
Abstract
Objective
Studies in India and other low-income countries find an inconsistent association between mobility/migration and sexually transmitted infections (STIs) among men. This study comprehensively examined the association between mobility and STIs among men in India. It also assessed heterogeneous associations of mobility, alcohol consumption, and risky sexual behavior with STIs using interaction analysis.
Methods
We utilized a sample of 71,128 sexually active men aged 15-54 years from the 2019-21 National Family Health Survey-5. Binary logistic regression models were employed to study the associations.
Results
Among the study participants, 16% were mobile and away from home for a month or more in the last 12 months. Around 29% of men reported alcohol consumption and 6% had risky sexual behavior (sexual intercourse with a non-marital/non-cohabitating partner). Regression results suggest that mobility (AOR: 1.41, 95% CI: 1.29-1.55 [short-duration]; AOR: 1.95, 95% CI: 1.77-2.13 [long-duration]) and alcohol consumption (AOR: 1.32, 95% CI: 1.24-1.40) were significantly associated with an increased risk of STIs, even after controlling for socio-demographic covariates. Interaction analysis further reveals that mobile men who consumed alcohol and engaged in risky sexual behavior had a significantly higher likelihood of contracting an STI—twice as high in cases of short-duration mobility and three times higher in cases of long-duration mobility.
Conclusion
Our study indicates that both short and long-duration mobility are significantly associated with an increased risk of STIs among men. Alcohol consumption and risky sexual behavior further exacerbate the risk of STIs in mobile men. Initiatives for STI/HIV prevention among men must pay particular attention to temporary mobile men for both short and long durations.
Keywords
Introduction
The hidden epidemic of sexually transmitted infections (STIs) is a serious public health concern, primarily spread by unprotected sexual contact, including vaginal, anal, and oral sex. 1 Annually, an estimated 376 million new STI cases are reported worldwide. 2 STIs have a profound impact on the sexual and reproductive health of all genders. It is found to be significantly associated with an increased risk of reproductive tract morbidities, neonatal death, congenital deformities, and other adverse birth outcomes, as well as HIV transmission.3–6 In India, the burden of STI among men has substantially increased over the recent period. 7 The 2019-21 National Family Health Survey (NFHS-5) estimated that one in every nine adult men had symptoms of an STI in the last 12 months preceding the survey. 7 Infections are particularly prevalent among high-risk groups such as female sex workers, men who have sex with men, truckers, migrants, drug users and transgender people. 8
Previous studies conducted in India and other developing countries suggest a close connection between migration/mobility and the transmission of STIs, including HIV, due to the vulnerability of migrant and temporarily mobile males to risky sexual behaviors.9–14 These studies suggest that an embedded interplay of a complex set of socioeconomic, demographic, behavioral, and environmental factors underpin the association between migration/mobility and the adoption of high-risk sexual activities, leading to STIs. Studies have indicated that migrants and mobile population’s susceptibility to STIs and HIV/AIDS are heightened due to a number of factors, including their young age, never-married status or non-spousal residence, high poverty, peer pressure and norms, low perceived vulnerability of HIV/AIDS, substandard living environments with easy and close access to pornographic material, and limited access to healthcare.13,15–17 Studies have found a strong link between substance use (e.g., excessive drug abuse and alcohol consumption) and unsafe sexual activities, as well as the risk of STIs/HIV among migrant and mobile populations.18–22 Mobile population’s spatial instability puts them into frequent travel and transitions, making them vulnerable to high-risk social and sexual behaviors. They frequently visit commercial female sex workers and are more likely to engage in unprotected sexual acts. 23
Researchers have focused on the significance of migration and short-term mobility in the spread of the STI/HIV epidemic in India and other low and middle-income countries (LMICs). Many scholars have investigated the sexual practices of male migrants, particularly the poor migrants who reside in the slums of large cities. A previous study in India found that mobile youths (those who were away from their families) were more likely to have romantic relationships and initiate sex before marriage than those who were staying with their families. 24 Saggurti et al. (2008) 13 studied HIV risk behaviors of male migrant workers in India and found that compared to non-contractual employees, contracted labourers were much more likely to report alcohol consumption and HIV risk behaviors such as sex with sex workers, sex with non-spousal unpaid women, as well as had a higher risk of STI symptoms. In another study, Saggurti et al. (2009) 13 found that men with occupational mobility are significantly more likely to have one or more non-spousal sexual partners than those men who are not mobile. Using cross-sectional nationally representative data (NFHS-3, 2005-06) in India, Saggurti et al. (2012) 12 further showed that male migration and mobility increased the risk of HIV infection among married couples. In a case study of southwest India, Deering et al. (2008) 25 examined migration-related risk factors of HIV transmission and concluded that seasonal or short-term movement is a key factor in the HIV epidemic in India. The authors suggested understanding local sexual networks change for designing effective interventions in preventing HIV transmission. Similarly, a comparative cross-sectional study among two rural communities in Senegal and a rural community in Guinea-Bissau shows that short-term mobility appeared to be a risk factor for HIV infection among men in rural areas of West Africa. 26 A study among factory workers in Kolkata suggests that condom use was substantially low among both migrants and local workers. These workers, particularly migrants, also reported non-use of condoms while visiting female sex workers, putting them at risk of STI/HIV transmission. 27
Contrarily, a Lancet HIV study in rural South Africa found no statistically significant difference between the prevalence of HIV among migrants and non-migrants. Their findings imply that although migration can increase risky sexual activity, it does not always raise the risk of HIV infection, suggesting that migration was not a risk factor for HIV infection. 28 Another study on migration and HIV transmission in rural south India showed that migration does not appear to be a significant factor influencing married men’s sexual activity. 10 A study using a large-scale survey in India also reported no significant differences in sexual risk behaviors and STIs between migrant and non-migrant men. However, the study found temporary mobility, long-duration mobility in particular, had a profound impact on increasing the risk of having multiple sexual partners and STI infection. 17 Notwithstanding, some studies show a higher sexual risk behavior and STI/HIV infection among non-migrants as compared to migrants. A previous study by Saggurti et al. (2009) 13 in Mumbai, India, found that non-migrant men reported significantly more frequently having one or more non-spousal sex partners than migrant men. Moreover, a study among poor communities in Mumbai showed that non-migrants who are engaged in risky sexual behavior have a higher rate of HIV infection compared to migrant populations. 29 Therefore, the association between migration/mobility and STIs/HIV is not consistent and remains inconclusive.
