
Abstract
The 2024 UK guidelines for the management of syphilis are in line with current evidence and practice within the UK. Key updates are detailed at the start of the article. These guidelines are accompanied by the first UK guidelines for the management of syphilis in pregnant people and children, 2024.
New in the 2024 guidelines
• Administration of benzathine penicillin with lidocaine is now licensed and the recommended option • Macrolides are no longer an option for treatment due to antimicrobial resistance • Ceftriaxone is an alternative treatment; appropriate in most cases where penicillin cannot be used • Expanded use of PCR testing • Update to serology testing in light of withdrawal of the TPPA from the UK • Management of serofast individuals • Changes to recommendations for lumbar puncture • Change to management of treatment interruptions; extension to acceptable time of interruptions between benzathine injections
Objectives
• The main objective of these guidelines is to reduce the number of sexually transmitted infections (STIs) and the complications that can arise in people either presenting with signs and symptoms of an STI or undergoing investigation for possible infection. • Specifically these guidelines offer recommendations on the diagnostic tests, treatment regimens and health promotion principles needed for the effective management of syphilis. Management of the initial presentation is covered, as well as how to prevent transmission and future infection. • The guidelines are aimed primarily at healthcare professionals managing people aged 16 years or older in departments offering specialist care in STI management within the UK. However, the principles of the recommendations should be adopted across all levels of care (where appropriate, levels 1 and 2 may need to develop local care pathways). • The recommendations may not be appropriate for use in all clinical situations. Decisions to follow these recommendations must be based on the professional judgement of the clinician and consideration of individual patient circumstances and available resources.
Search strategy
• The previous UK and US guidelines for the management of syphilis were reviewed.1,2 • A systematic literature review was undertaken. Medline, Embase and the Cochrane library were searched for English language publications between January 2014 and December 2020 using the following terms: (i) syphilis AND (“partner notification” OR “contact tracing”); (ii) (syphilis OR neurosyphilis) AND (treatment OR therapy OR benzylpenicillin OR lidocaine OR ceftriaxone) AND intramuscular; (iii) (syphilis OR neurosyphilis) AND “rapid plasma regain”; (iv) “primary syphilis” AND “dark ground microscopy” AND (PCR OR serology OR IgM); (v) (syphilis or “Treponema pallidum”) AND PCR; (vi) (syphilis or “Treponema pallidum”) AND (“rapid tests” OR “point of care tests”); (vii) neurosyphilis AND diagnosis AND (CSF OR PCR OR TPPA OR titre OR serology); (viii) (syphilis or “Treponema pallidum”) AND typing; (ix) (syphilis or “Treponema pallidum”) AND “whole genome sequencing; (x) (syphilis or “Treponema pallidum”) AND (serology OR discordant OR confirmation OR algorithm); and (xi) (syphilis or “Treponema pallidum”) AND (immunoblot OR immunoassay).
Methods
• The guidelines writing group followed the BASHH Framework for Guideline Development.
3
Equality impact assessment
• Equality impact assessment was completed using the National Institute for Health and Care Excellence tool (see Appendix 1).
Stakeholder involvement, piloting and feedback
• The document was reviewed by the Clinical Effectiveness Group (CEG) of BASHH, and their comments incorporated. The draft guidelines were placed on the BASHH website and any comments received after 2 months were reviewed by the authors and acted on appropriately. The document was also piloted by target users and the public panel of BASHH, and their feedback considered by the authors.
Aetiology, transmission and epidemiology
• Syphilis is caused by infection with the spirochete bacterium Treponema pallidum subspecies pallidum.
4
• It is transmitted by direct contact with an infectious lesion or by mother-to-child transmission (transplacental passage) during pregnancy.
5
Approximately one-third of sexual contacts of individuals with infectious syphilis will develop the disease (transmission rates of 10%–60% have been reported).6,7 • Site of bacterial entry is typically genital in heterosexual patients, but 32%–36% of transmissions among gay and bisexual men who have sex with men (GBMSM) may be at extra-genital (anal, rectal and oral) sites through oral–anal or genital–anal contact.
8
In one study 13.7% of all syphilis transmissions were attributed to oral sex, with reports in other studies of 20% to 35% in GBMSM.9–11 Injecting drug use (sharing needles) and rarely blood transfusion (routine screening is performed in the UK and treponemal survival beyond 24–48 h at 4°C is unlikely) are also potential routes of transmission.12–14 • Syphilis predominates among GBMSM aged 25–34 years, many of whom are living with HIV. In England in 2019 there were 7982 cases of infectious syphilis, of which 5875 (74%) were in GBMSM, 43% of whom were living with HIV.
15
• Since 2014, the overall rise in infectious (primary, secondary or early latent) syphilis cases has included an increase in heterosexual cases, which had previously remained relatively low and stable. By 2019, diagnoses in women had increased by 135% to 597, and had doubled in men to 1016.
15
• Bisexual men accounted for 8% of diagnoses in GBMSM in England in 2019. Heterosexually identifying GBMSM may explain some of the difference in diagnoses between heterosexual men and women.15,16 • Syphilis cases have risen in almost all parts of the UK and remain persistently high in some geographical locations, including London, Manchester and Brighton.15,17
Public health
• Outbreaks of syphilis are often detected by genitourinary medicine clinicians who observe a change or an increase in cases, unusual patterns, or single cases of concern. Any unusual observations can be discussed with health protection teams and local public health staff. Each team will have a nominated lead for sexual health. The team can provide the context, surveillance data and local personnel to identify, investigate and manage a local outbreak, including health promotion, awareness raising and support. English-based local health protection teams can be found at: https://www.gov.uk/health-protection-team. • National outbreak control guidance provides a summary of key professional roles and responsibilities for identifying and managing STI outbreaks and a reference list of published syphilis outbreak investigations.
18
• Local public health and health protection teams are also engaged in longer-term actions as part of the response to nationwide increases in syphilis. These actions include targeted communication to the population at risk and the wider community of health providers who may see cases of syphilis during their work. In 2019, in response to the continued increase in syphilis in England, an action plan was published that brought together existing recommendations for clinicians, public health specialists, specialty societies and sexual health service commissioners into a single document.
16
Classification and clinical features
• Syphilis is a multi-stage, multi-system disease, which is broadly defined as congenital or acquired syphilis.
