
Abstract
Background
Hepatitis C virus (HCV) coinfection is common among people living with HIV (PLWH) and is associated with adverse outcomes. However, the specific association between HCV coinfection and the risk of acute myocardial infarction (AMI) in PLWH remains unclear. This systematic review and meta-analysis aims to clarify this relationship.
Method
We searched MEDLINE and EMBASE databases from inception to October 2024 for cohort studies comparing the incidence of AMI in PLWH with HCV coinfection versus PLWH without HCV coinfection (HIV mono-infection). We used the generic inverse variance method with a random-effects model to pool risk ratios (RRs) and 95% confidence intervals (CIs). Heterogeneity was assessed using the I2 statistic. All statistical analyses were performed using Review Manager 5.4.
Results
Seven cohort studies, encompassing 94,664 participants (mean age 42 years, 83% male), met the inclusion criteria. HCV coinfection was associated with a significantly increased risk of AMI in PLWH (pooled RR = 1.25, 95% CI: 1.09, 1.44; I2 = 18%; p < .001) compared to HIV mono-infection. A subgroup analysis restricted to type 1 AMI was not statistically significant (pooled RR = 1.03, 95% CI: 0.84, 1.26; p = .78).
Conclusions
HCV coinfection is associated with a significantly increased risk of AMI in PLWH. Further research is needed to determine the pathophysiology of this relationship.
Key learning points
What is already known on this topic
• People living with HIV (PLWH) are at an increased risk of cardiovascular disease • Hepatitis C virus (HCV) coinfection is common among PLWH and is associated with adverse health outcomes. • The specific relationship between HCV coinfection and acute myocardial infarction (AMI) risk in PLWH has been unclear, with conflicting findings in previous studies.
What this study adds
(1) HCV coinfection is associated with a 25% increased risk of AMI in PLWH (pooled RR 1.25, 95% CI: 1.09, 1.44) compared to PLWH without HCV. (2) The association between HCV coinfection and AMI risk in PLWH remains significant even after sensitivity analysis, with a 35% increased risk (pooled risked ratio (RR) 1.35, 95% CI: 1.16, 1.56). (3) The findings emphasize the importance of addressing HCV coinfection as part of comprehensive care for PLWH to potentially reduce cardiovascular risk
Introduction
The coexistence of Hepatitis C virus (HCV) and Human Immunodeficiency Virus (HIV) infections presents a significant public health challenge, with HCV coinfection being prevalent among people living with HIV (PLWH), with prior literature estimating prevalence from 25 to 50%.1,2 Globally, over 38 million people are living with HIV, 3 resulting in least 47 million disability adjusted life years (DALYs) loss. 4 Complications from HIV can and should be prevented from this deliberating disease. People with HIV (PWH) are at an increased risk of cardiovascular disease (CVD), 5 although the additional impact of HCV coinfection remains a subject of debate. As antiretroviral therapy has improved the life expectancy of PLWH, there has been a notable shift in mortality patterns, 6 with non-AIDS-related causes, including cardiovascular disease, becoming increasingly prominent. Hepatitis C virus infection has been associated with increased acute myocardial infarction (AMI) risk in PLWH,7–10 although evidence remains disputed.11–13
The inconsistent results from individual studies highlight the need for a comprehensive synthesis of available evidence to elucidate the relationship between HCV coinfection and AMI risk in PLWH. This systematic review and meta-analysis aim to critically evaluate and synthesize the existing literature on the impact of HCV coinfection on AMI risk in PLWH. We aim to consolidate data from eligible studies, and seek to provide a clearer understanding of this association, which may inform clinical management strategies and guide future research directions in this field.
Methods
Search strategy
Summary of studies investigating the risk of myocardial infarction in HIV patients with Co-HCV infection.