Most of the prior studies focused on high-risk groups, which constrains us from generalizing the relationship between mobility and the risk of STIs for other population groups. Moreover, existing studies in India mainly focused on examining the role of migration in sexual risk behavior and transmission of STI/HIV infections. Only a few studies investigated the role of temporary mobile men, particularly long truck drivers, engaging in sexual risk behaviors and spreading STI/HIV infections.30–33 For example, a study among long truck drivers in rural India concluded that a large number of truck drivers are engaged in risky sexual activities with prostitutes. These truck drivers have found poor HIV/AIDS awareness and condom use and a high rate of HIV infection. 32 Similarly, a study in Tamil Nadu, India, found that mobility, such as frequent travelling of long truck drivers, plays a significant role in the transmission of HIV infection. 33
There is limited evidence available to understand the relationship between temporary mobility and STI infections in India using a large-scale national survey. To our knowledge, only one study investigated the association between mobility and STIs using a nationwide survey in India, and that was conducted more than a decade ago.
17
Moreover, this study was solely focused on examining the direct association between mobility/migration, STIs, and other risk behaviors. None of the previous studies explored the pathways in the association between mobility status and STIs through intersectional axes of alcohol use and risky sexual behavior. Given that mobile men often engage in alcohol consumption and risky sexual behavior, it is crucial to examine the multiple risk factors for STIs by employing these pathways in the analysis. Hence, considering the dearth of research and the importance of this topic in the Indian context, the present study attempts to examine the association between mobility (both short- and long-duration mobility) and STI infection among males in India using a nationally representative survey. Further, we aim to test whether alcohol use and risky sexual behavior play a significant role in shaping the association between mobility and STI. In this context, it is important to define mobility status. Mobility encompasses short- or long-term movements that do not necessarily involve permanent relocation. For example, temporarily mobile individuals may stay away from home for a few days or months but are expected to return to their permanent residence.
17
Men who are intermittently mobile, like construction workers, truck drivers, and salesmen, maintain a permanent residence, but their social networking, vulnerability, and exposure experiences may differ from those who are not mobile. Mobility patterns may have a profound impact on men’s sexual behavior and their risk of contracting STIs. We hypothesize that temporarily mobile men who move frequently and are away from their families for an extended period may engage in more high-risk behavior and are more susceptible to STI than those who are not mobile. Figure 1 shows the conceptual pathways between mobility, alcohol use, risky sexual behavior and STI infection. Pathways indicating linkages between mobility, alcohol consumption, risky sexual behavior and experience of STIs among men.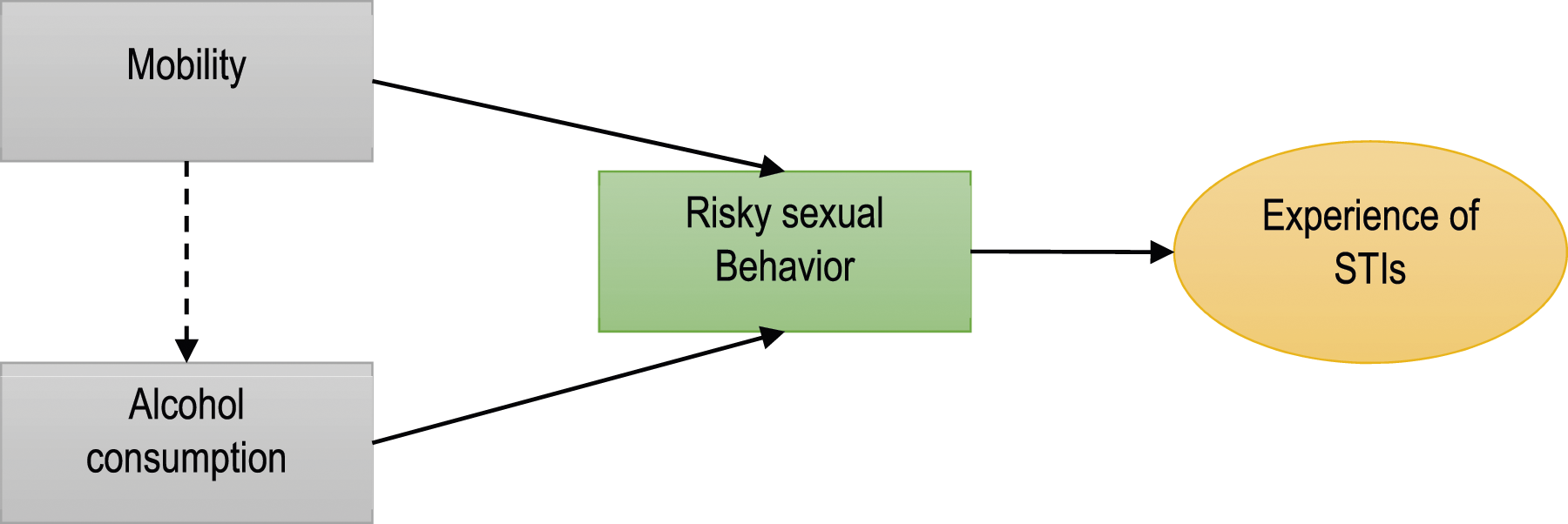
Methods
Data source
We used data from the fifth round of the National Family Health Survey (NFHS-5), conducted in 2019-21. NFHS-5 is a nationally representative, cross-sectionally sample survey conducted by the International Institute for the Population Sciences (IIPS), Mumbai, across all the states and union territories in India. The survey provides a myriad of essential and reliable information on household characteristics, maternal and child health, nutrition, mobility and mortality, women empowerment, domestic violence, and knowledge and awareness of HIV/AIDS. It also covers men’s information on health and well-being, including sexual life. A two-stage stratified sampling design was adopted to collect the data in the NFHS. The 2011 Census was used as a sample frame to choose primary sample units (PSUs). PSUs ─ villages in rural areas and census enumeration blocks in urban areas ─ were selected using probability proportional to size (PPS) systematic sampling. Then, households from each PSU were randomly selected using systematic sampling. A detailed description of the sampling design and data collection process is available in the national report of NFHS-5. 7 In NFHS-5, men’s data were collected for 101,839 samples aged 15-54 years. We used samples of 71,128 sexually active men aged 15-54 years.