Acquired (adult) disease
Early (infectious) disease
• Following contact, T. pallidum invades through the mucosal surface or abraded skin and divides at the point of entry to produce the chancre of primary disease. This incubation period is typically 21 days (range 9–90 days) but is dependent on the infectious dose; higher doses result in ulcers more quickly.7,19 Primary syphilis is characterised by a single papule and moderate regional lymphadenopathy. The papule subsequently ulcerates to produce a chancre, which is classically anogenital (penile, labial, cervical or peri-anal), single, painless and indurated with a clean base discharging clear serum but not pus. However, a significant minority of people with primary syphilis have painful and/or multiple chancres.
20
Chancres may also be multiple, painful, purulent, destructive and extra-genital (most frequently oral). When present at extra-genital sites and when painless, chancres may pass unnoticed. In the context of HIV co-infection, earlier studies indicated that chancres may be multiple, deeper and persist into the secondary stage of disease,21,22 although more recent studies in the antiretroviral era suggest no significant differences between early manifestations of syphilis in those with and without HIV co-infection.
20
Early after infection the bacteria disseminate widely via blood and the lymphatic system and are subject to local immune clearance; ulcers resolve over 3–8 weeks. • Untreated, 25% of patients will develop signs of secondary syphilis approximately 3–10 weeks after the appearance of the initial chancre .23,24 Secondary syphilis affects multiple systems and typically develops 3 months after infection .
5
It often presents with a widespread mucocutaneous rash and generalised lymphadenopathy. The rash may be maculopapular (50%–70%), papular (12%), macular (10%) and occasionally ulceronodular. The rash may, but does not usually, itch.23,25–27 It can affect the palms and soles (11%–70%), and hair follicles resulting in alopecia. Two further important mucocutaneous signs are mucous patches (buccal, lingual and genital) and highly infectious condylomata lata affecting warm, moist areas (mostly the perineum and anus).8,26 HIV infection does not appear to affect the mucocutaneous manifestations of secondary syphilis.22,23 Secondary syphilis may result in hepatitis, glomerulonephritis (mediated by antibody–treponeme complex deposition), splenomegaly and, more rarely, pulmonary, bone and gastric involvement.28–30 Patients can develop neurological complications during secondary syphilis. These are typically acute meningitis (headache, neck stiffness, photophobia and nausea) and cranial nerve palsies including eighth nerve palsy with resultant hearing loss and possible tinnitus.23,31 Eye involvement may result in uveitis (most commonly posterior and bilateral), optic neuropathy, interstitial keratitis and retinal involvement.27,32–34 Co-infection with HIV may increase the likelihood and severity of ocular and neurosyphilis.23,27,33,35 • Previous syphilis infection may reduce the likelihood of clinical symptoms with subsequent infections.36–38 Previous infection does not confer immunity and individuals are susceptible to re-infection.
Latent disease
• Secondary syphilis will resolve spontaneously in 3–12 weeks and the disease enters an asymptomatic latent stage.
23
The latent stage is defined as early within 2 years, and late thereafter (ending with the development of tertiary disease). The distinction between early and late latent disease is somewhat arbitrary, but important as approximately 25% of untreated patients will develop a recurrence of secondary disease during the early latent stage.
24
Late (tertiary) disease
• Late disease occurs in approximately one-third of untreated patients around 20–40 years after initial infection. It is divided into gummatous (15% of patients), cardiovascular (10%) and late neurological disease (7%).
24
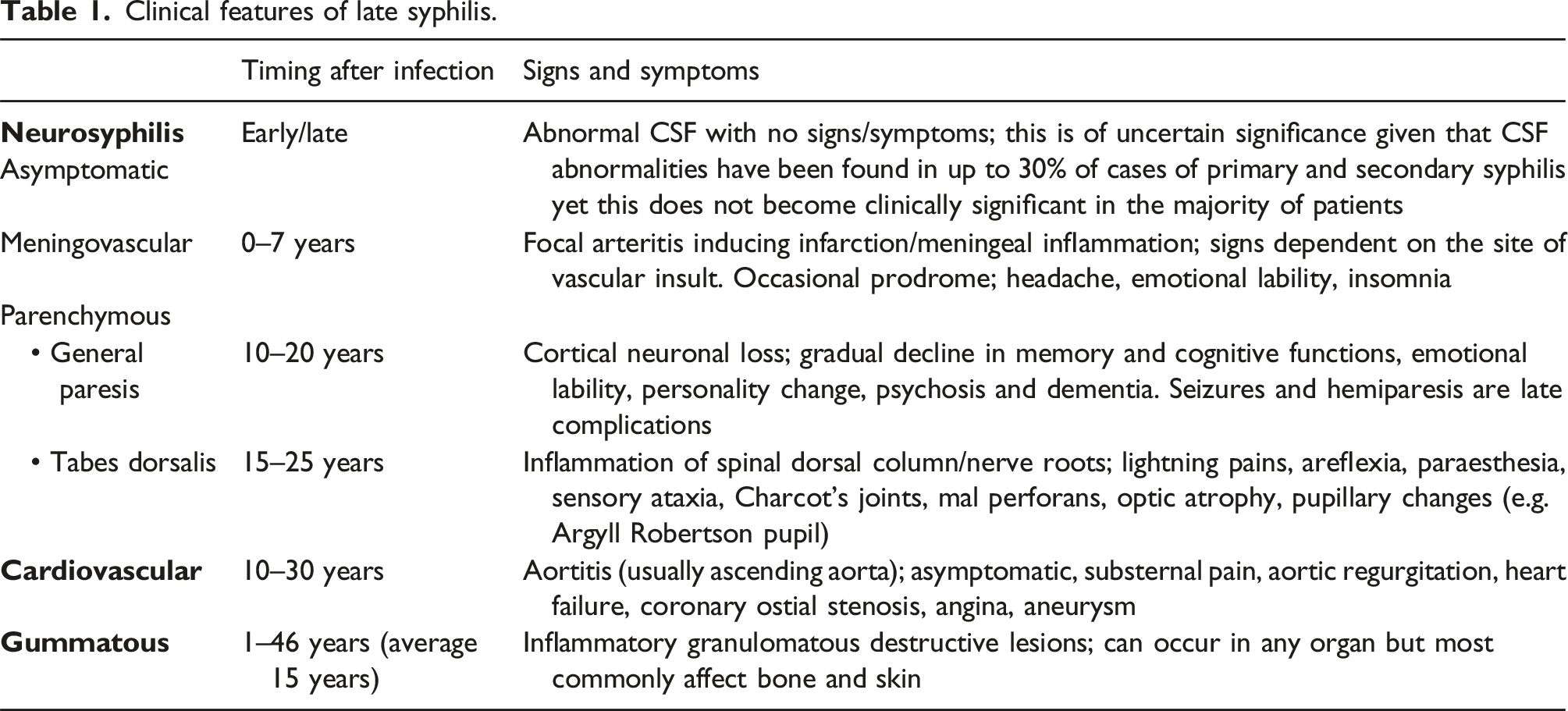
The clinical manifestations of late syphilis are highly variable and are rarely seen due to the use of treponemicidal antibiotics for other indications. The clinical features of symptomatic late syphilis are summarised in Table 1. Clinical features of late syphilis.
