
Abstract
Background
Sexual Health Hounslow completed targeted outreach in local asylum seeker populations. The methods and results of STI and BBV screening in this population are described.
Methods
A dedicated clinic 0.4 miles from the largest contingency hotel opened in January 2023, advertised through targeted hotel-based outreach. A hotel-based clinic opened in 2024.
A retrospective case-note review of all asylum seekers attending sexual health services in Hounslow between 01/02/2011 and 01/12/2023 was conducted.
Results
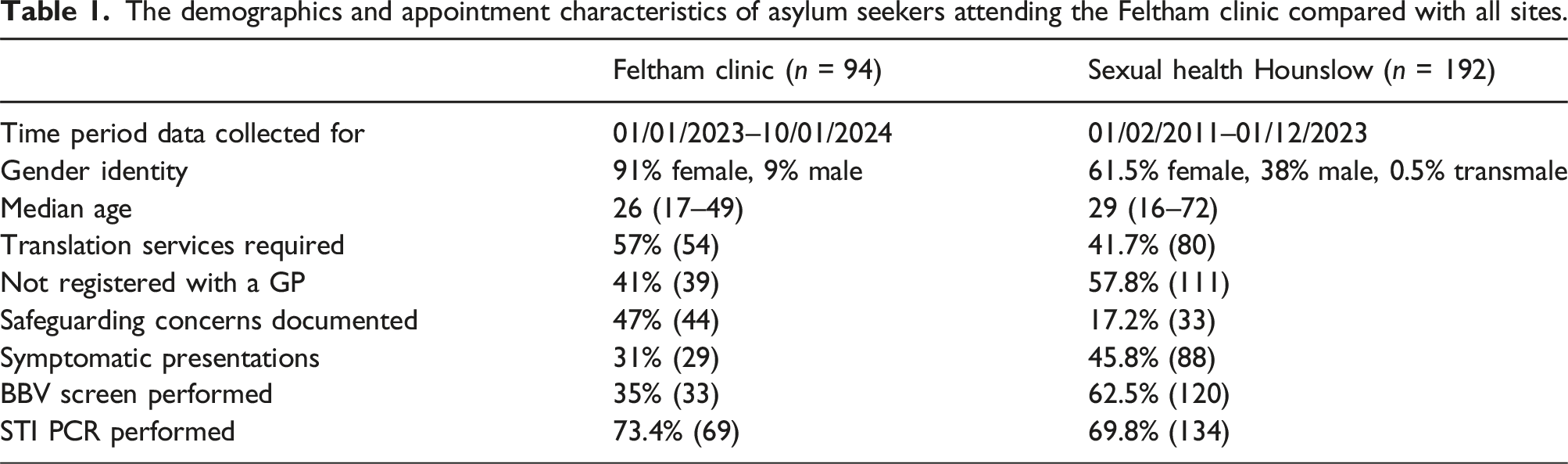
192 asylum seekers were included. 80 (41.7%) required translators. 111 (57.8%) were not registered with a GP. Thirty-three (17.2%) had a safeguarding concern. Eleven (9.2%) service users tested positive for HIV, two (1.7%) had a positive Hepatitis B surface antigen and three (2.5%) had a positive Hepatitis C antibody. Three (2.5%) required treatment for syphilis, six (4.5%) tested positive for gonorrhoea and 17 (12.7%) tested positive for chlamydia.
Conclusions
Rates of STIs in this cohort were high: 9.2% HIV and 12.7% Chlamydia prevalence versus 0.17% and 0.29% respectively in England. Patterns of STIs in this cohort differed from national trends. Targeted outreach can improve engagement, testing and care in excluded populations.