Outcome variable
Our outcome of interest in this study was symptoms of an STI among men. Respondents who reported being sexually active ever were asked three questions about symptoms of STIs: whether the respondent had a disease through sexual contact, an abnormal discharge from penis, or a sore or ulcer on or near penis. A binary outcome variable was constructed where men who reported at least one symptom were considered to have an STI, labelled as ‘1’, otherwise coded as ‘0’. All questions were asked for a reference period of the last 12 months preceding the survey.
Key exposure variable
The key exposure variable in our study is mobility, defined using responses from the NFHS-5 survey. Respondents were asked if they had been away from home for one month or more in the last 12 months, and those answering affirmatively were further queried about durations of six months or more. Based on these responses, we categorized the mobility variable into three groups: (a) no mobility; (b) short-duration mobility (away for one month or more but less than six months); and (c) long-duration mobility (away for six months or more). This classification aligns with a similar methodology used in a prior study in India based on NFHS-3 data (Gupta et al., 2010).
We further identified two important pathway variables: (a) alcohol consumption and (b) risky sexual behavior. A binary variable was constructed for alcohol consumption based on self-reported information, with 'yes' indicating alcohol consumption (coded as ‘1’) and 'no' denoting non-consumption (coded as ‘0’). The assumption, supported by literature, is that mobile men, especially those consuming alcohol, are more likely to engage in high-risk sexual behavior. We operationalized risky sexual behavior as engaging in sexual intercourse with a non-marital or non-cohabitating partner, constructing a binary variable based on responses to questions about the time since the last sexual encounter and the relationship with the partner. Those having intercourse with someone outside of marriage or cohabitation in the last 12 months were coded as '1', and those who had not were coded as '0'. This indicator aligns with NFHS recommendations for assessing high-risk sexual behavior in India.7,34,35
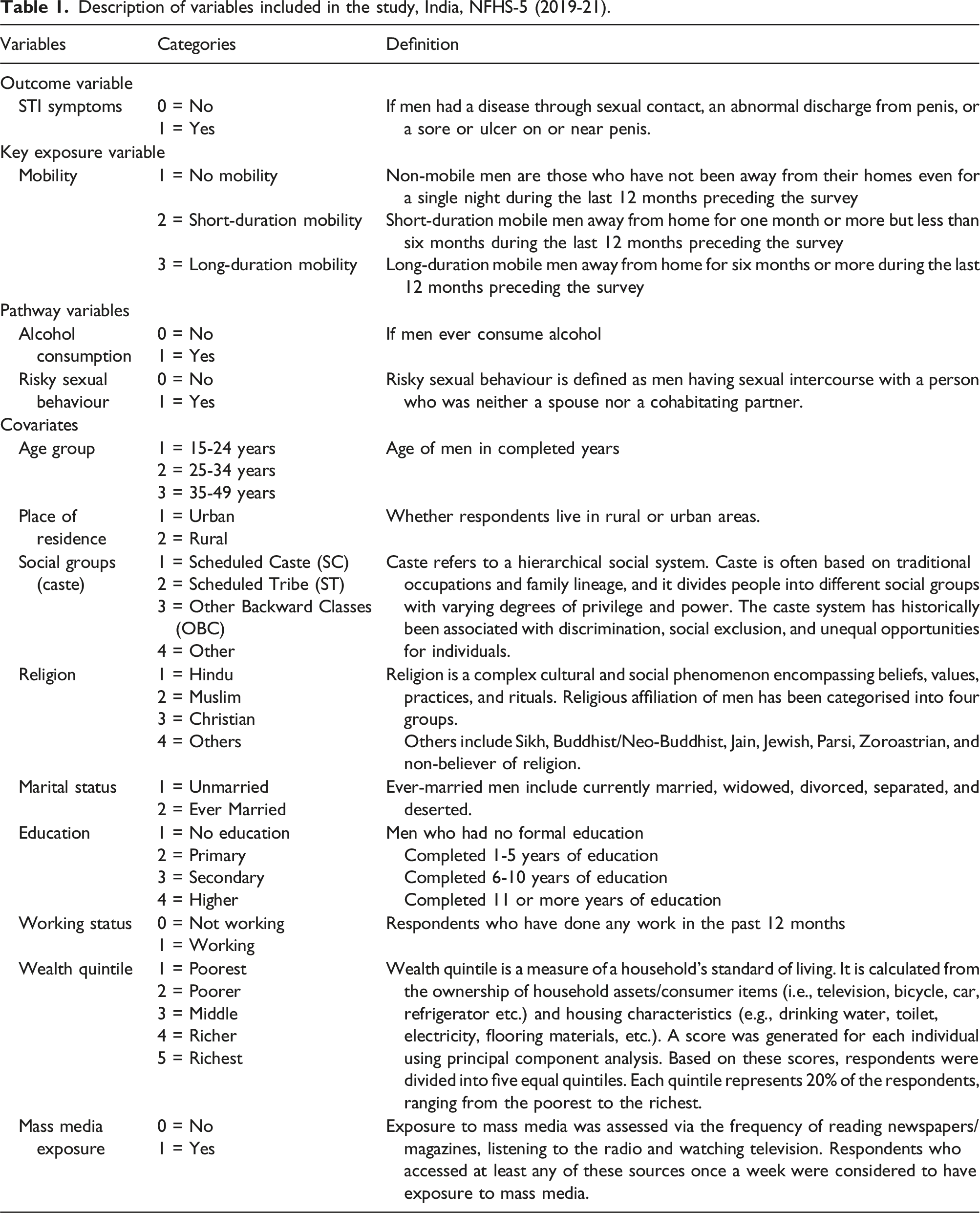
Covariates
Description of variables included in the study, India, NFHS-5 (2019-21).
Data analysis
We employed a comprehensive analytical approach to investigate the association between mobility, alcohol consumption, risky sexual behavior, and STI symptoms among men. Initially, unweighted numbers and percentages summarized study participants, and the prevalence of STI symptoms was calculated across key exposure, pathways and socio-demographic variables. Pearson’s chi-square statistic tested the statistical significance of these differences.
