
Abstract
Background
Local HIV testing policy is based on clinician assessment of risk factors and HIV indicator conditions, with patient consent required before testing. This project aimed to increase HIV testing among hospital inpatients with community-acquired pneumonia, reduce reliance on clinician judgement, and promote more equitable testing practices.
Methods
Adult hospital inpatients (aged ≥16 years) with community-acquired pneumonia discharged between July and November 2024 were included, irrespective of specialty, and assessed for evidence of HIV testing within the preceding 12 months. Weekly HIV testing rates were monitored throughout the project as a series of quality improvement measures were introduced. These included a hospital grand round presentation, safety briefing, targeted education, guideline updates, an electronic community-acquired pneumonia–HIV order set, and educational posters.
Results
A total of 894 hospital inpatients with community-acquired pneumonia were included, of whom 148 (17%) were tested for HIV. Testing rates increased from 4% at baseline to 29% following successive interventions and rose by 3.6% per week over the study period (IRR 1.036, 95% CI 1.01–1.063; p = 0.005). Pathway-embedded interventions produced more sustained improvements than education alone. Male patients were more likely to undergo HIV testing than female patients (19.8% vs 13.0%; χ2 (1) = 7.67, p = 0.006), with the greatest disparity observed among patients aged 50–69 years (35.3% vs 8.6%; χ2 (1) = 21.7, p < 0.001). Testing rates also differed significantly by age group (p < 0.001), being highest among patients aged 30–49 years and lowest among those aged ≥70 years. All 148 HIV tests were negative.
Conclusions
HIV testing improved significantly following sequential interventions, with pathway-embedded system changes producing more sustainable improvements than education alone. Persistent age- and sex-related disparities suggest clinician risk perception continues to influence HIV testing practices. Low-prevalence settings should consider electronic testing pathways, automated prompts, and the feasibility of opt-out testing approaches.
Introduction
Despite substantial advances in HIV diagnosis and treatment, undiagnosed HIV infection remains an important public health challenge in the United Kingdom.1,2 Late diagnosis leads to poorer outcomes and increased mortality.2,3,4 National guidance recommends HIV testing for patients presenting with HIV indicator conditions, yet implementation remains inconsistent in hospital settings.3,5,6 In low HIV prevalence areas like ours, routine opt-out HIV testing is not commissioned and testing often relies on clinician awareness of indicator conditions and risk perception. Rates of late HIV diagnosis remain disproportionately high, suggesting current testing pathways are failing to identify some patients earlier in the course of infection.2,7
Community-acquired pneumonia (CAP) is a recognised HIV indicator condition, with an undiagnosed HIV prevalence of 0.76%. 6 A local audit of 549 patients identified CAP as the most common HIV indicator condition among hospitalised patients, yet only 10% of patients had received an HIV test within the preceding 12 months. A local staff survey of 58 healthcare staff demonstrated inconsistent knowledge of HIV indicator conditions, local testing guidance and appropriate test selection, highlighting persistent barriers to routine HIV testing.
This quality improvement project aimed to increase the rate of HIV testing among adult inpatients with CAP from a baseline rate of 10% towards a target of 100% testing in eligible patients, in line with national guidance.3,5 The project sought to achieve this by embedding HIV testing within routine clinical pathways, reducing reliance on clinician risk perception and promoting more equitable and destigmatising testing practices. A secondary aim was to evaluate whether sequential educational, guideline-based and electronic system interventions could produce sustained improvements in HIV testing rates.
Methods
This quality improvement project was conducted at a UK district general hospital. Adult patients (≥16 years) discharged between July and November 2024 were identified from hospital discharge records using International Classification of Diseases, 10th Revision (ICD-10) codes. Patients with a discharge code for community-acquired pneumonia (J10–J18) were included in the project. Cases were reviewed electronically to confirm CAP, with hospital-acquired and historical diagnoses excluded. In line with opt-out testing guidance, a completed HIV test was defined as a test performed within the preceding 12 months. Weekly HIV testing rates were monitored throughout the project, involving six sequential Plan-Do-Study-Act cycles.
Statistical analyses were performed using Python. Descriptive statistics were used to summarise patient demographics and HIV testing rates. Weekly HIV testing rates were analysed using Poisson regression to assess the cumulative effect of sequential quality improvement interventions over time. Results are presented as incidence rate ratios (IRR) with 95% confidence intervals (CI). Differences in HIV testing rates by sex and age group were analysed using Chi-square tests. Statistical significance was defined as p < 0.05.
Intervention 1 - Grand round presentation
A trust-wide grand-round presentation was delivered to all trust stuff to improve awareness of HIV indicator condition testing and local HIV testing guidance.
Intervention 2 - Trust safety briefing
A trust-wide emailed safety briefing highlighted the case of a patient who had become critically unwell with an advanced HIV condition, having presented to hospital several months earlier with a CAP, representing a missed opportunity to diagnose HIV at an earlier stage.