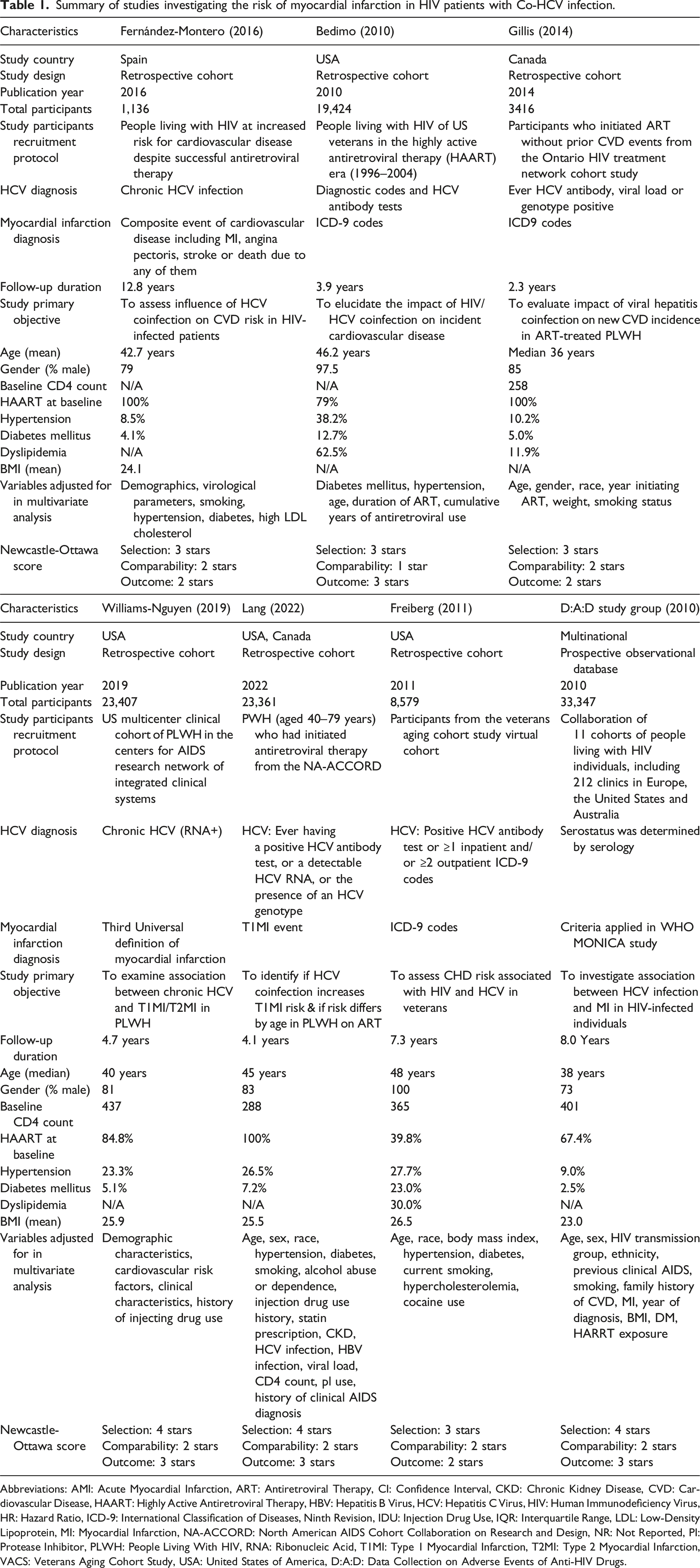
Abbreviations: AMI: Acute Myocardial Infarction, ART: Antiretroviral Therapy, CI: Confidence Interval, CKD: Chronic Kidney Disease, CVD: Cardiovascular Disease, HAART: Highly Active Antiretroviral Therapy, HBV: Hepatitis B Virus, HCV: Hepatitis C Virus, HIV: Human Immunodeficiency Virus, HR: Hazard Ratio, ICD-9: International Classification of Diseases, Ninth Revision, IDU: Injection Drug Use, IQR: Interquartile Range, LDL: Low-Density Lipoprotein, MI: Myocardial Infarction, NA-ACCORD: North American AIDS Cohort Collaboration on Research and Design, NR: Not Reported, PI: Protease Inhibitor, PLWH: People Living With HIV, RNA: Ribonucleic Acid, T1MI: Type 1 Myocardial Infarction, T2MI: Type 2 Myocardial Infarction, VACS: Veterans Aging Cohort Study, USA: United States of America, D:A:D: Data Collection on Adverse Events of Anti-HIV Drugs.
