
Abstract
Background
We sought to determine the prevalence of sickle cell trait (SCT) and apolipoprotein-1 (APOL1) risk variants in people living with HIV (PLWH) in Nigeria, and to establish if SCT and APOL1 high-risk status correlate with estimated glomerular filtration rate (eGFR) and/or prevalent chronic kidney disease (CKD).
Methods
Baseline demographic and clinical data were obtained during three cross-sectional visits. CKD was defined as having an eGFR<60 mL/min/1.73 m2. We collected urine specimens to determine urine albumin-creatine ratio and blood samples for sickle cell genotyping, APOL1 testing, and for creatinine/cystatin C assessment. The associations between SCT, APOL1 genotype, and eGFR/CKD stages/CKD were investigated using linear/ordinal logistic/logistic regression models, respectively.
Results
Of 2443 participants, 599 (24.5%) had SCT, and 2291 (93.8%) had a low-risk APOL1 genotype (0 or 1 risk variant), while 152 (6.2%) had high-risk genotype (2 allele copies). In total, 108 participants (4.4%) were diagnosed with CKD. In adjusted analyses, SCT was associated with lower eGFR (adjusted mean difference [aMD]= −2.33, 95% CI -4.25, −0.42), but not with worse CKD stages, or increased odds of developing CKD. Participants with the APOL1 high risk genotype were more likely to have lower eGFR (aMD= −5.45, 95% CI -8.87, −2.03), to develop CKD (adjusted odds ratio [aOR] = 1.97, 95% CI: 1.03, 3.75), and to be in worse CKD stages (aOR = 1.60, 95% CI: 1.12, 2.29) than those with the low-risk genotype. There was no evidence of interaction between SCT and APOL1 genotype on eGFR or risk of CKD.
Conclusion
Our findings highlight the multifaceted interplay of genetic factors in the pathogenesis of CKD in PLWH.
Introduction
Combination antiretroviral therapy (ART) has significantly decreased premature mortality and morbidity associated with HIV,1,2 yet the incidence of certain non-communicable diseases (NCDs), such as HIV-associated kidney disease, continues to rise among people living with HIV (PLWH). Globally, HIV-associated kidney disease remains a problem, particularly among persons of African descent, where host genetic factors place some individuals at considerably higher risk for development of non-diabetic kidney disease. At least three to four times as many people have chronic kidney disease (CKD) in sub-Saharan Africa (SSA) when compared to persons residing in high income settings.3,4 Chronic kidney disease (CKD) can be defined as the presence of severely increased albuminuria (urine albumin/creatinine ratio [uACR] >300 mg/g) and/or reduced estimated glomerular filtration rate (eGFR<60 mL/min/1.73m2). In SSA, the prevalence of CKD among ART-naive PLWH ranges from 6% to 48%, with the highest prevalence being recorded in Nigeria. 5 There is a dearth of studies on the causes, development, and prevention of CKD in SSA, despite evidence of its high prevalence and effects. This is particularly true for ART-treated PLWH, who have a higher chance of developing kidney dysfunction, as well as other long-term end-organ complications.6–8
A significant risk factor for the onset of progressive CKD is homozygosity (or compound heterozygosity) for Apolipoprotein 1 (APOL1) genetic variations that offer protection against Trypanosoma brucei infection. According to estimates, APOL1 high-risk genotypes may be responsible for one-third of CKD cases among African ancestry persons living with HIV. 9 Kopp et al. have shown that the APOL1 high-risk genotype confers significant risk for focal segmental glomerulosclerosis (FSGS), HIV-associated nephropathy (HIVAN), and hypertension-attributed end-stage kidney disease. 10 The APOL1 risk allele frequency is highest in West Africa, particularly in Nigeria, and among persons of Igbo and Yoruba descent.11–13 Approximately 50% of people with high-risk genotypes who are HIV-positive and not receiving ART will develop CKD.14,15 Similar to APOL1 high-risk individuals who are HIV-negative, APOL1 high risk individuals living with HIV continue to have a significantly higher risk for CKD, even when HIV replication is controlled. 16
Sickle cell disease (SCD) is caused by a hereditary variation of the beta-globin gene called sickle hemoglobin (HbS), which protects against malaria.17–20 Proteinuria, hematuria, and urinary concentration defects are the hallmarks of sickle cell nephropathy, 21 and kidney failure may occur after a protracted period of glomerular hyperfiltration. 22 Sickle cell trait (SCT) (HbAS) carriers, i.e., those with one sickle hemoglobin gene, have a normal life expectancy and, despite the possibility of occasional sickle cell nephropathy symptoms, rarely experience sickle cell crises. Whereas two studies from SSA were unable to confirm a relationship between SCT and CKD,23,24 investigations in African Americans have revealed associations between SCT and CKD, albuminuria, and a more rapid fall in eGFR.25,26 Very little research has been conducted among PLWH to investigate the potential connection between SCT and kidney illness. Hung et al. 27 described SCT as a potential risk factor for CKD and albuminuria among people of African ancestry living with HIV in the UK, but these results need further confirmation, especially among communities in SSA.