Intervention 3 - Local and departmental teaching
Educational sessions for resident doctors and allied health professionals focused on HIV testing indications, consent, requesting processes and access to specialist support.
Intervention 4 - Update of local CAP and antimicrobial guidelines
Local CAP and antimicrobial guidelines were updated to include routine HIV testing recommendations. This involved discussion with microbiology, respiratory and guidelines teams.
Intervention 5 - Introduction of CAP-HIV testing bundle
An electronic CAP-HIV testing bundle incorporating HIV testing alongside routine CAP investigations was introduced into the pathology requesting system.
Intervention 6 - Patient and staff information posters
Patient and staff information posters were displayed in clinical and waiting areas to reinforce HIV testing awareness (Figure 1). Intervention 6 – patient and staff information posters.
Results
A total of 894 adult inpatients with an ICD-10 discharge code for CAP were identified between July and November 2024. Of these, 148 (17%) underwent HIV testing, with all results confirmed negative. Weekly testing rates demonstrated considerable variability early in the project, followed by an overall upward trend. Testing declined towards the end of the study period, although remaining above baseline levels (Figure 2). Weekly percentage of completed HIV tests from July to November 2024. Points represent weekly performance and the dashed line shows the overall linear trend. Shaded regions denote successive Plan-Do-Study-Act cycles.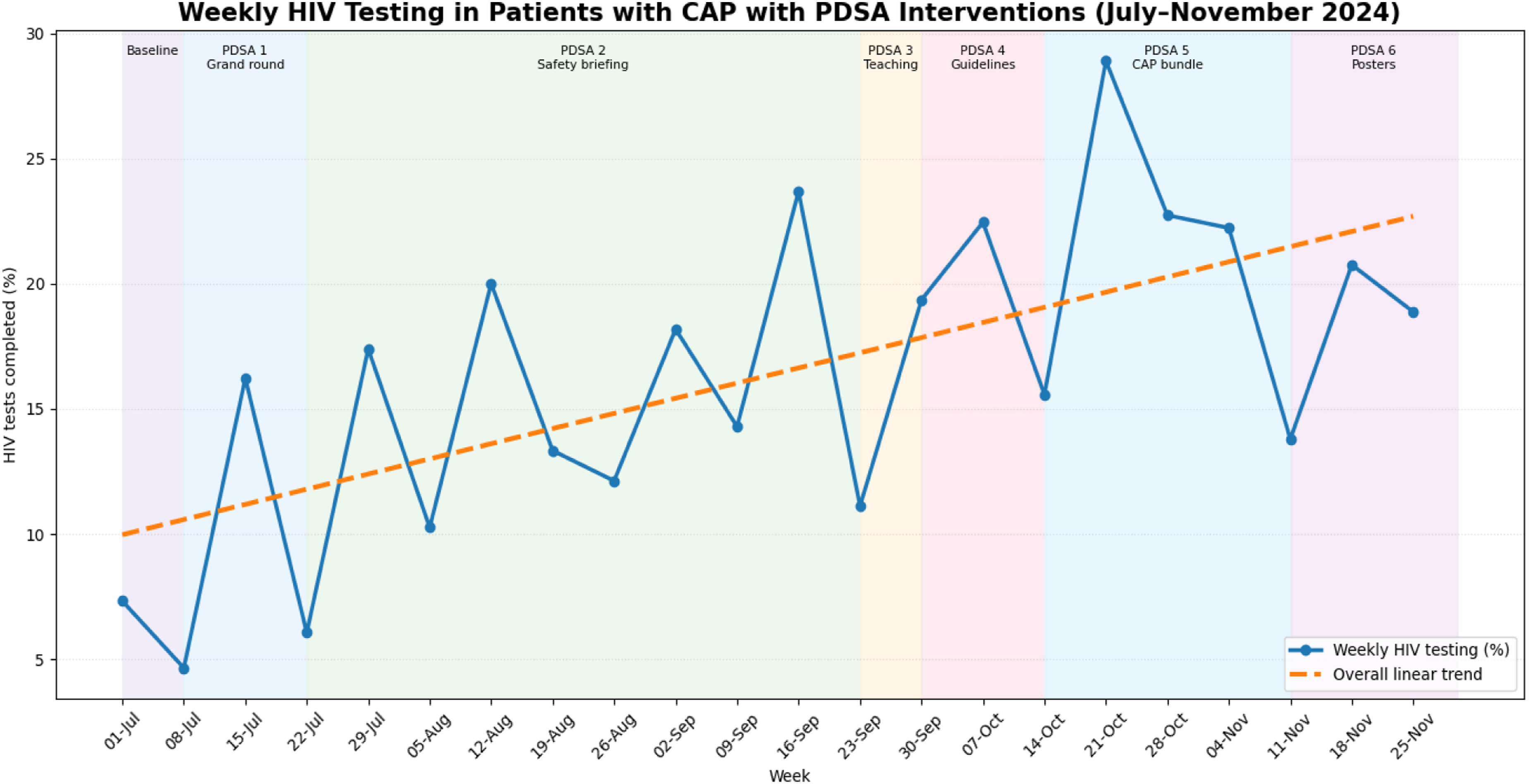
Educational interventions were associated with transient improvements, whereas more sustained increases were observed following guideline changes and introduction of the electronic CAP-HIV testing bundle. Overall, testing rates increased from 4% at baseline to a peak of 29%.