Gummatous disease
• In the Oslo study, 15% of patients developed gummatous disease.
24
These granulomatous lesions with central necrosis can occur within 2 years, but are typically seen after an average of 15 years
5
. They can occur anywhere, but most often affect skin and bones. Granulomatous lesions rapidly resolve on administration of therapy.
Cardiovascular disease
• Cardiovascular syphilis typically occurs 15–30 years after infection. Cardiovascular syphilis only becomes symptomatic or complicated in 10% of patients.
24
The ascending aorta is the predominant site of damage resulting in dilatation and aortic valve regurgitation. Rarely, the coronary ostia may become involved and saccular aneurysms may develop.
39
Neurological disease
• Meningovascular syphilis typically occurs 5–10 years after infection (but sometimes earlier). It is not typically considered to be tertiary disease. Meningovascular syphilis may present with infectious arteritis which may result in ischaemic stroke (the middle cerebral artery territory is most commonly affected). Prodrome may occur in the weeks/months prior to stroke including headache, emotional lability and insomnia. • General paresis: this is a progressive dementing illness that occurs 10–25 years after infection secondary to cortical neuronal loss. Initial forgetfulness and personality change develop into severe dementia, and seizures and hemiparesis may occur (late stage). • Tabes dorsalis occurs 15–25 years after infection (longest of neurological complications). It is characterised by sensory ataxia and lightning pains; pupillary abnormalities are common (Argyll Robertson pupil) and dorsal column loss (absent reflexes, joint position and vibration sense) can be present.
Clinical diagnosis
History
• A full and accurate history is important to identify potential complications of symptomatic infection (both early and late) and to distinguish between late latent, previously treated and non-venereal T. pallidum infection (yaws, pinta and bejel), which may have identical serological results. • Full sexual history for: o Primary syphilis – to include all sexual partners in the last 3 months o Secondary and early latent syphilis – to include all partners in the last 2 years o Late syphilis – according to history and previous treponemal serology, lifetime partners and possibly children. • Directly question for symptoms of syphilis • Fully explore previous syphilis diagnoses: o Year and place of diagnosis o Treatment received (drug, route and duration) o Serological results (contact treating centre if necessary/possible). • Previous syphilis testing (with consideration of the screening tests used at the time): o Antenatal screening o Blood donation o Sexual health screening. • Potential for previous infection with non-venereal T. pallidum infection: o Childhood skin infections (yaws) o Previously resident in an endemic area/country. • Full obstetric history (where appropriate): o Adverse pregnancy outcomes (which may be due to syphilis) o Identify live births and children who may have late congenital disease.
Examination
• Early disease (primary or secondary) to include the following, when relevant symptoms are present: o Genital examination o Skin examination including mouth, scalp, palms and soles o Neurological examination. • Symptomatic late disease (including suspected late congenital disease); clinical examination may be undertaken when relevant symptoms are present and may include: o Skin o Musculoskeletal system o Cardiovascular system o Nervous system.
Laboratory diagnosis
Demonstration of T. pallidum using direct detection methods
• Dark ground microscopy:
40
o Gives immediate results o Should be performed only by experienced observers as it is subjective and may lead to false-positive or false-negative results o Is less reliable in examining rectal and non-penile genital lesions and is not suitable for examining oral lesions due to the presence of commensal treponemes o Can detect cases of primary syphilis prior to the development of a serological response. • Molecular diagnostics41–43: o Commercial assays are available for the molecular detection of T. pallidum o Polymerase chain reaction (PCR) has been shown to have higher sensitivity and specificity than dark ground microscopy and can be used on oral or other lesions where commensal treponemes may also be present o Can detect cases of primary syphilis prior to the development of a serological response o In certain circumstances, PCR may aid diagnosis by demonstrating T. pallidum in tissue samples or vitreous fluid,44–46 although most assays are not validated for such specimen types.
• Where appropriate expertise and equipment are available, dark ground microscopy should be performed on possible chancres: 2A. • Molecular testing for T. pallidum is appropriate on lesions where the organism may be expected to be located: 1A.
Serological tests for syphilis
• Treponemal antibody tests cannot differentiate syphilis (caused by infection with T. pallidum subspecies pallidum) from the endemic treponematoses, yaws, bejel (also known as endemic syphilis) and pinta (caused by infection with T. pallidum subspecies pertenue, endemicum and carateum respectively). Positive treponemal serology in patients from a country with endemic treponemal infection should therefore be treated for syphilis as a precautionary measure unless they have been adequately treated for syphilis previously.
47
• Antibody tests can be classified as: o Non-treponemal tests: using an antigen consisting of cardiolipin, lecithin and cholesterol such as the Venereal Diseases Research Laboratory (VDRL) carbon antigen test and the rapid plasma reagin (RPR) test. UK laboratories perform the RPR test rather than the VDRL test as it is less technically demanding and not easily available. These tests usually produce a positive result around 6 weeks after infection, reach peak titres after 1–2 years and remain positive with low titres in late disease, if infection is untreated.
48
o Treponemal tests: treponemal enzyme immunoassay (EIA) or chemiluminescent immunoassay (CLIA), Treponema pallidum haemagglutination assay (TPHA), Treponema pallidum latex agglutination (TPLA) assay. The Treponema pallidum particle agglutination (TPPA) assay was withdrawn from the UK in 2022 due to regulatory requirements. Most of these tests are based on recombinant treponemal antigens and detect treponemal immunoglobulin (Ig)G and IgM antibodies. These tests usually continue to produce a positive result throughout life. o T. pallidum-specific IgM antibody tests: anti-treponemal IgM EIA and immunoblot. IgM reactivity lasts for an average of 6 months but can persist for 12–18 months even after adequate treatment.
