
Abstract
Background
To our knowledge, the prevalence, risk factors and distribution of C. trachomatis genotypes are rarely mentioned in Vietnam. This study aimed to find the prevalence, risk factors and distribution of C. trachomatis genotypes in infertile Vietnamese women.
Methods
Endocervical swabs were collected from infertile women at the National Hospital of Obstetrics and Gynecology, Vietnam, between January 2020 and December 2021. All samples were analyzed for C. trachomatis presence by Cobas 4800 CT/NG Test. Sequencing methods of ompA gene were used to determine the C. trachomatis genotypes. An approximately 1200 bp ompA fragment was aligned with reference sequences from GenBank to identify the corresponding genotype.
Results
The prevalence of endocervical C. trachomatis infection was 15.6% of 761 participants. Factors independently associated with CT infection among infertile women, obtained by multivariate analysis, included abnormal vaginal discharge, cervicitis, lower abdominal pain, a history of ectopic pregnancy, having more than one sex partner, and age at first intercourse. Among the samples, genotype E (25.93%) was most frequently found, followed by genotypes D/Da (22.23%), F (13.58%), G/Ga (12.35%), J (12.35%), H (6.17%), K (3.70%), B/Ba (2.47%), and I/Ia (1.23%), respectively. Genotype F was related to types of infertility, and genotype H was associated with a history of miscarriage.
Conclusions
The present study indicated a high prevalence of C. trachomatis in infertile Vietnamese women. The most common genotypes found in this population were E, D, and F. Our findings suggest that routine screening is necessary for early detection and performance of infection control methods.
Introduction
Chlamydia trachomatis (CT) is known as the most common bacteria of sexually transmitted diseases (STD) worldwide. CT is an obligate, intracellular, nonmotile, gram-negative bacterium.1,2 This etiological agent also occurs among infants and immunocompromised adults as infections of the eyes and respiratory tract.3–5 In women, CT has been found in 3%–30%, usually asymptomatic, but may lead to ectopic pregnancy, pelvic inflammatory disease, and infertility if left untreated. 6 Chlamydial infection of the lower genital tract is also known to be a risk factor for cervical cancer and human immunodeficiency virus (HIV) infection.7–10 Therefore, the prevention and control of this etiological agent are urgently needed. 9
Currently, CT is divided into 19 human genotypes based on the antigenicity of their MOMP and are categorized as A, B/Ba, C, D/Da, E, F, G/Ga, H, I/Ia, J, K, L1, L2, L2a, and L3.8,11 According to previous studies, CT genotypes A–C are usually responsible for trachoma, genotypes D–K are mostly responsible for urogenital infections, and genotypes L1–L3 predominate in lymphogranuloma venereum.10,11 Epidemiological data worldwide have pointed out that the distribution of CT genotypes varies by gender, geographic region, ethnicity, and sexual behavior. 8 A previous study showed that, differences in virulence of specific genotypes might be the cause of diverse clinical presentations of chlamydial infection. 12 Hence, an understanding of the genotype prevalence associated with CT infection and disease in humans is necessary to inform the design of effective control programs for sexually transmitted diseases. 11
In Vietnam, the diagnosis of chlamydial infection is not routinely performed, and the infection is not informed to the Health Department. However, previous studies showed that the prevalence of chlamydial infection in Vietnamese women of reproductive age varies between 3.7% and 48%.13,14 Although several studies have indicated the prevalence of chlamydial infection in Vietnam, there is a lack of reports on infertile women. Additionally, data on CT genotypes among humans have been poorly reported. Thus, this study has been performed to determine the prevalence, risk factors and distribution of CT genotypes isolated from endocervical specimens of infertile Vietnamese women.
Materials and methods
Study design, duration, and participants
The current cross-sectional study was conducted at the National Hospital of Obstetrics and Gynecology (1000 beds; Hanoi city, Vietnam), located in North Vietnam between January 2020 and December 2021. Participants were selected from among infertile women attending the outpatient clinic. From January 2020 to December 2021, the total population served by this clinic was about 9,274, with approximately 2276 cases undergoing infertility treatment. All cases of infertility were tested for Chlamydia trachomatis (CT) and Neisseria gonorrhoeae (NG) using Cobas 4800 CT/NG Test (Roche, Germany). The inclusion criteria were: (1) determination as an infertile woman via self-report or as identified by a gynecologist, (2) willingness to participate in current study, (3) a written informed consent form for the enrollment, and (4) willingness to answer questions in the questionnaire. Exclusion criteria were as follows: they declined to grant consent, the use of any systemic or topical antibiotics (doxycycline, tetracycline, azithromycin, or erythromycin) for treating urogenital CT infection in the preceding 7 days, HIV infection, active menstruation, and had an invalid sample for PCR. All participants in the study were informed of the benefits, intent of the research, and the procedures to be utilized in collecting the data. Out of the 2276 cases, 61 did not meet the selection criteria and were eliminated.
