using strategies such as intensified screening and treatment of STIs in high prevalence populations.
17
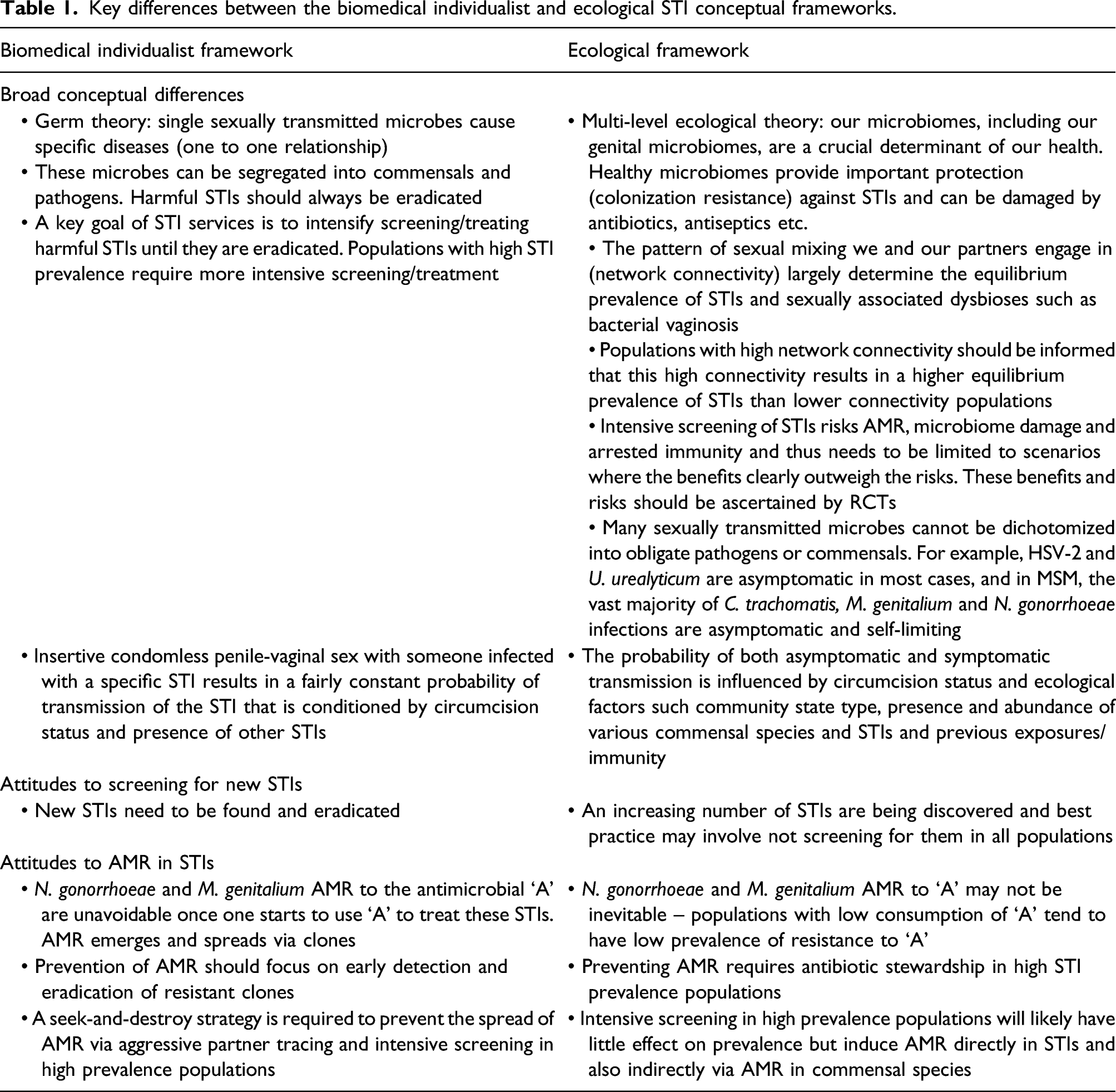
According to the biomedical individualist framework (left), the prevalence of STIs is determined by downstream factors such as insufficient STI screening and treatment (A). Intensified screening and treatment results in the eradication of N. gonorrhoeae (yellow bacteria) from the grey individual (B). Populations are seen as largely composites of individuals/partnerships and hence intensive screening is predicted to eradicate N. gonorrhoeae at a population level too (B). By eradicating N. gonorrhoeae, intense screening reduces the risk of AMR emerging in N. gonorrhoeae (C). In contrast, the ecological framework interprets the high N. gonorrhoeae prevalence as a function of the dense local sexual network (grey bars represent active sexual partnerships). Whilst intensive screening and treatment will likely eradicate N. gonorrhoeae from a particular individual following an episode of screening, this individual is at high-risk of reinfection as a number of his partners and their partners are infected. Treatment also results in antimicrobial resistance in his commensal bacteria (red bacteria) and a loss of bacterial diversity including possible colonization resistance (bacteria with dashed outlines represent eliminated bacterial species). A subsequent gonorrhoea infection from one of his partners (dashed arrow) can then acquire the new AMR from the commensal bacteria via transformation (double headed arrow). Furthermore, the intense screen/treat intervention will have no impact on network connectivity which is the underlying determinant of the high N. gonorrhoeae prevalence. If screening reduces N. gonorrhoeae (C) this will create a selection pressure for N. gonorrhoeae to acquire AMR so as to enable it to return to its equilibrium prevalence for this degree of network connectivity. Key differences between the biomedical individualist and ecological STI conceptual frameworks.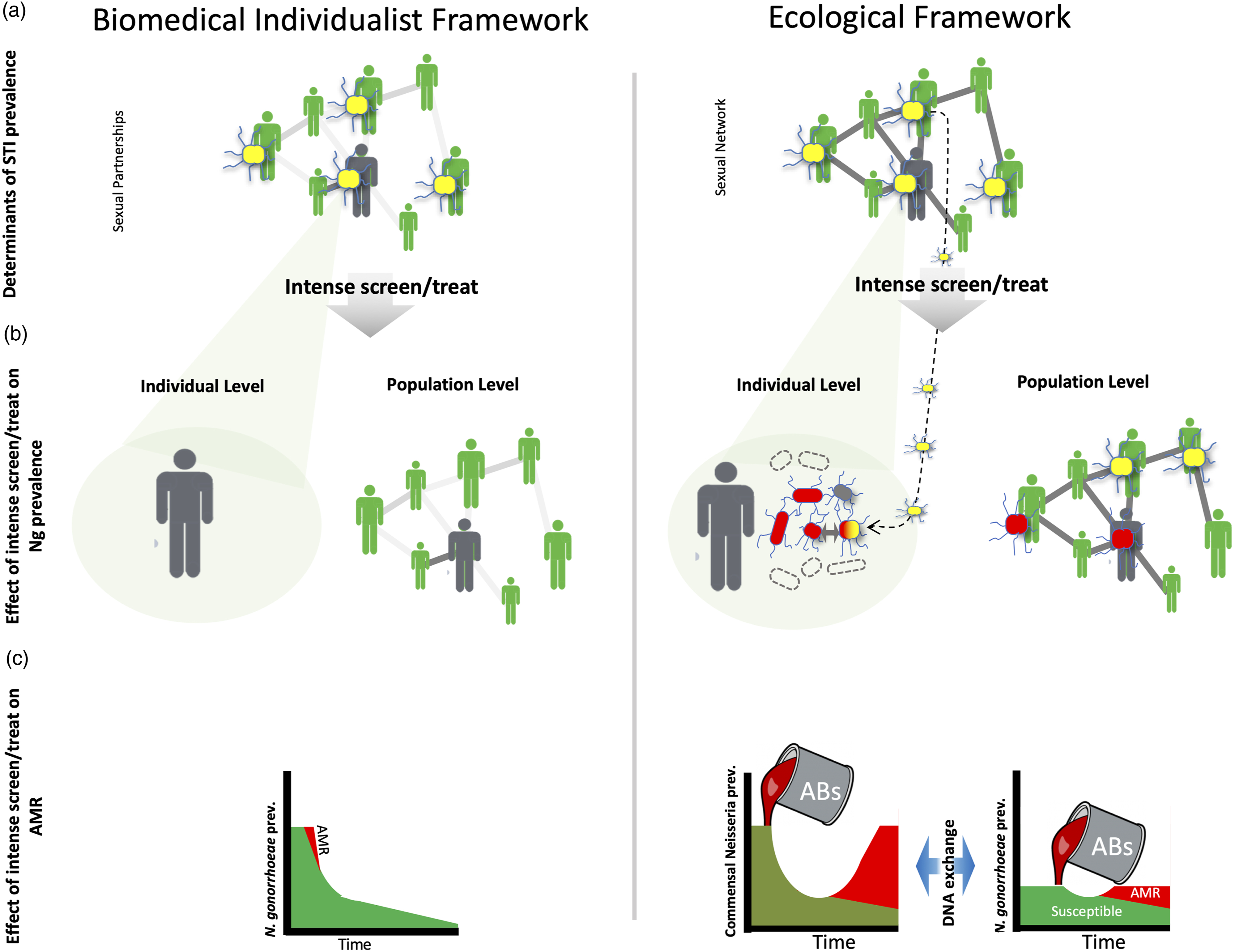