Eligibility criteria
Studies were included in this meta-analysis if they met the following criteria: they were cohort studies (either prospective or retrospective) investigating the association between HCV coinfection and incident acute myocardial infarction (AMI) in people living with HIV (PLWH). Included studies were required to have a clearly defined group of PLWH with HCV coinfection (confirmed by serological testing for HCV antibodies or detection of HCV RNA) and a comparator group consisting of PLWH without HCV coinfection (HIV mono-infection). The outcome of interest, incident AMI, needed to be defined using established criteria, including clinical presentation, electrocardiographic findings, and/or elevation of cardiac biomarkers. Finally, studies must have reported a risk ratio (RR), hazard ratio (HR), or odds ratio (OR), along with a corresponding 95% confidence interval (CI), or provided sufficient data to allow for the calculation of these effect sizes. Studies that did not fulfill all of these criteria were excluded.
Data extraction
A standardized, pre-piloted data extraction form was developed and utilized by two independent investigators (PD and NS) to systematically extract relevant information from each included study. The extracted data encompassed study characteristics, participant demographics, methodological details, and outcome data. Specifically, we recorded the first author’s last name, publication year, study country, and study design (prospective or retrospective). We extracted the total number of participants, as well as the number in each comparison group (HCV coinfected and HIV mono-infected), and details regarding the participant recruitment protocol. We documented the specific criteria used for diagnosing both HIV and HCV infection, and the criteria used to define and ascertain AMI events. We also extracted the duration of follow-up, the mean or median age of participants, and the percentage of male participants. Covariates utilized in each study were recorded. For each study, we extracted the reported effect estimate (RR, HR, or