
Abstract
Background
Our study aimed to measure HIV prevalence and associated risk factors among men who have sex with men (MSM) in three regions of Paraguay in 2020.
Methods
MSM were recruited for cross-sectional surveys in three regions of Paraguay using respondent-driven sampling. Interview were conducted face-to-face to collect demographic characteristics and risk and preventive behaviors. The analysis assessed HIV prevalence and associated risk factors in the three samples of MSM within each region.
Results
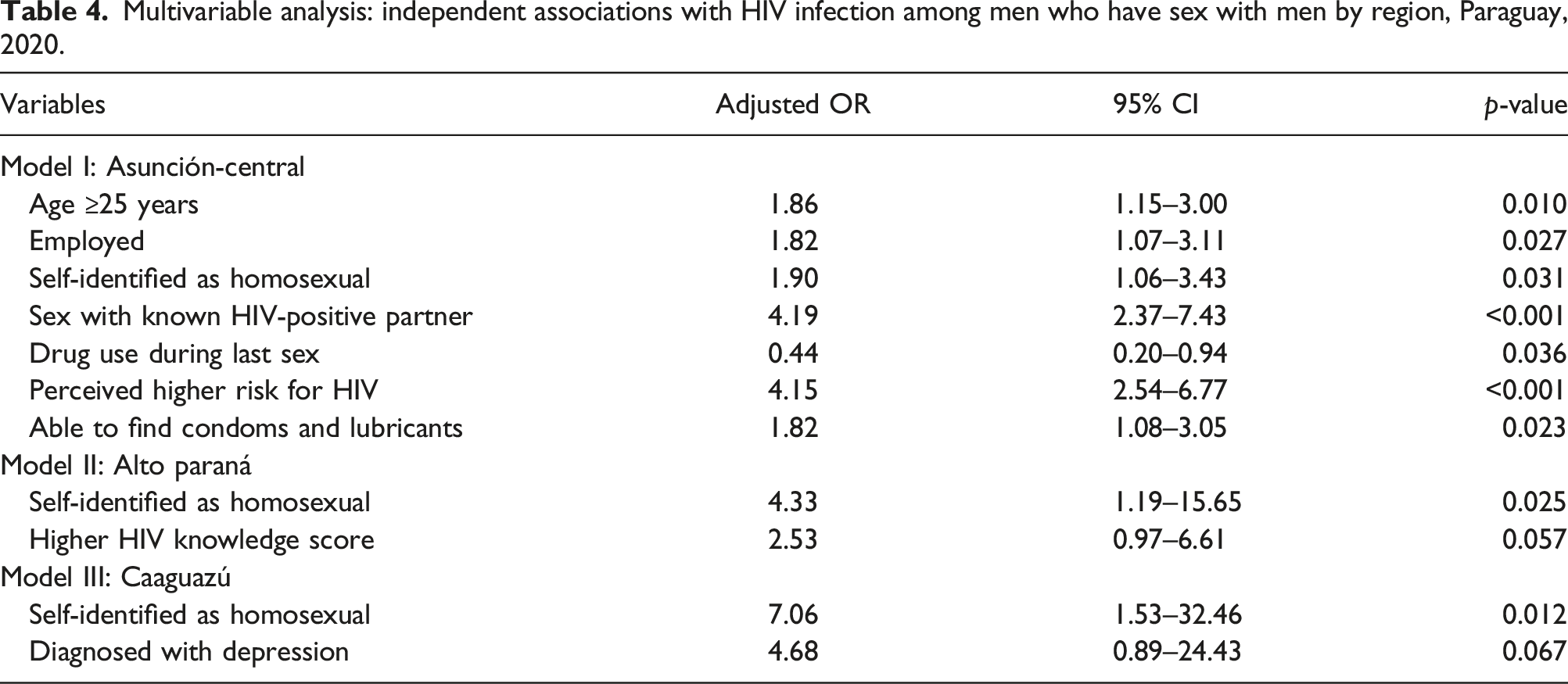
A total of 1,207 MSM were recruited, including 559 in Asunción-Central, 245 in Alto Paraná, and 403 in Caaguazú. HIV prevalence was 24.2% (95% CI 20.6–27.9) in Asunción-Central, 10.2% (95% CI 6.7–14.6) in Alto Paraná, and 3.2% (95% CI 1.7–5.4) in Caaguazú. In Asunción-Central, associations with HIV were age ≥25 years (1.86, 95% CI 1.15–3.00), being employed (1.82, 95% CI 1.07–3.11), self-reporting as homosexual (1.90, 95% CI 1.06–3.43), having sex with a known HIV-positive partner acquisition (4.19, 95% CI 2.37–7.43), self-perceived as being at higher risk for HIV acquisition (4.15, 95% CI 2.54–6.77), and able to access condoms and lubricants (1.82, 95% CI 1.08–3.05). In Alto Paraná, associations with HIV were self-reporting as homosexual (4.33, 95% CI 1.19–15.65) and having higher HIV knowledge (2.53, 95% CI 0.97–6.61). In Caaguazú, associations with HIV were self-reporting as homosexual (7.06, 95% CI 1.53–32.46) and being diagnosed with depression (4.68, 95% CI 0.89–24.43).