Sample size estimation and sampling technique
The sample size for this study was determined using Kish Leslie formula with the reference infection rate of 15.7%. 15 With a 95% confidence interval, an absolute precision of 5% and an anticipated population proportion, the minimum sample size was 204 infertile women. However, a total of 761 infertile women were enrolled. The study subjects were enrolled conveniently until the sample size was achieved.
Data/sample collection
Participants were interviewed by gynecologists, nurses, and trained research staff to obtain socio-demographics, medical history, symptoms, sexual history, previous history of sexually transmitted infections (STIs) of partner, and obstetrical and gynecological history. The study procedure and questionnaire were designed to follow the hospital patient management protocols.
Clinical samples
Endocervical swab specimens included in this study were obtained from the cervix of 761 infertile Vietnamese women at the National Hospital of Obstetrics and Gynecology (1000 beds; Hanoi city, Vietnam), located in North Vietnam. Samples were taken from each individual by trained nurses with sterile cotton swabs according to the manufacturer’s instructions for the Cobas 4800 CT/NG Test (Roche, Germany) after obtaining written informed consent. Subsequently, these specimens were transported to the clinical microbiology laboratory within 2 h for diagnosis of CT infection.
Chlamydia trachomatis detection
Endocervical swab specimens were analyzed for CT presence by Cobas 4800 CT/NG Test (Roche, Germany) and Cobas 4800 system following the manufacturer’s protocol. CT positive specimens were stored at −20°C until DNA extraction for CT genotyping.
Polymerase chain reaction amplification of ompA gene
CT genomic DNA was extracted from 500 µl of Cobas® PCR Media (Roche) using QIAamp DNA Mini Kit (Cat.No.: 51304, Qiagen, Germany) with DNA Bacteria protocol, following the manufacturer’s instructions. The concentration of total DNA was measured by using a NanoDropTM 2000 Spectrophotometer (Thermo Scientific, USA). DNA extracted from the samples was maintained at −20°C until used in the PCR reaction.
In this study, to increase the sensitivity of the ompA gene amplification, semi-nested PCR reactions for this target were used as described previously. 11 In the first round, the ompA gene was amplified by using two primers: CT1 (forward: 5’-GCC GCT TTG AGT TCT GCT TCC TC-3’) and CT5 (reverse: 5’-ATT TAC GTG AGC AGC TCT CTC AT-3’). 11 Primary PCR was performed in a final volume of 25 µl consisting of 3 µl of the DNA template, 12.5 µl Master Mix 2X (Promega, USA), 0.5 μL of each primer (0.2 μM), and 8.5 μL of deionized water. The amplification conditions for the first round PCR were as follows: 94°C for 5 min, 10 cycles of 95°C for 1 min, 60°C for 1 min, 72°C for 1.5 min, 20 cycles of 95°C for 1 min, 55°C for 1 min, 72°C for 1.5 min, and a final extension at 72°C for 10 min. In the next stage, 2 µl of the first round PCR was added to the second round PCR that contained primer PCTM3 (forward: 5’- TCC TTG CAA GCT CTG CCT GTG GGG AAT CCT-3’) and the previous primer CT5 (reverse), 11 using the same conditions as the first round PCR. PCRs were performed using the Thermo Mastercycler gradient cycler (Thermo Scientific, USA). After amplification, the PCR products were analyzed on 1.2% agarose gels containing RedSafe™ Nucleic Acid Staining Solution (iNtRON, Korea) in 1X TBE buffer for about 1.5 h at 90 V and visualized with UV light (UVP, Canada). The 100 bp DNA ladder (Cleaver Scientific, England) was included in each electrophoresis to determine PCR product size.
