
Abstract
Background
Care cascades can inform providers about differences in engagement and retention in care between patient populations thereby improving participation by targeting interventions more effectively. The objective of this study was to assess the uptake and retention of participants along the anal cancer screening algorithm within a single HIV clinic.
Methods
Retrospective procedural and demographic data were collected within a Ryan White HIV/AIDS Program clinic from 18 December 2017 to 29 May 2021. A care cascade was constructed among eligible participants who engaged and were retained in the anal cancer screening algorithm. Engagement was defined as having at least one anal Pap smear. Retention was defined as having a follow-up anal Pap smear, and/or high resolution anoscopy, as indicated. Risk ratios (RR) were calculated to reveal factors associated with initiation and retention in screening.
Results
Of 821 eligible participants, 312 (38%) engaged in screening and 205 (66%) were retained in care. Anoreceptive intercourse was positively associated with engagement (RR 2.81, 95% confidence interval [CI] 2.05–3.90, p<0.001), whereas male gender was negatively associated (RR 0.26, 95% CI 0.20–0.33, p<0.001). Abnormal cytology results on Pap smear were associated with retention (RR 1.39, 95% CI 1.03–1.86, p=0.03).
Conclusions
Overall engagement in anal cancer screening is low within our clinic, particularly among men, but retention in the screening program is notably better, especially among those with abnormal cytology. Target populations have been identified to increase awareness, and qualitative studies are underway to understand perceptions and barriers to engagement in anal cancer screening.
Introduction
It is predicted that there will be over 9400 new cases and over 1600 deaths due to anal cancer secondary to Human Papillomavirus (HPV) infection in the United States during 2022. 1 HIV significantly increases the risk of anal squamous cell cancer, likely due to a combination of immunosuppression and increased likelihood of persistent HPV infection. 2 Current practice is to treat anal cancer with chemoradiation and surgery which can lead to significant morbidity; however, pre-cancerous anal lesions can be treated with application of topical medications, hyfrecation, or local excision with intent to avoid progression to anal cancer. 3 Screening can be carried out through anal Pap smear to detect abnormal cytology, high resolution anoscopy (HRA) to visualize lesions, and biopsies to assess for dysplasia/neoplasia. There are currently no national guidelines on anal cancer screening, but the International Anal Neoplasia Society, among other organizations, advocates that screening is important for prevention and improving prognosis of this disease, particularly in people living with HIV (PLWH).4–6
Little is known about the demographic and clinical factors that contribute to disparities in patient engagement and retention in anal cancer screening programs. Care cascade models have been used to compare differences in subpopulations along step wise screening and treatment programs for a variety of disease processes, including HIV.7,8 This method of analysis can be a valuable tool for informing a health system about subpopulations with disparities in initiation and retention in HIV-related care. 9 We aimed to evaluate the uptake within our newly created anal cancer screening program to identify opportunities for programmatic improvement.
Methods
Study design and participants
This was a retrospective study to evaluate engagement and retention along the anal cancer screening care cascade within the Ryan White HIV/AIDS Program (RWHAP) Clinic at the University of Virginia (UVa). Patients were eligible for anal cancer screening via anal Pap smear if they were actively receiving HIV care in our clinic and were ≥30 years of age or experienced any concerning symptom such as anal pain, itching, bleeding or lesions. All eligible patients from 18 Dec 2017 to 29 May 2021 were included in this analysis. This study was reviewed by the Institutional Review Board at UVa and was considered exempt from ethical review and written patient consent given that it relied solely on data that were routinely collected for healthcare purposes, analyzed in retrospect for program evaluation.
Clinical setting
The UVa RWHAP clinic established an anal cancer screening program on 18 December 2017, which was staffed by a nurse (part-time in 2017 and 2018, full-time from January 2019 onward), a board-certified infectious disease physician, a board-certified colorectal surgeon, as well as a nurse practitioner specializing in obstetrics and gynecology who offered anal cancer screening bundled into routine gynecological care.
