
Abstract
Background
Different countries in sub-Saharan Africa (SSA) have established guidelines to reduce HIV transmission and improve its management in prisons. This narrative review aimed to examine established literature on HIV care and management among incarcerated persons in SSA to identify successful interventions that could inform improved guidelines, policies, and practices related to the clinical care of this population.
Methods
We searched PubMed, Scopus, Web of Science, Embase, and TRIP Medical Databases in August 2022 for articles published between 1st January 2010 and 30th June 2022. We identified 27 eligible articles based on the Population/Concept/Context framework.
Results
HIV screening primarily involved mass campaigns rather than formal prison programmes, with limited implementation of universal testing and treatment. Although a few studies reported on access to antiretrovirals (ARVs), prisoners in urban areas and females had disproportionate access. Barriers identified include poor living conditions, high levels of stigma, and resource constraints. Inter-prison transfers, release from prison, and lack of established programmes hindered follow-up and linkage to care.
Conclusions
The implementation of strategies such as universal testing and treatment, human resource strengthening, financing plans for testing, ARV care, and frequent assessment of risk could improve HIV care and management in prisons in SSA.
Keywords
Background
In many countries, the prevalence of HIV in prisons is reported to be several times greater than in the general population.1,2 Compared to other regions of the world, sub-Saharan Africa (SSA) has the highest proportion of incarcerated people living with HIV. 2 A meta-analysis of the prevalence of HIV in prisons reported a pooled prevalence rate of 6% for Africa. 2 Mirroring global trends, the prevalence rates of HIV are higher in female prisoners than in their male counterparts.2,3 The high prevalence of HIV in prison populations in SSA has been attributed to factors such as prison overcrowding, risky sexual behaviour before and during incarceration, drug injection, weak infection control, limited access to HIV services, and recidivism.4,5
While HIV poses a significant physical health and psychological burden on individuals, its effects in incarcerated populations are more severe. For instance, the incidence of tuberculosis (TB), a major cause of mortality among people living with HIV (PLHIV), is considerably higher in correctional settings. 6 For instance, Edge et al. reported that co-infection of HIV and TB among prisoners ranged from 2.4 to 74.3%. 7 Other comorbid conditions such as liver fibrosis are higher among prisoners living with HIV. 8 Also, the double stigma of being incarcerated and living with HIV has significant mental health implications.9,10
Incarcerated persons often receive insufficient attention in their HIV care compared to PLHIV in the general population in Africa. 3 Additionally, guidelines and policies on HIV care are not routinely followed in prisons in Africa.11,12 The WHO consolidated guidelines for key populations focus on specific areas including “HIV prevention, harm reduction, HIV testing and counselling, HIV treatment and care, sexual and reproductive health, and the prevention and management of co-infections and co-morbidities”. 12 However, policy implementation varies significantly across countries, with some countries such as South Africa, having made more progress in translating policy into action, compared with other SSA counterparts. 3 Furthermore, even in countries where guidelines have been adopted, their degree of efficacy has not been fully elucidated. 13 The overall impact of HIV policies in prisons in SSA requires evaluation to determine their efficacy, progress made, and limitations to their implementation.
Numerous barriers may prevent adequate, sustainable, and effective care of incarcerated persons. These include limited human resource capacity, poor financing, HIV-related stigma and lack of understanding, weak referral systems or linkage to care, and inadequate health and prison infrastructure.3,14 Furthermore, stigma by prison staff affects management and follow-up as well as trust between inmates and their service providers. 15 Individual-level factors such as mental health, risky behaviours (e.g., substance abuse and unprotected sex), and violence also contribute to challenges in management among incarcerated persons. 14 Timely reviews of progress made and persisting barriers in care are useful and necessary to direct interventions to improve care and management and thereby reduce the disease burden in this vulnerable population. This narrative review aimed to examine established literature on HIV care and management among incarcerated persons in SSA to identify successful interventions that could inform improved guidelines, policies, and practices related to the clinical care of this population.