The purpose of this study is to determine the prevalence of SCT and APOL1 kidney risk variants in a large cross-sectional sample of ART-treated PLWH in northern Nigeria and to establish if this population’s SCT and APOL1 high-risk status correlate with eGFR and/or prevalent CKD. Findings from this study could improve our understanding of the links between SCT, APOL1 genotype status, and eGFR as predictors of kidney function, in addition to informing the care of patients living with both conditions in Nigeria.
Methods
Setting
This study included data collected at the S.S. Wali HIV clinic of Aminu Kano Teaching Hospital (AKTH), which is supported by the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR). Kano is Nigeria’s most populous state and has an estimated HIV prevalence of 1.3%. 28 The S.S. Wali HIV clinic provides comprehensive care to more than 10,000 PLWH and is the research site for clinical trials supported by the U.S. National Institutes of Health (NIH) and the Bill and Melinda Gates Foundation. AKTH has a long-standing research and training partnership with Vanderbilt University Medical Center.
Study design/participants
This is a cross-sectional study performed among eligible participants who visited AKTH for treatment. Participants in the study had to meet the following inclusion criteria: (i) be HIV-positive (based on medical chart review with documented HIV ELISA results); (ii) be on ART for at least 6 months; (iii) be between the ages of 18 and 70 years; and (iv) able and willing to provide written informed consent. For this study, we included data from participants with sickle cell and APOL1 genotype and known eGFR measurements. Data collection for the study occurred between January 2019 and March 2021.
Study procedures
The complete study protocol has been described elsewhere.13,29 Briefly, consented subjects participated in three cross-sectional study visits. Baseline demographic and clinical data were obtained at the initial research visit (time zero). Each participant provided one first-morning voided urine specimen on the second and third study visits for the determination of urine albumin-creatine ratio (uACR), and a blood sample on the third visit for APOL1 and HbS genotyping and for measuring serum creatinine and cystatin C (CyC), which was then used to compute eGFR using the CKD-EPI-Cr-CyC equation.30,31 At each scheduled appointment, seated blood pressure was assessed using analog sphygmomanometers following a minimum of 5 minutes of rest.
The HemoCue Albumin 201 point of care diagnostic kit (Angelholm, Sweden) was used for urine albumin estimation. The Hitachi Cobas C 311 (Roche Diagnostics, Mannheim, Germany) automated analyzer system was used to estimate serum creatinine and cystatin C. Analytic quality was assured by testing precinorm and precipath quality control samples with each assay run. Quality control values that fell outside the established laboratory range (>± 2 SD) were rejected. The analysis was repeated following corrective measures, such as temperature checks, onboard reagent stability checks, and equipment troubleshooting. Internal QA/QC for cystatin was performed as per manufacturer’s instructions, namely, utilizing standard control materials (cystatin C Control Set Gen (2) manufactured by Roche Diagnostics to test each analytical run or batch of specimens.