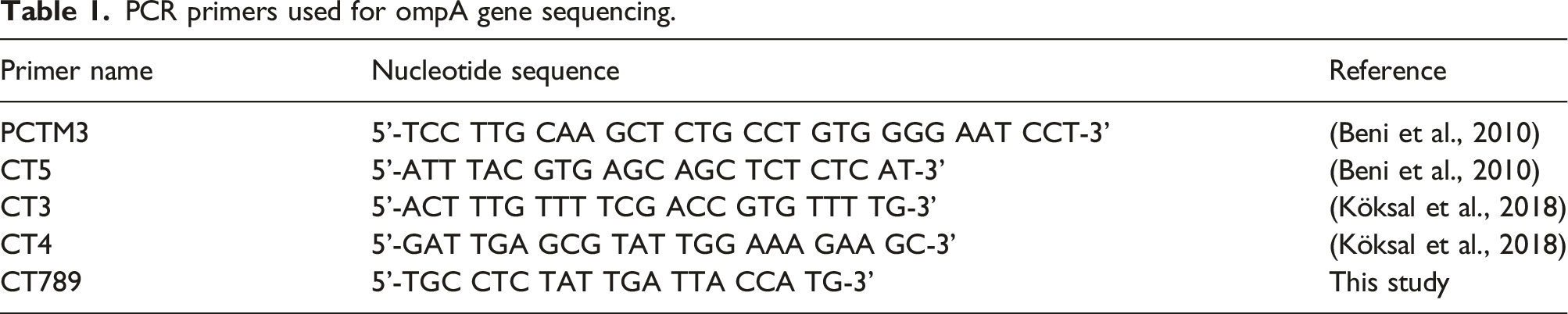
Outer membrane protein A gene sequencing
PCR primers used for ompA gene sequencing.
Statistical analysis
The data obtained in the study were analysed using IBM SPSS Statistics for Windows, version 20.0 (IBM Corp., Armonk, NY, USA). Statistical analysis was performed by student T-test. Univariate analysis of the relationship of prevalence with risk factors (age group, clinical characteristics, and disease history) was conducted. Factors that had significance of p-value <.05 in the univariate analysis were then entered into a multiple logistic regression analysis. If the p-value was lower than 0.05, the observed results were considered statistically significant. The sequences of the ompA gene of CT were analyzed independently by comparing them with the available data in the GenBank database, using the BLAST tool (https://blast.ncbi.nlm.nih.gov/Blast.cgi).
Ethics approval and consent to participate
