
Abstract
Background
Non-anemic macrocytosis is frequently observed among HIV-positive persons treated with zidovudine in resource-limited settings. Although zidovudine-associated anemia is well recognized, the probability and predictors of progression from non-anemic macrocytosis to anemia are still unknown.
Methods
A retrospective cohort study was conducted among HIV-positive persons receiving zidovudine-containing antiretroviral therapy (ART) with non-anemic macrocytosis. Kaplan-Meier and Cox regression analyses were used to determine the probability and predictive factors of progression from non-anemic macrocytosis to anemia, respectively.
Results
Of 318 HIV-positive persons, 59.4% were male; mean age was 44.3 years. The median follow-up duration was 5.8 years. The probabilities of progression to anemia at 1, 3 and 4 years were estimated at 9.4, 17.3 and 21.3%, respectively. Almost all anemia was mild asymptomatic. Duration of zidovudine use [hazard ratio (HR) = 1.141; 95% confidence interval (CI),1.036-1.256; p = .007], CD4 count prior to start zidovudine [HR = 0.991; 95%CI,0.982-0.999; p = .038], and hematocrit level at development of macrocytosis [HR = 0.683; 95%CI,0.541-0.861; p = .001] were significant factors to predict progression to anemia.
Conclusion
Non-anemic macrocytosis in HIV-positive persons receiving zidovudine-containing ART can progress to anemia. Longer duration of zidovudine use, lower CD4 cell counts at ART initiation, and lower hematocrit level at development of macrocytosis are predictive factors for progression to anemia.
Introduction
Zidovudine, or azidothymidine (AZT), a thymidine analog in the nucleoside reverse transcriptase inhibitor (NRTI) class, has been used in combination with other antiretroviral agents of antiretroviral therapy (ART). Although AZT is replaced with other newer NRTIs in the current treatment guidelines, it has been widely used for decades in resource-limited settings according to the limited options.1–5 There are still a substantial number of HIV-positive persons that have been taking AZT in developing countries, which has saved their lives for over a decade without clinically significant adverse effects. In addition, AZT is still used as an alternative choice in many developing countries where there are a high number of people living with HIV, and the constrained resources are a limitation.3–5
It has been well established that AZT can cause serious adverse effects including lactic acidosis, lipodystrophy, myopathy and blood disorders, such as severe anemia or neutropenia.6–9 Non-anemic macrocytosis and macrocytic anemia are both commonly observed among HIV-positive persons who receive AZT in both clinical trials and real-life practices.9,10 The pathogenesis of non-anemic macrocytosis and the progression to anemia is due to interrupted DNA synthesis, mitochondrial dysfunction and alteration in the cholesterol and fatty acid composition of the erythrocyte plasma membrane,11–13 which cannot be prevented by vitamin B12 or folic acid supplementation. 14 Estimates of the prevalence of AZT-related anemia range from 5.4% to 16.2% depending on the definition and clinical setting.15–17 Although the severity of anemia is usually asymptomatic, severe life-threatening anemia has been reported. 16 Switching of AZT to other antiretroviral agents is required for some persons who encounter severe anemia. According to previous clinical trials, the hemoglobin level and anemic symptoms were significantly improved after switching AZT to other antiretroviral agents. 18
Nonetheless, most HIV-positive persons who receive AZT-containing regimens and develop macrocytosis have rarely progressed to symptomatic anemia. With the limited options of ART in resource-limited settings, switching stable AZT-containing regimens to other regimens without AZT may be hesitant for both primary care physicians and HIV-positive persons. To date, the information of progression from non-anemic macrocytosis to anemia in HIV-positive persons receiving AZT-containing regimens is still limited. The purpose of this study was to determine the probability, severity and predictive factors of progression to anemia in HIV-positive persons who received AZT-containing regimens and had non-anemic macrocytosis. The findings of this study could be used to guide the management of AZT-related non-anemic macrocytosis among people living with HIV.