Primary screening tests
• Treponemal EIA/CLIA detecting both IgG and IgM are used as screening tests as they are performed using automated high-throughput platforms.
47
• The clinical utility of the IgM test is limited by its suboptimal sensitivity and specificity. It should not be used to stage disease or decide the duration of treatment required, or to diagnose repeat infections.49–51 A positive IgM result may be useful if primary or congenital syphilis is suspected. • Rapid point-of-care tests using finger prick blood samples are useful for on-site testing in outreach settings, provided positive results are confirmed by laboratory tests. Currently there are no treponemal tests that are approved for use with oral fluid.
52
• Self-sampling kits for syphilis use capillary blood, collected via dried blood spot or mini-tube.
53
These samples are screened in the laboratory for treponemal antibodies; usually the sample volume is insufficient for confirmatory testing or for an RPR test.
Confirmatory tests
• Positive screening tests should be confirmed with either TPHA/TPLA or a second EIA/CLIA, as false-reactivity rates can be high in low-prevalence populations.
47
• Most EIA/CLIAs use one or more recombinant treponemal antigens. They are sensitive but may have poor specificity. Where possible, laboratories should use a second treponemal assay that uses different antigen targets to the screening assay to inform the likelihood of false-positive screening results. • Low level reactivity (as defined by the local laboratory) in two EIA/CLIAs (with a negative RPR) could possibly be due to non-specific cross-reactivity in both assays and should be interpreted in context of the clinical presentation and history of risk. A sample should be repeated 2 weeks later to exclude early syphilis. • Conversely, TPHA/TPLA may be less sensitive than some EIA/CLIAs resulting in true screen positive results which fail to confirm. It is important to request a second sample 2 weeks later if early syphilis is suspected, to look for the evolution of serological markers. Specimens may also fail to confirm due to a waning immune response to past infection. • Another specimen should always be tested to confirm positive results, including on the day that treatment is commenced so the peak RPR titre is documented.
Tests for assessing serological activity of syphilis
• A quantitative RPR test with titration to the endpoint should be performed when treponemal tests indicate syphilis as this helps to stage the infection and indicates the need for treatment in some cases, for example where the patient has been previously treated and may have been re-infected.
49
• An initial RPR titre of >1:16 usually indicates active disease and the need for treatment, although serology must be interpreted in the light of the treatment history and clinical findings.
54
• An RPR titre of ≤1:16 does not exclude active infection, particularly in a patient with clinical signs suggestive of syphilis or where adequate treatment of syphilis is not documented. • A four-fold rise in the RPR titre in comparison to an earlier sample, is suggestive of recent syphilis infection.
Tests for monitoring the effect of treatment
• A quantitative RPR test is recommended for monitoring the serological response to treatment and should be performed on a specimen taken on the day that treatment is started as this provides an accurate baseline for monitoring response to treatment. • The treponemal tests remain positive throughout life in most patients, despite adequate treatment, and should not be used to assess disease activity. It is not necessary to repeat these tests for follow-up serology.
Repeat screening is recommended
• Repeat screening is recommended 2 weeks after presentation in those with dark ground microscopy or PCR negative ulcerative lesions that could be due to syphilis. • Repeat screening is recommended 3 months after any high-risk contact, as negative results within 3 months after infection cannot exclude early syphilis. • Repeat screening can be considered in other clinical situations including inconclusive serology and ongoing risk of infection.
False-negative syphilis serology
• Treponemal screening tests are negative before a chancre develops and may be for up to 2 weeks afterwards. • Negative results within 3 months of infection cannot exclude early syphilis. • False-negative screening results may be seen in immunocompromised individuals. • A false-negative RPR test may occur in secondary or early latent syphilis due to the prozone phenomenon (false-negative result due to high antibody titres) when testing undiluted serum; in such cases negative tests on undiluted serum samples should be repeated on diluted samples .
55
This may be more likely to occur in individuals living with HIV.
56
False-positive syphilis serology
• Occasional false-positive results may occur with any of the serological tests for syphilis. • In general, false-positive reactivity is more likely in older individuals, those with autoimmune disease and people who inject drugs. • In the absence of symptoms of syphilis or a history of syphilis, transient or persistent reactivity in a single treponemal test should be considered to be a false-positive result.
• An EIA/CLIA detecting both IgM and IgG is the screening test of choice: 1B. • Positive screening tests should be confirmed with a different treponemal test and a second specimen for confirmatory testing obtained: 1B. • A quantitative RPR test should be performed when screening tests are positive: 1A. • Negative serological tests for syphilis should be repeated at 2 weeks after observation of possible chancres that are dark ground microscopy and/or PCR negative: 1B.
Management of complications and late symptomatic (tertiary) disease
Neurosyphilis: neurological complications
• T. pallidum can infect the central nervous system (CNS), and this can occur at any stage of syphilis and result in neurosyphilis.24,57,58 • Every patient with a positive serological test for syphilis and symptoms suggestive of neurological involvement (such as cognitive dysfunction, motor or sensory deficits, cranial nerve dysfunction or symptoms/signs of meningitis or stroke) should have a thorough neurological examination. If symptoms indicate, this may include ophthalmic and otological examination.
59
• In those without neurological symptoms, routine neurological examination rarely adds diagnostic value and is therefore not recommended.
59
Investigations for neurosyphilis
• Routine CSF assessment of patients without symptomatic disease (regardless of HIV status) is not recommended60,61: 1A. • The indications to perform a CSF examination remains an issue of debate. However CSF examination is indicated when there is clinical evidence of neurological involvement, except for ophthalmic or otological syphilis where it is rarely useful, irrespective of stage of disease62,63: 1C. • Some advocate CSF assessment in those who have serological failure (<4-fold decrease in the antibody titre of a non-treponemal test 6–12 months after treatment of early syphilis) and the sexual history suggests no interim re-infection1,64 (2D), in those who are serofast (persistence of stable antibody titre, of a non-treponemal test, 1–2 years after treatment of early syphilis), or where there is clinical suspicion. Robust data justifying these indications are lacking. In such cases pragmatic treatment to cover neurosyphilis may be opted for, meaning that results of a lumbar puncture will not change management decision-making unless other CNS diseases need to be excluded. Conversely, having a baseline CSF analysis may be useful for comparison if a patient’s symptoms do not resolve and a repeat lumbar puncture will need to be performed. • Prior to lumbar puncture: o Fundoscopy should be performed. o Computed tomography or magnetic resonance imaging should be considered if symptoms or signs are present.
