
Abstract
Background: The prevalence of sexually transmitted infections (STIs) is high in New Caledonia (NC), but there are no data on Mycoplasma genitalium (MG). However, the syndromic treatment of urethritis used in the territory includes a single dose of azithromycin, which could generate resistance in MG.
Methods: We recruited 217 men referred to the Noumea public medical centre (CMP) with signs of urethritis and meeting the inclusion criteria from May 2016 to March 2018. Each was tested for Neisseria gonorrhoeae (NG), Chlamydia trachomatis (CT), Trichomonas vaginalis (TV) and for the first time in NC for MG by polymerase chain reaction (PCR).
Results: The prevalence of MG was 10.1% (22/217). Azithromycin resistance of MG (mutation in the 23S rRNA gene) could only be assessed for 10 of the 22 strains. Only one (1/10; 10%) was resistant. The prevalence of other STIs tested was high, as CT, NG and/or TV were associated in 77.3% (17/22) of MG-positive cases.
Conclusions: Although co-infections further justify syndromic management, the presence of MG in NC urethritis cases could call treatment guidelines into question.
Introduction
New Caledonia (NC) is a French island territory located in the South Pacific Ocean. Its population is approximately 270,000, young (32% are aged < 20 years), and multi-ethnic: 40% are of Melanesian origin; 27% European; 10% Polynesian; and 2.7% Asian. 1 Curable sexually transmitted infections (STIs) are a major public health problem in the South Pacific, particularly in NC. 2 However, there are few recent data on the prevalence of STIs, and none on Mycoplasma genitalium (MG).
Noumea’s South Province Public Medical Center (CMP) is the reference centre for free-of-charge screening and treatment of STI in NC. Based on data from the CMP (CMP’s activity reports, Blanco P., 2018), the prevalence of bacterial STIs is much higher than that in free anonymous STI testing centres in metropolitan France and French overseas departments. 3 Until this study, however, MG testing had never been performed in NC, due to lack of testing capacity. Moreover, syndromic management of STIs (including urethritis) is still widely performed throughout NC. This includes injection of benzathine benzylpenicillin combined with a single-dose oral administration of azithromycin and metronidazole. 4
The primary objective of this study was to estimate the prevalence of MG in men presenting to CMP with clinical urethritis and document the symptoms and patient profiles associated with MG carriage. The secondary objectives were to evaluate the prevalence of other STIs responsible for urethritis and assess the relevance of syndromic management guidelines in view of our results.
Methods
Included patients and samples
From 1 May 2016, to 30 April 2018, all men aged ≥ 18 years with clinical signs of urethritis at the time of referral to the CMP and who provided written informed consent were included. The clinical signs of urethritis were as follows: clear or purulent urethral discharge; urinary burning, pollakiuria, and/or dysuria; and meatus irritation. The exclusion criteria were residence in NC for < 6 months, antibiotic treatment (regardless of the pathology justifying treatment) in the 3 months preceding the consultation, or urination for < 2 h. An anonymous standardised questionnaire was used to collect data: age, type of social security coverage, declared ethnicity, sexual orientation, number of partners in the last 12 months, and history of STI.
Each patient was screened for Chlamydia trachomatis (CT), Neisseria gonorrhoeae (NG), Trichomonas vaginalis (TV), Ureaplasma urealyticum and parvum (U. spp.), and MG. Detections were conducted on first-void urine. Furthermore, serologies for human immunodeficiency virus (HIV), hepatitis B and C (HBV, HCV), and syphilis were performed according to the CMP’s screening protocol.
