
Abstract
Background
Following increased rates of domestic abuse/violence (DAV) reporting during the pandemic, London’s online sexually transmitted infection (STI) testing service (Sexual Health London, SHL) introduced routine DAV enquiry and directed survivors to supportive online information. SHL evaluated this adaptation.
Method
SHL’s database identified the first individuals that ordered a test-kit between 17.8.21-28.2.22 and triggered questions disclosing DAV. SHL clinicians only contacted these individuals if positive/abnormal STI results required communicating. Within these interactions DAV was opportunistically discussed and further counselling/support offered.
Results
3846/231460 (1.7%) service users triggered DAV question(s). The first 202 individuals were: median age 28 yrs (18–73 yrs); 66% (134/202) female; 72% (145/202) heterosexual; 75% (152/202) UK born. 27% (55/202) reported physical/emotional abuse, 81% (164/202) coercive control, and 22% (45/202) sexual abuse. 26% (52/202) had never visited a clinic. Telephonic discussion occurred with 10% (20/202) individuals: 10/20 accepted counselling/signposting; 2/20 referred to independent DAV advocate, 6/20 stated historic abuse, 2/20 mistakenly triggered, 2/10 declined support or disengaged. Of 29% (58/202) individuals that ordered another e-kit, 38% disclosed ongoing DAV and 9% sexual assault.
Conclusion
1.7% e-service users reported DAV. Telephonic DAV discussion was accepted by 80% individuals contacted. Despite providing online support 38% experienced ongoing/escalating abuse. Further engagement and support for DAV survivors using e-services is required.
Introduction
Domestic abuse and violence (DAV) is a major, global public health concern. Between 10% and 50% of all women report a lifetime prevalence of abuse from intimate partner(s) (World Health Organization, 2001). 1 The effects of DAV on victims, and their families, can be pervasive, long lasting and devastating. Routine DAV enquiry has proven to be acceptable by healthcare staff and patients. 2 The National Institute for Health and Care Excellence has recommended routine DAV enquiry within UK sexual health services, since 2014. 3 The British Association for Sexual Health and HIV (BASHH) published a national toolkit for staff in these services to screen attendees for DAV and support individuals after disclosure. 4
During the coronavirus-19 pandemic, London’s online sexual health service, Sexual Health London (SHL), rapidly expanded to maintain access to sexually transmitted infection (STI) testing and support sexual health clinics (SHC) that had either closed or whose capacity was heavily compromised. At the same time a global surge in DAV was realised and a call to action was announced by the Home Affairs Committee for innovative strategies to enable safe DAV disclosure and support survivors. 5 In August 2021, SHL introduced routine DAV enquiry and signposted service users who disclosed potential abuse to online support. We aimed to identify the number of service users experiencing DAV, provide a descriptive analysis of these users and explore the outcome of any DAV interventions.
Sexual Health London is an online postal STI testing service collaboratively funded by 30/33 London local authorities. It integrates with SHCs within the participating boroughs using bidirectional referral pathways. SHCs direct asymptomatic London residents (aged 16 years or over) to SHL for STI testing, enabling individuals with significant symptomatology or complex needs to be seen in clinic. SHL refers individuals needing STI treatment/care to SHCs. The e-service is delivered by a consortium comprising Preventx Ltd, Chelsea and Westminster Hospitals NHS Foundation Trust (CWFT) and Lloyds Pharmacy online doctor.
Method
In order to request a STI kit SHL service users must complete a sexual health questionnaire (triage). The triage includes DAV questions relating to emotional or physical abuse (Does a family member or a recent partner make you feel frightened or hurt you?), coercive control (Does a partner (current or last) make you feel like you are being controlled or manipulated?) and sexual abuse (Does someone close to you make you do anything sexual that you don’t want to do or can’t say no to?).
Service users that trigger (respond affirmatively to) any of the DAV questions are shown a message suggesting they may be experiencing abuse and provided with links to SHL DAV support pages: www.shl.uk/support/domestic-abuse-and-violence These pages include details of local/national support organisations, an urgent telephone line for the service user to call the SHL clinical team to discuss DAV (should they wish to) and information on “covering your (online) tracks”.
CWFT staff are responsible for the clinical governance and safeguarding of SHL and comprise the SHL clinical team. An alert/flag is applied to an individual’s electronic patient record (e-note) when they trigger. The SHL clinical team don’t directly contact flagged service users about DAV but if they do so for others reasons (e.g. relaying positive STI results) or if the survivor directly contacts the clinical team for any reason, and it is safe to do so, the alert prompts them to discuss the triggers, perform a safeguarding assessment and offer supportive interventions. Serious cases of concern are discussed with the CWFT safeguarding team which includes two independent domestic violence advocates (IDVA) and a police officer.