For APOL1 and HbS genetic analysis, the plasma buffy coat was isolated, and DNA was extracted using Qiagen extraction kits (Hilden, Germany). Genetic testing and genotyping were done using ThermoFisher Scientific TaqMan custom assays (Waltham, MA) targeting the three chromosome 22 APOL1 variants (rs73885319 [G1], rs60910145 [G1], and rs 71785313 [G2]) associated with CKD, including HIV-associated kidney disease. APOL1 risk alleles were defined by the presence of G1 and G2 haplotypes. We inferred APOL1 genotype from the number of risk alleles: individuals were classified as carrying two risk genotypes (G1/G1, G1/G2, or G2/G2), 1 risk genotype (G0/G1 or G0/G2), or no risk alleles (G0/G0). Each variant was tested for deviations from Hardy-Weinberg equilibrium among control subjects using the c2 goodness-of-fit test. All genetic analyses were performed at the Basic Research Laboratory, Frederick National Laboratory for Cancer Research, Frederick, Maryland; and all standard QC/QA procedures were adhered to for genetics testing.
Statistical considerations
Descriptive statistics were summarized overall and by SCT status as median (interquartile range [IQR]) for continuous variables and frequency (percent) for categorical variables. Chronic kidney disease (CKD) was defined as having an eGFR<60 mL/min/1.73 m2. The severity of CKD was also classified into three stages using established Kidney Disease Improving Global Outcomes (KDIGO) criteria, based on eGFR levels: stage 1 with eGFR
Results
Baseline cohort characteristics
A total of 2500 participants met the inclusion criteria for the original study. Of these, a total of 2443 participants (97.7%) were included in this study. Figure 1 details the reasons for exclusion: 22 participants were missing sickle cell genotype information, two participants had sickle cell disease, and 33 were missing APOL1 genotype information. Flowchart showing recruitment of study participants, Kano, Nigeria.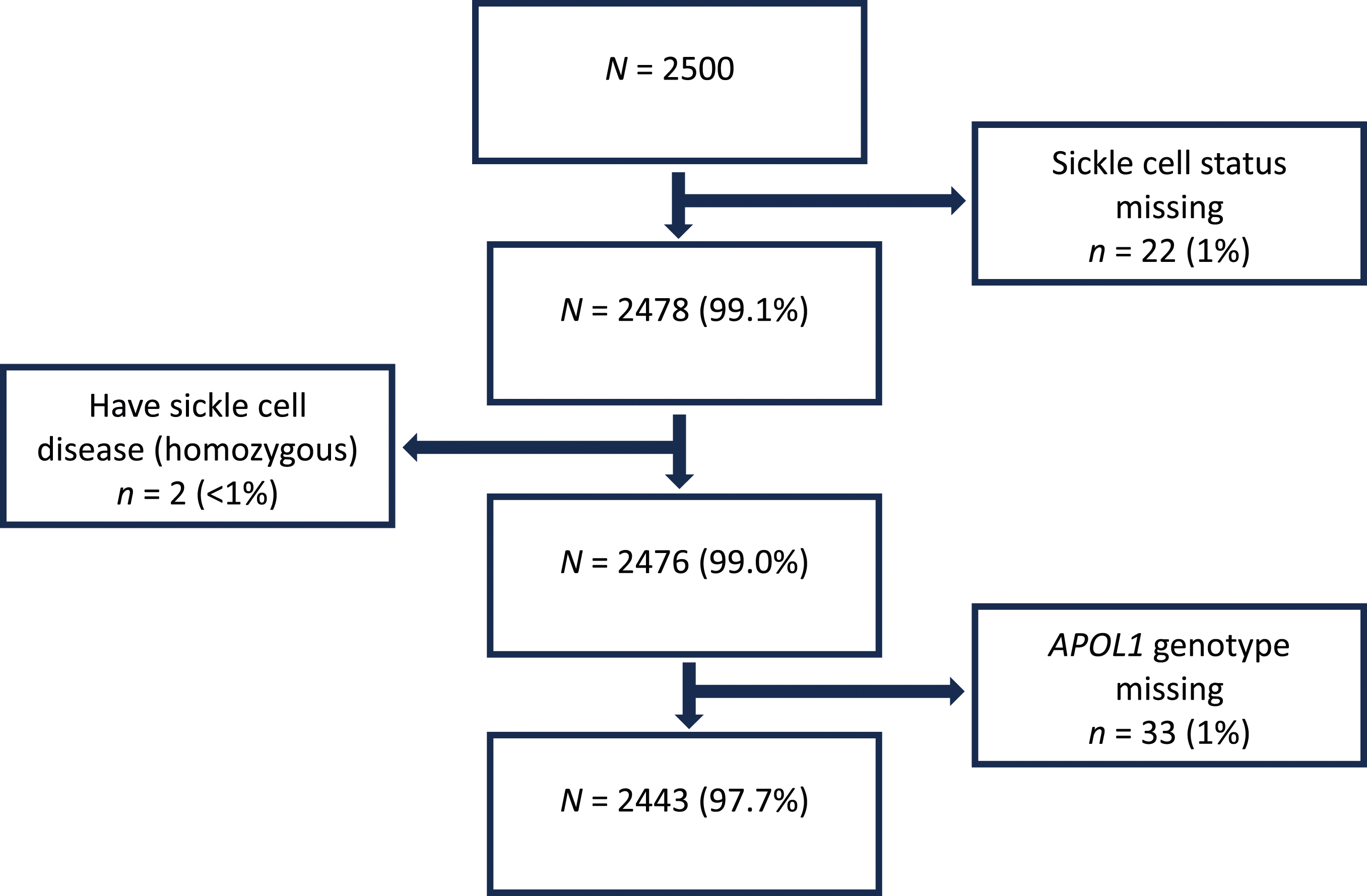
Characteristics of study participants by sickle cell disease trait status, Kano, Nigeria.
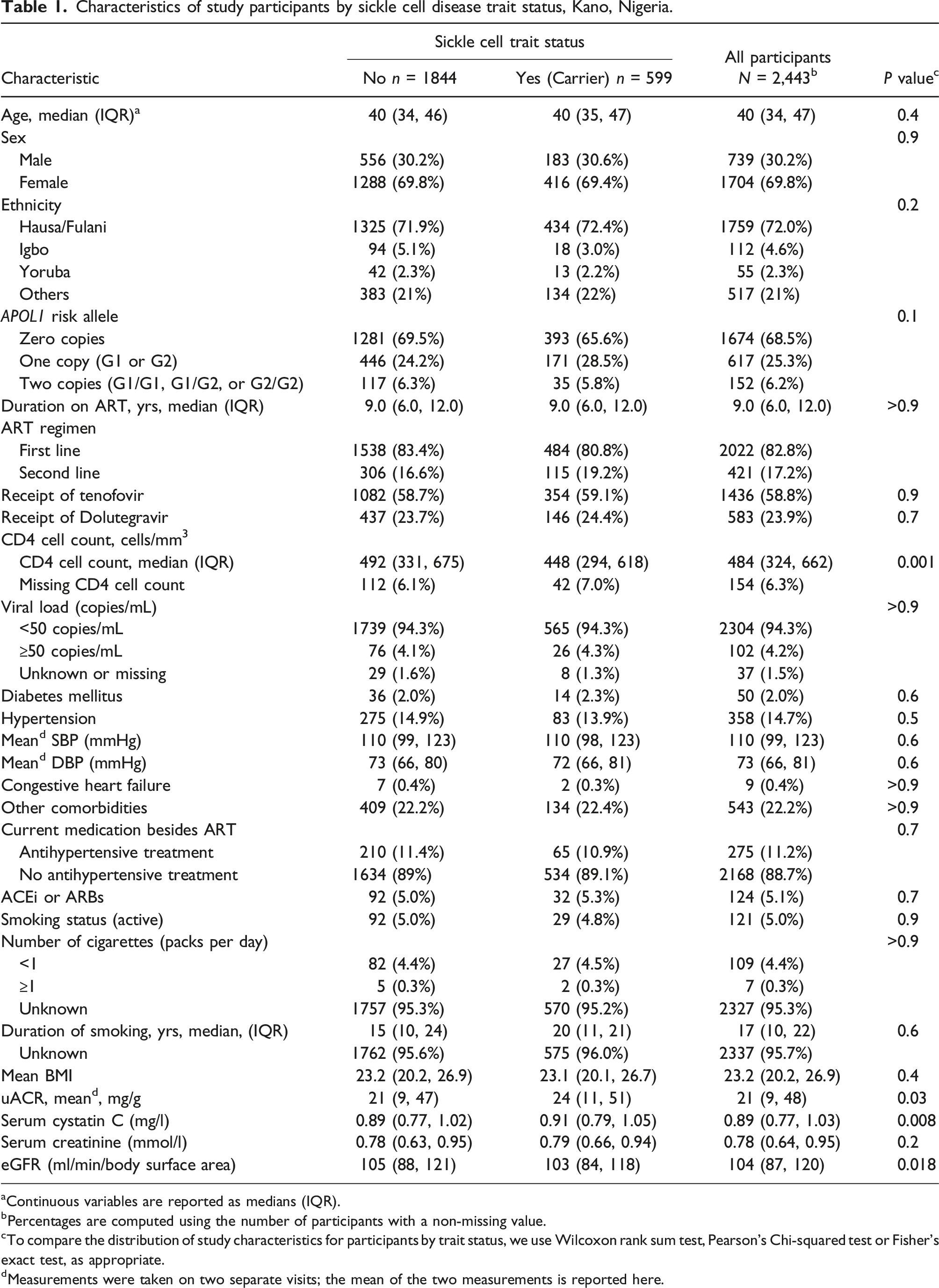
aContinuous variables are reported as medians (IQR).
bPercentages are computed using the number of participants with a non-missing value.
cTo compare the distribution of study characteristics for participants by trait status, we use Wilcoxon rank sum test, Pearson’s Chi-squared test or Fisher’s exact test, as appropriate.
dMeasurements were taken on two separate visits; the mean of the two measurements is reported here.
Sickle cell, risk alleles, and kidney parameters