Methods
We performed a comprehensive literature search from multiple data sources including PubMed, Scopus, Web of Science, Embase and the Trip medical database in August 2022, to identify original research articles on HIV care and management among incarcerated persons in SSA. Search terms used to identify literature included ‘incarcerated’, ‘prison*’, ‘inmate*, ‘convict*', ‘jail*’, ‘HIV’, ‘Human Immunodeficiency Virus’, ‘Persons living with HIV’, ‘PLHIV’, ‘AIDS’, ‘acquired immunodeficiency syndrome’, ‘ART’, ‘ARV’, ‘Retrovir*’, ‘sub-Saharan Africa’, ‘Africa’, and ‘Africa South of the Sahara’. The Boolean terms ‘AND’ and ‘OR’ were used for the final search results. The search terms were formed using the ‘Population (or participants)/Concept/Context’ (PCC) framework. Eligible materials were original research articles including cross-sectional studies, cohort studies, case-control studies, and systematic reviews published between 1st January 2010 and 30th June 2022. Both qualitative and quantitative studies were included with no language restrictions. For articles written in French, the English version of the article was obtained from the publisher. Where this was not possible, Google Translate was used for translation, with corroboration by a French-speaking researcher for any unclear translation.
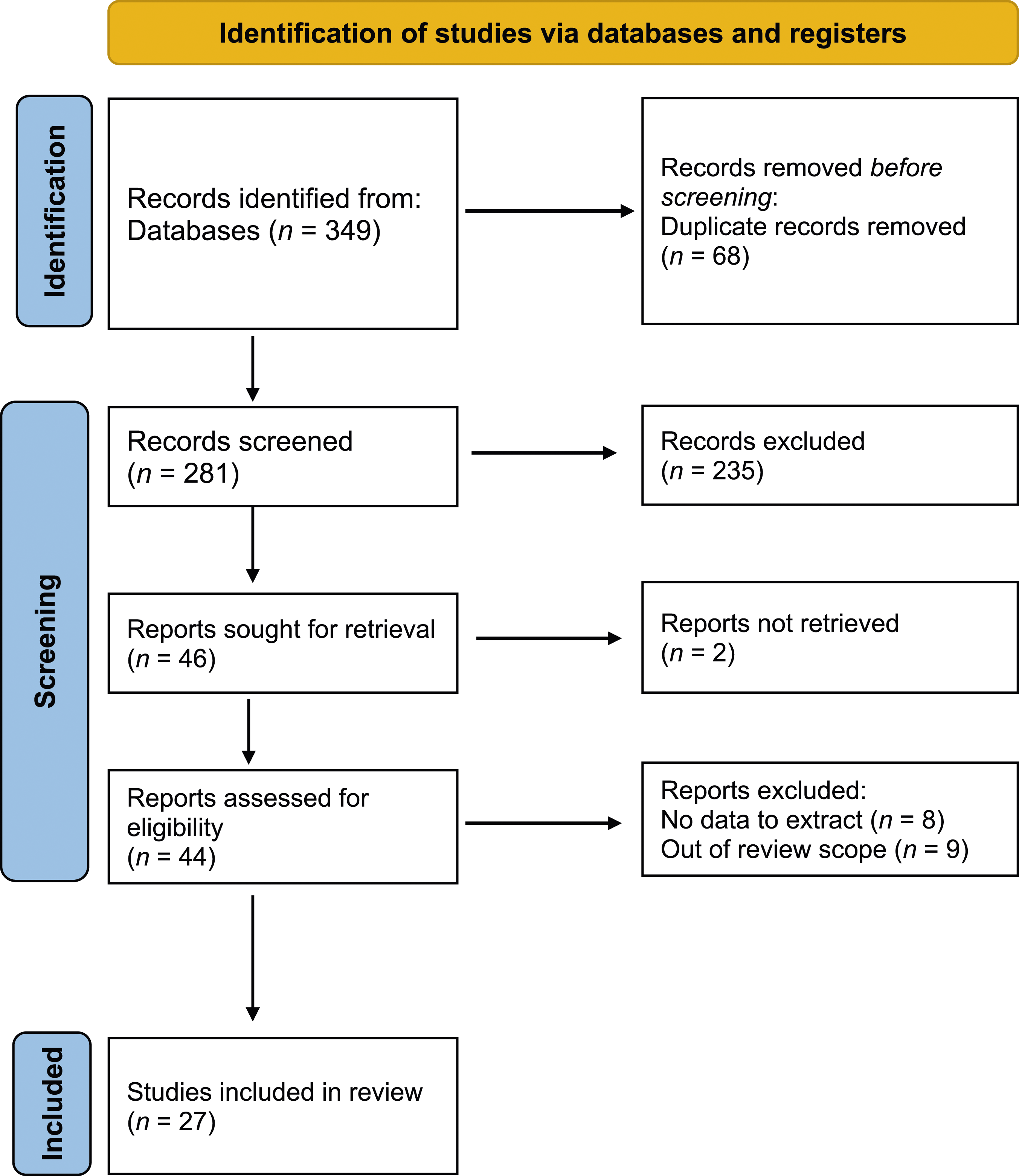
The title and abstract of each article were independently reviewed by three reviewers for inclusion. The inclusion criteria were 1) Original research articles on HIV care and management in incarcerated persons in SSA; 2) Review articles on HIV care and management in incarcerated persons in SSA; and 3) Articles published between 1st January 2010 and 30th June 2022. Disagreements were resolved by consensus. Themes that guided the review process on which reviewers built a consensus included: 1) Testing interventions (including screening and diagnostic testing); 2) Therapeutic interventions (including ART and non-ART related therapy, and counselling); and 3) Interventions related to linkage to care and follow-up. Our initial literature search identified 349 potential articles, which were imported into the Rayyan software, after which 68 duplicates were removed. We screened 281 abstracts and excluded 235 due to reasons such as studying the wrong population, being unrelated to HIV, occurring outside of sub-Saharan Africa, and the study setting being outside of the prison. Forty-six abstracts were selected for full-text review, after which 27 were identified as suitable for inclusion in relation to this narrative review (see Figure 1). The other 19 papers were excluded because they did not have any data to extract, did not focus on the key themes to be discussed, or could not be accessed in full text. PRISMA diagram.
16
Results
Characteristics of studies reviewed
Summary of studies included in the review.

Screening for HIV