This study was approved by the Ethics Review Board of the National Hospital of Obstetrics and Gynecology (Ha Noi, Vietnam) in March 2020 (ethics code: 221/QĐ-PTSW) and was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments.
Results
Chlamydia trachomatis prevalence
Seven hundred and sixty-one endocervical samples were collected from the cervix of infertile women, including 382 cases of primary infertility and 379 cases of secondary infertility. Out of the 761 samples, 119 (15.6%) were found to be positive for CT and 642 were negative. None of the endocervical samples were positive for Neisseria gonorrhoae. Infertile patients had a mean age of 29.29 ± 5.95 (range, 19–52 years).
Factors associated with genital C. trachomatis
Patient characteristics, prevalence and related factors of CT in endocervical samples.
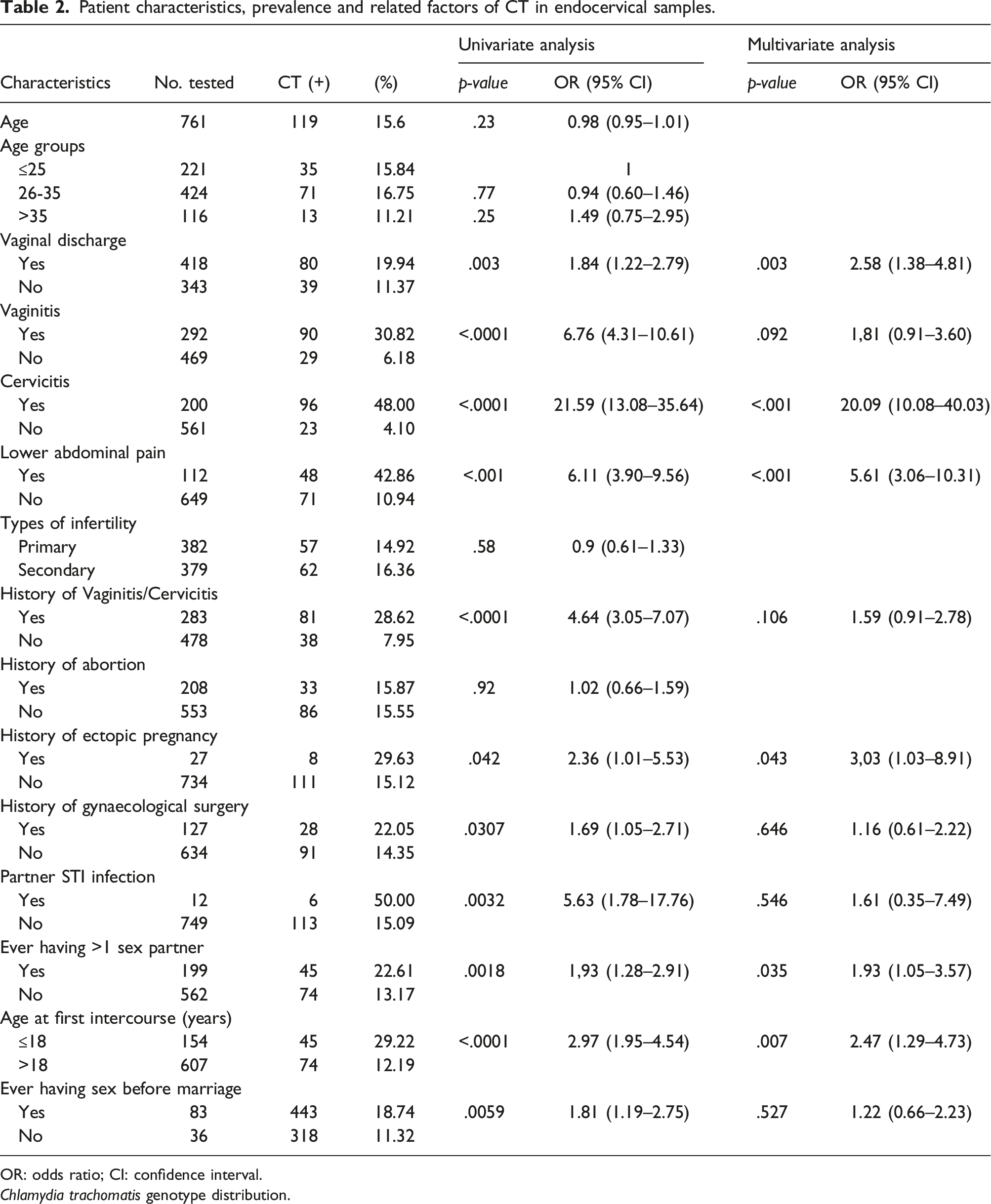
OR: odds ratio; CI: confidence interval.
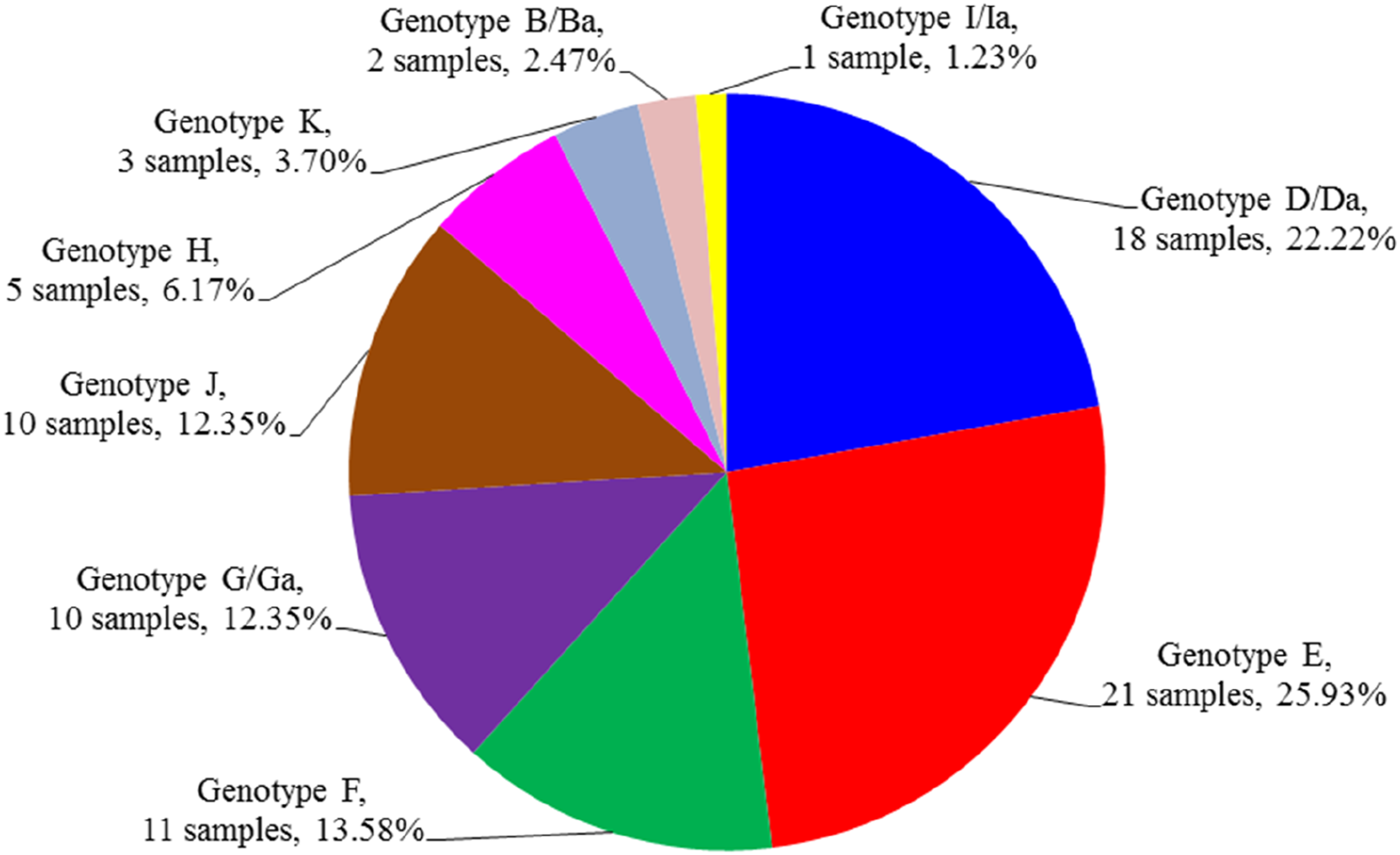
Chlamydia trachomatis genotype distribution.