Laboratory procedures
DNA extraction was performed on easyMAG (Biomerieux®) and amplification (45 cycles) on LightCycler 96 (Roche Diagnostics®) using two commercial kits (Diagenode®, Liege, Belgium) using Taqman probes with fluorescence emission: MG and TV were detected by multiplex polymerase chain reaction (PCR) (S-Dia-MGTV/DDGS-60-L100), and NG and CT by multiplex PCR (Dia-CT/NG-050.Vs1). Ureaplasma spp. were detected by bacterial culture using the commercial kit (Mycofast® RevolutioN (Ref: 00,060 EliTech MICROBIO), which is also used for routine diagnosis at the microbiology laboratory of Institut Pasteur of New Calédonia (IPNC). If MG was present, a consultation was scheduled at 1-month post-treatment to perform a follow-up PCR and assess for possible recontamination. As of February 2017, MG strains could be sent to the National Reference Center for STIs in Bordeaux, for detecting mutations associated with macrolide resistance in the 23S rRNA gene using the ResistancePlus MG assay (SpeeDx, Australia).
Statistical analysis
Data from the questionnaires were entered into EpiData (v3.1, EpiData Association, Odense Denmark) and then imported into the statistical analysis software (Stata 12, Stata Corp. College Station, TX. USA). The association of MG status with categorical variables was analysed using the Fisher’s or Mantel-Haenszel test, and that of continuous variables using the Student’s t-test or Wilcoxon test, depending on the distribution of