Six studies assessed interventions involving screening campaigns that estimated the prevalence of HIV in prisons across different countries.8,17,24,26,34,36 On the one hand, the studies suggest weak HIV infection control practices in SSA prisons in terms of screening at entry, during incarceration, and at exit from prison. This is reflected in the low proportion of inmates who knew their HIV status prior to screening. For example, only 3.2% of 30,571 inmates included in a screening programme at five correctional facilities in South Africa knew their HIV status prior to screening. 26 On the other hand, the studies indicated a relatively high uptake of HIV screening among inmates despite the stigma associated with HIV. Maggard et al., 34 found that the involvement of inmates as peer educators encouraged inmates’ participation in HIV and tuberculosis screening programmes in prisons.
The most common approach reported in these studies involved mass screening of inmates, with findings indicating a higher prevalence of HIV in prison settings compared to national estimates.17,24,26,34,36 For example, Maggard et al., reported an HIV prevalence of 22.9% during a mass screening of inmates in six prison facilities in Zambia. 34 In another screening campaign in five South African correctional facilities, Stevenson et al. found an estimated HIV prevalence of 17.7% with most (73.4%) being previously undiagnosed. 26 Prevalence rates of HIV were found to be considerably higher among female prisoners compared to male prisoners.17,24 Studies that reported on screening of new prison entrants suggest lower HIV prevalence rates in these populations compared to existing inmates and those exiting prison.24,36
Two studies34,36 included screening of encampment residents with findings suggesting that prevalence rates among encampment residents are relatively higher compared to the general population. Only one study 24 included screening of juveniles, with results showing a considerably lower prevalence of HIV among juveniles (3.9%) compared to adult prisoners (15%).
The only study that focused on comorbidity between HIV and mental health problems 10 showed a high prevalence of mental illnesses among female inmates living with HIV. In particular, most (70.6%) of the female inmates with HIV reported depressive disorder, and nearly half reported alcohol use disorder (48.4%) and post-traumatic stress disorder (46.8%). The results from this study underscore the need for integration of mental health services into prison health care, especially for inmates living with HIV.
Feasibility and sustainability of testing interventions
Three of the studies examined the feasibility and sustainability of HIV-related interventions in correctional settings. Based on three correctional facilities in South Africa and Zambia, Mukora et al. identified resource requirements and provided a costing guide for implementing and scaling up Universal Test and Treat (UTT), a population-based HIV intervention that involves HIV testing services, ART initiation, and ART maintenance, in correctional settings. 20 The unit cost of implementing UTT in correctional facilities was observed to be higher than in community settings. Substantial variations were also observed in the estimated cost and cost drivers of implementing UTT across prisons. These variations were linked to differences in staff costs, security requirements, and cost of supplies in the three correctional facilities.