Of the 119 positive clinical samples, 90 strains were randomly subjected to semi nested-PCR for ompA gene amplification and subsequent nucleotide sequences (Figure 1). The results showed that nine samples did not yield high-quality sequences, so they were excluded from further analysis. Eighty-one isolates were successfully sequenced and analyzed to identify the CT genotypes. The obtained sequences were clear and indicated no signs of mixed infection. According to the ompA gene analyzing results, nine genotypes were identified, the most common genotype was E (n = 21, 25.93%), followed by D/Da (n = 18, 22.23%), F (n = 11, 13.58%), G/Ga (n = 10, 12.35%), J (n = 10, 12.35%), H (n = 5, 6.17%), K (n = 3, 3.70%), B/Ba (n = 2, 2.47%) and I/Ia (n = 1, 1.23%). However, genotypes A, C, and L1-L3 were not found. The genotype distribution and frequency are shown in Figure 2. Electrophoretic separation of second-round PCR products for the detection of the ompA gene of C. trachomatis in endocervical swab specimens. Lanes 1-3 (isolates 417806, 410776, and 355710): clinical samples; lane 4: DNA Ladder 100 bp Standard; lane 5: positive control; lane 6: negative control. The distribution of CT genotypes among infertility women.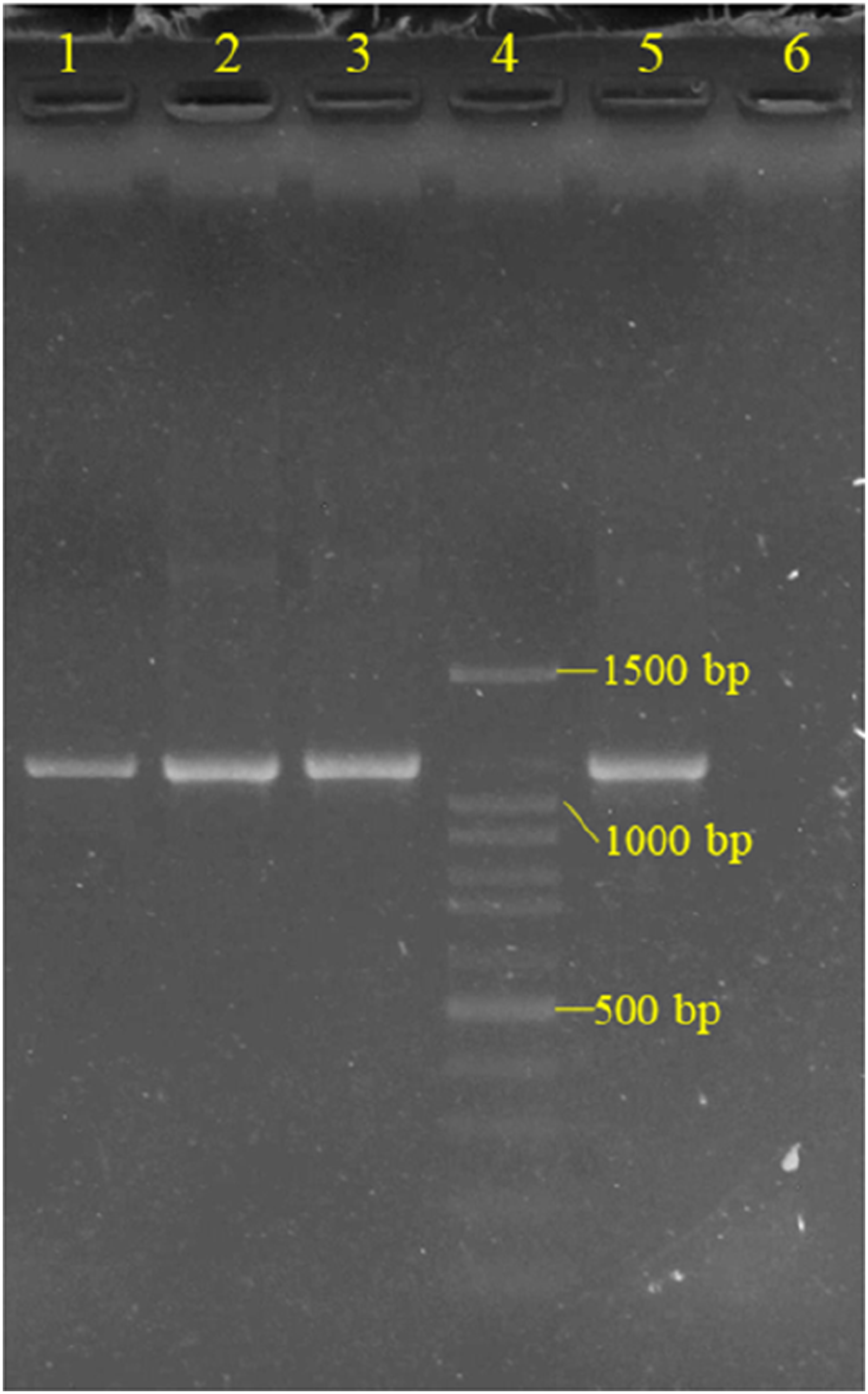
Twenty-two sequences of the ompA gene were also deposited in GenBank (USA) under accession numbers MZ407931 to MZ407947 and OP899639 to OP899643. BLAST results showed that the ompA sequences in this study indicated high similarity values, ranging from 99.10 to 100% when compared to those from the Genbank. Genotypes E, F, and G/Ga were highly preserved, showing 100% similar to alternative reference sequences, whereas ompA sequences of genotypes B/Ba, D/Da, H, I/Ia, J and K displayed from one to 10 nucleotide substitutions.
Associations between C. trachomatis genotypes and clinical manifestations
Associations of C. trachomatis genotypes with clinical characteristics in the study population.
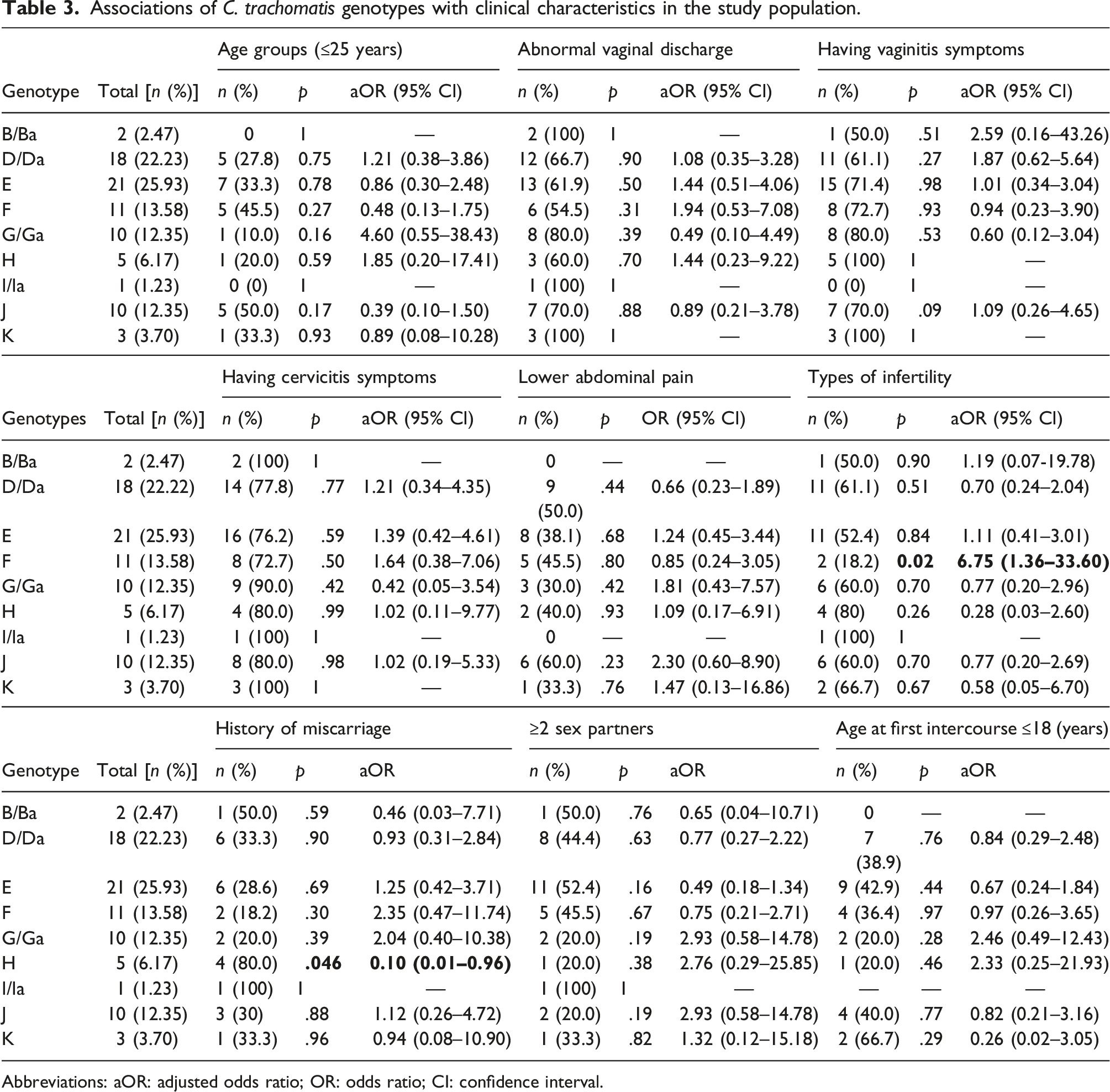
Abbreviations: aOR: adjusted odds ratio; OR: odds ratio; CI: confidence interval.