Introduction
In 2024, 123 million people were forcibly displaced due to conflict, violence, persecution or human rights violations. 1 In the year ending March 2025, 109 343 individuals claimed asylum in the UK, the highest number since 1979. 2 Although there is evidence that asylum seekers are at an increased risk of infection, including blood-borne viruses (BBV) and sexually transmitted infections (STIs),3–5 the quality of evidence is variable,6,7 exacerbated by the significant underuse of sexual health and reproductive services by this population. 5
In the London Borough of Hounslow, the asylum seeker population increased by over 460% between 2020 and 2025, 8 constituting 0.7% of the resident population.9,10 With over 69% of asylum seekers housed in contingency hotels, Hounslow has the second highest number of asylum seekers in Home Office Accommodation in the UK. 10 In response to the 2097 8 asylum seekers housed between six contingency hotels in the borough, Sexual Health Hounslow (SHH) developed targeted outreach to increase screening of STIs and contraceptive uptake in this population. We present the methods of outreach and initial outcomes from this program. We subsequently include a retrospective case note review describing the demographics and prevalence of STIs and BBV within asylum seeker populations attending sexual health services in Hounslow, to inform future initiatives.
Method
Assessing need
During the mpox outbreak in 2022, sexual health services saw an increase in referrals. SHH received numerous referrals from local contingency hotels. The referred asylum seekers had high translation, transport and safeguarding requirements and faced challenges with registration and follow-up. Many service users had never had a sexual health screen despite significant risk and had not attended local sexual health services before their referral. To assess the potential need, a list of all six local contingency hotels and occupancies was acquired from the local authority.
Aims
SHH aimed to increase testing of STIs and BBVs within locally housed asylum seekers to enable timely treatment and engagement in care, preventing onward transmission of infection.
By opening a walk-in service for asylum seekers, 0.4 miles from the largest contingency hotel, SHH aimed to reduce financial, transport and access barriers to testing and treatment.
By forming relationships with hotel management, local GP services and gaining regular exposure to hotels through targeted on-site outreach, SHH aimed to increase awareness of services and improve follow-up.
Project oversight
SHH operates across three sites offering testing and treatment of STIs and HIV as well as the provision of contraception. SHH worked with local general practitioners, the UK Government Home Office’s ‘find and treat’ program, the primary care network, commissioners and contingency hotel management to raise awareness of its services, create fast-track referral pathways and organise outreach within hotels.
Project development
A multidisciplinary working group of clinical and administrative staff across all three sites was established, meeting regularly to discuss and organize clinic provisions, timing and staffing.
Contact was made with hotel management to discuss local services, the aims of outreach, population demographics and flow through hotels. Clinical staff completed a tour of hotels to assess the feasibility of setting up outreach services on site.
Operating procedures and referral pathways were shared regularly at local clinical governance as well as with commissioners and local GP services.
Outreach
Health advisors ran drop-in outreach sessions in hotel lobbies. They were able to raise awareness of sexual health services, provide condoms, PrEP leaflets and home testing kits. They were available to directly book service users into clinic.
Clinic
The walk-in clinic ran once a week from 13:00–16:00. It opened on the 11th of January 2023. It was staffed by one senior receptionist, a health advisor, and a senior nurse and doctor. It operated a walk-in service, however, allocated slots for pre-booking. A domestic violence lead regularly attended to enable quick and effective safeguarding and support.
Progress
The Home Office ran a ‘find and treat’ pilot program completing systematic BBV screening in hotels. Working with SHH, they fast-tracked positive results into local services for treatment.
Following approval, a weekly clinic opened within contingency hotels in December 2024. Staffed by a health advisor and a senior nurse, the clinic offers asymptomatic screening, contraception including implants, condoms, PrEP, PEP, HBV and HPV vaccinations. Symptomatic patients or those requiring injectable treatments, coil or HIV care were either escorted to the walk-in clinic or directly booked into another site.
Evaluation
An audit of all attendances to Feltham Clinic between 11/1/2023 to 10/2/2024 and an audit of attendances to all sexual health services in the borough of Hounslow between 01/02/2011 and 01/12/2023 was completed. Electronic patient records were searched for service users residing at a postcode corresponding to known home office accommodation. Patients’ addresses, ethnicity, country of origin and notes were subsequently reviewed. The study population included all individuals over the age of 18 whose complete addresses matched known home office accommodation or individuals who had the correct postcode and had documentation of asylum status on their records. Individuals whose complete address did not match home office accommodation and did not have asylum status documented or who identified as UK born and White British were excluded. Patients who did not attend their appointment were also excluded. Demographics, safeguarding concerns, GP registration, translator utilisation and laboratory results were recorded.