Conclusions
HIV prevalence among MSM in Paraguay varied by region, being highest in the capital and major metropolitan area of Asunción-Central, followed by the border area of Alto Paraná. While being self-identified as homosexual was associated with HIV in all three regions, other associations differed, indicating prevention programs need to be tailored to the locale.
Introduction
Throughout the world, HIV has disproportionately affected key populations that experience high levels of stigmatization and marginalization, particularly men who have sex with men (MSM), transgender women, and female sex workers.1–3 MSM may make an under-appreciated contribution to the overall burden of HIV in low- and middle-income countries, particularly in Latin America, but even in sub-Saharan Africa where the epidemic has largely affected the general population.4–6 It is hypothesized that MSM are disproportionately affected by HIV due to a combination of structural, biological, social, and behavioral factors that increase their vulnerability. 6 Indeed, MSM worldwide are estimated to be 19 times more likely to be living with HIV than adult men overall. 7
The HIV epidemic in Paraguay may be increasingly concentrated among MSM. 8 The prevalence of HIV in the MSM population appears to have increased from 13 to 20.7% in Asunción-Central and 1.64%–2.68% in Caaguazú from 2014 to 2017. 8 In Alto Paraná, a region on the Brazilian border, the prevalence of HIV in MSM was measured at 12.4% in 2017. 8 Periodic surveys of MSM in multiple regions are needed to track where the epidemic is rising fastest, characterize local drivers of transmission, prevent the further spread of infection, and identify local priorities for prevention and treatment programs for MSM.
Our study aimed to assess the prevalence of HIV and associated factors among MSM in three distinct geographic zones of Paraguay in 2020. Asunción, the capital district, and surrounding Central department (hereafter referred to as the Asunción-Central region) is the country’s most populous region and contains the most urban metropolitan area. Alto Paraná (hereafter referred to as region) is Paraguay’s second most populous department, located on the border with Brazil, and a major commercial point of entry for goods. Caaguazú (hereafter referred to as region) is a large department located on the major transportation corridor between Asunción-Central and Alto Paraná. Current information about HIV infection and risk behaviors in different locations are essential for guiding prevention and care programs for HIV for MSM in these diverse regions of Paraguay.9,10
Methods
Overall study design
This study is a cross-sectional survey conducted from July to December 2020 measuring HIV prevalence and risk and preventive behaviors among MSM in three regions of Paraguay (Asunción-Central, Alto Paraná, and Caaguazú).
Study population
MSM were defined as men who reported having had oral, genital, or anal intercourse (insertive or receptive) with a man or with a transgender person during the 12 months prior to the study. To be eligible, they had to be 15 years of age or older and living or working in their respective study area (i.e. Asunción-Central, Alto Paraná, or Caaguazú). Participants had to provide verbal informed consent if age 18 years and older, and verbal consent and assent if age 15–17 years. In addition, the participant had to be referred to the study by another eligible participant. Persons under the influence of psychoactive drugs were not enrolled. The study targeted 300 to 400 participants for each of the three study sites calculated to obtain a precision of +/− 5% or less over a range of estimated point estimates for HIV prevalence and risk-related behaviors.