Discussion
CT is the most common bacterial agent in sexually transmitted infections worldwide. 16 The results from studies in several countries show that the prevalence of CT differs in different populations and depends on diagnostic methods.16,17 According to the World Health Organization, in 2020, approximately 128 million new CT cases were reported globally,18,19 but this issue has been reported in a very limited fashion in Vietnam, especially the genotypes of CT. The results from different studies worldwide show that distribution of CT genotypes varies between countries, depending on the region, gender, ethnicity, and sexual behaviors. 8 The findings regarding the prevalence of CT infection and the distribution of CT genotypes are necessary to help us understand the clinical and epidemiological characteristics and to adjust the guidelines for the diagnosis and management of CT infection.11,20
The available data from different regions of the world indicated that the prevalence rate of CT among infertile women ranged from from 2.0% to 68.0%.15,17,21,22 In this study, the CT infection rate among subfertile women in Vietnam was found to be 15.6%. The results of our investigation were similar to those of previous studies in Uttar Pradesh, India (15.7%) and Saudi Arabia (15.0%).15,23 Lower CT prevalence was observed in China (5.9%), Turkey (2.15%), Rwanda (3.3%), Jordan (3.9%), Argentina (5.3%), and Malaysia (7.3%).21,24–28 The higher prevalence rates were reported in Palestine (20.2%), Nigeria (28.0%), Netherlands (29.5%), Italy (31.8%), Iran (32.0%), and Tanzania (36.21%).29–34 Studies from New Delhi, India observed also a higher prevalence of CT among infertile women than in current research (28.1% vs 15.6%). 