In an earlier qualitative study in the same prisons, Topp et al., 29 highlighted the importance of policy framework, resource adequacy, and efficiency of health service delivery systems in the feasibility and sustainability of quality UTT in correctional facilities. In particular, the existence of national UTT policy and systems for delivering and monitoring HIV care served as a backbone for the successful implementation of UTT and enhanced its sustainability in South African correctional facilities. In contrast, although implementation of the UTT was found to be feasible in Zambian correctional facilities due to alignment with national policy and positive attitudes towards HIV care, lack of resources and weak health delivery systems were found to undermine the programme’s sustainability.
Access to antiretroviral therapy
Generally, only a few studies reported access to ART, other treatment strategies, and supportive treatment. In some jurisdictions, there was reasonable satisfaction with ART services and a high intake of antiretrovirals (ARVs). However, prisoners in urban areas were reported to have more access to ARVs than those in rural areas. Also, females were less likely to have access to ARVs. In the paper by Todrys et al., none of their prisons offered cotrimoxazole prophylaxis in Zambia, and there was no availability of condoms in the prisons assessed. 39 Also, Motshabi et al. presented on lack of ongoing counselling. 38
Treatment adherence and coverage
Strategies for adherence to ART were diverse. Fuge et al., 19 in Ethiopia reported good adherence when inmates were offered a medication schedule. However, in Namibia, Shalihu et al., 35 described that there were no reminders for inmates to take their medication. Notably, supportive treatments such as cotrimoxazole use were broadly not reported. The ability to remind the prisoners to take their medications was closely related to the number of prison officers trained and available to dispense medications. The ratio of the healthcare staff to the prison population was linked to delay in linkage to care in Ethiopia. 19
Treatment coverage was generally poor. Jaquet et al. reported that only one of the eighteen inmates surveyed was aware of their status and was started on ARVs. 8 Common themes that affect treatment coverage include a reduced ratio of health staff to inmate populations, delay in linkage to care and loss of follow-up with the transfer of inmates to other prisons.
Barriers and facilitators
Several barriers were identified in accessing ARVs and other supportive services. Some obstacles included inadvertent disclosure of inmates' HIV status to the rest of the population, high levels of stigma, poor living conditions, limited human resources, and fragmented referral systems. Other factors included inadequate medical and drug supplies and a lack of adolescent-friendly services.22,32,35
Despite these challenges, a study in Ethiopia found that medication adherence improved with the use of radio and television, as well as social cues such as the sunset. Also, access to information through peer education and support and building organizational capacity and infrastructure were found to facilitate management. 19
Outcomes of care
Several studies assessed the outcomes of care among incarcerated persons. These outcomes include viral load suppression (defined as having less than 1000 copies of HIV per millilitre of blood) whilst on ART, rates of loss to follow-up within the prison, during transfer to another facility or after release, and finally linkage to further care whilst incarcerated or at the time of release.
Viral load suppression
In their study, Fuge et al., 19 found viral load suppression to be slightly lower for inmates (94%) compared to non-incarcerated persons (95.5%), although the difference was not statistically significant. It was also found that the risk of poorer viral load suppression was associated with female prisoners, those aged 31-35, and those facing stigma. Similar rates of viral load suppression were reported in a retrospective cohort study in South Africa, where among ART-naive patients, viral suppression was achieved in 94.7% of cases. 32
Linkage to care and loss to follow-up
Linkage to care within prisons and after release is also a key component of HIV care and management. Among South African inmates, roughly two-thirds (65%) self-reported linkage to care. 27 Fernando et al., 21 found that peer-based rehabilitation had no significant association with linkage to care after release; however, being imprisoned at a long-term site was associated with a higher likelihood of post-release linkage to care. Furthermore, Mabuto et al., 27 identified that factors such as older age, initiation of ART during index incarceration and longer duration of incarceration were associated with a higher likelihood of self-reported linkage to care.