Methods
A retrospective cohort study was conducted among HIV-positive persons who received AZT-containing regimens with asymptomatic non-anemic macrocytosis. The information was retrieved from the medical records at an infectious disease clinic of a medical-school hospital. Inclusion criteria were (1) HIV-positive persons aged above 15 years old, (2) had received AZT-containing ART regimen for at least 6 months, and (3) had non-anemic macrocytosis from routine complete blood counts (CBC) at regular visits. Non-anemic macrocytosis was defined as mean corpuscular volume (MCV) above 100 femtolitres (fL) and hemoglobin level above the criteria for anemia. According to the World Health Organization (WHO) criteria, anemia was defined as hemoglobin levels below 12.0 g/dL in women and below 13.0 g/dL in men. 19 Mild anemia was described when hemoglobin was from 11.0 to 11.9 g/dL in women, and from 11.0 to 12.9 g/dL in men. Symptomatic anemia was defined as anemia with symptoms such as tiredness, dizziness, palpitations or chest pain unresponsive to fluid replacement, and the symptoms improved following the transfusion. 19
HIV-positive persons were excluded if they were found to have G6PD deficiency, thalassemia disease or trait, iron deficiency anemia, chronic kidney disease stage 4 (GFR<30 mL/min/1.73 m 2 ), cirrhosis, hypothyroidism, active cancer, pregnancy, gastrointestinal bleeding, abnormal uterine bleeding, menstrual disturbance or active opportunistic infections (OIs) during the study period. The cohort included HIV-positive persons who met the inclusion and exclusion criteria between January 2008 and December 2010, and followed up until the end of study in January 2020. The study was approved by the institutional ethics committee, and informed consents were obtained from all HIV-positive persons in the study.
The following information was retrieved from the medical records age, sex, body weight, risk of HIV acquisition, co-infections of hepatitis B or viruses, history of OIs prior to ART initiation, medications for OI prophylaxis such as co-trimoxazole or dapsone, types of antiretroviral regimens, CD4 counts and HIV viral load at the initiation of ART. Hemoglobin level, hematocrit level, and mean corpuscular volume (MCV) recorded at the timing of ART initiation and every 3-month routine clinic visit were also retrospectively retrived from the medical records. HIV-positive persons were followed up until they developed anemia, being censored due to loss to follow-up or being transferred to other care, or death.
Discontinued treatment was a term used to describe the HIV-positive persons who could not continue AZT in the ART regimen with any reasons such as severe adverse events or suboptimal virological response, or death. Transfusion requirement was indicated when hemoglobin level was below 8 g/dL or having symptomatic anemia.
Data analysis was performed using SPSS version 16. The descriptive data was presented in simple tables of percentages for categorical variables and mean ± standard deviation (SD) for continuous variables with normal distribution. Median and interquartile range (IQR) were used instead for continuous variables without normal distribution. Kaplan-Meier method was used as survival analysis to determine the probability of progression to anemia. Cox proportional hazard model was used to determine predictive factors of progression to anemia. All tests of significance were two sided, and a p-value less than .05 was considered significant.
Results
Baseline characteristics of HIV-positive persons with non-anemic macrocytosis.