63
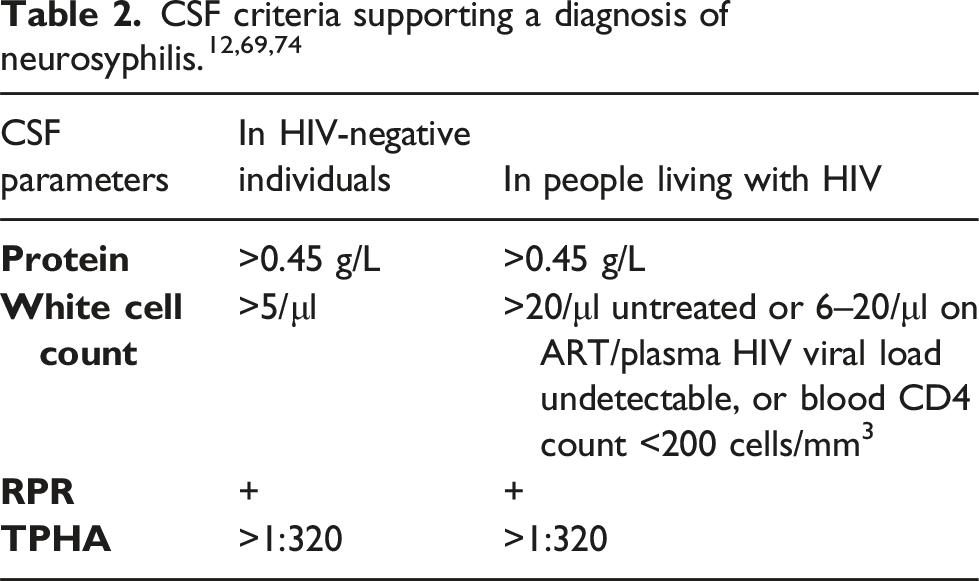
o Serum RPR titre does provide guidance as to whether a lumbar puncture should be undertaken. In a retrospective study of patients with latent syphilis, a negative VDRL test result in the peripheral blood was found to have 100% sensitivity in excluding CSF abnormalities compatible with the diagnosis of neurosyphilis, whereas a serum RPR titre of 1:32 has been demonstrated to be associated with CSF abnormalities similar to those seen in neurosyphilis.63,65 • Examination of CSF should include all the following (see Table 2): o Total protein o White cell count o A non-treponemal test (RPR) • Interpretation of CSF findings o No single test can diagnose neurosyphilis and similarly no CSF result can definitively exclude a diagnosis of neurosyphilis.60,62,66,67 The lack of a diagnostic gold standard means that studies use different definitions for neurosyphilis, and this limits the strength of the evidence base for informing recommendations. o CSF findings should be interpreted in the context of the clinical presentation of the patient and serological tests. o For accurate interpretation, it is vital that the CSF is not macroscopically contaminated with blood.
68
o While a raised protein level has been noted in neurosyphilis, a normal protein level is also possible.
69
o Most individuals who have symptomatic neurosyphilis have a raised white cell count (>5 cells/mm3) in the CSF,
70
although in cases of parenchymous neurosyphilis this may not be the case.
71
It can also be raised in a number of scenarios such as HIV infection in the absence of syphilis.66,69 o A positive CSF RPR in the absence of substantial blood contamination supports a diagnosis of neurosyphilis. Limited data suggest that the RPR may be slightly less sensitive than the VDRL in the CSF. CSF RPR is 51%–82% sensitive and 82%–100% specific. Given that the VDRL test is not available in the UK, CSF RPR testing is recommended. o The sensitivity of CSF VDRL is <50% in ocular syphilis and <10% in otosyphilis.
72
o Following the withdrawal of the TPPA assay from the UK, RPR testing is required. If CSF RPR is negative, consider performing TPHA if available and validated by the laboratory. A negative CSF TPHA test makes a diagnosis of neurosyphilis highly unlikely. A positive CSF TPHA test is highly sensitive for neurosyphilis but lacks specificity because reactivity may be caused by transudation of immunoglobulins from the serum into the CSF
73
or by leakage through a damaged blood–brain barrier resulting from conditions other than syphilis. o CSF TPHA titres can help to distinguish between higher antibody levels associated with neurosyphilis due to intrathecal antibody production and lower levels due to passive transfer from the blood. A CSF TPHA titre >1:320 is sensitive and specific for neurosyphilis and may be helpful in supporting the diagnosis of neurosyphilis when the CSF RPR is negative.74,75 o The evidence base for the use of T. pallidum PCR for diagnosing neurosyphilis is weak; studies are generally small and heterogenous due to lack of a diagnostic gold standard. In studies using a positive CSF VDRL to diagnose neurosyphilis, the sensitivity of the PCR varies between 40% and 70% and specificity between 60% and 100%. T. pallidum PCR is not recommended as a routine test.
76
o In people living with HIV without syphilis co-infection, CSF white blood count >5 cells/mm3 is associated with a CD4 count of ≤40 cells/mm3 or not taking antiretroviral therapy (ART). Therefore, a CSF pleocytosis in patients on ART, plasma HIV viral load <50 copies/ml and peripheral blood CD4 count >200 cells/mm3 are more likely to be due to neurosyphilis rather than HIV infection.
69
Investigations for cardiovascular syphilis
• The diagnosis of cardiovascular syphilis is made by the presence of the typical clinical features combined with positive syphilis serology after exclusion of other causes.
64
• Patients with suspected cardiovascular syphilis need to be assessed by a cardiologist. • In those without cardiovascular symptoms, a routine chest X-ray is not recommended.
77
Investigations for ophthalmic syphilis
• The diagnosis of ophthalmic syphilis is based on ophthalmic symptoms and signs combined with positive syphilis serology after exclusion of other causes.