35 The prevalence rate of CT among subfertile women in Vietnam in our study was within the reported range. The reasons for these varieties are due to the prevalence of CT depending on gender, social demographics, sexual behavior characteristics, different regions of the understudy population, the method for CT identification, etc.8,15,17,21 Previously, no information about the prevalence of CT among subfertile women was available in Vietnam. Our results, especially the genotypic distribution, are probably the first research of CT infections in Vietnamese subfertile women. Consequently, more investigations are required to determine the specific rate of CT colonization in Vietnam.
The age of the infertile women included in this study ranged from 19 to 52 years old. The results of this study showed that the prevalence of CT is higher in young women, with the prevalence among infertile women under 35 accounting for 16.43%. Our findings are in agreement with previous studies.17,23,26 This suggests that younger age is an important risk factor for CT infection and confirms that these individuals as a primary determinant for selective CT screening programs.15,17 The US Preventive Services Task Force also recommended that all sexually active women younger than 25 years or older with risk factors for infection should be screened for chlamydia every year. 36 In this study, the prevalence of chlamydial infection in the primary infertility group was lower than in the secondary subfertility group (14.92% vs 16.36%), but the difference was not statistically significant. The findings of our study were similar to those of previous investigations in Aligarh, India, and in Amman, Jordan.26,35 In contrast, significant differences have been observed between the two groups in New Delhi, India, and in Jazan city, Saudi Arabia.15,23 This information indicates that the impact of subfertility types on the prevalence of CT infection is still indistinct. However, the prevalence of CT infection is higher in subfertile women compared with that in the general population.23,26,37 Unfortunately, in this study, we did not compare the proportion of chlamydial infection in infertile women and the general population. Therefore, more studies are needed to analyze the relationship between CT infection and infertility in Vietnam.