OR) and its associated 95% CI for the association between HCV coinfection and incident AMI. If adjusted and unadjusted effect estimates were reported, we extracted both, prioritizing the adjusted estimate for the primary analysis. Discrepancies in data extraction between the two investigators were resolved through discussion and consensus, and, if necessary, consultation with a third investigator (TSu). Two investigators (PD and NS) applied the Newcastle-Ottawa Scale for cohort studies to evaluate research quality, focusing on the quality of participant recruitment, comparability between groups, and accuracy of outcome ascertainment. 14
Statistical analysis
Data analysis was conducted using Review Manager 5.4 software from the Cochrane Collaboration. Point estimates with standard errors from each study were combined using DerSimonian and Laird’s generic inverse variance method. 15 Due to heterogeneous background populations and protocols among the studies, a random-effects model was employed. Statistical heterogeneity was assessed using Cochran’s Q test, supplemented by I2 statistics to quantify the proportion of total variation across studies attributable to heterogeneity rather than chance. I2 values categorize heterogeneity as insignificant (0%–25%), low (26%–50%), moderate (51%–75%), or high (>75%). 16 A funnel plot will be utilized to examine potential publication bias if sufficient studies are available.
Results
We reported our findings following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Our search strategy identified 800 studies (701 from EMBASE and 99 from PUBMED). After removing 55 duplicates, we reviewed those studies by title and abstract, excluding 731 studies that did not meet the eligibility criteria related to study design, participants, or article type. Subsequently, we thoroughly reviewed 14 articles and excluded seven for not reporting the relevant outcome.17–23 Ultimately, seven studies met the eligibility criteria for our meta-analysis.7–13 Figure 1 illustrates our search methodology and selection process, and Table 1 details the characteristics and quality assessment of the included studies. Prisma diagram and study selection flowchart.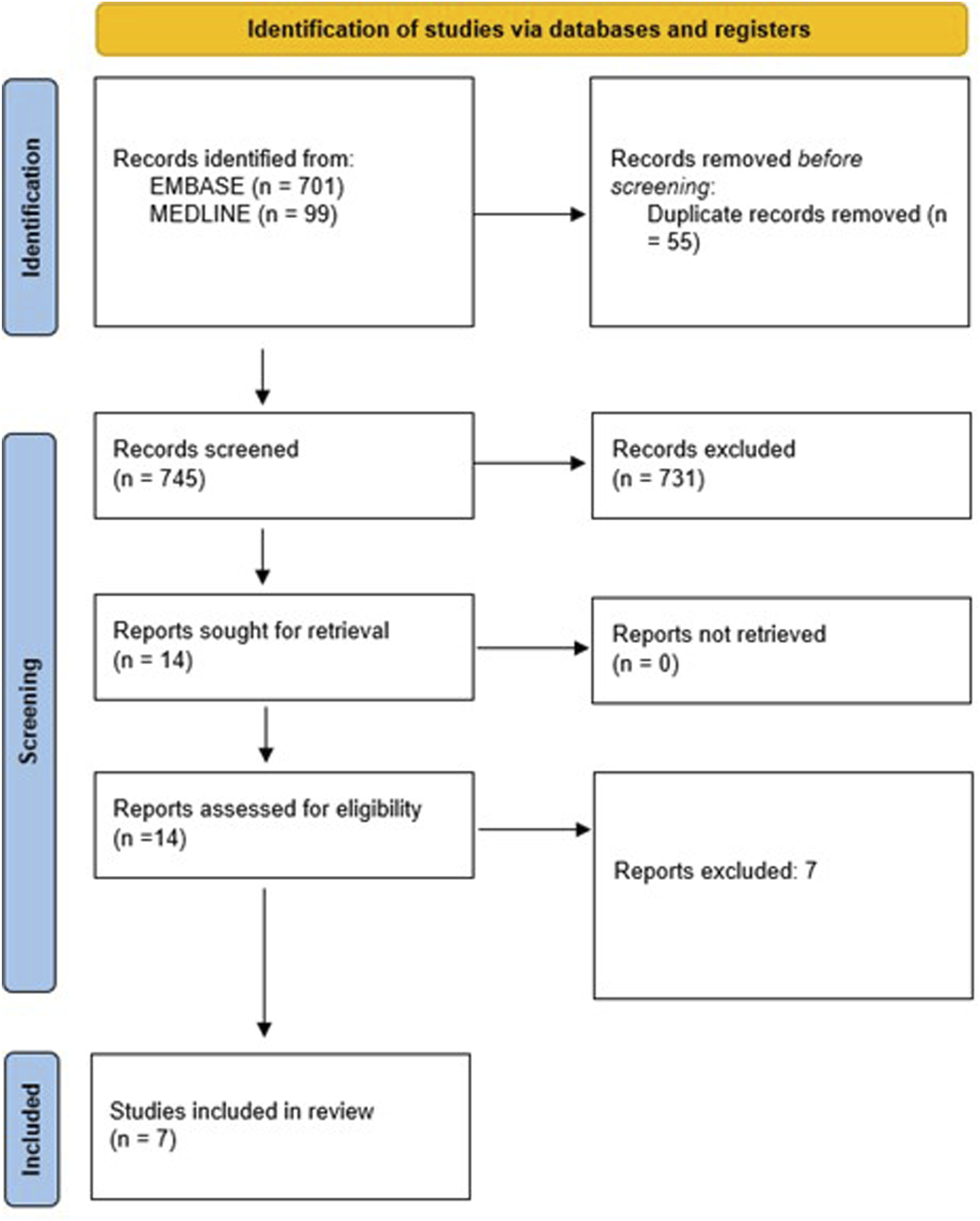