Binary logistic regression models were then utilized for bivariate and multivariable analyses, assessing the association between independent variables and the outcome of the study. Four sequential models were applied, progressively incorporating alcohol consumption, risky sexual behavior, and adjusting for covariates. Interaction analyses further explored nuanced associations, examining the combined impacts of mobility, alcohol use, and risky sexual behavior on STI symptoms. Both unadjusted and adjusted models were employed, controlling for socio-demographic covariates.
Results of logistic regression models were presented as crude and adjusted odds ratios with 95% confidence intervals, utilizing p-values to denote significance levels. Sample weights were applied, and potential endogeneity was addressed by including pathways and controlling variables. Multi-collinearity was tested using the variance inflation factor, with no detected issues. Stata, version 16.0, facilitated all statistical analyses, ensuring a robust and thorough exploration of the complex interplay between mobility, alcohol consumption, risky sexual behavior, and STIs among men.
Results
Characteristics of participants
Descriptive statistics and prevalence of STI symptoms by selected variables, NFHS-5 (2019-21).
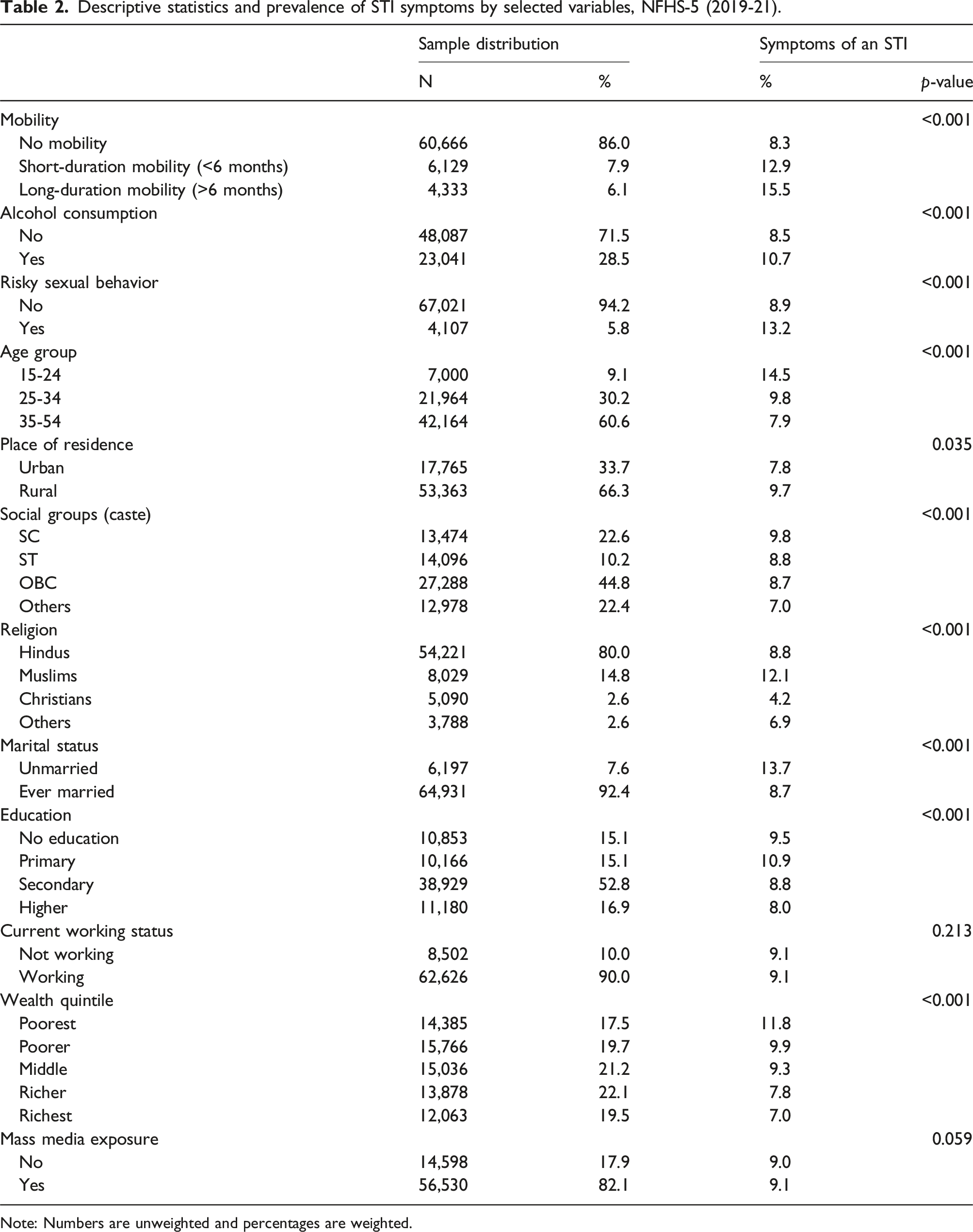
Note: Numbers are unweighted and percentages are weighted.
Prevalence of STI symptoms by independent variables
A greater proportion of men who were mobile for short (12.9%) and long durations (15.5%) experienced STIs compared to those who were not mobile (8.3%). Men who consumed alcohol reported a higher prevalence of STI symptoms than those who did not (10.7 vs 8.5%). Additionally, men who had sexual intercourse with a non-marital or non-cohabitating partner had a higher prevalence of STIs than those who did not (13.2 vs 8.9%) (Table 2).
The prevalence of STIs was notably higher among younger men compared to older men. Men living in rural areas had a slightly higher proportion of STIs than those in urban areas (9.7 vs 7.8%). STI symptoms were more prevalent among men from marginalized social groups, such as SC, ST, and OBC and those identifying as Muslim. Unmarried men experienced a significantly higher proportion of STI symptoms than their married counterparts (13.7 vs 8.7%). STIs were also common among men with no formal education or lower levels of education and those from the poorest quintile of household wealth (Table 2).
Association of mobility, alcohol use, and risky sexual behavior with STI symptoms
Binary logistic regression models showing the association of mobility, alcohol consumption, and risky sexual behavior with STI symptoms among men in India.