A number of authors have termed this intensive-screen/treatment perspective the biomedical individualist framework because the paradigm focuses on individual humans or microbes as the basic level of analysis.4,5,18 STI prevalence is viewed as being largely dependent on factors relating to biomedical interventions – such as the adequacy and intensity of STI screening and treatment, condom use and circumcision prevalence.5,8,11 The focus is ‘downstream’ – on microbes and individuals.11,13 Little attention is paid to the ‘upstream’ factors such as the connectivity of local sexual networks which determine the prevalence of STIs. 4
Five limitations of the biomedical individualist framework
STI prevalence is a function of sexual network connectivity and not STI treatment efficacy
A range of different types of evidence suggests that the prevalence of individual STIs is predominantly a function of the degree of connectivity of the population’s sexual network (reviewed in11,13,19). As an example, increases in STI incidence in high-income countries in the last two decades have occurred not as a result of declines in the quality of STI services but rather largely as a result of increases of network connectivity (largely declines in condom usage and increases in partner numbers) in men who have sex with men (MSM; Figure 2).5,8,20 Likewise, the dramatic declines in syphilis incidence in MSM in high-income countries in the 1980s had little to do with changes in STI treatment efficiency. Instead, they were a result of changes in condom usage, the number of partners and AIDS deaths, all of which reduced sexual network connectivity.5,21 Appreciating that dense sexual networks underpin the rises in STIs is crucial because radical STI prevention would require reducing this connectivity.5,22 The ‘zero-grazing’ campaign in Uganda is one example of how interventions targeting network connectivity can reduce STI incidence.