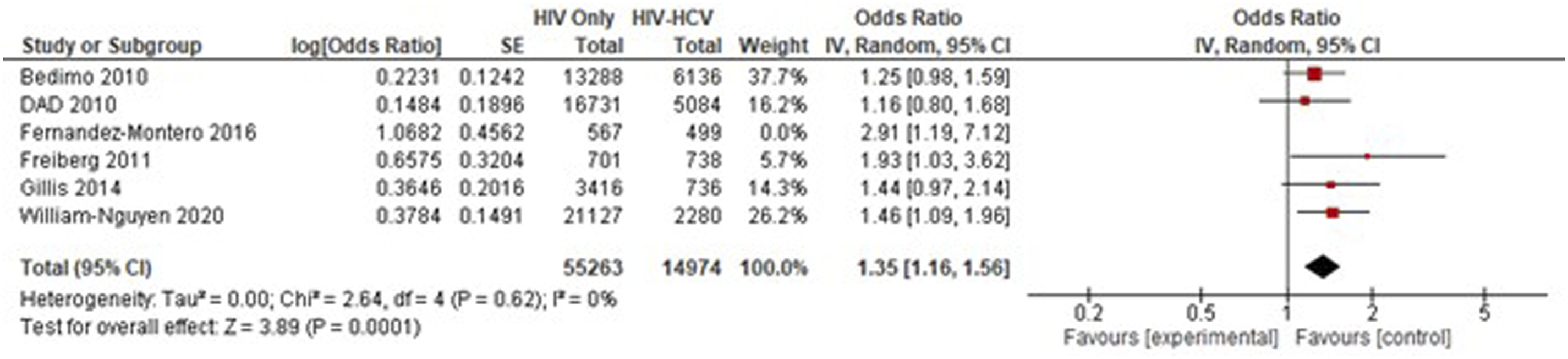
A total of seven cohort studies with 94,664 participants investigated the association between HCV and AMI. The average participant age was 42 years old and 83% were male as shown in Table 1. Of note, all seven studies are from developed countries. Further demographic and clinical characteristics of the study populations, such as baseline CD4 counts, HIV viral load status, hypertension and other co-morbidities, are detailed in Table 1 and provide a more comprehensive understanding of the cohorts. The pooled analysis of all seven studies showed that HCV coinfection was associated with a significantly increased risk of AMI in PLWH compared to HIV mono-infection (pooled RR = 1.25, 95% CI: 1.09, 1.44; p < .001; I2 = 18%; Figure 2), when compared to HIV individuals without HCV disease. Minimal statistical heterogeneity was observed (I2 = 18%). Subgroup analysis, focusing only type 1 myocardial infarction, revealed non-statistical results (pOR 1.03, 95% CI: 0.84, 1.26; p = .78, Figure 3). Sensitivity analysis, removing Lang et al. study due to its focus on type 1 myocardial infarction as the specific outcome, revealed a statistically significant pooled increased risk of myocardial infarction (pooled OR 1.35, 95% CI: 1.16, 1.56; p < .001, Figure 4) with no statistical heterogeneity (I2 = 0%). Pooled analysis of the included study. Subgroup analysis of Type-1 myocardial infarction. Pooled analysis with sensitivity analysis.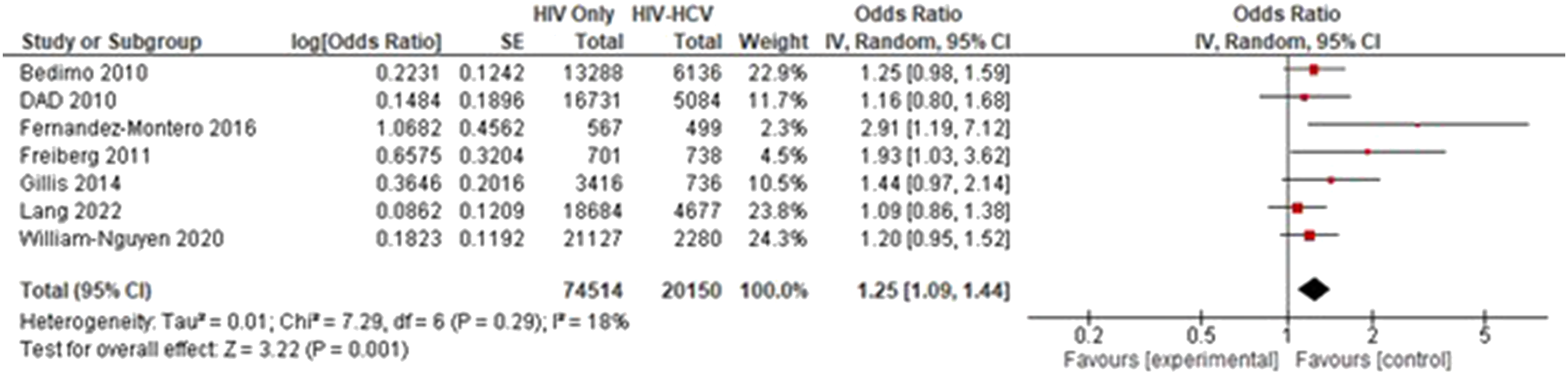

Discussion
This current study is the largest systematic review and meta-analysis to consolidate data on how HCV coinfection in PLWH affects risk of incident AMI. The pooled analysis indicated that PLWH with coinfected HCV have 25% higher risk of AMI event compared to individuals without HCV coinfection. This finding highlights the importance of considering HCV status in cardiovascular risk assessment for PLWH.