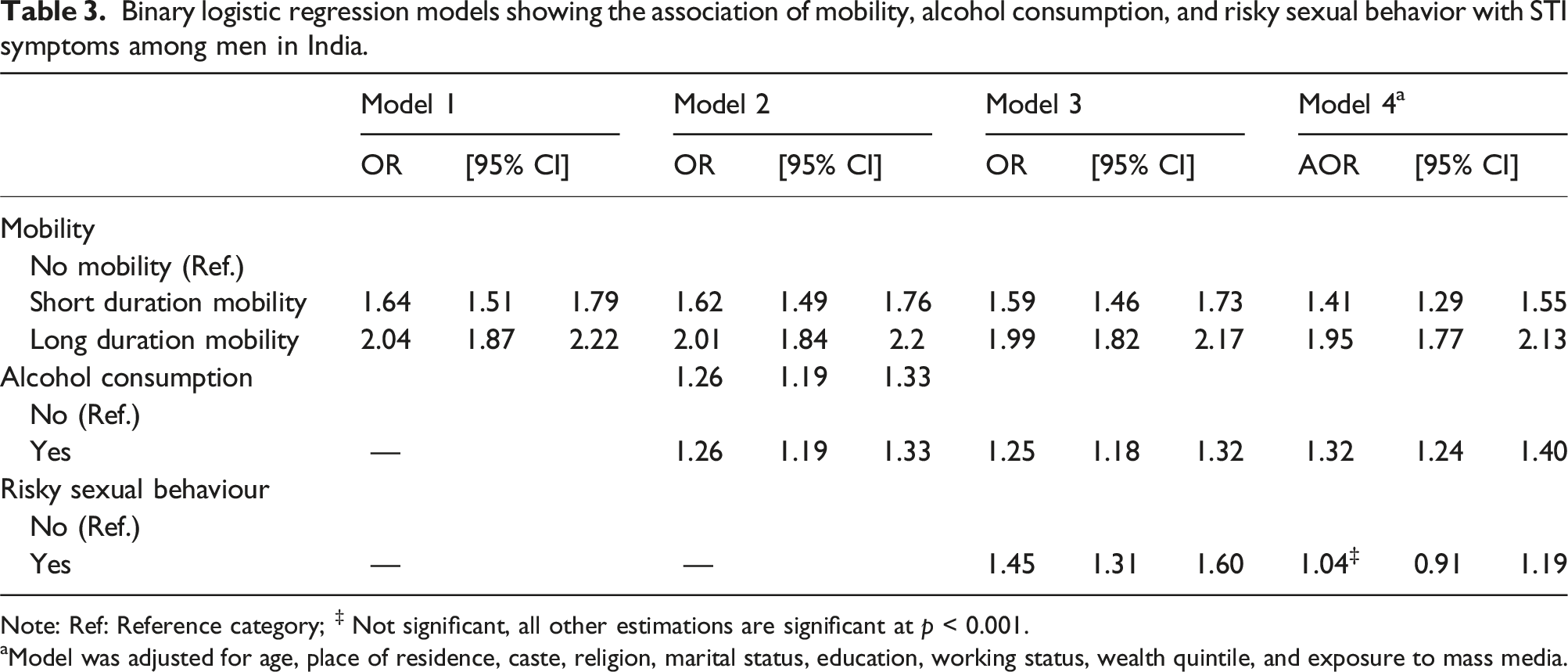
Note: Ref: Reference category; ‡ Not significant, all other estimations are significant at p < 0.001.
aModel was adjusted for age, place of residence, caste, religion, marital status, education, working status, wealth quintile, and exposure to mass media.
Multivariate analyses further indicate that men living in rural areas, belonging to the Muslim religion, currently working and having mass media exposure were associated with higher odds of STI symptoms. In contrast, men who belonged to the ST, OBC, and other social groups, were ever-married and from upper quintiles of household wealth were significantly associated with a decreased likelihood of experiencing an STI (Figure 2). Multivariate logistic regression results (odds ratio with 95% confidence intervals) showing the influence of key predictors and other covariates on STI symptoms among men in India, NFHS-5.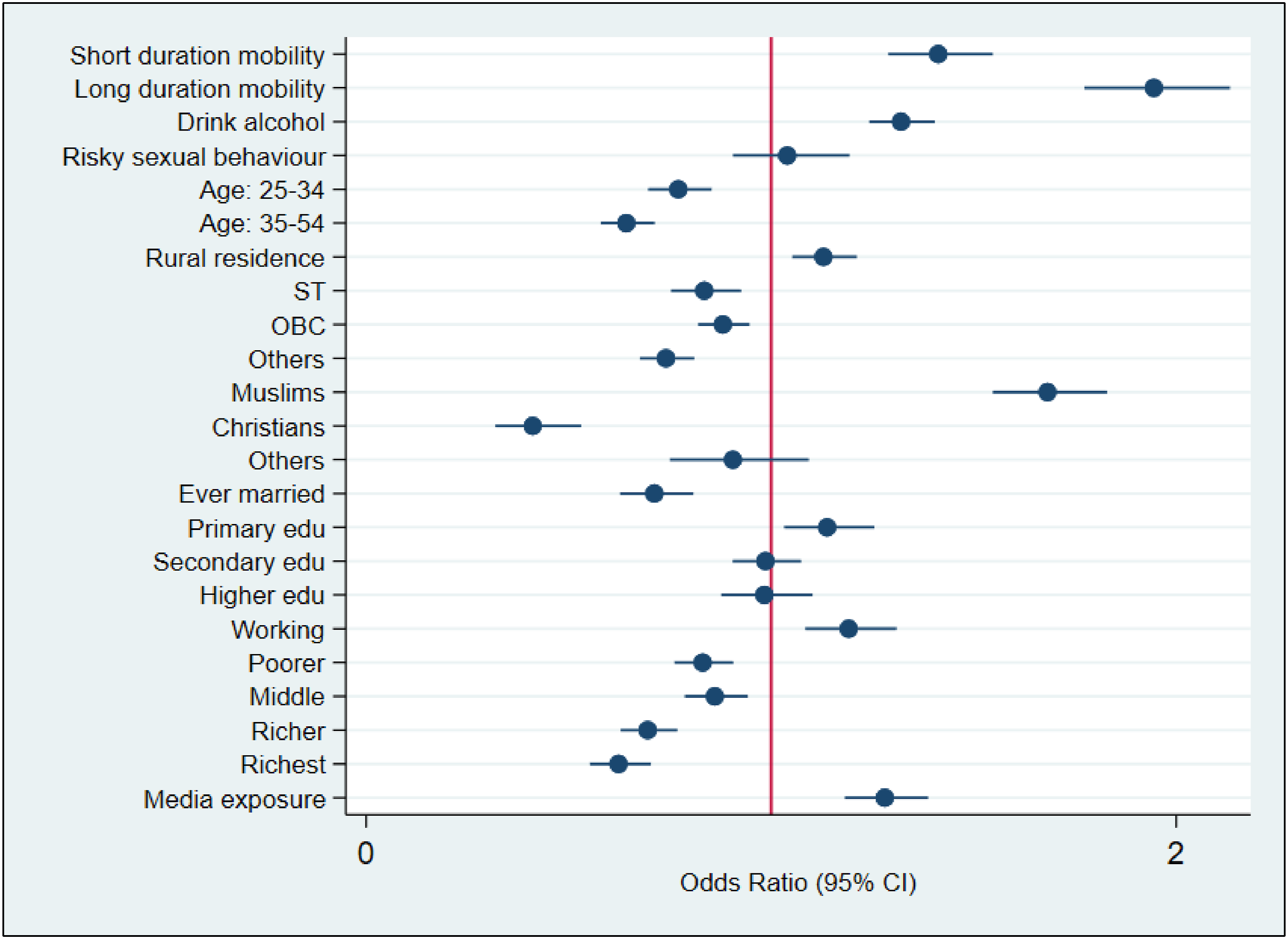
Interaction analysis
Interaction analysis showing the heterogeneous association of mobility and alcohol consumption with STI symptoms among men in India.