Given lack of standardized guidelines, our clinic adopted an approach similar to that developed by the New York State Health Department. 4 An annual anal Pap smear was recommended for people ≥30 years old living with HIV and/or experiencing anal pain, itching, bleeding or lesions. Anal Pap smears with normal cytology results were to be followed with a repeat anal Pap annually. If the anal Pap yielded a cytology result of low-grade squamous intra-epithelial lesion (LSIL), HRA was recommended within 6–12 months. HRA was recommended within 3–6 months for atypical squamous cells of unknown significance (ASCUS) and within 3 months for high-grade squamous intraepithelial lesions (HSIL). If the HRA yielded normal biopsy results, appropriate follow-up included a repeat anal Pap within 12 months. If the HRA yielded a biopsy result of anal intraepithelial neoplasia grade 1 (AIN 1), repeat HRA was recommended within 12 months without need for hyfrecation. For AIN 2–3, repeat HRA with hyfrecation was recommended within 6 months. Any biopsies showing invasive anal carcinoma prompted referral to colorectal surgery.
Data collection
Data were collected from the clinic-specific CAREWare database 10 as well as individual chart review via the electronic medical record. In addition to demographic and clinical data, information regarding the use of Ryan White services such as transportation assistance, medical case management (MCM), substance dependence services, mental health services, and clinic attendance for general HIV care were collected, as defined below. Laboratory data included current HIV-1 RNA viral load, nadir CD4+ T-cell count, anal Pap smear cytology results, and anal biopsy pathology results, as well as their respective dates.
Definitions
Individuals were categorized into two groups along the care cascade based on engagement and retention. Individuals were considered engaged in screening if they had received an anal Pap smear through the clinic and were considered retained in screening if they had received any follow-up test to their initial anal Pap smear (either a repeat Pap smear or HRA).
Gender identity was limited to male and female. Patients identifying as transgender were excluded due to small sample size (n=9) and inability to make meaningful statistical conclusions. Race/ethnicity was categorized into non-Hispanic white, non-Hispanic black, Hispanic, and other. Use of transportation assistance resources was a binary variable based on if an individual had received grant-funded transportation assistance related to a clinic appointment during the study period. MCM enrollment was defined by having a telephone encounter or progress note from a MCM team member confirming enrollment during the study period. History of anal receptive sex was defined as having documentation of this form of sexual activity. If there was no documentation of the term “anal receptive sex” or “anal intercourse”, the person was given the designation “Not Documented”. If someone had no clear documentation of anal receptive sex and had a history of anal gonorrhea or chlamydia infection, it was inferred that they had a history of anal receptive intercourse.
Statistical analyses
Descriptive statistics are reported for demographic and clinical factors for the entire cohort, for those who engaged in anal cancer screening services (i.e. only 1 anal Pap), and for those who were retained in care (i.e. at least 1 anal Pap plus follow up). Stepwise care cascades were synthesized using the number of participants in the eligible, engaged, and retained categories and the number of tests in the following levels: anal Pap smear, abnormal cytology result, initial HRA, abnormal biopsy result, and repeat HRA.
Using R version 4.0.2 and RStudio (R Foundation for Statistical Computing), crude risk ratios (cRR) were calculated to estimate the associations of demographic and clinical factors with engagement and retention. Adjusted risk ratios (aRR) were calculated for variables with p-values less than 0.1. Given only one characteristic was significantly associated with retention, a multivariate analysis was not performed and aRRs were not calculated.
A subgroup analysis was performed among those who had an abnormal screening Pap smear who proceeded to have an initial HRA. The average number of days between first abnormal cytology result and HRA was calculated for each cytology result. Results were stratified by gender and compared with a student’s T-test and Mann-Whitney U test for normally and non-normally distributed means, respectively. These were also stratified by year (2018, 2019, 2020) and compared with an ANOVA and Kruskal–Wallis test for normally and non-normally distributed means, respectively. Given that only partial data were available for 2021, this year was excluded from this analysis. Results from December 18–31, 2017 were included in the 2018 data.