Formative research and study preparation
In the month prior to recruitment and data collection, a formative assessment was carried out to guide the conduct of the research. In-depth interviews were conducted with key informants from the MSM populations of the three regions. Key informants were asked about their preferences on study site locations, best days and hours of operations, appropriate incentive amounts, and the different social networks that MSM belonged to. Following key informant advice, five sites were chosen to conduct the study (two in Asunción and one each in Central, Alto Paraná, and Caaguazú). The study sites were located in private offices (i.e. not governmental health clinics or MSM-focussed NGOs) chosen to provide sufficient space for a reception area and private interview rooms. The formative phase identified study staff to conduct the interviews and counseling. Study staff were MSM or persons with experience in providing HIV prevention services to MSM, including personnel of the partnering NGOs and MSM referred by key informants. Staff were trained on the procedures of the study and certified in HIV counseling by the investigators. Key informants also pilot tested the data collection instrument to identify elements that were missing and improve clarity and comprehension. The key informants were recruited thorough local non-governmental organizations (NGOs) that work with MSM and by referrals from other key informants to include MSM who did not access services with the NGOs. Members of these NGOs also participated in planning of the study, development of the questionnaire, pilot testing, data collection, and validation of the final results and interpretations.
Sampling and recruitment
Respondent-driven sampling (RDS) was used to obtain a diverse recruitment of the MSM populations in each region. RDS begins with the selection of “seeds”, that is persons who are purposefully recruited to be eligible members of the study population, well-networked with other MSM, and willing to recruit from their social networks. Initially, three seeds were selected in each region (9 total). Seven seeds were later added to replace seeds that did not produce recruitment chains within the first several weeks. Seeds were diverse with respect to belonging to or not belonging to the collaborating NGOs, socioeconomic and education levels, areas of residence, and age. Seeds underwent all steps of study participation, including consent, interview, and HIV testing. Upon completion, seeds were instructed in how to recruit other eligible MSM from their social networks. Three coupons with codes to link recruiter to recruits were given for the purpose of referring their acquaintances to the study. Recruits in turn were instructed to recruit three more eligible participants. This process continued with each wave of recruits until the sample sizes were met or the study period ended.
Persons presenting with a coupon to the study site were first screened for eligibility. To be eligible, the person had to meet the above eligibility criteria and have a valid coupon that they received from someone they personally knew who participated in the study. If eligible and interested, verbal informed consent was obtained. Participant data were entered into software to track recruiter-recruit connections, identify potential duplicate participants, and monitor recruitment progress with respect to key demographic and risk indicators. Each person, including seeds, received a $4.40 incentive for their completion of the study and $2.20 for each referral of an eligible participant to the study. In this manner, long chains of peer referrals diversified and established the enrollment.
Survey instrument
A face-to-face, structured questionnaire collected sociodemographic characteristics, sexual behaviors with men and women, serostatus of partners, commercial sex work, self-reported sexual identity and orientation, knowledge about HIV transmission, perception of their risk for HIV, access to HIV testing, able to access condoms and lubricants, and history ever being diagnosed with a mental health disorder. The assessment of level of HIV knowledge comprised five questions on transmission and prevention and was analyzed as having all correct answers (high knowledge) or not. For the screening of common mental disorders and psychological distress, we used the SRQ-20 questionnaire designed by the WHO for the detection of common mental disorders and psychological distress in vulnerable populations and in developing countries. 11 The questionnaire was administered on paper by the trained research staff in Spanish or Guarani according to the participant’s preference. The time required for completion was 30–60 min.
Laboratory methods
Once the survey was concluded, serological specimens were collected for HIV testing. HIV testing followed a standard algorithm of rapid sequential tests using kits approved by the National HIV Program of the Ministry of Health of Paraguay, namely HIV-1/2 STAT Pak Assay (Chembio Diagnostic Systems, NY, USA) and SD. BIOLINE HIV-1/2 3.0 (Standard Diagnostics, Inc, Korea). For diagnosis, the national reference laboratory performed ELISA tests on all samples with that were positive or discordant on the two sequential rapid test results. For any specimen reactive on ELISA, a plasma HIV-1 viral load was measured. For quality control, ELISA was also performed on a 20% systematic sample of specimens with a non-reactive results on the rapid tests.
Statistical methods
Data are presented as unweighted sample means. The distribution of sociodemographic characteristics, risk and preventive behaviors, and psychosocial measures are tabulated for the entire sample, for each region, and by HIV status and compared between regions using the chi-square test. Due to wide heterogeneity in HIV prevalence and key indicator variables, bivariate comparisons of HIV prevalence were made within each region using the chi-square test and logistic regression analysis. Variables associated with HIV at p < 0.05 in bivariable logistic regression analyses were entered into a multivariable logistic regression model. Variables with p < 0.10 were retained in the final model. Analyses were done using Stata SE 16.0.