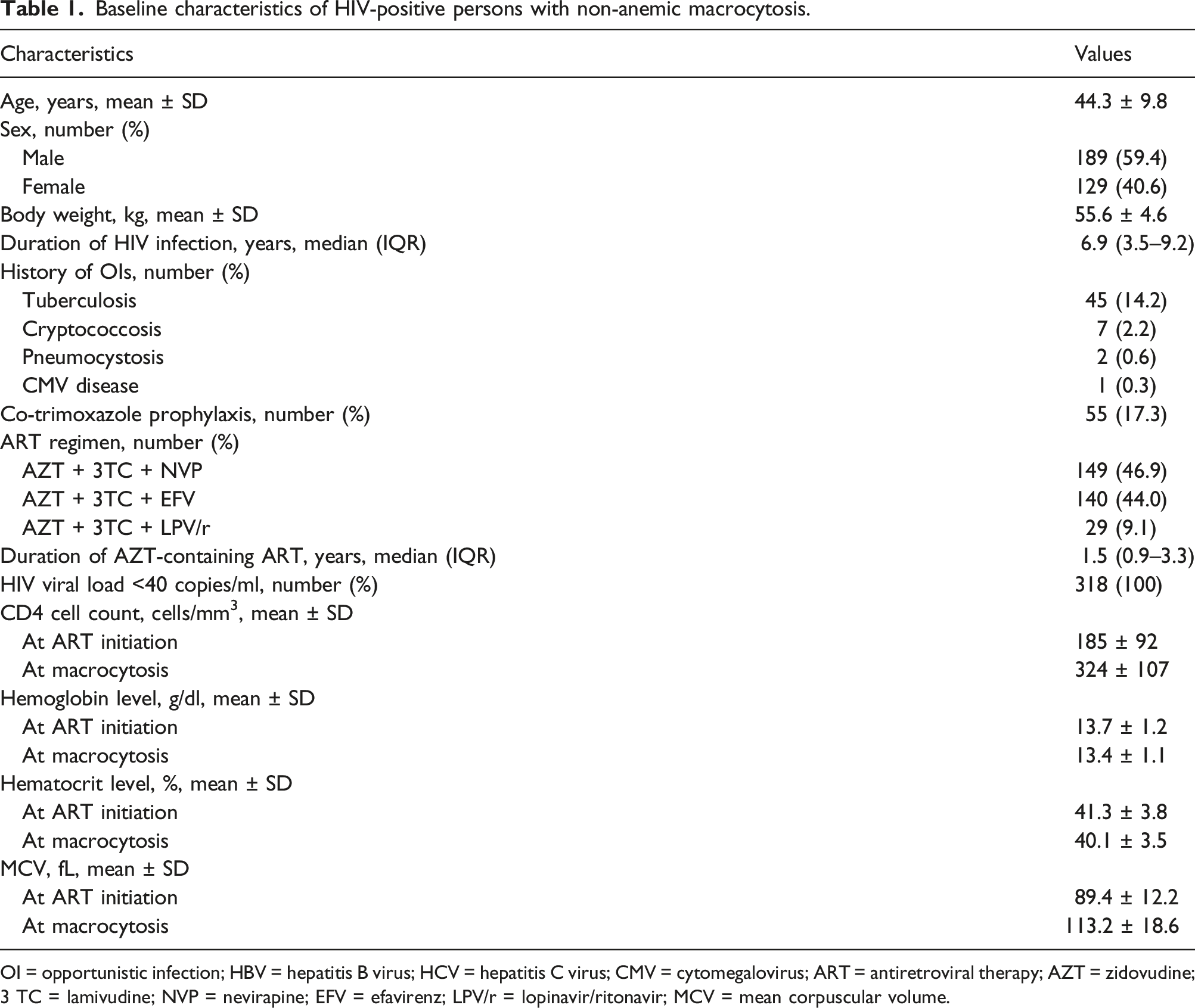
OI = opportunistic infection; HBV = hepatitis B virus; HCV = hepatitis C virus; CMV = cytomegalovirus; ART = antiretroviral therapy; AZT = zidovudine; 3 TC = lamivudine; NVP = nevirapine; EFV = efavirenz; LPV/r = lopinavir/ritonavir; MCV = mean corpuscular volume.
Predictive factors of progression to anemia in HIV-positive persons with non-anemic macrocytosis (Cox regression).