64
• Clinical ophthalmic assessment should be considered in patients with secondary, early latent, tertiary and late latent syphilis, and a fundoscopy performed if any clinical ophthalmic symptoms are noted. • If ophthalmic syphilis is suspected, immediate referral to and management in collaboration with an ophthalmologist is crucial.
Investigations for otosyphilis
• The diagnosis of otosyphilis is made by the presence of audiological symptoms, such as new hearing loss, tinnitus or vertigo, combined with positive syphilis serology after exclusion of other causes.
64
• Otosyphilis is one of the potentially reversible causes of hearing loss.
78
• If otosyphilis is suspected, immediate referral to and management in collaboration with an audiologist or ear, nose and throat specialist is important.
Investigations for gummata
• Diagnosis of syphilitic gummata is usually made on clinical grounds: typical nodules/plaques or destructive lesions in individuals with positive syphilis serology. • Histological examination of a lesion may suggest this diagnosis and T. pallidum may be identified within the nodules by PCR.
7
• Those with positive syphilis serology and possible neurological, ophthalmic, otological, cardiovascular or gummatous symptoms or signs require examination and further evaluation by appropriate specialists: 1C.
General advice and considerations
• All patients should be offered holistic sexual healthcare including screening for other STIs including HIV, appropriate vaccinations including hepatitis B and HPV, and HIV pre- and post-exposure prophylaxis, as appropriate. • All patients should be provided with detailed information about syphilis, including the long-term implications for their health and that of their partners/families. This should be reinforced with clear and accurate written information. • There is very little evidence to inform advice about the recommended duration of sexual abstinence following treatment, however patients should be advised to refrain from sexual contact of any kind until 2 weeks following treatment completion. • Robust evidence for the optimal management of complications and tertiary syphilis, justifying the antimicrobial agent, dose and duration of treatment, is lacking.79,80 • The recommendations are based mainly on laboratory considerations, biological plausibility, expert opinion, case studies and clinical experience. • For treatment of neurosyphilis, a treponemicidal level of an antimicrobial should be achieved in serum/CSF. A penicillin level of >0.018 mg/L is considered treponemicidal, but a higher concentration might be preferable for more rapid elimination of treponemes. The maximal elimination effect is attained at a level of 0.36 mg/L. The level of antimicrobial agent should be treponemicidal for at least 7 days to cover several treponemal division times (30–33 h) in early syphilis with a sub-treponemicidal interval of not more than 24–30 h. Longer duration of treatment is given in late syphilis based on more slowly dividing treponemes in late syphilis. Treponemes may persist despite apparently successful treatment indicating that some treponemes may be ‘resting’ or dividing very slowly.79,81,82 • In the case of neurosyphilis, the aim of treatment is to prevent further progression or sequelae and biological plausibility suggests that regimens that achieve treponemicidal levels of an antimicrobial in the CSF should be the treatment of choice.
83
• If treatment for neurosyphilis is interrupted for more than 24 h the course should be re-started; this is because of the need to maintain continuous CSF treponemicidal levels of treatment throughout the course. • Parenteral rather than oral treatment has been the treatment of choice because therapy is supervised and bioavailability is guaranteed. • Benzathine penicillin G should not be used for neurosyphilis because it does not reliably achieve sufficient concentrations in CSF.84–89 Although both benzathine penicillin G and standard regimens of procaine penicillin G do not achieve treponemicidal levels in CSF and CSF involvement is common in early syphilis, CSF abnormalities are uncommon after recommended treatment of early syphilis. The prevalence of late syphilis remains low indicating that treatment is effective and suggesting that host immune responses in early syphilis have an essential role. A single dose of 2.4 MU benzathine penicillin G in patients with asymptomatic neurosyphilis showed a CSF relapse rate of 21% which was twice that of other penicillin preparations.
90
• Intravenous (IV) administration of aqueous crystalline penicillin G or intramuscular (IM) procaine penicillin combined with oral probenecid are the treatments of choice in neurosyphilis. Data comparing these two options are lacking.1,64,82 • Within the UK, procaine penicillin with probenecid (QDS) is the preferred treatment option for neurosyphilis, in the USA it is considered an acceptable alternative to admission and intravenous therapy.1,91 • To cover the longer division times in late syphilis, a ‘safety margin’ is provided by giving parental regimens lasting 10–21 days. In the UK, a duration of 14 days is used. • Non-penicillin antibiotics that have been evaluated include doxycycline, erythromycin and azithromycin. Doxycycline has been evaluated more than any other non-penicillin antibiotic but all studies have been observational and retrospective. Doxycycline has superseded the older tetracyclines; although 100 mg once (OD) or twice daily (BD) for 14 days is effective,92–96 failure of doxycycline OD has been reported.92,97,98 Erythromycin is not effective as it does not effectively penetrate the CSF or placental barrier.
99
Azithromycin has shown good treponemicidal activity in animal studies and several controlled studies.100,101 However, rapid emergence of resistance to azithromycin with clinical failure has been described in several studies which appears to be linked to intrinsic macrolide resistance in some strains of T. pallidium.102,103 • Several different ceftriaxone regimens have been shown to be effective for the treatment of early syphilis.104–113 • Linezolid has been shown to be an effective treatment in animal models of syphilis but there have been no human trials to date.
114
• Benzathine penicillin G is recommended as first-line treatment for syphilis, and penicillin resistance has never been reported despite decades of use. Previously, macrolides have been recommended as an alternative treatment to penicillin. Macrolide resistance is mediated by a point mutation at either position A2058 G or A2059 G in the 23S rRNA gene. Macrolide resistance and treatment failure have emerged rapidly worldwide, possibly selected by widespread macrolide use. Hence macrolides are no longer recommended as a treatment option for syphilis.115–117 • Treatment of neurosyphilis in patients with significant penicillin allergy is challenging, and penicillin desensitisation is probably the best option. Ceftriaxone (2 g/day IM or IV for 10–14 days) should be explored as an alternative, but evidence of its efficacy is limited.106,110,118,119 Risk of cross-reactivity between penicillin and ceftriaxone is low, but skin testing for β-lactam allergy and desensitisation can be done if needed. Cardiovascular and neurological lesions may progress despite adequate treatment for syphilis. • Patients with soya or peanut allergy should be referred for allergy testing or treated with procaine penicillin or ceftriaxone.