Results
The Feltham clinic conducted 94 consultations with asylum seekers over 52 weeks, from 11/01/2023 to 10/1/2024. Following the implementation of targeted outreach and the opening of Feltham clinic, SHH attendances by asylum seekers increased across all three sites (Graph 1). The most common countries of origin were Iran (33, 17.2%), El Salvador (25, 13%) and Namibia (13, 6.8%). The demographics of both clinics are included in Table 1. Graph showing the number of asylum seekers attending SHH services per week. The demographics and appointment characteristics of asylum seekers attending the Feltham clinic compared with all sites.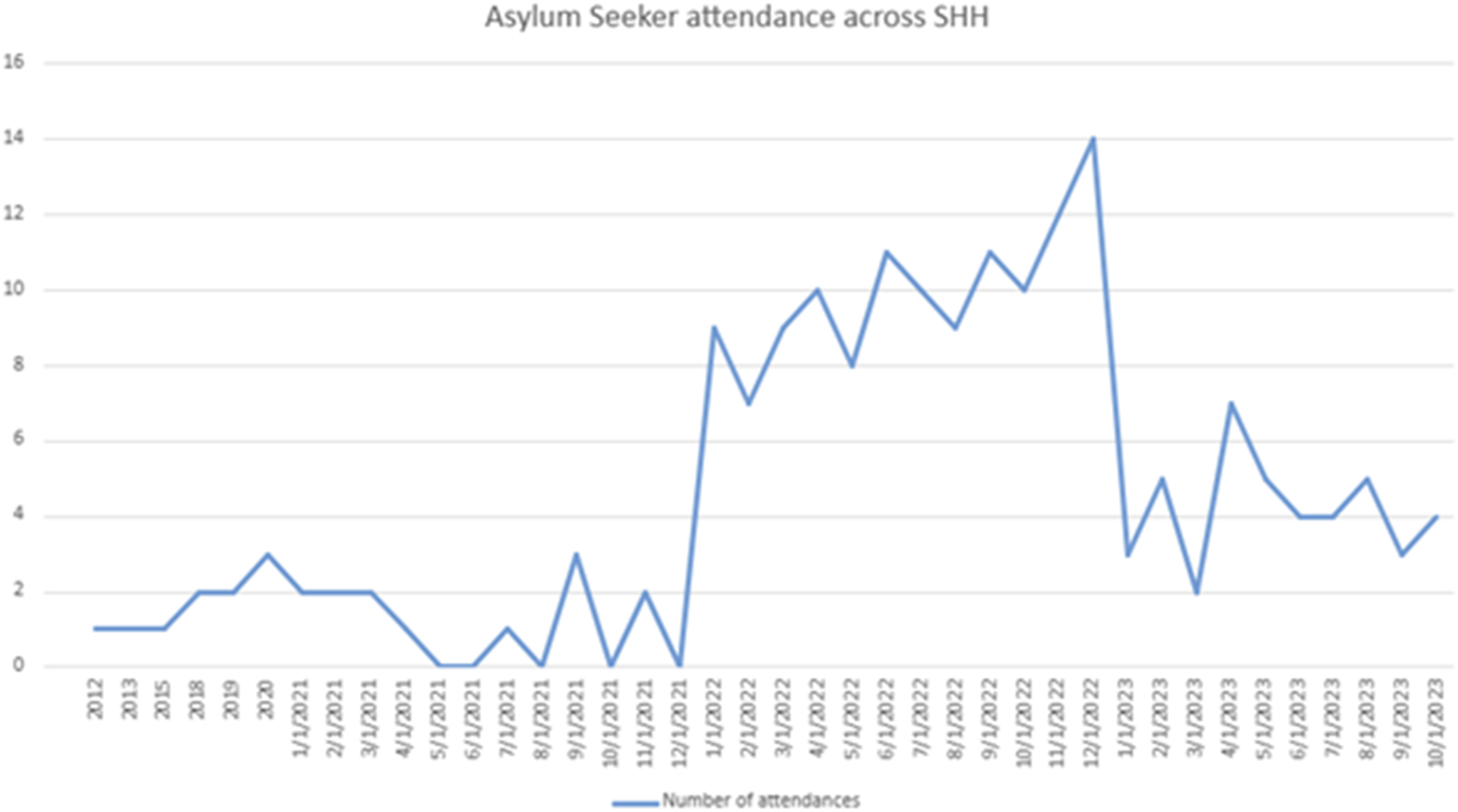
The results of all BBV and STI screening at SHH.