variables. After dichotomisation, variables whose association with MG-positive or MG-negative status was p < 0.2 were included in a logistic regression model to document their association after adjustment for other variables. Other a priori variables of interest were retained in the model. Statistical analyses were conducted with a significance level set at 0.05.
Ethics
Ethics approval The New Caledonian Advisory Committee on Ethics for Life Sciences and Health approved this study [2016]
Results
Prevalence and risk factors for the presence of MG
Factors associated with the presence of MG.
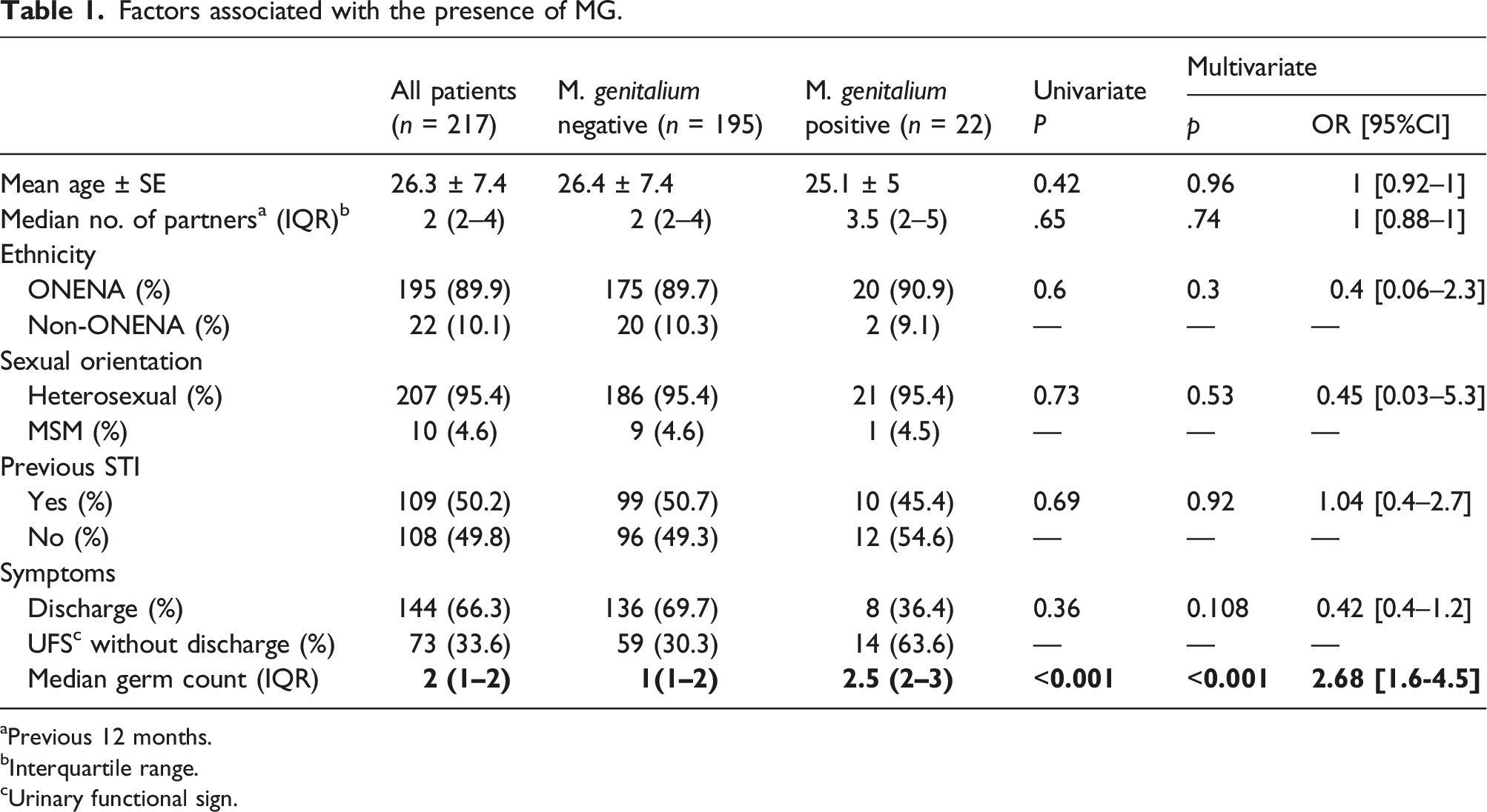
aPrevious 12 months.
bInterquartile range.
cUrinary functional sign.
Prevalence (% and 95% confidence interval) of pathogens and idiopathic urethritis by age.

In multivariate analysis after adjustment, the presence of MG was independently associated with an increase in the number of associated organisms (OR = 2.7; [1.6–4.5], p < .001) (Table 1).
The prevalence of other screened pathogens and idiopathic urethritis were all higher than that of MG (Table 2).
U. spp. titres ≥ 104 colour changing unit/mL on first-void urine without associated CT, NG, TV, or MG accounted for 3.7% of urethritis cases (8/217), but they were found at those titres in association with other pathogens in 30.4% (66/217) of the samples.
monomicrobial and polymicrobial infections with MG.
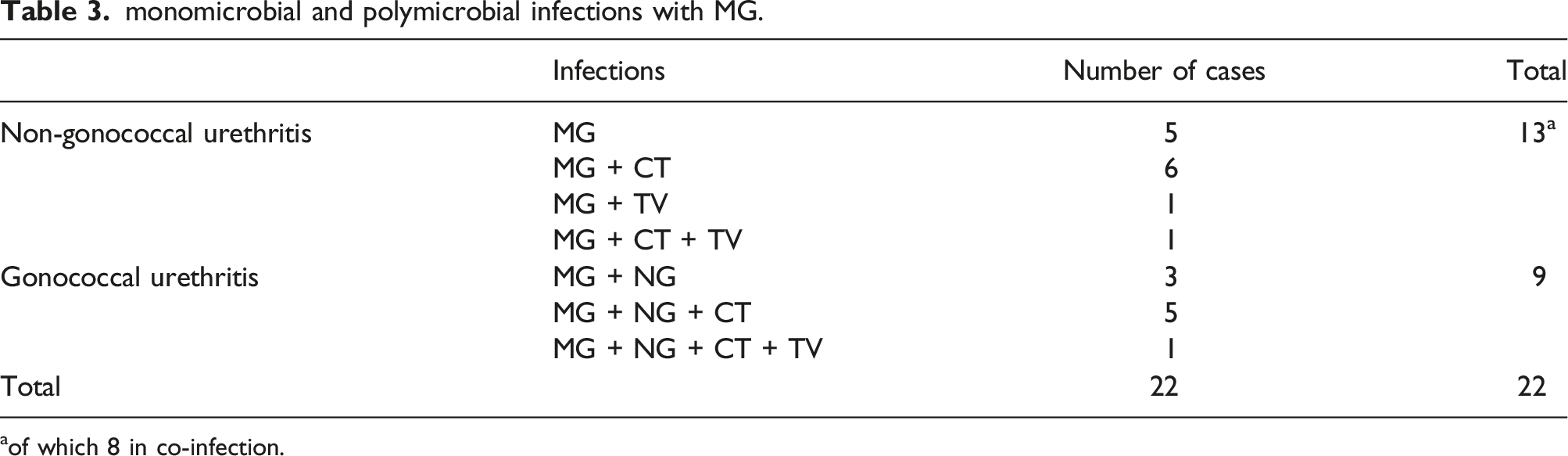
aof which 8 in co-infection.