22
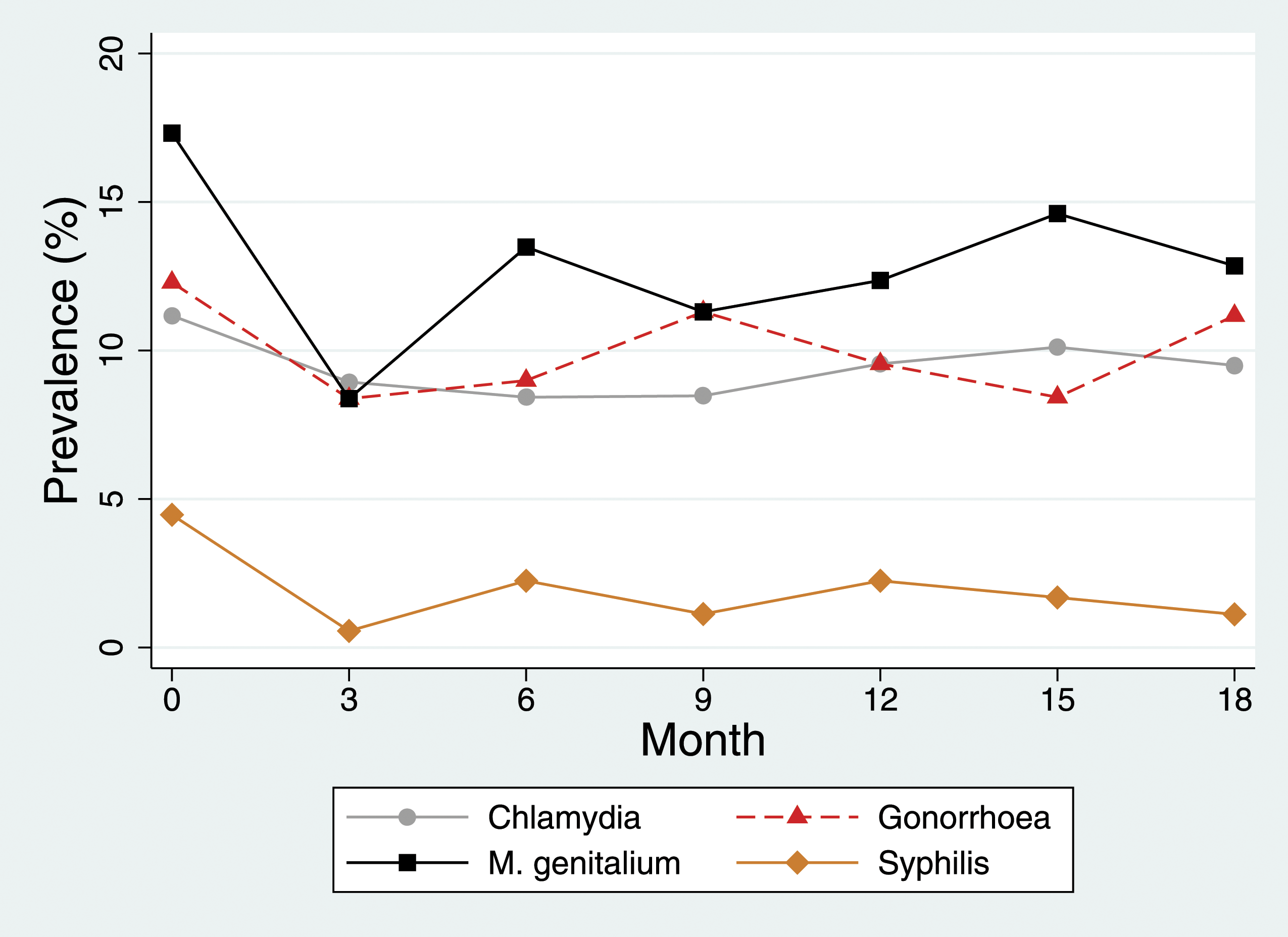
Being focused on individuals and microbes, the biomedical individualist framework has paid insufficient attention to this fundamental connection between sexual network connectivity and STI prevalence.16,23 MSM PrEP cohorts offer a useful example. These cohorts typically report approximately a median of 5–10 partners per 3-month period.24–26 This translates into equilibrium prevalences of around 10% for each of C. trachomatis, M. genitalium and N. gonorrhoeae (Figure 3).16,25,26 Estimated annual incidence of primary/secondary syphilis among MSM and heterosexuals in the United States, 1963–2013, and cases of primary/secondary syphilis in men and women in the United Kingdom, 1960 to 2015. The approximate timing of the AIDS epidemic and introduction of antiretroviral therapy (ART) are indicated with arrows (modified from 