Adjusted analyses examining variables associated with eGFR and chronic kidney disease (CKD; eGFR<60 mL/min per 1.73 m2).
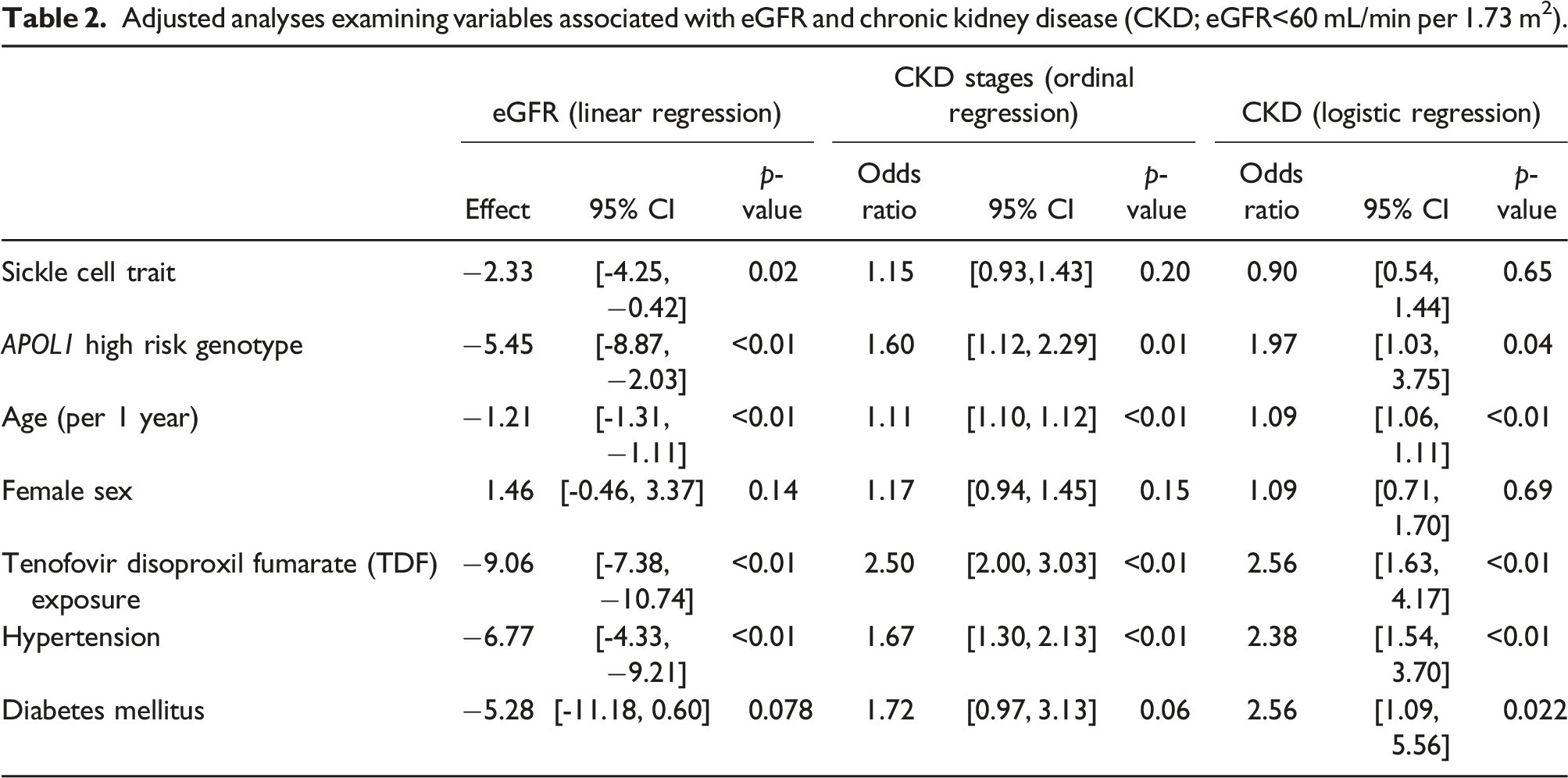
When eGFR was categorized into the three stages of kidney disease, participants with SCT had 17% higher odds of being in a higher (more severe) CKD category compared to those without SCT, although this finding was not statistically significant (OR = 1.17, 95% CI [0.96, 1.43]; p = .12). However, the association between APOL1 high risk genotype and being in a worse CKD stage was statistically significant; participants with the high risk APOL1 genotype had 1.69 times higher odds of being in a more severe CKD category compared to those with the low risk APOL1 genotype (OR = 1.69, 95% CI [1.20, 2.38], p = .002). In an adjusted model that included age, sex, current TDF use, hypertension, diabetes mellitus status, and the two genetic variables, the SCT and APOL1 genotype odds ratios were similar to those in the unadjusted model (Table 2). Specifically, in the adjusted model participants with SCT had higher, but not statistically significant, odds of being in a more severe CKD category compared to those without SCT (OR = 1.15, 95% CI [0.93, 1.43], p = .20) while those with the high risk APOL1 genotype had 60% higher odds of being