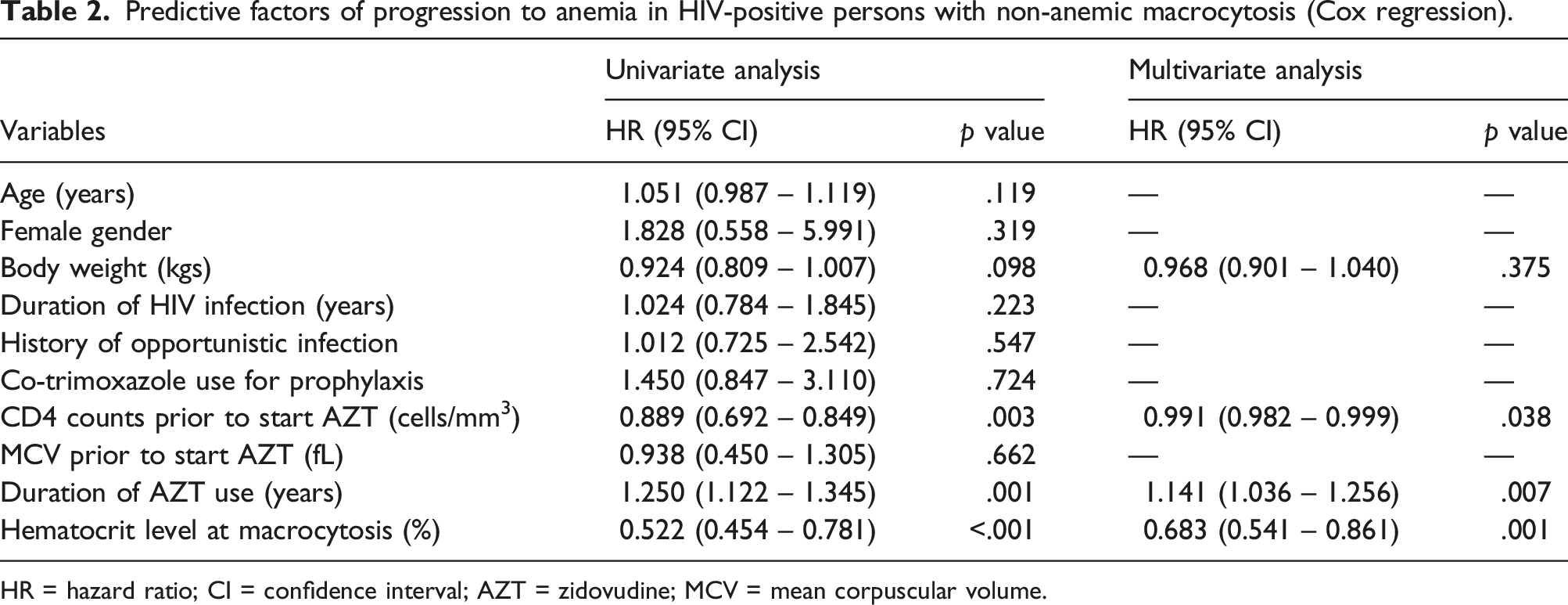
HR = hazard ratio; CI = confidence interval; AZT = zidovudine; MCV = mean corpuscular volume.