5,8). Prevalence of bacterial STIs (%; C. trachomatis, M. genitalium, N. gonorrhoeae, T. pallidum) in the BePrEPared Study in Belgium. In this PrEP observational study in Belgian men who have sex with men, these four STIs were tested for at three monthly intervals and all STIs (excluding M. genitalium) treated if detected at each visit.26,45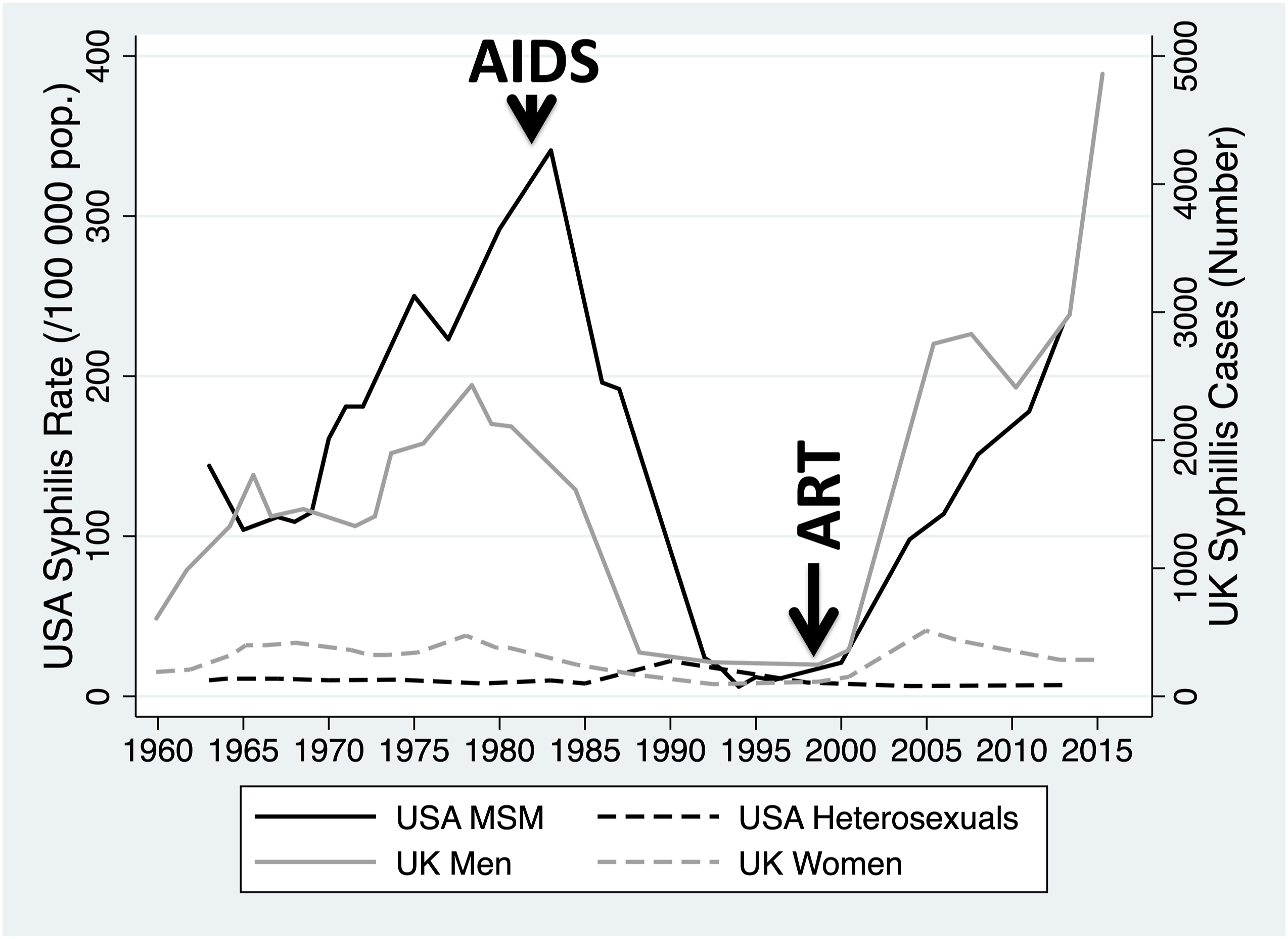
There is also compelling individual-level evidence that the incidence/prevalence of most STIs increases with lifetime number of partners (Figure 4). A population-based survey from a mining town in South Africa, for example, found that the seroprevalence of HIV in young women increased from 7% to 62% in those reporting 0 and 4 or more lifetime sex partners, respectively. The corresponding increase for herpes simplex virus-2 (HSV-2) seropositivity was even more dramatic – from 9% to 86%.