Poisson regression demonstrated a significant increase in HIV testing over the course of the project. Each additional week following implementation of the interventions was associated with a 3.6% increase in HIV testing (IRR 1.036, 95% CI 1.01-1.063, p = 0.005).
Overall, HIV testing was performed in 90 of 454 male patients (19.8%) compared with 57 of 440 female patients (13%). Male patients were significantly more likely to undergo HIV testing than female patients (χ2 (1) = 7.67, p = 0.006).
Age-stratified analysis demonstrated that this disparity was primarily driven by patients aged 50–69 years. Within this age group, 36 of 102 males (35.3%) underwent HIV testing compared with 9 of 105 females (8.6%) (χ2 (1) = 21.7, p < 0.001). No statistically significant sex differences were observed among patients aged <30 years (p = 0.315), 30–49 years (p = 0.305), or ≥70 years (p = 0.241).
HIV testing rates also varied significantly across age groups (χ2 (3) = 17.33, p < 0.001). The highest testing rate was observed among patients aged 30–49 years (26.8%), followed by those aged 50–69 years (21.7%), patients aged <30 years (14.8%), and patients aged ≥70 years (12.8%).
Discussion
Only 17% of eligible patients underwent HIV testing during the study period, despite national guidance recommending HIV testing for all patients presenting with HIV indicator conditions.3,5 This highlights the continued gap between guideline recommendations and routine clinical practice.
Educational interventions produced transient improvements, whereas more sustained gains followed guideline changes and implementation of the electronic CAP-HIV testing bundle, supporting evidence that pathway-embedded interventions are more effective than education alone. 8
Despite overall improvement, statistically significant age- and sex-related disparities in testing were evident. Male patients were significantly more likely to undergo HIV testing than female patients, with this disparity being particularly pronounced among individuals aged 50–69 years. Testing rates were also lowest among patients aged ≥70 years. HIV-related stigma remains a recognised barrier to HIV testing, diagnosis, and engagement with care. 9 The disparities observed in our cohort may therefore reflect continued reliance on subjective clinician judgement regarding who is perceived to be “at risk” of HIV, rather than routine application of indicator condition-based testing pathways. Our findings support the development of more integrated and normalised HIV testing systems that minimise reliance on individual clinician discretion, helping reduce variation in testing practice and mitigate unconscious bias.
Although no positive HIV diagnoses were identified, this finding should be interpreted cautiously given the low HIV prevalence setting, relatively small number of HIV tests performed and short study duration. The primary aim of indicator condition-based testing is to reduce missed opportunities for diagnosis and improve adherence to testing guidance, rather than solely maximise immediate case detection.3,6,10 Despite the absence of positive results, this project demonstrated that HIV testing can be successfully embedded within CAP care pathways in a low-prevalence setting.
Limitations
This single-centre quality improvement project was conducted in a low HIV prevalence setting, which may limit the generalisability of the findings to areas with different HIV prevalence and testing practices. Patient identification relied on ICD-10 coding and retrospective record review, introducing the potential for incomplete case ascertainment and selection bias. The short study duration, relatively small sample size and sequential implementation of multiple interventions without a control group limited assessment of long-term sustainability and the independent effect of individual interventions. Finally, although significant age- and sex-related disparities in testing were identified, the study did not formally assess factors such as clinician attitudes, perceptions of HIV risk, patient acceptance, or organisational barriers. Consequently, explanations relating to stigma, unconscious bias, and risk perception remain speculative rather than directly measured.
Conclusions
Despite improvements with educational and system-level interventions, overall testing rates remained below those recommended by national guidance, and significant disparities persisted among women and older adults, suggesting that stigma and assumptions regarding HIV risk continue to influence testing behaviour.
A key learning from this project was that even pathway-embedded interventions remain dependent on clinician engagement and can be bypassed in routine practice. Consequently, unless testing is incorporated into systems that reliably prompt or automate HIV testing for all eligible patients, improvements may be difficult to sustain over time. Educational interventions alone were resource-intensive and produced only transient improvements, particularly within an environment characterised by workforce pressures, competing priorities and frequent staff turnover.
For organisations seeking to improve HIV testing in low-prevalence settings, sustainable approaches are likely to include integrated electronic test bundles, automated prompts linked to HIV indicator condition diagnoses, and assessment of the feasibility of opt-out testing in clinical areas with a higher prevalence of HIV indicator conditions. These approaches may help reduce variation in practice, minimise reliance on clinician recall and judgement, and reduce the influence of unconscious bias and HIV-related stigma.
Footnotes
Ethical considerations
Ethical approval was not required for this quality improvement project.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declare no potential conflicts of interests with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on request.