• All patients with syphilis should receive holistic sexual healthcare: 1A. • Patients should be given a clear explanation of their diagnosis of syphilis and its implications, reinforced with written information: 1D. • Patients with early, infectious syphilis should be advised to abstain from sexual contact until all lesions (if any) have resolved or until 2 weeks after treatment completion: 1C. • Parenteral treatment with the appropriate penicillin preparation is the treatment of choice: 1B. • Macrolide antibiotics are not recommended due to antimicrobial resistance and inability to reliably cross the placenta and blood–brain barrier: 1B.
The Jarisch–Herxheimer reaction
• The Jarisch–Herxheimer reaction can occur in late syphilis and can be potentially life threatening if there is involvement of critical sites (e.g. coronary ostia, larynx and CNS).1,64,120–122 • The pathogenesis of the Jarisch–Herxheimer reaction remains poorly understood and the value of steroids in prevention of this reaction remains unclear. It has been reported that corticosteroids may exert a positive effect, but the data are not conclusive.120–122 No clinical trials have compared the benefits of steroid treatment and timing of steroid therapy. • There is evidence to suggest that prednisolone can prevent the febrile episode of the Jarisch–Herxheimer reaction and it is biologically plausible that steroids may help to prevent the wider complications of the reaction. • It has been suggested that early steroids may prevent both the Jarisch–Herxheimer reaction and clinical deterioration of symptoms such as optic neuritis and uveitis, neuroretinitis and cochleovestibular dysfunction.123–125
Follow-up
• Follow-up examination of CSF should be performed 6 weeks to 6 months after treatment of neurosyphilis to monitor the decrease in white blood cell count and protein level1,64: 2D. • Limited data suggest that routine CSF measurement can be avoided in patients with satisfactory reduction of serum RPR titres.37,126
Management of syphilis in individuals living with HIV
Clinical features
• Clinical features of syphilis are generally no different in people living with HIV from those in HIV-negative individuals although there are many case reports of more florid manifestations in people with HIV.22,127,128 • People living with HIV are at increased risk of re-infection with syphilis; this observation may be related to risk behaviour
129
although some experts have suggested a different immunological response.
130
Further research is necessary to investigate this. Being on ART does not increase the risk of contracting syphilis. • In people living with HIV, risk of neurological or ophthalmic complications in early syphilis appears be like the risk in those without HIV; there is not enough evidence to assess the risk of these complications in late syphilis. • Studies have shown that co-infection with syphilis is associated with a transient decrease in CD4 count and increase in viral load
131
; however, most studies were conducted when indications for starting ART were different from today. For the last few years, most people living with HIV have been taking effective ART and hence the effect of co-infection with syphilis on these parameters needs to be re-evaluated. Conversely, in a more recent meta-analysis, Seña et al. found no association between CD4 count, HIV viral load or ART and serological treatment failure.
132
Diagnosis
• There are no differences in the serological diagnostic algorithms specifically for people living with HIV. • Unusual serological patterns such as false-negative test results and delayed seroreactivity are seen rarely.
133
• Diagnosis of neurosyphilis in people living with HIV is complicated by pleocytosis and elevated CSF protein levels seen in individuals with asymptomatic HIV. Indications for CSF examination in people living with HIV are the same as those for HIV-negative individuals: 1B. Some experts suggest that CSF examination should be performed in people living with HIV with a high RPR titre (≥1:32) and/or those with a low CD4 count (<350 cells/mm3).
Treatment
• Most experts and guidelines recommend the same treatment regimens/protocols as for HIV-negative individuals.
94
For all stages of syphilis, there is no evidence to suggest that people living with HIV need to be treated differently compared to HIV-negative individuals134–138: 1B. • Prolonged treatment or additional antibiotic therapy has not been associated with significantly better outcomes.138,139 • There are limited studies looking at the efficacy of non-penicillin regimens in people living with HIV but for non-tertiary presentations doxycycline appears as effective as penicillin.
140
• The post-treatment non-treponemal serological response is delayed at 6 months as compared to individuals without HIV but this difference is not significant at 12 months after treatment.128,141,142 • People living with HIV on ART have reduced serological failure rates.
143
• People living with HIV who are allergic to penicillin should be managed in the same way as those without HIV co-infection.
Follow-up
• The serological response in people living with HIV may be slower than in those without HIV, standard follow-up is recommended, wherever possible to coincide with follow-up visits for HIV care: 1B. • Routine syphilis serological screening for people living with HIV at 6-monthly interval is recommended
144
: 1B.
Recommended regimens
Potentially incubating syphilis/epidemiological treatment
1. Benzathine penicillin G 2.4 MU IM single dose: 1C. 2. Doxycycline 100 mg orally (PO) BD for 14 days: 1C.
Early syphilis (primary, secondary and early latent)
Late latent, cardiovascular and gummatous syphilis
Neurosyphilis including neurological involvement in early syphilis
1. Procaine penicillin 1.8–2.4 MU IM OD PLUS probenecid 500 mg PO QDS for 14 days 1,64,91,152: 1C. 2. Benzylpenicillin 10.8–14.4 g OD, given as 1.8–2.4 g IV every 4 h for 14 days1,64,152: 1C. • Alternative regimens: 1. Ceftriaxone 2 g IM or IV for 10–14 days91,104–106,110,118,153: 2D. 2. Doxycycline 200 mg PO BD for 28 days
98
: 2D. 3. Amoxycillin 2 g PO TDS PLUS probenecid 500 mg PO QDS for 28 days
151
: 2D. • Steroids should be given with all anti-treponemal antibiotics for neurosyphilis; 40–60 mg prednisolone OD for 3 days starting 24 h before the antibiotics.
Syphilis in individuals living with HIV
• Treatment as appropriate for the stage of infection; individuals with HIV to be given the same treatment regimens as HIV-negative individuals: 1B.
Treatment interruptions for late syphilis
• A single dose of benzathine penicillin G 2.4 MU produces consistently treponemocidal blood levels of penicillin for 2–4 weeks so additional doses are not required if any subsequent doses are received within 14 days of the previous dose.
79
• When treating neurosyphilis, continuous treponemicidal levels are required within the CNS throughout the treatment course, so if treatment is interrupted for more than 24 h the course should be re-started:1B.
Preparation of IM penicillin injections
• IM benzathine penicillin is more tolerable to the patient if diluted with lidocaine which is now licensed in the UK, so this preparation is recommended: 1D.