27
Similar associations have been found in other STIs such as Chlamydia trachomatis, human papillomavirus, N. gonorrhoeae, Treponema pallidum, Trichomonas vaginalis, hepatitis C and genital mycoplasmas (reviewed in
5
). Positive association between lifetime numbers of sex partners and (a) human papillomavirus (HPV), (b) bacterial vaginosis (BV) and herpes simplex virus-2 (HSV-2) in non-Hispanic black (red line) and non-Hispanic white (blue line) women in the United States of America. One reason for the left shifting of the non-Hispanic black plot is the higher sexual network connectivity of this population.5,19 All the data come from different samples taken from the National Health and Nutrition Examination Survey (figures produced using WebPlotDigitizer-4.2 from figures in 39,118,119).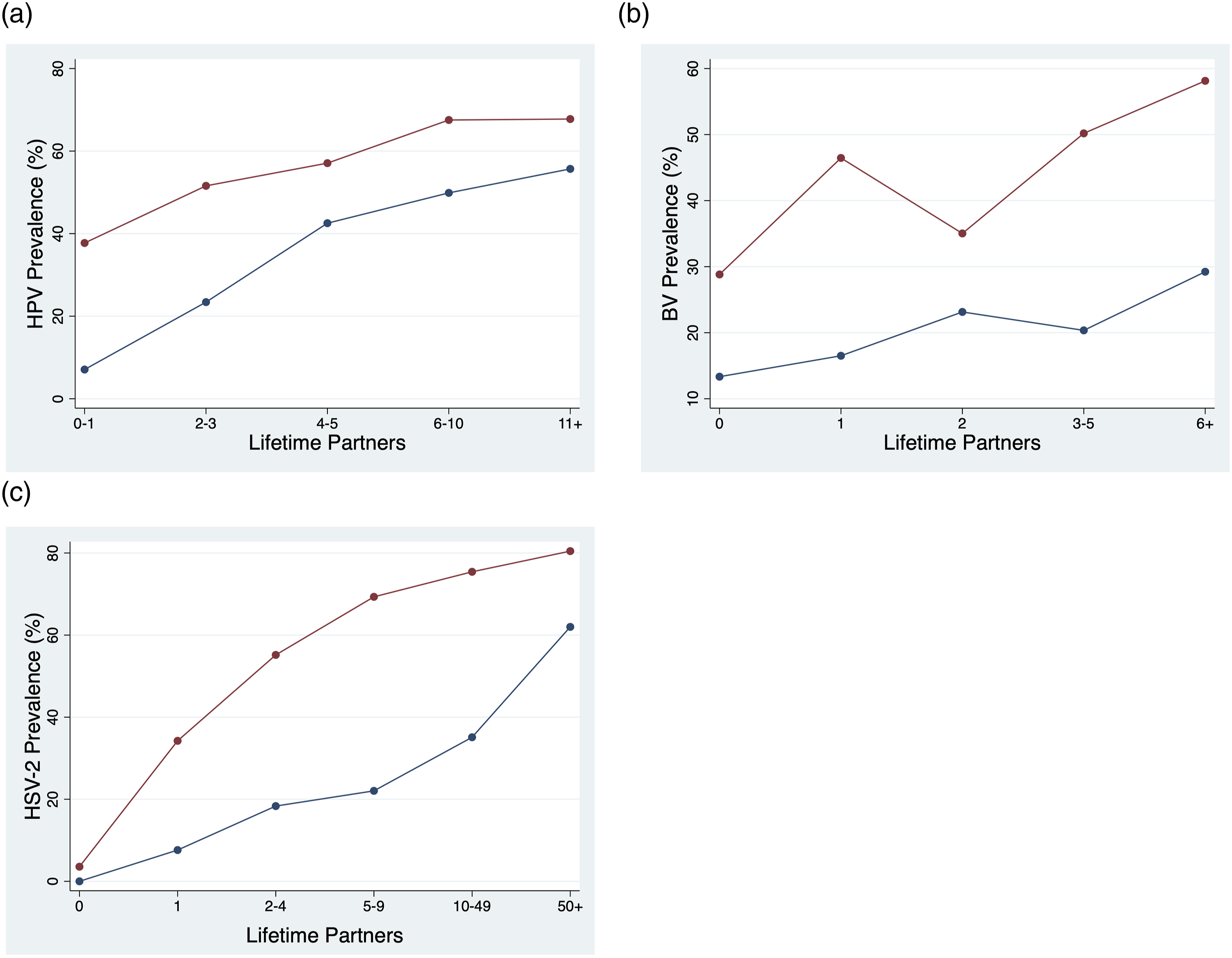
Positive associations have also been found between the number of lifetime partners and the prevalence of bacterial vaginosis (BV; Figure 4).28,29 An increasing body of evidence has emerged that suggests that BV is a polymicrobial community state type whose component bacteria are transmitted via sex .30–33 Although the probability of BV is influenced by a myriad of risk factors,30,31,34,35 one plausible reason for the large differences in BV prevalence between populations is related to differences in sexual network connectivity.29,36–38
Of note in particularly dense networks, the majority of individuals may be HSV-2 positive or have BV.27,37 The same may be true of individuals with high-risk behaviour in lower connectivity populations (Figure 4).5,39 There is no evidence that we could find that screening/treatment would reduce the prevalence of HSV-2 or BV in these populations. Rather these high prevalences can be productively viewed as the equilibrium prevalences for this degree of network connectivity.5,38
There is little or no evidence that intensive screening/treating STI has an effect on STI prevalence
By focussing largely at the individual level, the biomedical individualist framework assumes that screening and treating STIs such as gonorrhoea and chlamydia will reduce the prevalence of these infections (Figure 1). 18 Two cluster randomized controlled trials (RCTs) have, however, assessed the effects of repeated rounds of chlamydia testing targeting young men and women in the general population and found no reduction in estimated prevalence.40,41 Likewise, repeated population-based cross-sectional studies have found that screening had little or no effect on prevalence.42,43 The evidence base for screening gonorrhoea and chlamydia in populations with higher network connectivity like men who have sex with men (MSM) on PrEP is even poorer. No RCTs have been performed in MSM, and the observational data suggest that screening has no effect on prevalence. 16 Even three monthly, three site screening is not associated with reductions in incidence or prevalence (Figure 3).16,25 Likewise, the available evidence suggests that intensive screening does not have an impact on the prevalence of M. genitalium in MSM PrEP cohorts.44,45 The evidence base for screening other STIs such as HIV, hepatitis C and syphilis in populations such as MSM is however much stronger (reviewed in 46 ).