Ethical considerations
To preserve confidentiality of the participants, informed consent was verbal and no names or other identifying information were collected. Results of the HIV tests were linked to survey responses through the use of a non-identifying code that can be consistently created by the participant (e.g. comprising partial date of birth, initials, and other items known to the participant but not the survey team). Final results of laboratory tests were delivered to study site also using the unique code. Participants received post-test counseling, linkage to HIV care if positive, and referrals for other health and social services. The protocol review and approved by the Ethics Committee of the Central Laboratory of Public Health in Paraguay.
Results
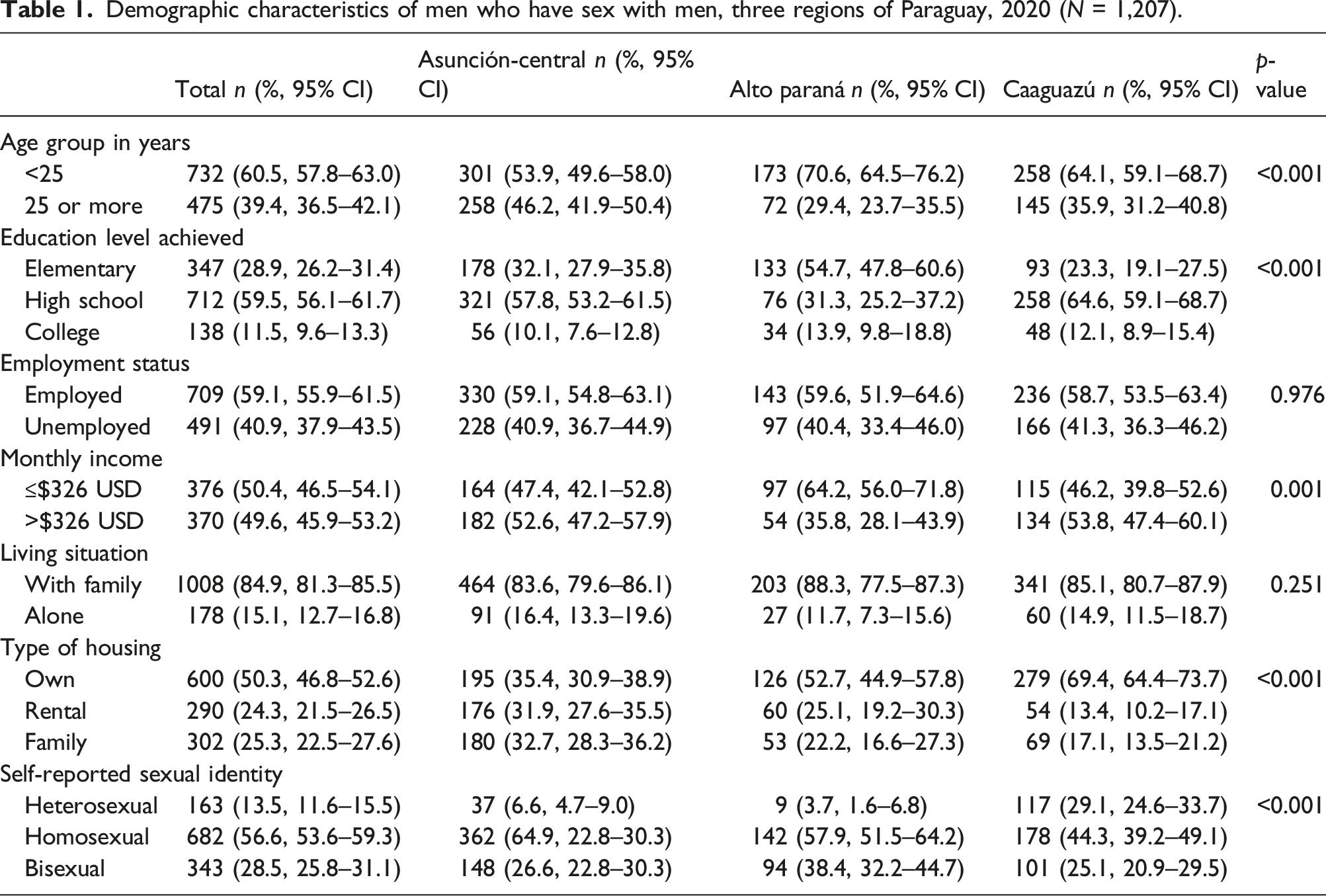
Demographic characteristics of men who have sex with men, three regions of Paraguay, 2020 (N = 1,207).