DAV questions were incorporated into the triage on 17.8.21. Adult service users who reported potential DAV, whilst completing a triage between 17.8.21 and 28.2.22 were identified from the SHL database. The e-note of the first 202 service users to trigger were manually reviewed and demographic data were collected. Approximately 10% of service users receive abnormal results requiring SHL clinical intervention so this sample size was deemed sufficient to evaluate acceptability of opportunistic DAV discussion.
Results
Demographic data and types of domestic abuse reported by service users.
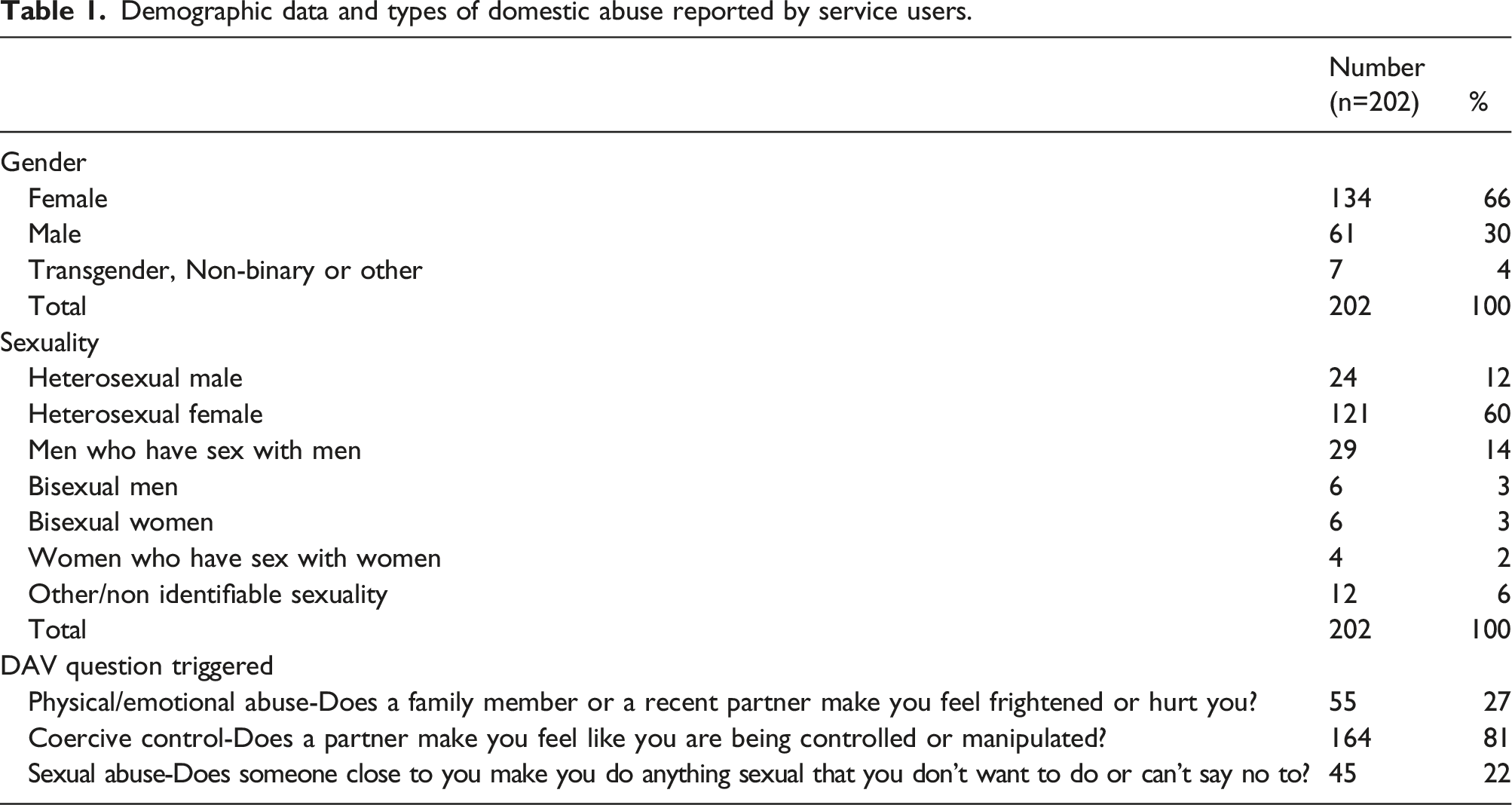
264 triggers were selected by 202 service users and shown in Table 1: 81% reported coercive control, 27% physical/emotional abuse and 22% sexual abuse. Ten (5%) service users triggered all three DAV questions, 42 (21%) two questions and 150 (74%) one question.