An increasing number of STIs are being discovered and it may be best to avoid screening for them
The number of microorganisms that can be transmitted via peno-vaginal and -anal sex, and cause symptomatic infections is expanding. For example, Leptotrichia/Sneathia spp, BVAB-2, BVAB-3, Mycoplasma penetrans, Neisseria meningitidis and Haemophilus influenzae have been found to be causes, or likely causes, of non-gonococcal urethritis.47,48 Likewise, a range of the human herpesviruses and arboviruses can be sexually transmitted and cause disease.49,50 Oral sex and kissing can result in the transmission of some of these same organisms as well as others such as commensal Neisseria spp.51,52 Seen from within the logic of the biomedical individualist framework, one may advocate intensive screening and treatment of these STIs in order to try and eradicate them. This is the approach followed in a number of centres worldwide where multiplex PCRs (targeting as many of the novel STIs as possible) are used for all patient groups (symptomatic and asymptomatic) deemed at risk of STIs. 53 One of these PCRs in clinical use, for example, targets three viruses (Cytomegalovirus, HSV-1 and HSV-2), 13 bacteria (C. trachomatis, Mycoplasma genitalium, Mycoplasma hominis, Haemophilus ducreyi, N. gonorrhoeae, Treponema pallidum, Ureaplasma parvum and Ureaplasma urealyticum, Strep. agalactiae, Escherichia coli, Gardnerella vaginalis, Atopobium vaginae and Lactobacillus crispatus) and Trichomonas vaginalis. 54
The fact that an organism is sexually transmitted is, however, insufficient evidence that it should be tested for or eradicated. Thus, although organisms such as U. parvum and M. hominis are sexually transmitted, they do not cause symptomatic STIs. 53 As such, various groups have argued that these species should be considered as part of the ‘normal’ genital microbiome.8,53,55 The prevalence of these organisms is also high. A recent study estimated that the prevalence of U. urealyticum, U. parvum and M. hominis in adult women to be 3–15%, 5–20% and 20–89%, respectively. 53 Prevalence is heavily dependent on risk behaviour. The prevalence of genital mycoplasmas in women, for example, increases from close to zero in those with no lifetime partners to 38% in those with one and 75% in those with three or more lifetime partners. 56 The widespread use of multiplex PCR tests will lead to a large proportion of those tested being diagnosed and treated for these ‘STIs’.53,57 In addition to the unnecessary economic costs this entails, there are also psychological costs (associated with being diagnosed with an ‘STI’) and risks associated with inducing AMR .53,57 These concerns led the European STI Guidelines Editorial Board to release a position statement arguing against testing for U. parvum and M. hominis in STI clinics and only considering testing for U. urealyticum in the setting of confirmed urethritis where no other cause is found and then only considering treatment if a high bacterial load is present. 53
Intensive STI treatment may prevent the emergence of immunity
U. urealyticum is only associated with urethritis in men with less than 10 lifetime sex partners, and the association is strongest in those with less than five partners. 58 The absence of an association between U. urealyticum and urethritis in those with 10 or more lifetime partners suggests that these individuals have acquired adaptive immunity. 58 This, in turn, suggests that early diagnosis and treatment may prevent the development of this immunity. This phenomenon may not be limited to U. urealyticum. A case control study, ecological-level studies and studies in animal models, have all found evidence that early diagnosis and treatment may prevent the acquisition of immunity to C. trachomatis infection.59–63
The significance of the detection of U. urealyticum is thus context-specific – men with more than 10 lifetime partners are more likely to be colonized with this organism but less likely to be symptomatic. Furthermore, men with more lifetime partners may be better off if they are not tested for the presence of this organism and treated as this might circumvent the emergence of immunity.