Results
There were 821 people eligible for anal cancer screening during our study period. Among them, 509 (62%) had documentation of having been offered a visit for anal cancer screening. Three hundred twelve of those eligible (38%) engaged in anal cancer screening services, of whom 205 (66%) were retained in follow-up services (Figure 1). Cascade of Care. Panel A shows the number of individuals in each step of the care cascade (i.e. eligible, offered screening, engaged, and retained) as defined in the methods. Panel B shows the number of tests that fit each step in the care cascade, specifically from anal Pap smear to repeat HRA.
Distribution of characteristics in each cohort.
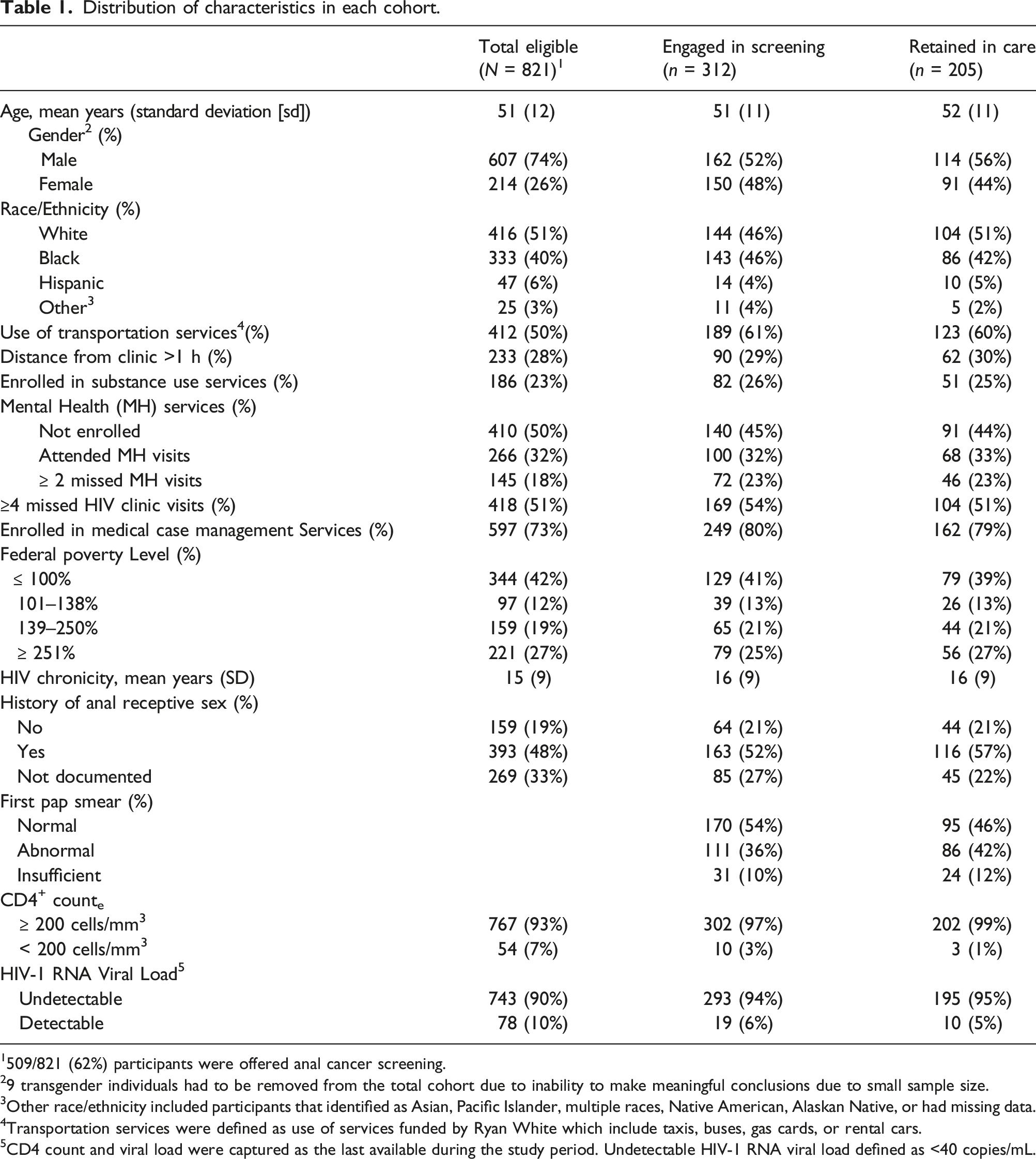
1509/821 (62%) participants were offered anal cancer screening.