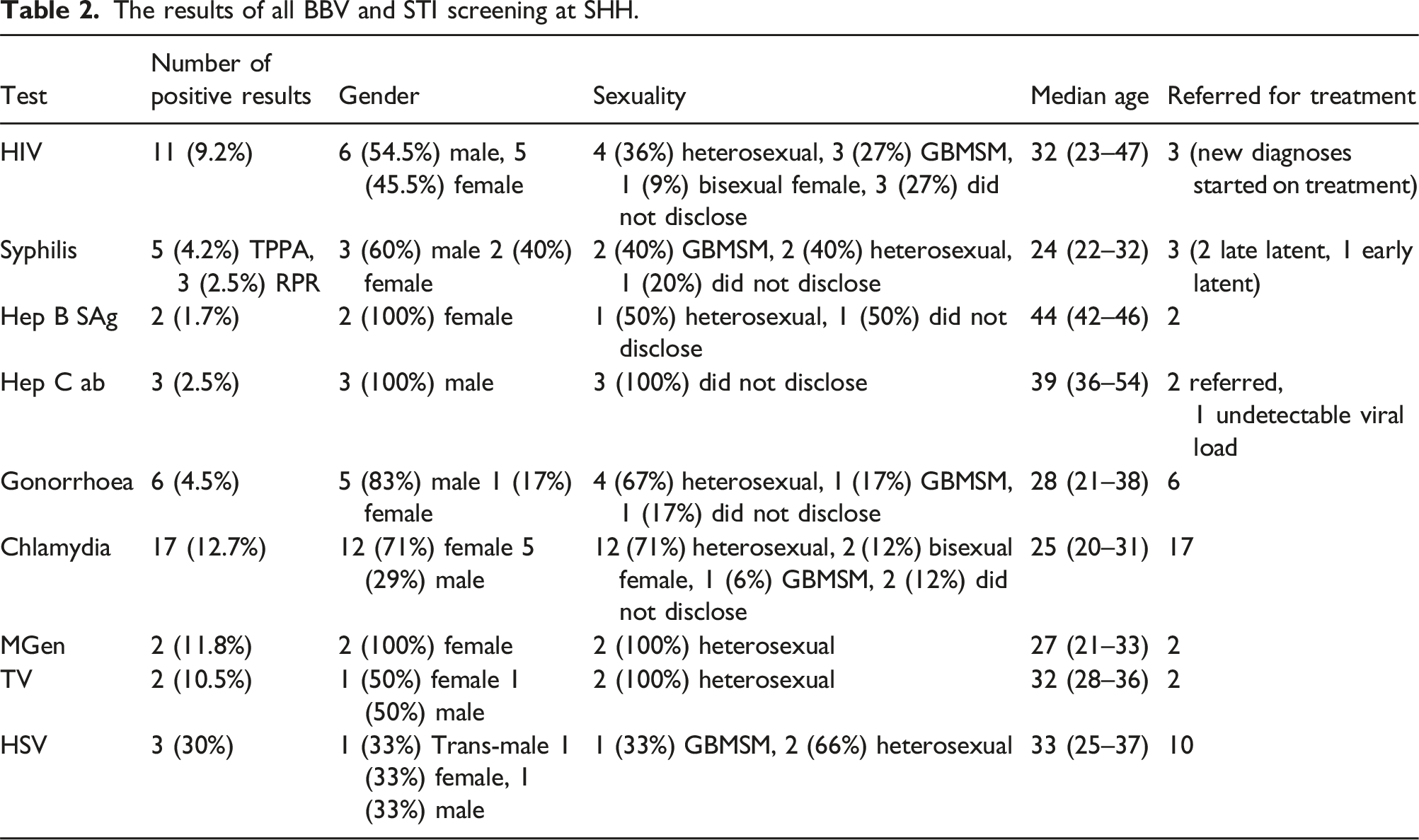
Eleven (9.2%) service users tested positive for HIV. Three (27%) were new diagnoses, two of which were identified through Emergency Department opt-out testing, one of whom presented with haemorrhage secondary to gastric B cell lymphoma. Two service users living with HIV were also living with Hepatitis B. The median nadir CD4 of new diagnoses was 159, (55–954). Of the new diagnoses, the median time in the UK before diagnosis was 60 days (21–180). Two of three diagnoses were established on antiretrovirals within 1 month, the third within 7 months secondary to multiple missed appointments.