Our microbiomes are critical for our health and intensive STI screening strategies involve a high-risk for induction of AMR and dysbiosis including loss of colonization resistance
The biomedical individualist framework emerged at a time when little was known about the crucial role that the human microbiome plays in health. 64 Unsurprisingly, therefore, it paid little attention to how heavy antimicrobial exposure related to STI treatment may damage individual and population microbiomes. More recently, tremendous progress has been made in understanding the important role that our microbiomes play in the development and optimal functioning of most of our organ systems.65,66 A healthy vaginal microbiome, for example, is important for ensuring optimal pregnancy outcomes and protection against STIs.34,64 An increasing body of evidence points to the adverse effects of high-level antimicrobial exposure on the microbiome and other parameters of health.66–69 One of these concerns is that excessive antimicrobial consumption has played a role in the dramatic loss of microbial diversity in certain contemporary urbanized populations.67–71
Despite this evidence, very few empirical studies have assessed the adverse effects of high antimicrobial exposures such as those seen in PrEP cohorts. Intensive gonorrhoea/chlamydia screening in MSM on PrEP has been found to result in very high consumption levels of azithromycin and ceftriaxone.44,72 Both are broad-spectrum antibiotics that, according to the WHOs AWARE classification, should be reserved for infections where there is clear evidence of benefit and no alternatives exist. 73 Both have a large effect on human microbiomes.68,71 Screening PrEP cohorts for gonorrhoea/chlamydia three monthly, as advocated in numerous countries results in the consumption of approximately 12 defined daily doses per 1000 inhabitants per year (DID) macrolides.44,72 This exceeds the approximate thresholds for the induction of AMR in M. genitalium, Streptococcus pneumoniae and T. pallidum by 5- to 9-fold . 74 Furthermore, ecological studies from the United States and Europe have found evidence of an association between the intensity of gonorrhoea/chlamydia screening in MSM and the prevalence of gonococcal AMR.75–77 Studies of mass antimicrobial therapy for T. pallidum, N. gonorrhoeae and the related N. meningitidis have also found that mass treatment was associated with the emergence of AMR.12,78–80
Bystander selection of AMR
Intense screening will also induce AMR in other bacterial species via bystander selection. 81 A single dose of azithromycin, for example, results in steep increases in macrolide resistance in commensal streptococci. 82 The high levels of macrolide consumption levels resulting from screening in PrEP cohort have been found to be strongly associated with the induction of AMR in a range of pathobionts and commensals including group A streptococci and S. pneumoniae .72,82,83 Antimicrobial consumption has also been found to be a strong risk factor for AMR in commensal Neisseria.84,85 This is of critical importance because this AMR can be transferred to N. gonorrhoeae and N. meningitidis via transformation. 86 Phylogenetic analyses have confirmed that transformation from commensal Neisseria has played a key role in the genesis of cephalosporin, macrolide and fluoroquinolone AMR in both these pathogens.55,86 These findings have led to the pharmacoecological theory of AMR in STIs, which argues that an important part of the reason why AMR in N. gonorrhoeae, M. genitalium and T. pallidum has frequently emerged in core-groups is the combination of dense sexual networks and excessive consumption of antimicrobials. 23 As already noted, the dense networks typically seen in PrEP cohorts translate into a high equilibrium prevalence of around 10% for N. gonorrhoeae (Figure 3). 16 Seen from a biomedical individualist framework, this high gonococcal prevalence is likely to trigger enhanced screening and treatment. This may reduce the prevalence temporarily but the greater the reduction in prevalence, the greater the selection pressure placed on N. gonorrhoeae to acquire AMR which will enable it to return to its equilibrium prevalence for this degree of network connectivity (Figure 1(c)). 23 This AMR may be acquired by chromosomal mutations but it may also be acquired from commensal Neisseria who by virtue of their close to 100% prevalence in a human population are placed under an even greater selection pressure to acquire AMR by the high antimicrobial exposure (Figure 1(c)).23,87 Appreciating how placing dense sexual networks under high antimicrobial exposure can result in AMR is facilitated by ecological level thinking. 85
Loss of colonization resistance
A healthy microbiome also provides colonization resistance to pathogens.47,88 Broad-spectrum antimicrobials are known to lower the colonization resistance to new infection by up to 10,000-fold.66,89 No studies that we are aware of have evaluated what the effect of 12 DID macrolide consumption is on colonization resistance. Recent studies have, however, suggested that this may be important to investigate. Certain commensal Neisseria species have been shown to be able to protect against meningo- and gonococcal infection.90–92 An RCT investigating if regular mouthwash with an antiseptic that was bactericidal for N. gonorrhoeae could reduce the incidence of this infection in a PrEP cohort found that mouthwash use was paradoxically associated with an increased incidence of N. gonorrhoeae. 93 As a possible explanation, the authors suggested that the mouthwash may have eliminated the commensal bacteria which were protecting against N. gonorrhoeae infection. 93 Likewise, various commensal lactobacilli have been shown to protect against the acquisition of cervical gonorrhoea and other STIs.34,94,95 A similar phenomenon may apply to vaginal colonization by group B Streptococcus, where the presence of other beta-haemolytic streptococcal species appears to protect against the presence of this opportunistic pathogen 96 Although the data from other anatomical sites is less compelling, a number of studies have found that resident commensals such as certain streptococci may protect against gonococcal urethritis.97–100 If heavy exposure to antimicrobials had a detrimental effect on protective commensals, this could therefore increase susceptibility to STIs.