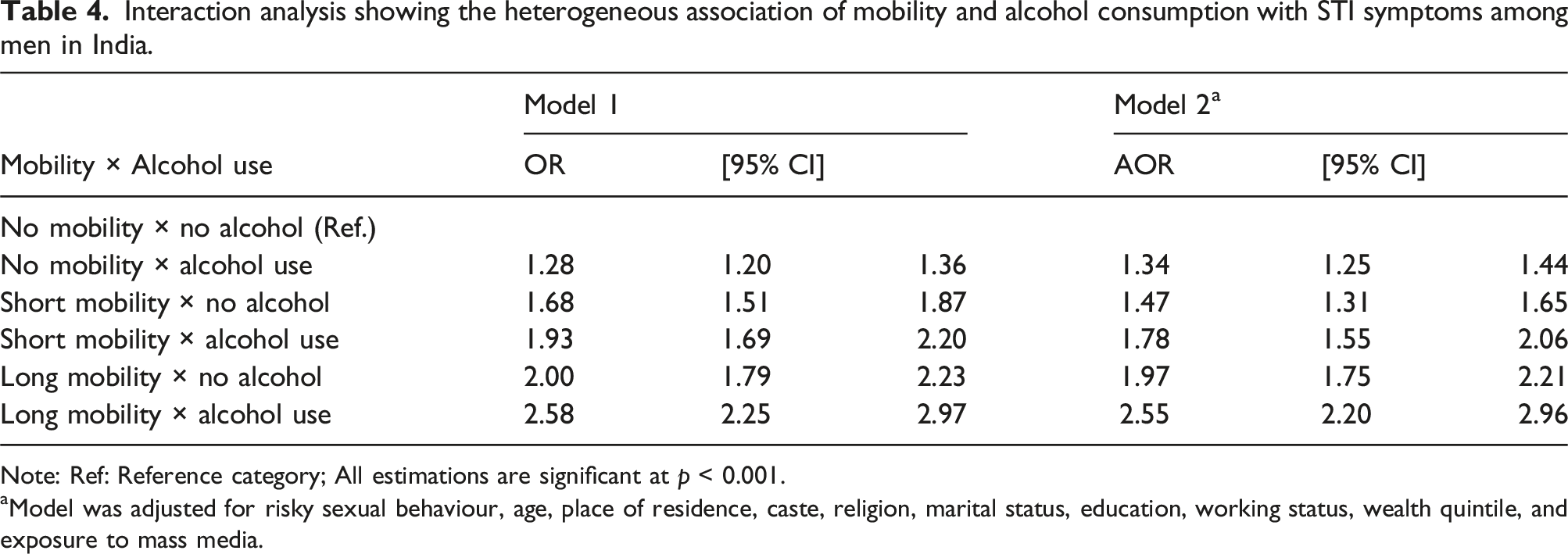
Note: Ref: Reference category; All estimations are significant at p < 0.001.
aModel was adjusted for risky sexual behaviour, age, place of residence, caste, religion, marital status, education, working status, wealth quintile, and exposure to mass media.
Interaction analysis showing the heterogeneous association of mobility and risky sexual behavior with STI symptoms among men in India.