CT infection in women is difficult to diagnose because approximately 70% of infections are asymptomatic.15,16,38 However, in this study, a significantly high prevalence of CT infection was observed among women with abnormal vaginal discharge and lower abdominal pain. Similar results were seen in studies in India.15,35 Thus, in addition to screening for chlamydial infection in young adult women, CT screening in symptomatic women should also be performed.
To our knowledge, this is the first study on the genotype distribution of CT infections in Vietnam. In this study, nine CT genotypes were identified, including E, D/Da, F, G/Ga, J, H, K, B/Ba, and I/Ia. Among those, genotype E was the most prevalent, followed by D/Da and F, while genotypes H, K, B/Ba and I/Ia had a lower percentage. Notably, genotypes G/Ga and J have a relatively high prevalence (12.35%). The same genotypes E, D, and F were found in India (47.8% E, 32.2% D, and 20% F) in infertile women, Argentina (46.9% E, 21.0% D, and 16.1% F) in symptomatic patients, and Taiwan (22% E, 19% D/Da, and 16% F) in patients with genital chlamydia infection on examination.15,39,40 In many countries, these three genotypes have also been reported more commonly in urogenital infections.38,41 However, our findings were slightly different from reports from some countries. Genotypes D, F, and K are the most prevalent among STD subjects in Thailand, while genotypes F predominate in Mexico and Brazil.16,38,42 Genotypes D and J were the most common among isolates from Guangxi and Guangzhou, China, accounting for 29.69% and 28.6%, respectively.8,43 The reasons for such changes in the distribution of CT genotypes might be due to different geographical locations, characteristics of the study population, and the duration of these studies.15,40 Thus, additional investigations should be carried out to clarify the prevalence and genotypes of CT in Vietnam.
The results from current study showed that clinical characteristics, including age groups, abnormal vaginal discharge, vaginitis, cervicitis, lower abdominal pain, having more than two sex partners, and age at first intercourse (less than 18 years), were not associated with any CT genotypes. The studies have found an association of CT infection between genotype F and types of infertility, and genotype H and a history of miscarriage among infertile women. The results of current study are in accordance with some previous studies. In a study in Shenzhen, China, genotypes D, H, and K of CT was observed to be related to gravidity, abnormal cervical cytology, and contraception, respectively. 44 In other study that also performed in China, association between genotype G of CT and abnormal vaginal discharge was observed. 43 The data from Jalisco, Mexico indicated that genotype D was associated with infection during previous pregnancies, and genotype E was related to green vaginal discharge and having more than two sex partners. 45 In a similar study performed at India, genotype D of CT was significantly related to age 30-34 years (p = .02). 15 The reasons for such varying association between CT genotype and clinical characteristics may be due to differences in the characteristics of the subjects being analyzed, mixed-genotype infections of CT, and variation in virulence between genotypes.43,46,47
Conclusion
The results of the current study showed that the prevalence of CT infection in infertile women in Vietnam is 15.6%. Risk factors for CT infections among infertile women, obtained by multivariate analysis, included abnormal vaginal discharge, cervicitis, lower abdominal pain, a history of ectopic pregnancy, having more than one sex partner, and age at first intercourse less than 18 years. Of nine genotypes found, E (25.93%) was the most common genotype, followed by genotypes D/Da (22.22%) and F (13.58%). Genotype F was related to types of infertility, and genotype H was associated with a history of miscarriage. The current findings suggest that routine screening is essential for early detection and the implementation of infection control measures.
Footnotes
Acknowledgements
We gratefully thank all the staff of the National Hospital of Obstetrics and Gynecology (Hanoi, Vietnam) who kindly contributed to patient handling and sample preparation. We are also indebted to the Department of Medical Parasitology (Vietnam Military Medical University) for providing the equipment used for the molecular analysis of the samples.
Author contributions
NH, VVD, TQP, and DNA designed the study; NH, VVD collected the samples and patient enrolment information; NLV, NTNQ, and DNA identified species and genotypes of the responsible agent. NH, HDC, and DNA carried out the statistical analysis and prepared Tables 1–![]() . NH, HTY, DNA, and VVD drafted the manuscript. HTY, TQP and NTNQ revised the manuscript. All authors read and approved the final manuscript.
. NH, HTY, DNA, and VVD drafted the manuscript. HTY, TQP and NTNQ revised the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Hospital of Obstetrics and Gynecology, Hanoi city, Vietnam (Grant no. 221/2020/PTSW to NH).
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.