The case for an eco-social conceptual framework
Taken together, these five insights reveal serious problems resulting from the biomedical individualist STI framework and particularly so when considering high STI prevalence populations. The number of ‘STIs’ that is being tested for in symptomatic and asymptomatic individuals is expanding and more intensive screening is being promoted for STIs such as N. gonorrhoeae, C. trachomatis without any RCT-based evidence of benefit. The resultant antimicrobial exposure exceeds thresholds for induction of AMR in a range of bacteria. Intense treatment may also be exerting adverse effects on immunity, colonization resistance and dysbiosis. The WHO and other public health screening guidelines are clear that screening programmes should not be introduced until RCTs have been conducted that establish a net-benefit of such a programme.101–103 Given that such RCTs have not been conducted in high STI prevalence populations, it is appropriate to ask why screening for STIs such as gonorrhoea and chlamydia is being intensified in these populations? One possible explanation is that an individualistic focus has led to insufficient attention being placed on population-level processes such as the association between antimicrobial consumption and AMR. 104
An eco-social STI framework is simply a multi-level framework that includes interactions within and between factors at multiple levels such as subcellular, between microbes, individual humans, sexual networks and sociopolitical and economic contexts (Figure 1; Table 1).2,3,6,11,13,104 An advantage of explicitly adopting an eco-social STI framework is that it makes it easier to appreciate the connections between sexual behaviour, sexual network connectivity, resulting STI equilibrium prevalence and the probability of AMR emerging and spreading within individual Neisseria and other species given different levels of STI screening and antimicrobial consumption (Figure 1). If a clinician only considers an individual patient (biomedical individualist perspective), it is understandable how they might think that best practice for individuals from high STI prevalence populations would be intensive STI screening and treatment (Figure 1). If they were to operate from an eco-social perspective, they would, however, be more likely to appreciate the various reasons to be circumspect as regards intensive screening noted above. The mere fact that an organism can be sexually transmitted is insufficient evidence to target it for elimination or even label it as an STI. From an ecological framework, the appropriate exchange of microbiota is regarded as important for health.67,69 Using an eco-social framework, a reasonable case could also be made that certain of the classic bacterial STIs such as C. trachomatis, M. genitalium and N. gonorrhoeae should not be thought of as obligate pathogens.7,105 If these three organisms result in self-limiting, asymptomatic infections in over 90% of transmissions in MSM networks, then these organisms could be viewed as being opportunistic pathogens such as N. meningiditis or Staphylococcus aureus.7,81 Both of these species circulate at a high prevalence in certain demographic groups and although they can cause severe illness, this is infrequent.7,81,104 Furthermore, even though chemoprophylaxis/therapy may result in reduced carriage, this is generally not promoted outside of hospital settings as the reduction in prevalence is temporary and associated with the induction of AMR.104,106,107 If C. trachomatis, M. genitalium and N. gonorrhoeae were to be regarded as opportunistic pathogens in MSM, this would make it easier to limit testing for these organisms to symptomatic individuals until RCTs show evidence of net-benefit of screening asymptomatic individuals. As noted above, the cessation of screening for these organisms could lead to a large reduction in antimicrobial consumption in PrEP cohorts.
It could be objected that we have created a false dichotomy between biomedical individualist and eco-social frameworks. This is not our intention. An adequate framework for STI epidemiology needs to be explicitly multi-level incorporating relevant insights from submolecular to pathogens, microbiota, individuals, partners, sexual networks and various social, economic and political processes. Due to space constraints, we have not been able to go into any detail pertaining to the various social and environmental systems that play a vital role in configuring sexual behaviour and resultant sexual networks.108,109
Conclusion: Insights from COVID-19 and climate meltdown
There is an increasing recognition that integrative, multi-disciplinary and multi-level ecological thinking is necessary if we are to turn back the tide of widespread environmental destruction, mass extinctions, antimicrobial resistance and the increasing rate at which zoonoses such as SARS-CoV-2 are emerging.110–115 A critical ecological concept here is the importance of considering our individual and combined ecological footprints. 115 Various types of evidence reveal the need to reduce our ecological footprints to below a threshold which allows planetary ecosystems to flourish or at least persist. 112 The determination of this threshold depends on an assessment of what an ecologically sustainable level of consumption is and then dividing this up amongst humans. 112 In a similar vein, we need to reduce our antimicrobial footprints below key AMR inducing thresholds if we wish to avoid AMR taking more lives than cancer in 2050.115–117 This is particularly important in high STI prevalence populations. 23 The evidence reviewed here suggests that an eco-social STI framework provides a more complete account of the risk of AMR emerging and spreading than biomedical individualist frameworks. It also provides a better fit with the other recent findings reviewed above, such as the link between network connectivity and STI prevalence. As such, future research should be directed at evaluating various ways of incorporating eco-social frameworks in STI clinical care and prevention activities.
Footnotes
Authors’ contributions
CK conceptualized the arguments and wrote a first draft. CK was responsible for drawing the graphics. CK, TB and CVD contributed to and approved the final version of the article.
Competing interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.