The median (IQR) follow-up duration after the development of macrocytosis was 5.8 (3.1–8.8) years in this study. Sixty-six persons (20.8%) had progressed to anemia; 61 (19.2%) with mild asymptomatic anemia, and 5 (1.6%) with moderate symptomatic anemia which needed switching of AZT to other antiretroviral agents. Anemia secondary to other causes had been investigated in persons who progressed to anemia, according to the decision of primary physician. Five persons with moderate symptomatic anemia had complete recovery of clinical symptoms and hemoglobin levels within 6 months after switching AZT to other antiretroviral agents. None required blood transfusion. Of 61 persons with mild asymptomatic anemia, 58 (95.1%) still had the same range of anemia until the end of study; the rest had hemoglobin level within the normal range. From Kaplan-Meier analysis, the probabilities to develop anemia at 1, 3 and 4 years were estimated at 9.4, 17.3 and 21.3%, respectively (Figure 1). Kaplan-Meier analysis of progression to anemia in HIV-positive persons with non-anemic macrocytosis.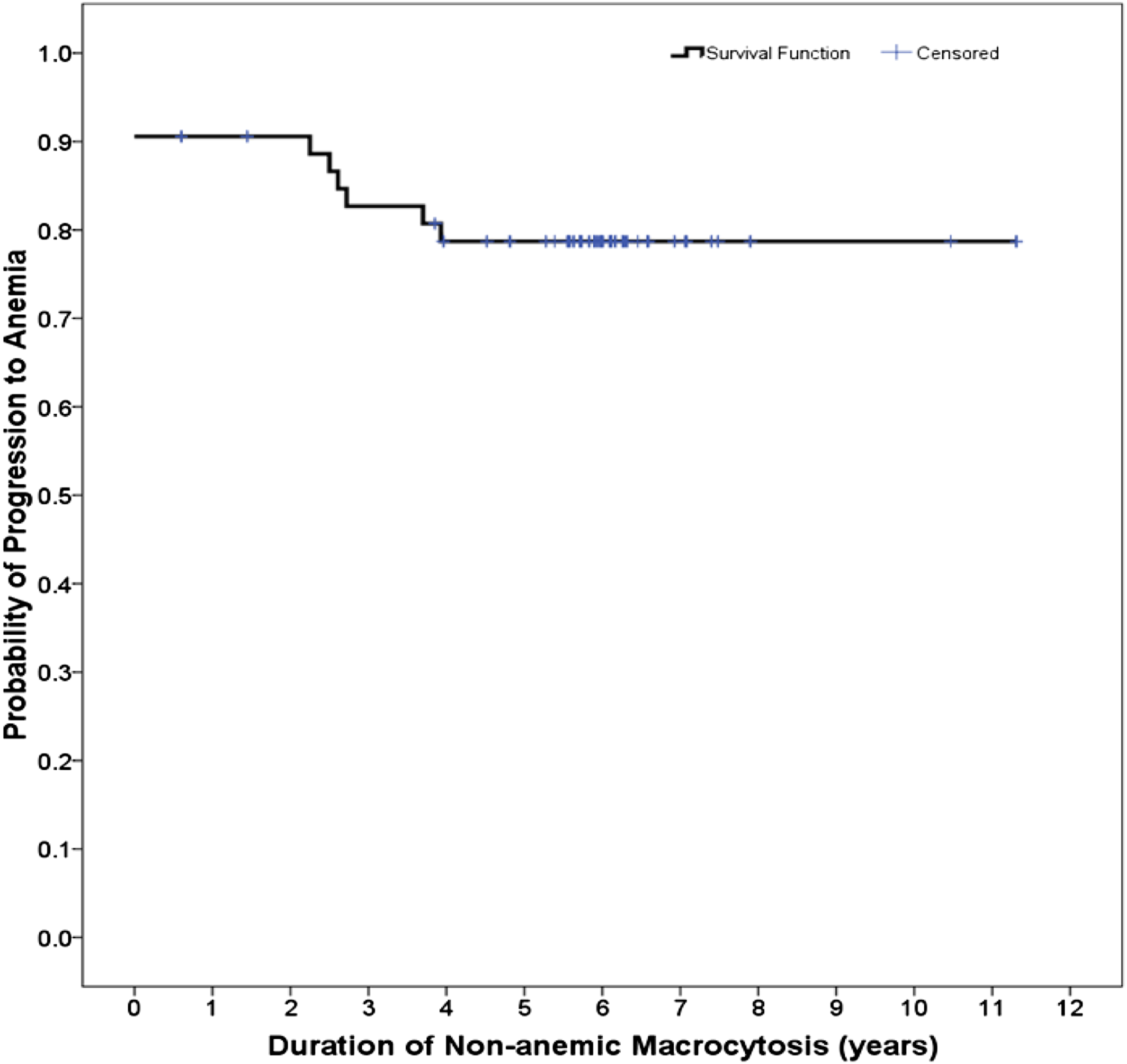
From Cox regression analysis, duration of AZT use [hazard ratio (HR) 1.141; 95% confidence interval (CI) 1.036–1.256; p = 0.007], CD4 count prior to start AZT [HR 0.991; 95% CI 0.982–0.999; p = 0.038], and hematocrit level while developing macrocytosis [HR 0.683; 95% CI 0.541–0.861; p = 0.001] were significant factors to predict progression to anemia (Table 2). Other factors including age, sex, body weight, duration of HIV infection, history of OIs, co-trimoxazole prophylaxis, compositions of other antiretroviral drugs, and MCV prior to starting AZT were not associated with progression from non-anemic macrocytosis to anemia.