Factors associated with co-infections.
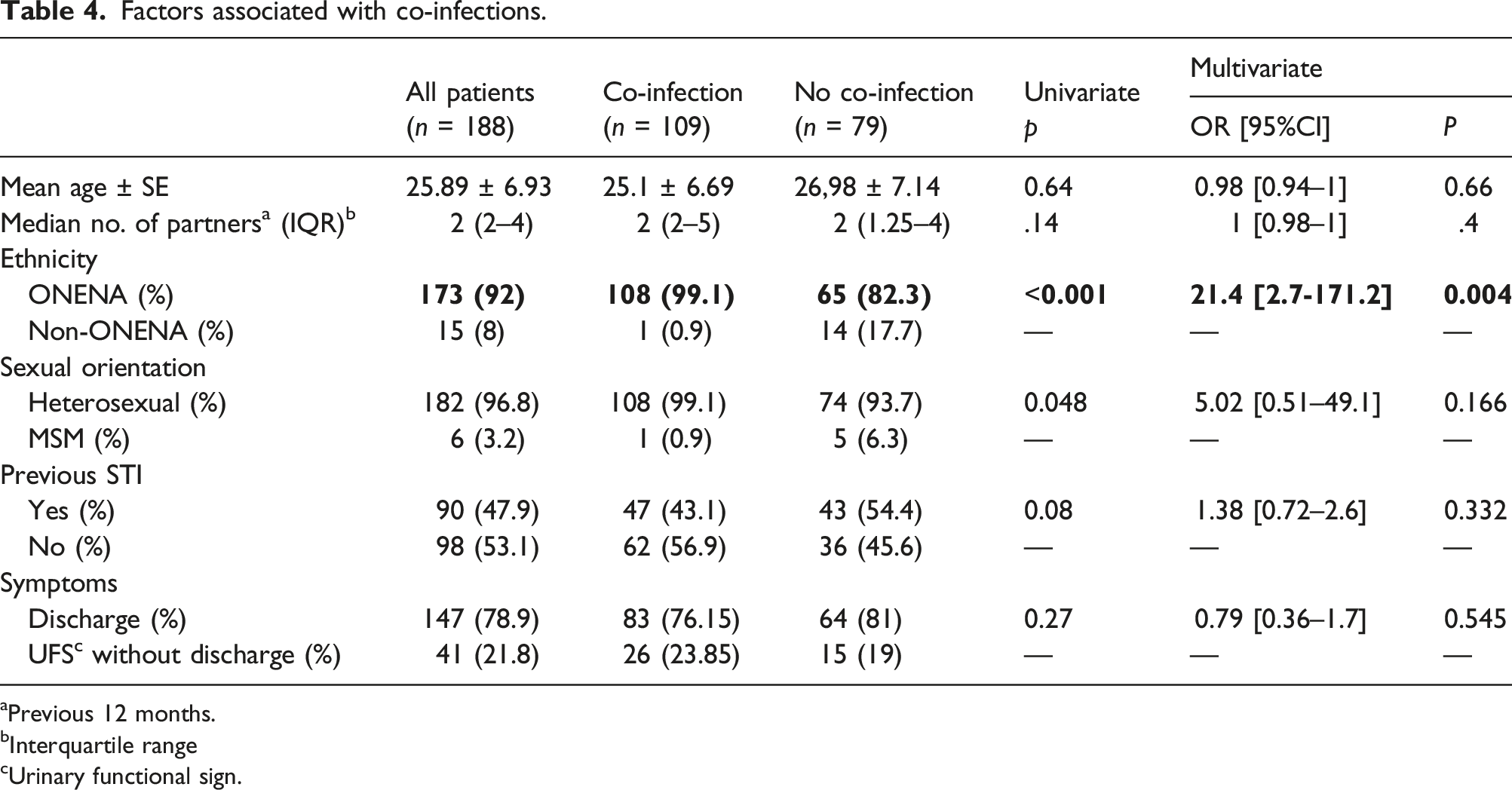
aPrevious 12 months.