in a more severe CKD category than those with the low-risk APOL1 genotype (OR = 1.60, 95% CI [1.12, 2.29], p = .01). SCT and APOL1 genotype showed no evidence of interaction on the association with stage of kidney disease (p = .98). Results were similar in secondary analyses that also included participant ethnicity as a covariate.
In models that dichotomized eGFR as CKD present (eGFR<60 mL/min/1.73 m2) or absent (eGFR≥60 mL/min/1.73 m2), there was no statistically significant association between SCT and CKD (OR = 0.92, 95% CI [0.58, 1.46], p = .74). In contrast, APOL1 high risk alleles (recessive model) were associated with higher risk of CKD (OR = 2.04; 95% CI [1.01, 3.76]; p = .032). There was no evidence of an interaction between sickle cell trait and APOL1 genotype on risk of CKD (p = .39). Associations were similar after adjusting for age, sex, current TDF use, hypertension, and diabetes status (Table 2). In adjusted analyses, we failed to detect a statistically significant association between SCT and risk of CKD, (aOR = 0.90; 95% CI [0.55, 1.42], p = .65). Having the APOL1 high-risk genotype was associated with a higher risk of CKD (aOR = 2.16; 95% CI [1.13, 3.82]; p = .013). Results were similar in secondary analyses that also included participant ethnicity as a covariate.