29 transgender individuals had to be removed from the total cohort due to inability to make meaningful conclusions due to small sample size.
3Other race/ethnicity included participants that identified as Asian, Pacific Islander, multiple races, Native American, Alaskan Native, or had missing data.
4Transportation services were defined as use of services funded by Ryan White which include taxis, buses, gas cards, or rental cars.
5CD4 count and viral load were captured as the last available during the study period. Undetectable HIV-1 RNA viral load defined as <40 copies/mL.
Crude and adjusted risk ratios (RR), confidence intervals (CI) and p-values estimating the association of characteristics with engagement in screening and retention in care along the care cascade.
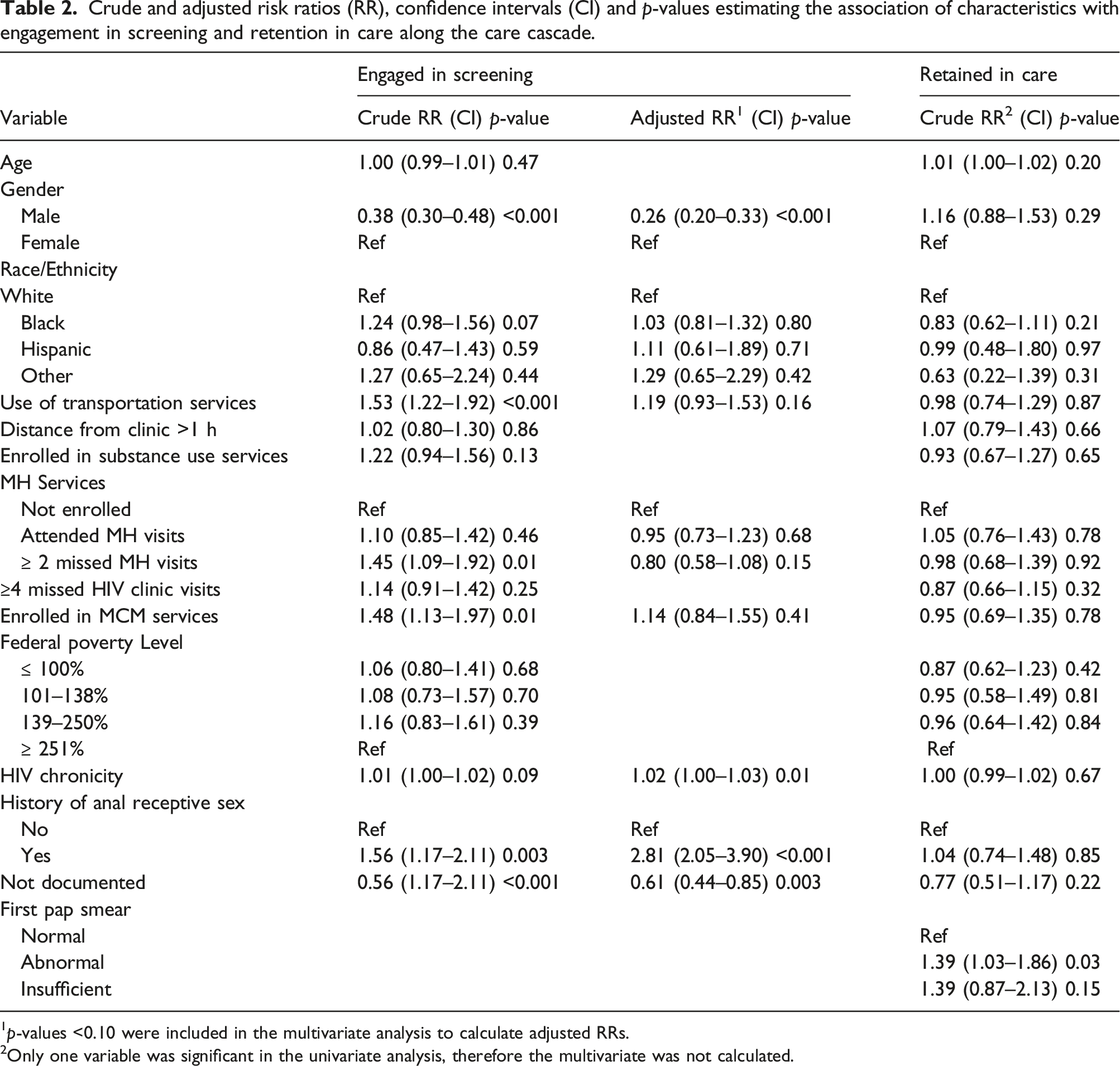
1p-values <0.10 were included in the multivariate analysis to calculate adjusted RRs.
2Only one variable was significant in the univariate analysis, therefore the multivariate was not calculated.
Throughout the study period, 617 separate anal Pap smears were collected. Of these Pap smears, 212 (34%) had abnormal cytology, 331 (54%) had normal cytology, and 74 (12%) had insufficient cells for analysis. Of Pap smears with abnormal cytology results, 172 (81%) were