The pathogenesis of cardiovascular disease is significantly influenced by endothelial dysfunction. 24 Hepatitis C virus (HCV) has been shown to directly infect and replicate within vascular endothelial cells, contributing to this dysfunction. 25 First, HCV induces the oxidative stress by disrupting the balance between reactive oxygen species (ROS) and antioxidant defenses. 26 Furthermore, HCV infection promotes a chronic inflammatory state characterized by elevated levels of pro-inflammatory cytokines, 27 exerting systemic effects beyond the hepatic environment, as seen in the thickening of the intima-media and plaque in people with HCV. 28 In addition, HCV can interfere with insulin signaling, potentially leading to insulin resistance and diabetes, 29 while simultaneously altering lipid metabolism towards a more atherogenic profile.
Co-infection with both viruses may create a synergistic effect, exacerbating systemic inflammation, accelerating the atherosclerotic process, and increasing the likelihood of plaque rupture. 30 While our subgroup analysis investigating type 1 myocardial infarction did not reach statistical significance, the potential role of HCV in sepsis-induced myocardial dysfunction warrants consideration. HCV infection can trigger systemic inflammatory response syndrome (SIRS) or sepsis, potentially leading to demand ischemia and consequent myocardial injury. 31 The heightened risk of AMI in PLWH with concurrent HCV infection likely arises from a complex interplay of chronic inflammation, immune dysregulation, and traditional cardiovascular risk factors. Chronic HCV infection is marked by persistent systemic inflammation, evidenced by elevated levels of IL-6 and TNF-α. 32 This chronic inflammatory state, particularly in the context of HIV-associated immune activation, can significantly contribute to endothelial dysfunction, an early and critical step in atherogenesis and thus causing the higher risk of myocardial infarction. The mean age of the cohorts in this meta-analysis (42 years) is younger than the typical age of AMI onset globally; however, HIV infection itself is a risk factor for premature cardiovascular disease. The follow-up durations in the included studies should be considered in this context, as longer follow-up might reveal different patterns.
This study has several limitations. First, the observational nature of the included cohort studies limits our ability to infer causality. Second, although we extracted data on covariates adjusted for in the original studies, there was considerable variability in the adjustment strategies used. Some studies may not have adequately controlled for important confounders, such as traditional cardiovascular risk factors (hypertension, smoking, diabetes, dyslipidemia), HIV-specific factors (ART regimens, duration of HIV infection, CD4 count, viral load), and substance use (particularly injection drug use, which is a strong risk factor for both HCV and CVD). This residual confounding could potentially overestimate the true effect of HCV coinfection. Third, the definitions of HCV infection and AMI varied across studies, which could introduce some heterogeneity. Fourth, all included studies originated from high-income or developed countries, which may influence the generalizability of these findings. Finally, we were unable to assess publication bias due to the small number of included studies.
Conclusion
This meta-analysis provides strong evidence that HCV coinfection is associated with a significantly increased risk of AMI in PLWH. These findings underscore the importance of routine HCV screening and treatment in PLWH as part of a comprehensive cardiovascular risk management strategy. Specifically, cardiovascular risk assessments for people living with HIV should thoroughly consider the status of HCV infection, whether acute, chronic, or previously treated, to ensure a comprehensive evaluation and appropriate preventative measures. While HCV eradication with direct-acting antivirals (DAAs) has been shown to improve metabolic and inflammatory markers, further research, particularly prospective studies, is needed to determine whether DAA therapy reduces AMI risk in this population.
Supplemental Material
Supplemental Material - Hepatitis C increases acute myocardial infarction risk in people living with HIV: A systematic review and meta-analysis
Supplemental Material for Hepatitis C increases acute myocardial infarction risk in people living with HIV: A systematic review and meta-analysis by Thanathip Suenghataiphorn, Narisara Tribhuddharat, Pojsakorn Danpanichkul, Thitiphan Srikulmontri, and Narathorn Kulthamrongsri in International Journal of STD & AIDS.
Footnotes
Author contributions
Conceptualization – TSu, NK, Data curation – TSu, Formal analysis – TSu, Funding acquisition – N/A, Investigation (Search) – TSr, NT, Investigation (Ottawa Scoring) – PD, NT, Methodology & Validation – TSu, Writing, original draft – TSu, NT, Finalized the manuscript – TSu , PD, All authors have read and approved the final version of the manuscript for submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Supplemental Material
Supplementary Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.