In a prospective cohort study conducted in South Africa and Zambia, in which clinical outcomes for incarcerated persons with HIV were examined following a UTT intervention, it was found that 95% of inmates were retained in an onsite ART programme at 6-month follow-up, and that of these, 97% had achieved viral load suppression (<1000 copies per ml). 28 However, these high retention rates were not demonstrated in another study conducted in a correctional facility in South Africa, where roughly 59.7% of inmates were in follow-up care 6 months after ART initiation, and only 33.9% at month 12. 32
Discussion
Despite its importance in the management of HIV, we found that routine screening of incarcerated persons for HIV is largely absent in many prisons in SSA. This situation constrains the diagnosis and treatment of inmates who may be living with HIV, and thereby undermine efforts at preventing the transmission of HIV. The absence of routine HIV screening in prisons in SSA could be attributed to resource and capacity limitations for managing infectious diseases, especially HIV, in correctional settings. Nonetheless, our review suggests that prison inmates may be less likely to resist routine screening efforts, which could facilitate efforts towards the management and prevention of HIV. Indeed, it has been suggested that the implementation of HIV-related intervention is relatively easier in prison populations due to the ease of access to the inmates. 34
Findings from studies that focused on mass screening as broader HIV-related interventions underscore the high HIV burden among prisoners. The reported prevalence rates are considerably higher than national or regional averages,26,34 although some of the studies suggest a decline in prevalence rates over time. 26 Similar to findings in other reviews, 2 female inmates were at greater risk of being HIV-positive. It is important to note, however, that the few studies that included screening for HIV in prisons as part of an intervention were done in southern and central Africa. Thus, estimates reported in those studies may not be representative of other regions in Africa.
While individuals with poor health may be more likely to be incarcerated because conditions commonly associated with poor health (e.g., illicit drug use, unemployment, and poverty, etc.) also increase the likelihood of involvement with the criminal justice system, 36 findings from the reviews suggest that prison conditions may increase the likelihood of HIV transmission. This is seen not only in the relatively higher prevalence of HIV found among prisoners in exit screenings but also among individuals living around prison encampments compared to the general population. The higher prevalence of HIV among residents in prison encampments has implications for strategies for the management and prevention of HIV infection.
Interventions that focus on testing all inmates followed by treatment of those diagnosed with HIV, such as UTT, have been found to be effective in the management and prevention of HIV in the general population. UTT encompasses a strategy that recommends screening all populations at risk of HIV and initiating therapy for those diagnosed as HIV positive earlier, regardless of their WHO clinical stage or CD4 count. It includes active testing, adherence counseling, improvement in treatment coverage, and outcomes of HIV infection. 12 It is, however, important to note that evidence on the feasibility and sustainability of UTT in prison settings appears inconclusive. Such programmes tend to thrive on dedicated healthcare systems and the availability of resources. 28 However, the apparent neglect of healthcare systems in prison settings in many countries in SSA could undermine the feasibility and sustainability of UTT due to the high cost of implementation and resource limitations.
Access to healthcare is a measure of the proportion of a population that gets appropriate health services. It is primarily used to assess the inequities in the reach of healthcare. 40 Although HIV treatment is widely accessible, we found in this review that the provision of services in different SSA jurisdictions was vastly different. Whereas in parts of Ethiopia and South Africa, they reported reasonable satisfaction with ART services and a high coverage of ARVs for inmates, prisoners in Namibia said that they did not get reminders to take their medication, suggesting a lack of physical accessibility.19,22,35 With this evidence, it may be reasonable for ART services within correctional centres to provide structured systems or schedules to notify inmates of treatment times and how they may readily access medicines.
Furthermore, even in the same setting, prisoners in urban areas reported having better access to ARVs than their rural counterparts. 4 Again, female prisoners had disproportionately less access to antiretroviral therapy.19,23 A recent study by Blue et al. 41 reported that, in North Carolina, apart from the issue of access to medicines while incarcerated, the availability of ARVs was further impacted by inadequate prison resources. The limited health and human resource capacity in African settings has been well elucidated, and such challenges within prison settings pose a significant risk to the adequacy of care received by inmates, as was reported in some of the studies reviewed.
Closely related to access to ARVs is treatment adherence. Adherence can be measured either by a direct method, such as the medication possession ratio or an indirect approach, such as self-reporting. 42 In Ethiopia, prisoners could adhere to ARVs because they were given specific medication schedules, improving adherence. 19 Some strategies that have been proposed to enhance adherence and promote coverage include structured guidance, care continuation and professional assistance. 43 In their 2006 guidance, the WHO also recommends the provision of treatment and support equivalent to what exists in the community. 44
In providing optimal HIV care and services to this vulnerable population in SSA, several barriers were identified in our review, including non-disclosure and inadequate medical and drug supplies. 30 The prison population already faces challenges such as limited resources that result in understaffing. The limited staff also must take care of other healthcare needs of the inmates, making them unable to provide optimal care to prisoners living with HIV. 45 Additionally, education on risk reduction measures such as teaching condom use and prevention of STIs should form part of HIV care services within prisons.18,31,33
This review found rates of viral load suppression among inmates, including those who were treatment naïve, of greater than 90%. The high viral load suppression rate suggests that ART regimens are effective among the incarcerated population when they receive the appropriate level of care. Similar findings were reported in a previous systematic review of outcomes of antiretroviral therapy among prisoners. 46 The major implication is that the care continuum and provision of ART therapy must be appropriately maintained to achieve viral load suppression among prisoners living with HIV.