The SHL team received contact by the service user or had a reason (aside from DAV trigger) to make contact with the service user in 31 cases (15.3%). Eight service users reported a recent sexual assault, and had declined input around this so were not contacted, and three did not respond to contact efforts. A telephonic discussion took place in twenty (10%) service users: 10/20 accepted counselling and signposting to other services of which two were referred to an IDVA, 6/20 stated the abuse was historic and required no further action, 2/20 claimed to have triggered by mistake, one service user 1/10 declined support for current abuse and another 1/10 disengaged after initial contact.
29% (58/202) of service users revisited the service to order further STI test kit(s). Of these, 38% (22/58) continued to trigger the DAV questions: 23% (5/22) triggered on different or additional DAV questions and 9% (5/58) disclosed a new sexual assault.
Sexual health details, obtained from the triage responses, included high risk activity and indications for additional sexual health interventions. See Figure 1. 77% (156/202) individuals engaged in high-risk activity (e.g. chemsex, sex parties), were from a vulnerable group (e.g. HIV positive, sex worker), or were eligible for urgent preventative interventions (e.g. HIV post-exposure prophylaxis). Sexual Health triage responses including high risk activity and eligibility for additional interventions.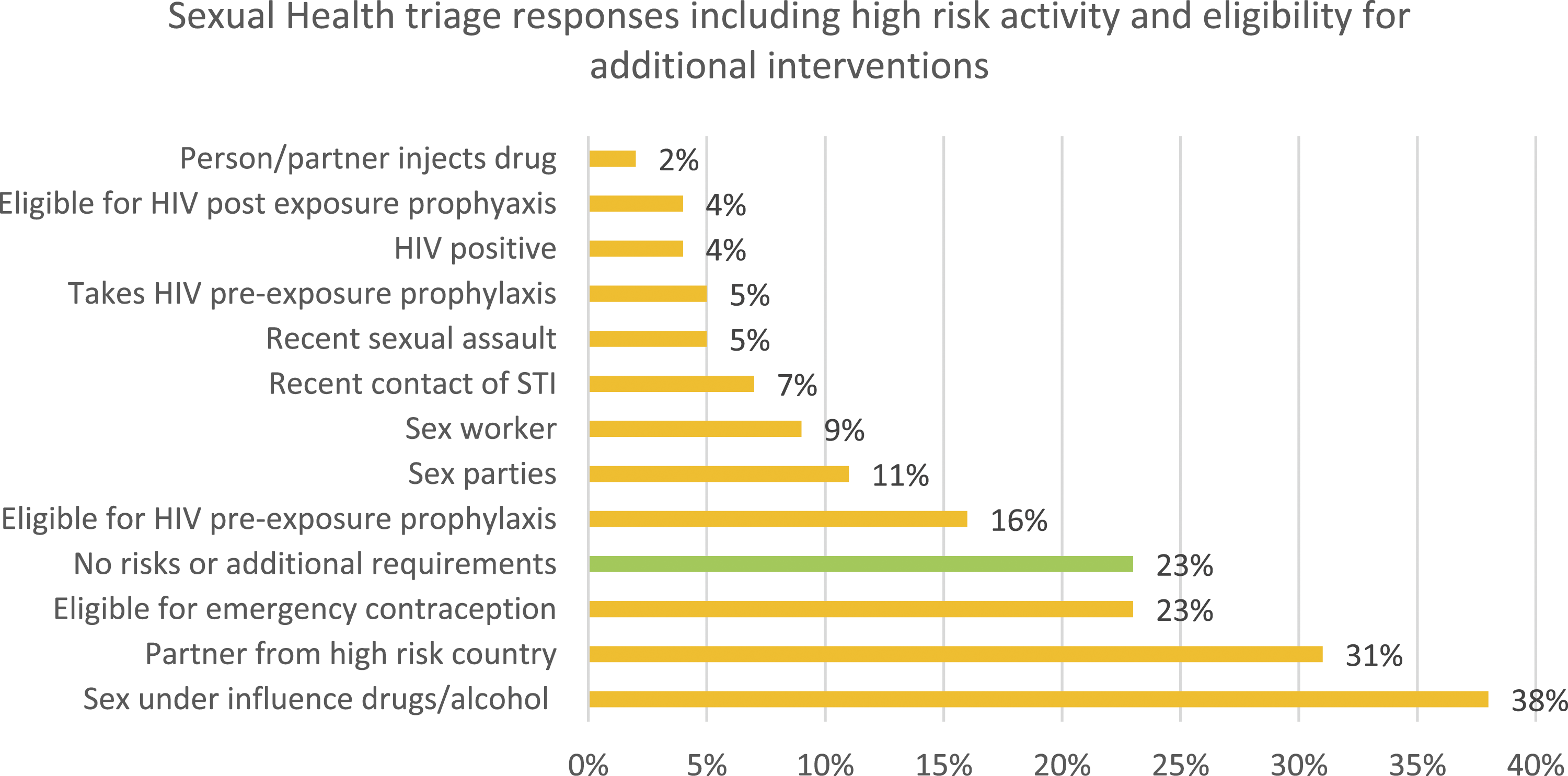
The STI kit return rate was 76% (154/202) and STI positivity 4% (chlamydia, gonorrhoea and syphilis). 26% (52/202) had never visited a clinic.