In adjusted analyses, older age, use of TDF, hypertension, and diabetes were associated with lower eGFR, higher odds of worse CKD stage, and higher odds of CKD (Table 2). For every 1-year increase in age, there was a decline of 1.21 units in eGFR, 1.11 times higher odds of being in more advanced CKD stages, and 1.09 times increased odds of having CKD. Tenofovir use was similarly associated with eGFR decline (adjusted mean difference = −9.06, 95% CI [-7.38, −10.74]; p < .01), higher odds of being in more advanced CKD stages (OR = 2.5, 95% CI [2.00-3.03], p < .01), and increased likelihood of developing CKD (OR = 2.5, 95% CI [1.63-4.17], p < .01). Increased odds of developing CKD were seen with hypertension (OR = 2.38, 95% CI [1.54-3.70], p < .01) and diabetes mellitus (OR = 2.56, 95% CI [1.09, 5.56], p = .022). There was no evidence of an association between participant sex and eGFR, higher category of CKD, or occurrence of CKD. Sensitivity analysis failed to reveal an association between ethnicity and eGFR, CKD stage, or the development of CKD. Secondary analysis yielded comparable results when participant viral load, CD4 count, and ACE-ARB were added as covariates (Table S1). Similarly, the multiple imputation adjusted model that included these covariates produced consistent results (Table S2).
Discussion
In this large cross-sectional study of virologically suppressed ART-experienced adults living with HIV in Nigeria, we found that SCT was associated with reduced eGFR but not with the development of CKD or CKD stage. We also found that consistent with prior studies,10,32–35 possession of the high risk APOL1 genotype was consistently associated with decreased eGFR, higher CKD stages, and increased odds of developing CKD. Our findings regarding well-established traditional risk factors for CKD, such as age, hypertension, diabetes mellitus, and antiretroviral therapy (TDF use), align with prior reports.36–38 These results underscore the complex interplay of genetic and non-genetic (lifestyle/environmental) factors in shaping kidney health trajectories in persons living with HIV.
Sickle cell trait is mostly a benign condition, but not always. Persons with SCT may on occasion present with manifestations of kidney disease, such as impaired urinary concentrating ability, hematuria, and papillary necrosis.21,22,39,40 We found the association of SCT and kidney function in our study population to be nuanced, showing significance in the linear regression model for eGFR but not in the ordinal and logistic regression models for CKD stages and occurrence of CKD, respectively. This finding is not entirely unexpected, as the relationship of SCT to CKD is not firmly established. Whereas some studies suggest a higher risk of CKD and/or lower eGFR in persons with SCT compared to those without SCT,25,41,42 others did not.23,24 Reports of faster decline in eGFR among persons with SCT, consistent with our study, have also been reported.25,42 However, unlike our study, most reports did not account for participants’ HIV status. An exception is a cross-sectional study that included PLWH of African ancestry in England, 27 which found SCT to be associated with reduced eGFR (<60 mL/min per 1.73 m2 and <90 mL/min per 1.73 m2) and albuminuria. The discrepancy in findings regarding the link between SCT and impaired kidney function across studies could be attributed to differences in ascertainment of outcome measures (eGFR, CKD), study design and power, participant demographics, genetic diversity, and the distribution of comorbid conditions with potential kidney effects (e.g., hypertension, diabetes mellitus, obesity), among others. 41
We were unable to discern an interaction effect between APOL1 genotype and SCT on the occurrence of CKD, suggesting that the effects of these genetic traits on kidney function likely act independently within our cohort. Our finding agrees with two large population-based studies of self-reported African Americans,25,26 but contrasts with a recent report from the Democratic Republic of Congo, 41 where APOL1 high risk status and SCT were found to be synergistically associated with lower GFR (test for interaction, p = .012). Unlike in our study, the participants in all three reports were, however, not restricted to persons with HIV. Further research to confirm or refute these findings in PLWH is warranted.