followed up with an HRA, whereas 110 (33%) of Pap smears with normal cytology were followed up with a repeat surveillance Pap smear (Figure 1). A total of three individuals were diagnosed with anal squamous cell carcinoma.
Men and women had no significant difference in mean time to undergoing HRA for those with both LSIL and ASCUS cytology results (83 vs 247 days, p=0.09; 91 vs 124 days, p=0.83). Only men had HSIL results and therefore this stratification could not be compared. When stratified by year, time to HRA decreased significantly in all cytology categories over time (Figure 2). Of note, average time to HRA was within the goal timeframe for our clinic with the exception of HSIL in 2018 (Figure 2). Time to first HRA per year. Time to HRA in days, displayed by year and stratified by anal Pap smear result. Background shading represents the goal timeframe for conducting an HRA based on the specific anal Pap smear result. Anal Pap smears with Low-grade squamous intra-epithelial lesions (LSIL, light blue) were recommended to have HRA performed within 365 days; atypical squamous cells of undetermined significance (ASCUS, gray), within 90-180 days; high-grade squamous intra-epithelial lesions (HSIL, purple), within 90 days.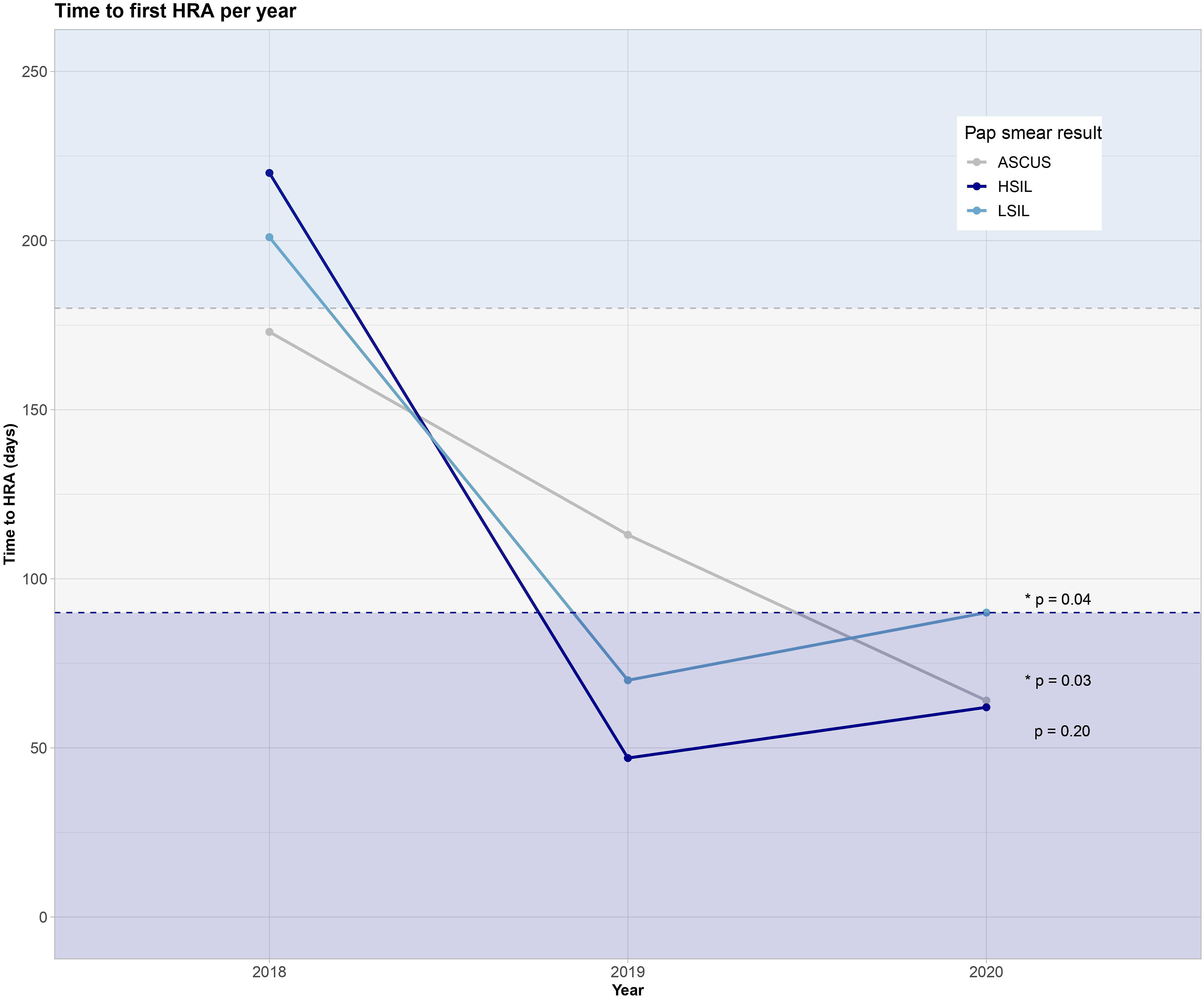
Discussion
In this single-site study, we assessed individual and clinical attributes associated with participation in our clinic’s anal cancer screening program. We found that overall engagement in anal cancer screening services was low, but among those who initiated screening, retention in follow-up screening services was relatively high. There was differential uptake based on gender identity and among people who engage in anal receptive sex and those who do not. HRAs occurred mostly within the goal timeframe, and time from abnormal cytology result to HRA has decreased over the lifetime of the HRA clinic.
Approximately one third (38%) of eligible people in our clinic have engaged in anal cancer screening. This uptake is lower than the 54% observed in a previous, similar single center study. 11 An important factor contributing to this statistic on our study is that only 62% of eligible people have documentation of being offered anal cancer screening services. This deficit may be due to providers’ perceptions of risk for anal cancer varying across patients, or it may have been influenced at the time by a lack of clear evidence-based guidelines for screening. Additionally, this may not represent a lack of offering services, but rather a lack of documentation.