Discussion
Provision of sexual and reproductive healthcare via digital services has seen an exponential expansion globally, which has become more evident because of the pandemic. Online STI testing services account for 40% of STI screens in England, having experienced a 34% increase between 2019 and 2020. 6 SHL receives over 50,000 STI test kit orders a month, has experienced a 2.4 fold increase in kit orders over the pandemic making it one of the largest publicly funded online sexual health services in the world. This is the first international study to report the results of routine DAV enquiry within online STI testing services.
We found 1.7% of online service users disclosed potential DAV. This is comparable to the prevalence of DAV reported by London SHC attendees (Barker 2.2%, Sohal 4–7%, Weller 0.57%) but lower than estimates (5.5%) amongst the wider population in England and Wales.7–9 The characteristics of those triggering are similar to other studies in that most are young, female and of white ethnicity. The surge seen in national DAV data where coercive control is overrepresented also mirrors our findings. 10
There are limitations in performing routine enquiry online compared to during clinic attendance. Weller et al demonstrated routine DAV enquiry, via telemedicine, in a London SHC to be effective and increased disclosures compared to pre-pandemic. 9 Otherwise there is limited international data on the outcomes of routine enquiry using digital or remote methodologies. Enquiry in clinic is usually conducted within a face-to-face interactive discussion, having built rapport with staff and trust obtained from the attendee. BASHH recommend the four step enquiry method (Ask. Validate. Assess. Action) to aid disclosure and engagement. Tools such as the Power and Control wheel can be used to help victims recognise they are in an abusive relationship and prompts such as visual signs and non-verbal cues can lead a discussion to successful disclosure. 11 Although digital services are accessible 24 hr/7, days a week and ask every service user about DAV, making every contact count, without a nuanced discussion or personalised interaction they may be less likely to identify and therefore support survivors of abuse. Furthermore SHC policies usually aim to see attendees on their own whereas the safety of a digital user can’t be assumed or easily verified.
It is concerning 38% of service users who revisit SHL continue to disclose abuse with a quarter reporting escalating abuse. This suggests the DAV information content on SHL is insufficient in isolation. Unfortunately there is no evidence from randomised trials of a beneficial effect of eHealth interventions on DAV. 12 Given the acceptability of telephonic support in this study, there appears an unmet need in providing interactive support that supplements online information, to all survivors who may want it. A means of capturing consent to contact the service user as well as agreeing a safe and convenient time and an acceptable method for that contact, are all factors that need to be considered to meet this demand.
Immediate substantial DAV support can be provided during a SHC attendance. Over 75% individuals disclosing abuse require additional sexual health interventions that SHCs routinely provide. Yet a quarter of our survivors have never accessed SHC. Reasons for non-attendance to clinic can be manifold–geographical distance, inconvenient opening times, travel costs, stigma, embarrassment and isolation or because overburdened clinics increasingly direct asymptomatic individuals to test online. DAV is indiscriminate and can affect anyone, from any walk of life, and with the expanding use of internet STI services it is becoming important these services consider routine DAV enquiry, establish appropriate effective referral pathways to SHCs and DAV organisations and/or develop digital solutions that effectively support survivors.
SHL plan to use a larger dataset to further analyse online service users according to the types of abuse experienced. Further work is also required to explore and evaluate safe, effective and evidence based methods of identifying, engaging and supporting all survivors of abuse who access online services. Harnessing the expertise of our regional IDVA network would be welcomed. Most importantly with a sustained crisis in global funding of DAV services, efforts to scale up support must be underpinned by appropriate and increased provision of funding.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.