bInterquartile range
cUrinary functional sign.
Antibiotic resistance
During the period when the macrolide resistance mutation test was not yet performed, only five of the eight patients with MG who received syndromic management had returned at 1 month. In all five cases, the patients were symptom-free, and MG PCR was negative on the first-void urine.
Of 14 strains subsequently forwarded to the French National STI reference centre for macrolide resistance-associated mutation detection, one strain presented resistance mutation, nine strains did not, and the 23S rRNA of the remaining four strains could not be amplified. In total, nine (90%) of the 10 strains where MG resistance to macrolides could be assessed remained susceptible.
Of 22 patients with MG, only one did not receive syndromic treatment, as he had mild symptoms and was reliable enough to come for these results. He was a carrier of MG and CT and received an adapted treatment at the time of the delivery of the results after 1 week, whereas he had no more symptoms. Of 21 patients who received syndromic management, only one had persistent urethritis at 1 month. In addition to the high risk of recontamination, since his partners had not been treated, he was a carrier of the resistant MG strain, had concurrent TV, and had been previously treated for urethritis.
Discussion
Prevalence and co-infection
The prevalence of MG in our collection of urethritis cases in men was close to that observed in other studies, in both Oceania and other parts of the world.6–10 However, in our patient series, in which most (89.9%) participants were ONENA, the prevalence of MG was relatively low compared to that of NG, CT, and TV (Table 2). The positivity rate for these three pathogens was extremely high in our series, which may explain the frequency of MG co-infections with CT (13/22, 59%) and NG (9/22, 41.0%). As in other Melanesian populations,11–14 this high prevalence of curable STIs suggests the possibility of widespread asymptomatic carriage, which may also explain the low rate of urethritis considered idiopathic in our study.
Mycoplasma genitalium is the second most common cause of non-gonococcal urethritis (NGU) after CT. 15 This was also the case in our study, in which NGU accounted for 48.4% of all cases (105/217). However, the causal role of MG in the symptoms of NGU is tempered by the fact that co-infection with CT and/or TV occurred in 61.5% (8/13) of cases (Table 3)
Risk factors for MG carriage
We did not identify any specific clinical sign of MG urethritis. The lack of a specific clinical sign or risk factor associated with MG has already been highlighted in other studies. 16 Generally, it is the chronic, pauci-symptomatic nature or failure of first-line treatment that remains predictive of MG as a causative agent of urethritis. 17 This seems more difficult to document in our population. The ONENA population does not routinely seek Western medicine if symptoms are mild, as may be the case with urethritis caused by MG alone. 17 We identified only five patients for whom MG alone could be the cause of urethritis symptoms.