Self-reported linkage to care following release was found to be higher among older inmates and those who had been incarcerated for a longer period. It may be possible that self-reported rates are higher than actual rates of linkage to care, and therefore the true figure of those receiving continued therapy after release may be lower. Notwithstanding, studies in the USA have found similar trends in factors associated with linkage to care among incarcerated populations,47,48 albeit with a lower rate of overall continuity of care, estimated at roughly 36% of inmates. 27 It has been suggested that higher rates reported in studies from South Africa compared with the United States are related to free HIV care in South Africa compared to the USA and lower rates of illicit drug use. It is, however, important to note that risk-taking behaviours were still highly prevalent among inmates from South Africa, including the use of mandrax. 33 The implications for other African countries would be to ensure that risk reduction measures to reduce HIV spread within prisons and to encourage sustained HIV care post-release.
Furthermore, potential factors related to loss to follow-up or inadequate linkage to care may be related to the movement of inmates. 37 For instance, transferring inmates from one correctional institute to another was found as a potential reason for loss to follow up in the paper by Telisinghe, Hippner. 32 In the studies reviewed, there was little mention of specific interventions directed at ensuring linkage to care for inmates living with HIV. Without the institution of systems to ensure that therapy is maintained for prisoners in transition (e.g., upon release or from transfer from one site to another), loss to follow-up may continue to be prevalent within this population, reversing gains that have been made with viral load suppression.
Best practices in HIV care and management in prisons
A few measures emerged from our review that could be highlighted as best practices in the management of HIV in correctional settings in SSA. Prominent among these practices is the introduction of UTT in some southern African prisons. UTT seems to offer a more comprehensive approach to the management and prevention of HIV in correctional settings. According to Herce et al., the utility of UTT in prisons lies in its potential to “achieve levels of same-day ART uptake, retention in care, and viral suppression among incarcerated people with HIV that are comparable to those observed in community settings” (32, p. 1).
Additionally, measures such as offering medication schedules, setting reminders, and giving a supportive treatment environment were identified as best practices that can enhance treatment adherence. For instance, in some studies, the provision of extra portions of food to prisoners living with HIV helped alleviate the taxing effect of ART and enhance medication adherence. Access to basic gadgets like clocks also enhanced medication adherence, as they served as reminders for the administration of medication.
The involvement of inmate peer educators as actors in intervention delivery seems to hold promise for the management of HIV in prisoners. In this strategy, incarcerated persons are trained and mentored to provide services including psychosocial support and health education as part of health intervention delivery in prisons. 3 This practice can help to increase uptake in HIV interventions, minimise demands on highly trained and scarce professionals, reduce the cost of intervention delivery, and facilitate linkage to care. 34
Recommendations
A notable challenge with the implementation of HIV interventions in prison settings in SSA is the lack of access to testing and treatment services and the lack of resources and capacity to provide adequate testing and treatment services to prisoners. Thus, successful implementation of HIV interventions in SSA prisons requires strengthening of human resource capacity for HIV-related interventions including the training of prison healthcare personnel.
Additionally, funding is a likely impediment to the sustainability of interventions involving testing, ART, and continuity of care in prisons, as the cost of implementing HIV interventions seems to be considerably higher in correctional settings than in the general population. This calls for the development of innovative financing plans for HIV-related care in prison. For instance, social impact bonds, a means of attracting private sector capital to address social problems have been suggested as an innovative approach to funding HIV treatment. 49 This funding model, which has been experimented with in fighting malaria in Mozambique, 50 may be a useful approach to funding HIV, especially in correctional settings.
Our findings further call for a move away from ad hoc implementation of HIV prevention and treatment measures to more structured and regularized measures. This would involve implementing periodic screening for HIV and comorbidities including TB and mental illness, with subsequent provision of appropriate linkage to care for all conditions identified. This should be supported with structured treatment schedules for inmates, measures to improve adherence, gender-specific programming for HIV management, and structured linkages to care systems for prison-to-prison transfers. Improving the ratio of health care staff to inmates could also enhance linkage to care within prisons.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Global Fund to Fight AIDS, Tuberculosis and Malaria.