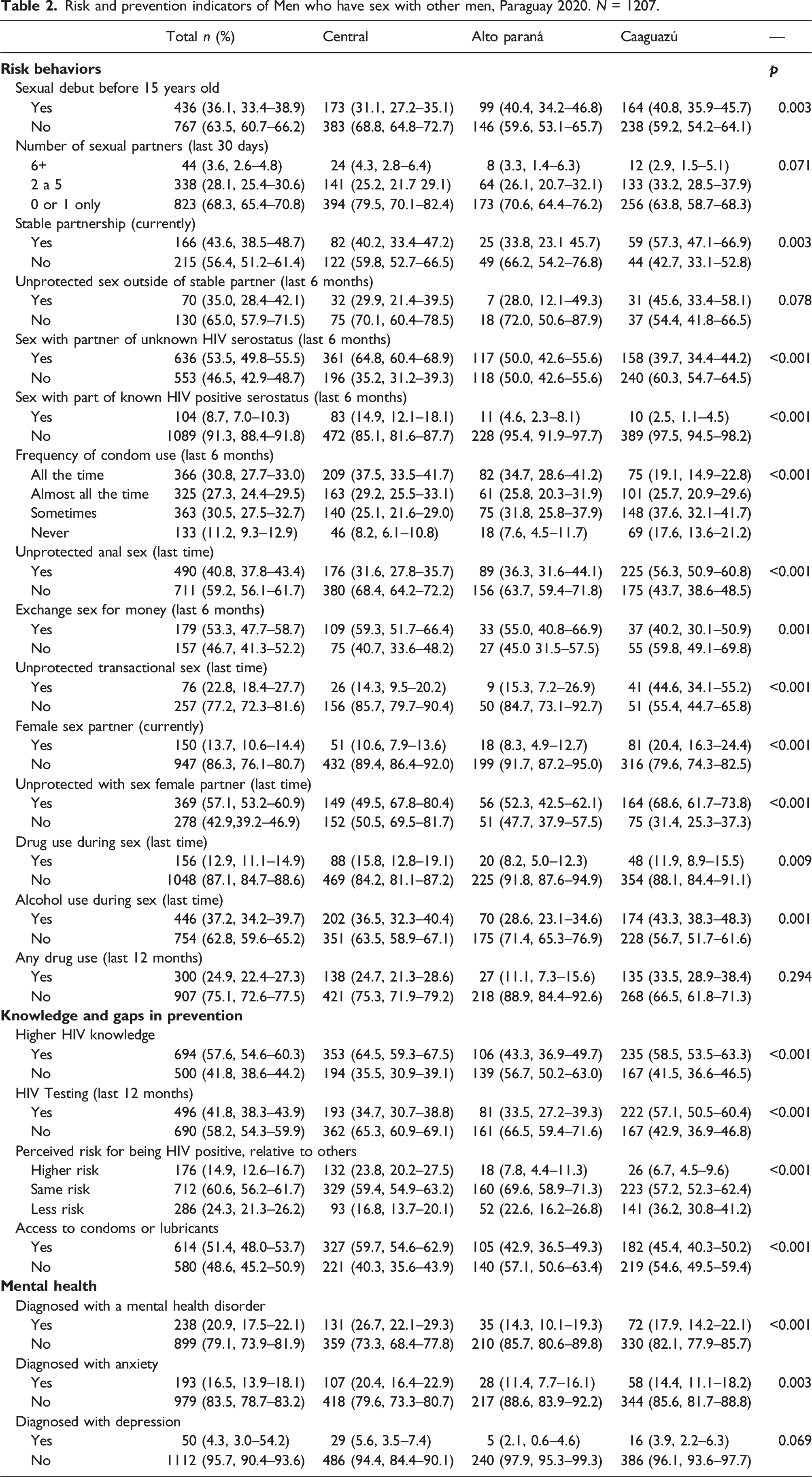
Risk and prevention indicators of Men who have sex with other men, Paraguay 2020. N = 1207.
Prevalence of HIV by demographic characteristics, sexual orientation, and risk behaviors among men who have sex with men, Paraguay, 2020 (N = 1,207).