Discussion
Data on the prevalence of STIs in asylum seeker populations in the UK are limited. This report describes the demographics, appointment characteristics and prevalence of common sexually transmitted infections in asylum seeker populations attending GU services in Hounslow.
Our targeted interventions, which reduce transport and financial barriers whilst working with GP, Home Office and hotel services to increase engagement and follow-up, was associated with an increase in asylum seeker attendance, indicated by graph 1. Our cohort, who were 62% female, 80% heterosexual, with a median age of 31, is comparable to UKHSA data on national GU attendances in 2023, 11 however, it differs from the overall population of those seeking asylum in 2023, who were 75% male, with the highest age group between years 18–29. 12
A Crime Survey for England and Wales report found 2.1% of adults in England and Wales had experienced sexual assault and 4.4% had experienced domestic abuse in the preceding year, significantly lower than our Feltham cohort where 47% reported a safeguarding concern. 13 The high rate of sexual assault and safeguarding in the Feltham clinic reflects the great need in this population as well as the benefit of holistic, accessible services. The high levels of translator use and safeguarding concern within this cohort correspond to a higher burden of clinical and administrative tasks. The low GP registration (58%) meant this workload could not be spread amongst community services and follow-up fell onto sexual health.
Infectious syphilis cases rose to 0.6% in 2023 in the UK, 14 four times less than our cohort (2.5%). One patient, who had been diagnosed with late latent syphilis, had been rapidly dispersed before the return of results. This case required prolonged health advisor input and translator support to coordinate completion of a benzathine penicillin regime in a different county.
The prevalence of HIV in our cohort was 9.2%, over 50 times higher than the national prevalence of 2023 (0.17%) 15 , similar to the prevalence ratio of 54.79 found by Santoso et al. 3 Unlike national trends, the ratio of female (45.5%) to male (54.5%) people living with HIV was similar in this cohort. The majority of new diagnoses were identified through emergency department testing, highlighting the benefits of its universality. Furthermore, new diagnoses were in the UK for a median of 60 days before diagnosis, potentially benefiting from universal screening on arrival.
Detection rates of GC and chlamydia were high compared to national numbers; 4.5% versus 0.12% 16 and 12.7% versus 0.29% 17 respectively. The majority of gonorrhoea diagnoses in our cohort were in heterosexual males, differing from national trends which describe the highest rates within GBMSM. 18
Limitations
This study exclusively captures individuals attending GU clinics, therefore individuals residing in private accommodation or presenting to alternative health services would not be captured. Excluding individuals who did not attend their appointment can lead to attrition bias. GU services rely on individuals to fill out their demographics for registration, often without the aid of a translator, formal identification or GP registration. Language barriers and fear may lead to discrepancies in details such as address, ethnicity, country of origin or sexuality, leading to the exclusion of asylum seekers.
Conclusion
Rates of STI diagnosis in this cohort were high (9.2% HIV and 12.7% chlamydia prevalence vs 0.17% and 0.29% respectively in England). Cases were complex and time consuming, as indicated by high levels of safeguarding concerns, requirement for translation services and lack of GP registration. Demographics of service users testing positive for STIs often differed from national trends, such as the higher proportion of females testing positive for HIV (45.5%). These differences must be accounted for when planning public health interventions. This descriptive retrospective case note review indicates a need for increased research, targeted outreach and prevention work within this population as well as ongoing funding for sexual health services supporting them.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data for this cohort can be shared upon reasonable request.