Antibiotic resistance
As has already been noted, MG resistance to azithromycin in NC appears to be lower than in metropolitan France. 18 Conversely, some countries in the South Pacific, such as Australia, have some of the highest resistance rates described worldwide. 19
Territory specificity and syndromic treatment
Whether for co-infections and resistance of MG to antibiotics, our data differ from those reported by other studies conducted in the South Pacific.20,21 However, data for Oceania on the prevalence of MG and its resistance often come from countries with higher average incomes, such as Australia and New Zealand, whereas our results seem to be closer to those found among other Melanesian populations. 11 These findings on territorial specificity are consistent with other observations, such as preserved susceptibility of gonococcus to penicillin G in NC. 22 As a result, for example, the NC recommendations do not suggest the same antibiotic treatment for NG if the suspected infection occurred in the territory or outside it. 4 Therefore, Benzathine benzylpenicillin is retained in the syndromic treatment of urethritis to preserve the susceptibility of gonococcus, and it has the advantage of being active if there is associated latent syphilis, as was the case for at least 5.78% (10/173) of our patients with urethritis for whom serology was requested. It should be noted that we also had 7.3% (13/171) of serological markers of probable syphilis. The specificity of these results, essentially due to ONENA individuals, who are in the majority of our sample, could be linked to the fact that there is little sexual exchange with neighbouring countries, because NC, like many other South Pacific territories, is relatively isolated geographically from its neighbours.
Other findings may partly explain the singularity of our observations. With regard to the prevalence of sexually transmitted bacteria, young NC individuals seldom use condoms. 23 Furthermore there is no screening program in NC, and ONENA populations seldom resort to such programs even when these are available. In our centre, which is unique in the territory, ONENA individuals are underrepresented in screening clinics and overrepresented in symptomatic STI clinics compared to their population in the Southern Province in 2014. 1
For many years, public health policies have focused on syndromic management and active screening for STI signs during medical consultations, without offering accessible large-scale screening. Oceanian, non-European, non-Asian ancestry individuals often delay seeking Western medical care. 24 They may also first resort to traditional treatments. As most STIs may spontaneously resolve or have long latency phases, they do not seek curative care but may remain carriers and therefore transmitters.
Complications related to STIs are frequently observed in NC. Gonococcal arthritis and chlamydial reactive arthritis represent 8% of the causes of atraumatic arthritis managed by the emergency department of the Nouméa hospital. 25 Between 2012 and 2017, as many as 43 pregnant women with active syphilis were identified in this same hospital. 26
The less repeated use of macrolide antibiotics in this population may explain the low MG macrolide resistance levels. Furthermore, differences in patient selection among the populations in which they are studied may explain differences in documented resistances levels.
The median age of MG-positive patients in our study was 25 years and only 45.4% reported a history of STI treatment. This does not necessarily correspond to the profile of patients most at risk of developing resistance, as may be the case, for example, of HIV pre-exposure prophylaxis users (PrEPers) who refer to sexual health centres in large European or Australian cities.
Biases and limitations
This is a monocentric study, the results of which cannot be extrapolated to the general population of NC because our recruitment was conducted at a referral centre for STIs, which, as for other provincial medical centres, provides care mainly for disadvantaged populations more often affected by STIs. 3 It has often been noted that the prevalence of STIs is highly heterogeneous, depending on sociodemographic factors. 27 Among the 195 men who were identified as ONENA, 61.6% had either no health insurance or received provincial financial assistance. Finally, the number of strains for which we were able to test for macrolide resistance mutations was low (10/22).
Conclusion
Our study shows that MG is present in 10.1% of urethritis cases in men treated at the Noumea CMP and that, in 77.3% of cases, it is associated with CT, NG, and/or TV. This high rate of co-infection associated with financial or geographical difficulties in accessing laboratory tests is an element in favour of syndromic management of STIs in NC. Moreover, young individuals are often in immediate need of care and do not systematically return for results. However, the presence of MG in urethritis cases in men in NC may now call into question the use of single-dose azithromycin for syndromic management, 28 especially as treatment recommendations may change for CT.29,30
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Institut Pasteur in New Caledonia and Provincial Directorate of Health and Social Affairs.