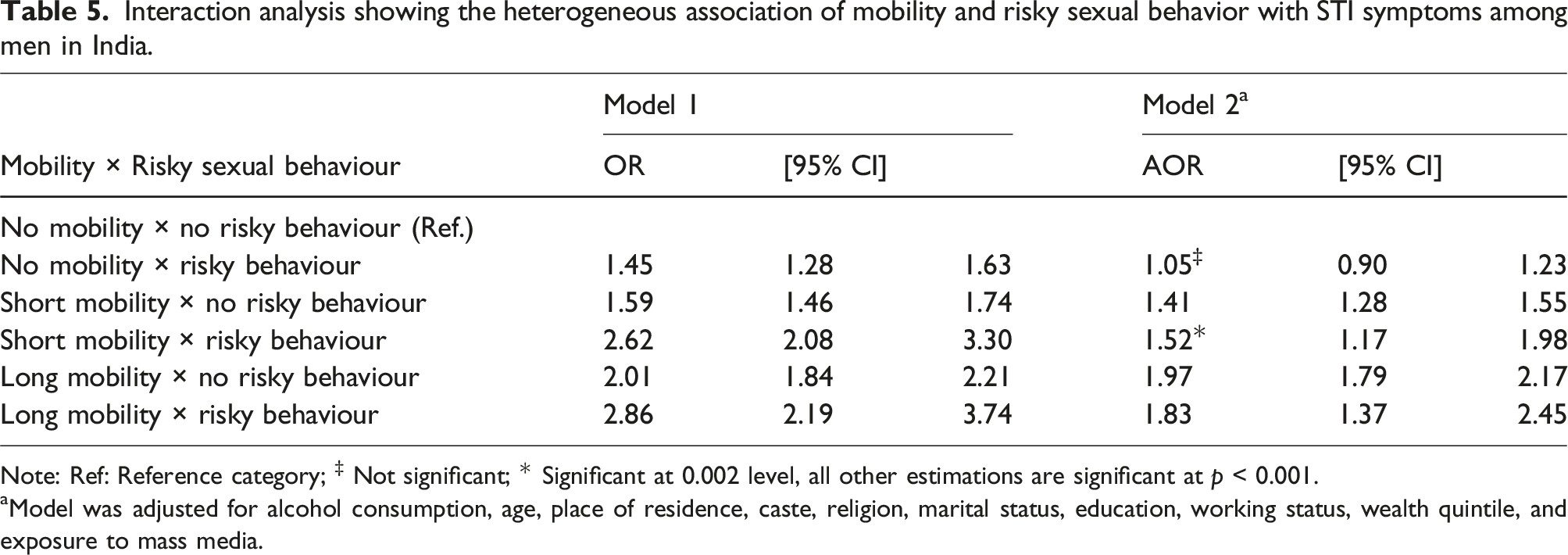
Note: Ref: Reference category; ‡ Not significant; * Significant at 0.002 level, all other estimations are significant at p < 0.001.
aModel was adjusted for alcohol consumption, age, place of residence, caste, religion, marital status, education, working status, wealth quintile, and exposure to mass media.
Interaction analysis showing the heterogeneous association of mobility, alcohol consumption and risky sexual behavior with STI symptoms among men in India.
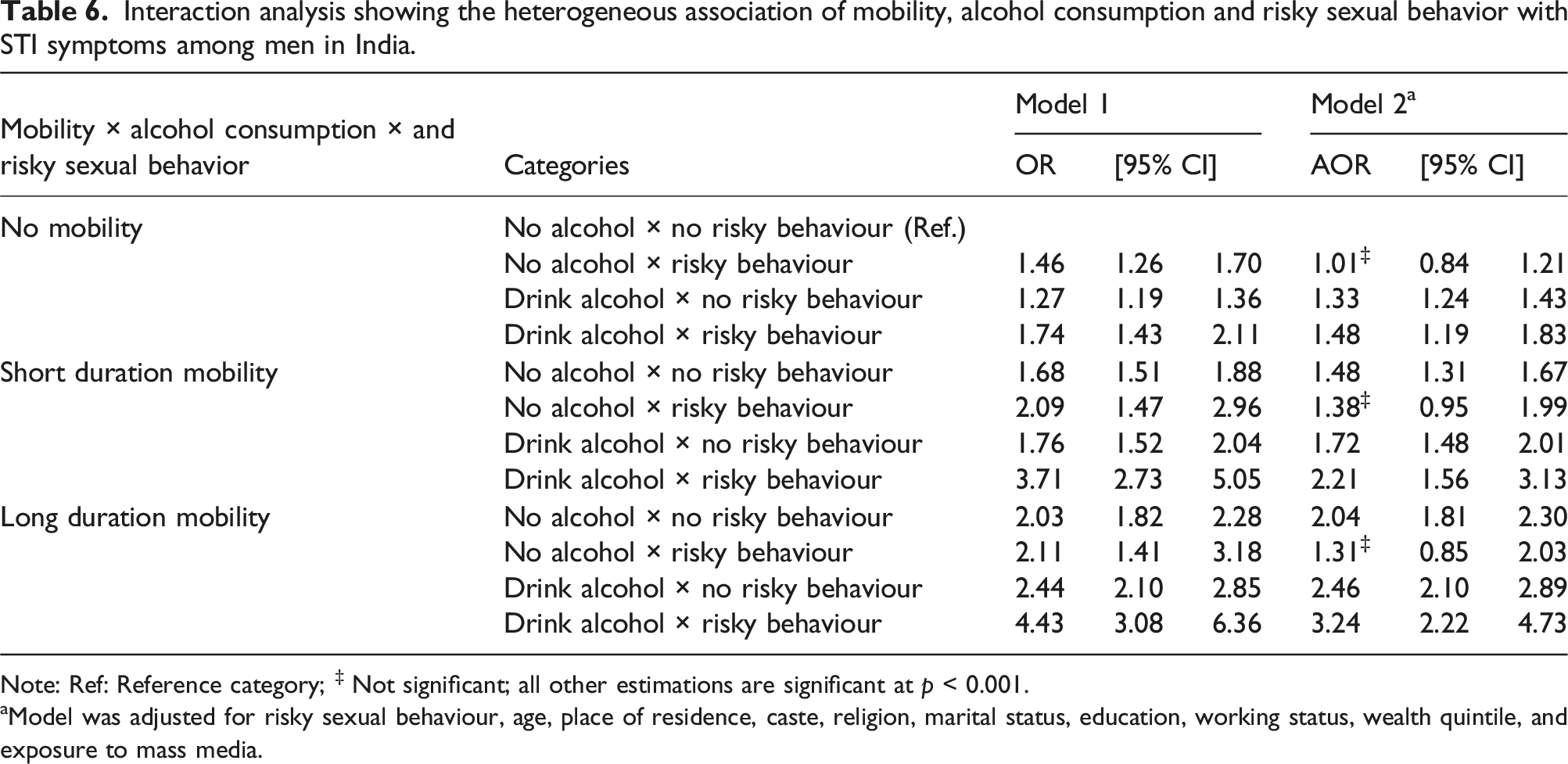
Note: Ref: Reference category; ‡ Not significant; all other estimations are significant at p < 0.001.
aModel was adjusted for risky sexual behaviour, age, place of residence, caste, religion, marital status, education, working status, wealth quintile, and exposure to mass media.
Discussion
The findings of this study suggest that mobile men in India are more likely to experience STI infection than non-mobile men. These findings are consistent with a prior study that assessed the association between mobility, sexual risk behavior and STI infection in India. 17 Gupta et al. (2010) 17 observed that men with short- and long-duration mobility who consume alcohol were significantly associated with an increased likelihood of having multiple sexual partners, engaging in high-risk sexual intercourse, and contracting STI infections.