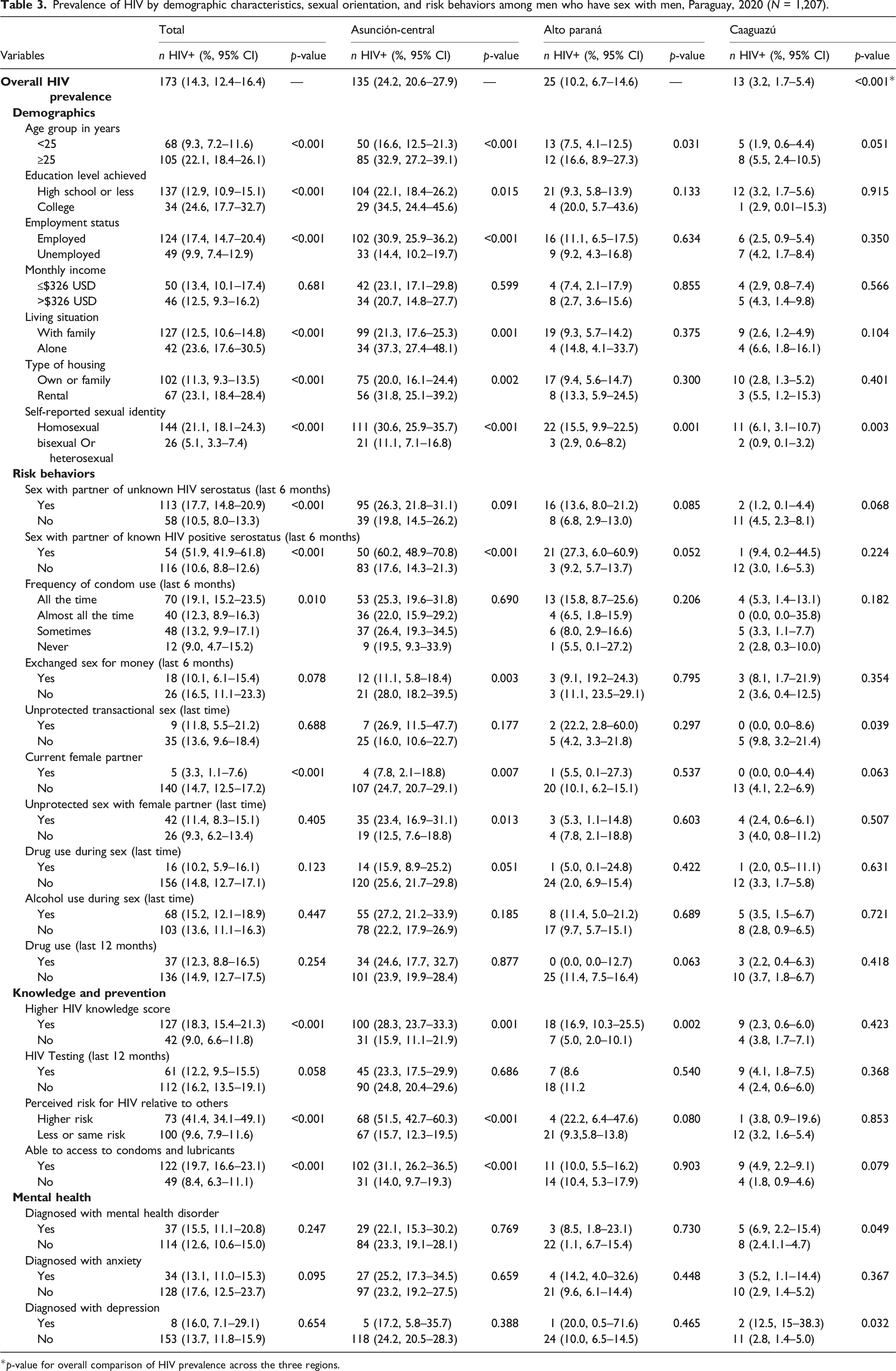
*p-value for overall comparison of HIV prevalence across the three regions.
Multivariable analysis: independent associations with HIV infection among men who have sex with men by region, Paraguay, 2020.