Reactions to treatment
• Patients should be warned of possible reactions to treatment. Facilities for resuscitation should be available in the treatment area. All patients should be kept on clinic premises for 15 min after receiving their first injection to observe for immediate adverse reactions. In addition, patients should be advised to seek urgent medical attention if they experience symptoms or signs of an allergic reaction: shortness of breath, itchy wheals on their skin, facial swelling or tightness in their chest or throat. • Jarisch–Herxheimer reaction (see above). • Procaine reaction (also known as procaine psychosis, procaine mania or Hoignes syndrome) is due to inadvertent IV injection of procaine penicillin. It is characterised by fear of impending death and may cause hallucinations or fits immediately after injection; it lasts less than 20 min. Calm, verbal reassurance is required. Management of seizures is as per local practice. • Facilities for the treatment of anaphylaxis should be available. Standard treatment protocols for the management of anaphylactic shock should be followed. • Penicillin desensitisation should be considered for patients reporting a history of penicillin allergy.154,155 Many people reporting penicillin allergy will not display hypersensitivity on re-exposure to penicillin because either the hypersensitivity has resolved or they were never allergic to penicillin. A careful history may help to identify the latter group • Patients with soya or peanut allergy should be referred for allergy testing or treated with procaine penicillin or ceftriaxone.
• Advise patients of possible or common reactions to treatment and, after administering parenteral therapy, observe for immediate reactions to treatment: 1C. • Steroid therapy is recommended when managing neurological (both early and tertiary) or cardiovascular syphilis to prevent potentially serious consequences of the Jarisch–Herxheimer reaction: 40–60 mg prednisolone OD for 3 days starting 24 h before anti-treponemal antibiotics: 1D. • Consider skin testing and subsequent penicillin de-sensitisation and treatment for those reporting allergy: 2A.
Management of sexual partners
• Specialist skills in gathering detailed, sensitive information are required for effective partner notification. • Partner notification should be discussed at the time of diagnosis by a trained healthcare professional with all patients with a diagnosis of syphilis. Where the outcome is not resolved at initial interview, there should be documented attempts to re-interview the patient in order to offer further support and gain further information to verify outcomes. A multidisciplinary team approach should be encouraged to ensure that partner notification is discussed with patients at all treatment/follow-up visits if necessary. • For patients with primary syphilis, sexual partners within the last 3 months should be notified as the incubation period is up to 90 days. Partner notification may need to be extended to 2 years for patients with secondary syphilis, clinical relapse or early latent syphilis. Sexual partners of those diagnosed with tertiary syphilis should be evaluated clinically and undergo serological testing, and receive treatment if necessary based on the results. • Of contactable sexual partners of patients with early syphilis, 46%–60% will also have the infection.
6
• Where it may be difficult for sexual contacts to be identified due to anonymity, service links offering screening and advice with venues such as ‘sex on premises’ and internet sites may be useful. • Individuals who are sexual contacts of a patient with early syphilis but are asymptomatic should be offered either epidemiological treatment or re-screening for syphilis 12 weeks after their last exposure. • In latent syphilis attempts should be made to locate any previous serology or documented treatment that would aid disease staging. This should then inform partner notification. Individuals with late latent syphilis are usually unable to transmit the infection to sexual partners. Although mother-to-child transmission may occur many years after initial infection, this becomes unusual as time progresses and after the early stage of syphilis. Unless the timeframe during which infection occurred can be determined, it is reasonable for sexual partners of, and children born to, women diagnosed with late latent syphilis of unknown duration to undergo screening. • Ways in which people meet sexual partners constantly change, therefore it is important that those who carry out partner notification should ensure they adapt, develop and update methods as necessary. • All patients should be offered patient and provider referral as a method of contacting any sexual partners. Use of electronic means of contact should also be considered (e.g. internet, app and text) for partner notification. The method agreed upon with the patient should be clearly documented and revisited at follow-up as necessary. Revisiting partner notification should be seen as a multidisciplinary responsibility as the patient may not see the same member of staff on different visits. • Further details can be found in the BASHH partner notification statement.
156
• Partner notification should be discussed with all patients at diagnosis, with re-interview if required. Different options for contacting partners should be fully explored to ensure optimum results. The ‘look back’ period should be appropriate for the stage of syphilis: 1B. • Epidemiological treatment should be offered for asymptomatic contacts within the window period: 1B.
• The purpose of follow-up is to identify re-infection and document effective treatment and partner notification. • It may take a number of months for the non-treponemal titres to drop 4-fold following treatment, particularly following treatment of re-infection. • Clinical and serological (RPR tests) follow-up is recommended at 3, 6 and 12 months then, if indicated, six monthly until RPR negative or serofast. • A sustained 4-fold or greater increase in the RPR titre suggests re-infection or treatment failure. Treatment failure is characterised by: o Four-fold or greater increase in non-treponemal test titre o Recurrence of signs or symptoms o Exclusion of re-infection • Specific treponemal tests usually remain positive throughout life following effective treatment; clear documentation is necessary to prevent unnecessary retreatment, and patients advised. • Re-infection should be retreated and sexual partners should be screened and epidemiological treatment considered. • Studies have shown retreating serofast serology does not show improvement in respone.
157
• In those with concomitant HIV infection, initial follow-up is as detailed above (coinciding with HIV follow-up visits).
• Minimal recommended follow-up with syphilis serology is three monthly for 6 months then at 12 months and, if indicated (e.g. HIV co-infection), six monthly or until serofast: 1D.
Auditable outcomes
• The percentage of confirmed syphilis cases having a record of an RPR titre obtained at treatment (standard 97% confirmed syphilis cases). • The percentage of confirmed syphilis cases having fully adhered to a recommended treatment (standard 97% confirmed syphilis cases). • The percentage of cases having the outcome of (an) agreed contact action(s), or the decision not to contact, documented for all contacts, within the appropriate look back interval (see https://www.bashh.org/resources/100/2012_bashh_statement_on_partner_notification_for_sexually_transmissible_infections) (standard 97% confirmed syphilis cases). • The percentage of confirmed syphilis cases having a record of an RPR titre obtained 6 months post-treatment (standard 65% confirmed syphilis cases).
Editorial independence
• These guidelines were commissioned and edited by the BASHH CEG, without external funding being sought or obtained.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.