We found that our anal cancer screening program has comparatively low engagement with men and people who do not report anal receptive sex and higher engagement associated with time since HIV diagnosis. Low uptake in heterosexual men may be due to a low perceived risk of anal cancer. Heterosexual men living with HIV have been estimated to have a lower rate of anal cancer than men who have sex with men (MSM) living with HIV, however they are estimated to have a higher rate than female PLWH. 12 Outreach to this subset of our clinic population may be enhanced by raising provider and patient awareness of these risks. We theorize that bundled care explains a higher relative engagement among female participants given that many of them also receive gynecological care, including cervical cancer screening, within our clinic. Lack of documentation of anal receptive sex was associated with decreased engagement likely due to nonresponse bias since screening appointments serve as an additional opportunity to retrieve a detailed sexual history. A positive association between engagement and HIV chronicity is reassuring given that time since HIV diagnosis confers increased risk of cancers, even after receiving anti-retroviral therapy and achieving immune system reconstitution. 13
Retention within anal cancer screening was comparatively better than initial engagement, with 62% continuing to have ongoing assessments. The only significant predictor for retention was having an abnormal cytology result on initial Pap smear. When compared to the proportion of initial HRAs carried out when indicated (81%), the proportion of repeat HRAs when indicated was lower (57%), similar to findings in Lam et al. 14 This finding may be explained by discomfort and inconvenience experienced with a participant’s first HRA, however this warrants further assessment because survey data in the literature shows high acceptability suggesting other factors could be contributing.14,15
The time interval between first abnormal anal Pap smear and HRA decreased over the study period. The stepwise decrease in time for follow-up procedures was seen despite the COVID-19 pandemic beginning in 2020, including temporary clinic closures and provider furloughs. The biggest shift was seen from 2018, the first full year of offering HRA services to patients in our clinic, to 2019 and was likely secondary to increased comfort with the flow of the clinic and the hiring of a full-time nurse for coordinating HRAs in December 2018.
This retrospective analysis has numerous limitations. About one third of participants lacked documentation regarding anal receptive sex practices. This may have altered estimates of risk among those who have had anal receptive sex. While this is known to be a risk factor for HPV exposure, it is increasingly recognized that people without a history of anal receptive sex are still at risk for HPV-associated anal cancers. 12 People who identify as transgender were excluded from data analysis due to small sample size, leading to a lack of information gained about this important subgroup of patients. Additionally, our analysis included the time to diagnostic HRA rather than therapeutic HRA. In our clinic, diagnostic and therapeutic HRAs were more likely to occur simultaneously in 2019 and 2020, with increasing provider proficiency. This may have led to an underestimation of the time to effective treatment during 2018.
Conclusions
This assessment has highlighted several opportunities to extend our programmatic reach. In order to increase engagement in our anal cancer screening program, effort can be focused on raising awareness among all PLWH and particularly heterosexual men living with HIV. We need to better understand patient views on risk factors and provide education to correct misperceptions, especially with informing PLWH of their increased risk regardless of anal receptive sex. A follow-up study is underway to survey individuals seeking care in the RWHAP clinic on their knowledge and perspectives around anal cancer screening. It will also be important to study how forthcoming evidence-based guidelines for anal cancer screening 16 affect engagement and retention in this care cascade in the future.
Footnotes
Acknowledgements
The authors would like to thank the University of Virginia Ryan White HIV/AIDS Program clinic and HRA clinic team as well as the patients we have had the opportunity to work with through the clinic. We would like to thank David Martin, PhD for his contributions to the statistical analysis and the Thomas-Heysell and Dillingham-McManus research groups for providing comments and insight while reviewing the work.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: R.D. reports that she provides consulting services to Warm Health Technologies, Inc. On work unrelated to this manuscript. The authors declare that there are no other conflicts of interest involved in this work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Allergy and Infectious Diseases at the National Institutes of Health (grant number T32 AI007046 to M.G.) and the Health Resources and Services Administration/Virginia Department of Health (RWB611GY21 to R.D. and T.T.).