Discussion
Our study documented wide variation in HIV prevalence and related risk factors among MSM across three regions of Paraguay. A striking one in four MSM were living with HIV in Asunción-Central. Among MSM in Alto Paraná, one in 10 were HIV positive. While in Caaguazú, HIV prevalence was under 5%. This pattern of the HIV epidemic among MSM prevails across many areas of Latin America. 12 In a recent review of HIV seroprevalence surveys of young MSM in 47 studies in 17 countries, HIV prevalence ranged from 1.2 to 32.6%. 12 Our finding of high HIV prevalence among MSM in some areas of the country is supported by a recent model estimating that three-fourths of new HIV infections are among MSM, and MSM have the highest incidence of new infections of any population in Paraguay. 13 The prevalence of HIV and attributable proportion of new infections in Paraguay are close to that of Australia, New Zealand, and western European countries where MSM have accounted for as much as 70% of HIV infections since the beginning of their epidemics.1,7,9
We also found variation in the potential drivers of HIV among MSM by region. In Asunción-Central, which contains the capital and major metropolitan area, correlates of HIV infection may be related to larger social networks and therefore increased sexual connections to other MSM, increased risk-related behaviors, and increased access to MSM-focused prevention programs. These increased connections may be reflected in factors such as having partners known to be HIV positive, perceived higher risk for HIV, and access to condoms and lubricants. Alto Paraná is less urban than Asunción but includes border areas, transportation corridors, and hotspots where MSM congregate. Here, risk factors for HIV infection also included indicators of social and sexual networks that include other MSM. These factors include identifying as homosexual and having higher HIV knowledge, the later resulting from information from peers. In Caaguazú, the least developed of the three study regions, identifying as homosexual was also associated with increased HIV prevalence, again as a potential marker for sexual networks with greater numbers of MSM. Uniquely, depression was associated with increased HIV prevalence in Caaguazú. The association of HIV infection with mental health conditions has been noted elsewhere 14 and environmental factors, such as sexual minority stress, are posited to increase the vulnerability of MSM with mental health problems to HIV risk. 15 Notably, we did not find independent associations between HIV prevalence and drug or alcohol use in Caaguazú or Alto Paraná, contrary to a previous study in Paraguay. 16
We recognize limitations of our study. First, our study was implemented in only three of the 17 regions of Paraguay, further variation in HIV prevalence and indicators of risk and preventive behavior across the country are possible. In particular, these three regions contain a large proportion of the urban population of the country, therefor our sample may not represent more remote provinces with larger rural areas. Second, the cross-sectional nature of the data limits causal inference. For example, the associations of HIV with higher HIV knowledge, access to condoms, and lower drug use may be “reversals” of cause and effect in that MSM diagnosed with HIV are linked to care, prevention, and health education programs. Third, variation in access to HIV treatment, as opposed to risk behavior alone, may also contribute to the differing levels of HIV prevalence since prevalence is a function of incidence and survival. Fourth, statistical power may be limited to detect smaller effects sizes for associations with HIV. This may be a particular concern for Alto Paraná which had the smallest sample size. Lastly, social desirability response bias may result in under-estimation for some measures such as illegal drug use and sensitive risk behaviors.
Despite limitations, our data provide a basis for planning and implementing programs for HIV prevention for MSM in Paraguay. HIV prevalence among MSM may be second only to transgender women in Paraguay 17 in terms of relative burden of disease while ranking number one in absolute numbers of people living with HIV. Ending the epidemic in our country will need to prioritize programs that reach these key populations.
Footnotes
Authors’ contributions
Gloria Aguilar: conceptualization, methodology, investigation, supervisation, data analysis, review manuscript
Tania Samudio: conceptualization, supervisation, review manuscript
Julieta Méndez: conceptualization, methodology, investigation, data analysis, draft manuscript and review manuscript
Gladys López: conceptualization, investigation, review manuscript
Liliana Giménez: conceptualization, methodology, investigation, review manuscript
Christian Schaerer: conceptualization, methodology, investigation, data analysis, review manuscript
Santiago Gómez: conceptualization, methodology, investigation, data analysis, review manuscript
Teresita Báez: conceptualization, methodology, investigation, data analysis, review manuscript
Zoilo Morel: conceptualization, investigation, data analysis, review manuscript
Sergio Munoz: conceptualization, methodology, investigation, data analysis, review manuscript
William McFarland: conceptualization, methodology, investigation, data analysis, review manuscript
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
The study protocol was approved by the Ethics Committee of the Central Laboratory of Public Health from Paraguay.
Consent to participate
All participants provided verbal informed consent; minors were deemed emancipated and consented for their participation.
Consent for publication
The survey was conducted anonymously to protect participants’ privacy and identity.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Global fund to fight HIV, TB and malaria; CIRD and Ministry of Public Health from Paraguay.