The strengths of this study include the large sample size, which improves the precision of our results, the recruitment of participants from a diverse clinical cohort of ART-treated virally suppressed adults, the use of standardized measures to ascertain eGFR, and the detailed APOL1 genotyping data from an indigenous African population. In addition, to our knowledge, this is the first description of the association of SCT and APOL1 with adverse kidney function in a large cohort of PLWH drawn from West Africa, a region with a significant prevalence of APOL1 high risk variants.
This study has limitations. The recruitment of participants from a single clinical site potentially limits the generalizability of our findings. We are also unable to draw definitive conclusions about causal associations due to the cross-sectional study design. The absence of detailed CKD pathologic diagnosis (kidney biopsy) represents additional limitations in the scope of our study. In addition, we may have residual confounding due to inability to include considerations of other conditions that could impact the likelihood of developing CKD, such as viral pathogens (e.g., Cytomegalovirus, hepatitis B or C), other endemic co-infections (e.g., parasitic infestations, tuberculosis), and environmental factors/exposures (NSAIDs, traditional medications, heavy metals, etc.). Regardless of these limitations, our study provides valuable insight into the complex relationship between genetic factors (specifically SCT and APOL1 genotype) and traditional risk factors (e.g., age, obesity, hypertension, diabetes), medication use (TDF), and their impact on kidney function and the risk of CKD in HIV-positive adults. The study also reaffirms the role of noncommunicable diseases (NCDs), such as hypertension and diabetes, on kidney outcomes in the context of HIV, underscoring the need for integration of HIV and NCD services, in addition to the development of comprehensive healthcare strategies addressing HIV and its associated comorbidities.43,44
Conclusion
In summary, we found SCT to be associated with a 2.33 mL/min/1.73 m2 lower eGFR, while the high-risk APOL1 genotype was associated with a 5.45 mL/min/1.73 m2 lower eGFR. Possession of the high risk APOL1 genotype was also consistently associated with worse CKD stages, and increased odds of developing CKD, as were other traditional risk factors for adverse kidney outcomes (age, TDF use, hypertension, and diabetes mellitus). These findings underline the importance of considering both genetic and non-genetic factors in assessing kidney health in this population and suggest potential avenues for further research. Longitudinal studies could provide insights into how these genetic and non-genetic factors influence the progression of kidney disease. Additional large well-designed studies are indicated to determine the need for APOL1 testing in persons living with HIV, especially in settings where sickle cell trait is prevalent.
Supplemental Material
Supplemental Material - Sickle cell trait, APOL1 risk allele status and chronic kidney disease among ART-experienced adults living with HIV in northern Nigeria
Supplemental Material for Sickle cell trait, APOL1 risk allele status and chronic kidney disease among ART-experienced adults living with HIV in northern Nigeria by Abdurrahman Abdulhamid, Bryan E. Shepherd, Usman J. Wudil, Chelsea Van Wyk, Faisal S. Dankishiya, Nafiu Hussaini, C. William Wester and Muktar H. Aliyu in International Journal of STD & AIDS
Footnotes
Acknowledgements
We acknowledge the assistance of members of the R3 and P-MICRO study teams.
Author contribution
A.A., B.E.S., C.W.W., and M.H.A. conceived the study; A.A., B.E.S., F.S.D., C.W.W., and M.H.A. designed the study protocol; F.S.D. and U.J.W. supervised data collection; A.A., B.E.S., N.H., and U.J.W. analysed the data. All authors participated in drafting the manuscript and critical review of the article; A.A., B.E.S., F.S.D., C.V., C.W.W., N.H., and M.H.A. finalized the manuscript; B.E.S. is the guarantor of the paper; all authors approve the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work is supported by the Fogarty International Center (FIC) of the U.S. National Institutes of Health, award numbers 1D43TW012268, 1D43TW011544 (with the National Institute on Alcohol Abuse and Alcoholism) and the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) R01DK127912. The findings and conclusions are those of the authors and do not necessarily represent the official position of the FIC, NIDDK, NIH, the Department of Health and Human Services, or the government of the United States of America.
Ethical statement
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request and in strict accordance with Nigeria data privacy regulations.
Supplemental Material
Supplemental material for this article is available online.