Discussion
The results of the present study showed that the characteristics of HIV-positive persons were typical for people living with HIV in the resource-limited settings, i.e. median CD4 cell count at ART initiation was lower than 200 cells/mm3 and a substantial proportion had history of OIs. 20 However, all HIV-positive persons who received AZT-containing ART had achieved complete viral suppression and recovery of CD4 cell counts. Macrocytosis was observed at a median of 1.5 years after receiving AZT-containing regimens which is similar to the results of previous reports.15,21
Approximately one-fifth of HIV-positive persons with non-anemic macrocytosis in this study had progressed to AZT-related anemia, within a median follow-up duration of 6 years. However, most persons progressed to mild asymptomatic anemia and did not require switching of AZT to other NRTIs. Of note, only 1.6% of HIV-positive persons with non-anemic macrocytosis progressed to symptomatic moderate anemia and required AZT discontinuation. No persons had severe anemia or required blood transfusion. This suggests that AZT-related non-anemic macrocytosis is relatively safe and is not a critical reason to discontinue AZT in persons on stable AZT-containing regimens.
From Kaplan-Meier analysis, the probabilities of progression to anemia at 1, 2, 3 and 4 years were estimated at 9.4, 9.4, 17.3 and 21.3%, respectively. Cox regression analysis revealed that duration of AZT use was a significant factor in predicting progression to anemia. Interestingly, no persons developed anemia after 4 years of non-anemic macrocytosis and the longest follow-up duration of macrocytosis in this study was 12 years.
In addition, Cox regression analysis also showed that CD4 cell counts prior to start AZT-containing ART and hematocrit level at development of macrocytosis were the other two significant factors in predicting progression to anemia. Previously, several literature have demonstrated the association of CD4 cell counts and anemia.,22–24 i.e. HIV-positive persons with CD4 cell counts less than 200 cells/mm3 were 3 times higher risk than those with CD4 cell counts above 200 cells/mm3 to have anemia. However, these previous studies included a substantial proportion of persons with anemia prior to ART initiation. Our study has demonstrated the progression from non-anemic macrocytosis to anemia.
Although some studies identified that the baseline hemoglobin at ART initiation was a predictive factor of AZT-related anemia,25,26 our study could not find this association. This could be explained by the fact that our cohort enrolled persons with non-anemic macrocytosis at the beginning. Therefore, we did not include persons with this risk. However, our study was able to show the significance of hematocrit in the development of macrocytosis as another predictor of progression to anemia, i.e. persons with higher hematocrit when we found non-anemic macrocytosis had a lower risk of progression to anemia.
The limitation of this study is the nature of retrospective cohort and had some missing data in some variables. However, the strength of long-term follow-up duration allows us to demonstrate the probability of progression from nonanemic macrocytosis to anemia, as well as the severity of anemia in this cohort.
In conclusion, HIV-positive persons receiving AZT-containing ART with non-anemic macrocytosis can progress to anemia, and most are mild asymptomatic anemia without life-threatening condition. Longer duration of AZT use, low CD4 cell counts at ART initiation, and lower hematocrit level at development of macrocytosis are predictive factors for progression to anemia.
Footnotes
Acknowledgements
The authors are grateful to our participants in this study for their great cooperation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the Thailand Research Fund (grant number RTA6080009).