Our study found that mobility (both short- and long-duration mobility) emerged as an important predictor of STIs among men. Further, high-risk sexual behavior and alcohol consumption are found to be important pathway factors which heighten the risk of STIs among mobile men. Mobile men may be at a higher risk of having sexual intercourse with non-marital or non-cohabitating partners compared to non-mobile men. Moreover, men who reported alcohol use may be likely to be engaged in high-risk sexual activities such as sexual intercourse with non-marital or non-cohabitating partners. Notably, alcohol consumption was found to be an independent association with STI symptoms. Although risky sexual behavior had a significant association with an increased risk of STIs when considering mobility and alcohol use in the analysis, it was no longer significant after controlling for socio-demographic covariates. The interaction analysis of mobility, alcohol use, and risky sexual behavior showed that long-duration mobile males who used alcohol and engaged in sexual risk behavior were more prone to STI infections than any other group. The reasons could be that migrants, especially construction workers and long-distance truck drivers, frequently indulge in sexual intercourse with commercial sex workers. They are more likely to have unprotected sex, have a low sense of risky behavior, and have limited knowledge and awareness of STIs. 36
Several previous studies in India consistently found that migrants and mobile men are more likely to engage in risky sexual behavior compared to the non-migrants/non-mobile population.13,17,37 A qualitative study among returned migrants (primarily from Mumbai, India) in Nepal documented that migrants frequently engage in sexual intercourse with multiple partners, and some continued extramarital sex after their return to Nepal. The study further noted that peer norms and pressure, alcohol drinking, cheaper sex, single life and low perceived vulnerability to HIV/STIs are the major reasons for engaging in risky sexual behavior among those returned migrants from India. 11 A systematic review and meta-analysis in China found that rural-to-urban migrants, particularly construction workers and long-distance truck drivers, are highly susceptible to STIs. 36 A study conducted in Central Asia also suggests that mobility is associated with an increased risk of STI and HIV transmission among non-migrants. Their study further highlights that the mobile population are more likely to engage in high-risk sexual behavior, such as multiple sexual partners, commercial sex, and unprotected sex. 38 A cross-sectional study among Tanzanian agricultural plantation residents documented that male migrants have a significantly elevated risk of STIs than their non-migrant peers. 39 In Uganda, a nationwide study shows that risky sexual behaviors like unprotected sex and multiple sexual partners were significantly associated with an increased risk of STIs. 40
In the context of the increasing STI infections and HIV epidemic in India, evidence of associations between mobility, alcohol use, risky sexual behavior and STI infection is critical for policy and programmatic points of view. The results of this study strongly imply that short and long duration mobility and alcohol use together have a profound and elevated risk for STI infections. Moreover, risky sexual behavior plays a mediating role in the association between mobility, alcohol use, and STI infection. As a result, efforts to limit the HIV epidemic that concentrate primarily on male migrants will continue to be only marginally successful. Additionally, temporarily mobile men who drink alcohol have a higher prevalence of risky sexual conduct and STIs. Temporarily mobile males, especially those who spend more time away from home, run the danger of engaging in risky sexual activity and drinking alcohol. Alcohol consumption among mobile men clearly appears as the most significant determinant for risky sexual behavior as well as STI infections. Interventions that target such high-risk groups could be helpful in reducing the risk of STIs and HIV transmission.
The findings of this study recommend focusing on mobile males who drink alcohol in order to prevent risky sexual behavior and STI/HIV transmission. The current study’s findings provide thoughtful insights into the association between mobility, alcohol use, sexual risk behavior and STI infection in India. The main strength of this study is the use of nationally representative data, which provides valuable evidence to make effective interventions in high-risk population groups to prevent STI/HIV transmission. However, our study is not without limitations and thus needs to be cautious while discussing the findings. First, the measure of STI symptoms is self-reported and may be biased. Many STIs are asymptomatic. Moreover, individuals having a disease through sexual contact would potentially involve a diagnosis or an understanding of sexually transmitted diseases. Second, the questions on sexual behavior, alcohol use, and STIs are extremely sensitive and are subject to reporting bias. Recall bias may also occur due to a longer reference period (12 months) for recalling STI symptoms. Third, risky sexual behaviour could also be biased because someone could report on their last sexual encounter with a spouse/cohabitating partner, but also have had a previous encounter with someone else. Fourth, the mobility measure is not comprehensive. The nature of mobility among males in India is much more complex and multifaceted. The survey did not ask about distance and place of destination. More focused research on patterns and characteristics of mobility and migration for a better understanding of the association using longitudinal data is warranted in order to provide evidence-based focused, targeted interventions. Finally, since data is cross-sectional and collected at a particular point in time, we are unable to understand that alcohol consumption, risky sexual behaviour and acquisition of STI occurred while the respondent was away from home. Causal inferences between the independent variables and the outcome variable could not be assessed due to the cross-sectional nature of the dataset.
Conclusion
Despite several efforts by the government, combating the risk of STI infections among vulnerable population groups remains challenging in India. Our study suggests that mobility (both short and long durations) was significantly associated with an elevated risk of STIs among men. Alcohol consumption and risky sexual behavior further heightened the risk of STIs among mobile men. The vulnerable population, especially mobile population groups in the context of alcohol use, can be informed about the negative consequences of STIs/HIV through awareness campaigns engaging with various stakeholders at the local level. Promoting safer sex relations among mobile men by improving easy access to condoms and other methods of contraception as well as sensitizing the potential risk of STI transmission through sexual risk behavior could be helpful. Initiatives for HIV prevention among men must pay particular attention to temporary mobile men for both short and long durations, particularly those mobile men who consume alcohol and engage in risky sexual behavior.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The ethical approval of the National Family Health Survey-5 (NFHS-5) was obtained from the ethics review board of the International Institute for Population Sciences (IIPS) Mumbai and reviewed and approved by the ICF International Review Board (IRB). Informed consent was obtained from each participant before conducting the interviews. The NFHS-5 is an anonymous, publicly available dataset with no identifiable information about the survey participants and is accessible upon a granted request from the DHS Program website at ![]() .
.