
Abstract
This article examines the diagnosis of general paralysis of the insane (GPI) at the Auckland Mental Hospital, New Zealand, between 1868 and 1899, and changes in the identified causes of this condition. It argues that despite long-standing evidence citing the role of syphilis, asylum doctors working in New Zealand were as reluctant as their English and Scottish colleagues to blame syphilis alone for GPI. It also argues that although syphilis became a more popular cause in the aetiology of GPI by the end of the nineteenth century, medical and non-medical sources continued to cite other causes for GPI.
In 1896 Thomas Clouston, a former Medical Superintendent of the Royal Edinburgh Asylum (hereafter REA) in Scotland, and Lecturer in Mental Diseases at the University of Edinburgh, addressed the British Medical Association’s Section of Psychology. In this speech Clouston (1898: 304) noted that: Man with a nervous heredity if he has got safely through childhood and adolescence may with care and obedience to Nature’s laws live to a good old age; but if he drinks too much, or carries with him an old syphilitic gland, or has to work too hard, he has not the staying power to resist these things. With a good heredity he might have withstood them; with a bad heredity in his nerve centres he falls a victim to general paralysis.
Since early in the nineteenth century the causes of general paralysis of the insane (hereafter GPI) have been discussed in international medical circles. Contemporary doctors and social commentators proposed an array of aetiological theories about the condition, some referring to the role of syphilis and others ignoring or refuting it. This debate forms the core discussion of the present article.
GPI was unusual among mental health diagnoses as it was recognized relatively early in the nineteenth century as a physical and behavioural manifestation of a change in brain physiology. Many other classes of mental illness, such as melancholia or mania, were not consistently linked to such a change. While Margaret Thomson (1988) and Gayle Davis (2008) have focused on GPI in nineteenth-century Scotland, it is a relatively unexplored topic in a New Zealand context, and one that illuminates Dr Thomas Clouston’s influence in nineteenth-century New Zealand medicine, demonstrating the mobility of medical theories through doctors’ education and medical journals.
This article centres on discursive constructions of GPI, arguing that the medical interpretations of the condition’s aetiology in the nineteenth century were far more complex than historians have previously claimed. This study analyses patient case notes from the Auckland Mental Hospital (hereafter AMH) of GPI patients to demonstrate that Clouston was not alone in his reluctance to attribute the condition to syphilis, and suggests that this reticence transcended the social and financial pressures exerted by conservative elites. This article examines nineteenth-century aetiological theories about GPI by exploring medical ideas about the condition, as well as opinions about GPI that the general population was exposed to, and outlines the ideas about GPI in circulation in non-medical New Zealand society. It then focuses on constructions of patients admitted to the AMH with the diagnosis of GPI between 1868 and 1899. This examination of a range of sources demonstrates the mobility of ideas about GPI, heredity and vice, through several channels of communication.
Mental health in New Zealand
By 1868 the AMH was one of several large, public mental hospitals in New Zealand. The colony at this time consisted of six provincial governments, one of which was based in Auckland city, in the northern half of the North Island (Ballantyne, 2009: 112). The AMH was built by the Auckland Provincial Government during 1865 and 1866, ‘from moneys appropriated for that purpose out of the Half-million loan’, a grant proposed to be ‘equal to that contributed by private liberality’ (Anon., 1851; King, 1871: 3). Asylum medicine in nineteenth-century New Zealand combined provincialism, partly due to the lack of transport and communication infrastructure at this time and the long distances between major cities, and an emerging sense of cohesion, enabled by a series of formal and informal networks. These networks, formed through membership of the New Zealand Medical Association, attendance at Inter-colonial Medical Congresses, and annual tours of inspection conducted by Inspectors General of Lunatic Asylums, ensured that despite often great distances and differences between mental hospitals throughout New Zealand, there was a sense of connection (Dawson, 1 2013: 63). There was a similarly complex relationship between New Zealand mental hospitals and their practices, and theories and practices occurring in British mental hospitals. Despite the great distance between New Zealand and Britain, and clear environmental and demographic differences between the two locations, great similarities also existed, through the employment in New Zealand of doctors educated in English and particularly Scottish universities and mental hospitals, and the availability of British medical publications in New Zealand (Dawson, 2013: 63, 73). There was also a relationship between the New Zealand Medical Journal (NZMJ) and the British Medical Journal (BMJ), as the former regularly published ‘London Letters’, relaying relevant events and ideas from the British Medical Association (BMA) (Dawson, 2013: 73). Ideas could therefore be transmitted, and were made mobile through these relationships and media.
The AMH served a population of approximately 165,800 people by the end of 1899 (Anon. [Census], 1901: 3). Figures from 1895 show that at that time there were 246 males and 146 female patients in the AMH, a total comprising nearly 20 per cent of the total number of patients committed to mental hospitals in New Zealand (Anon., 1896c). Its public mental hospitals prior to 1876 were managed by a layman and a Resident Surgeon (Dawson, 2013: 67), and in 1868 the AMH was managed by Inspector John King, a layman, while patient treatment was supervised by Dr Robert Elliot Fisher, a Belfast-trained Irish doctor (Wright-St. Clair, 2003: 136). After 1876 Resident Surgeons were replaced by Medical Superintendents, who managed individual mental hospitals, while all mental hospitals across New Zealand were overseen by the Inspector-General of Lunatic Asylums (Wright-St. Clair, 1988). Aside from Fisher and his successor, Dr Aickin, most doctors employed at the AMH as Resident Surgeons or Medical Superintendents were trained in England or Scotland. This, along with the availability of the BMJ and the Journal of Mental Science (JMS), is strongly suggestive of a powerful ‘British’ influence on practices at the AMH during the nineteenth century.
Statistics collected at mental hospitals from across New Zealand during the nineteenth century illustrate the significance of heredity and vice to contemporary discourses about mental illness. Government reports often included tables detailing causes of insanity in patients admitted to these institutions, and vice, in the form of drink, smoking, sexual excess, was a commonly cited factor. Vice, as a more ‘visible’ factor in a diagnosis, was more closely identified with insanity than heredity in popular discourses about GPI. 2 Yet heredity, despite its more concealed nature, formed a part of medical ideas about the aetiology of GPI. It is essential to note that, although the aetiological link between syphilis and GPI was not established beyond doubt until early in the twentieth century, there was an existing body of medical evidence as early as the 1860s promoting the role of syphilis in this diagnosis. These ideas circulated in British and European medical journals and textbooks. By the 1860s there was also a fever of concern about the role of prostitution in the spread of syphilis. From this it could be expected that there was a connection between prostitution and GPI but, crucially, this connection was not expressed in contemporary medical or popular sources, and has received very scant attention in recent historiography of GPI. Published medical discourses, the majority of which came from Britain, and the popular press, which often reprinted articles from English newspapers, were reluctant to identify GPI exclusively with syphilis during the nineteenth century. Historians have attributed this reluctance to the implications of such a connection for individual GPI patients, many of whom – at least in Britain – were married, urban-dwelling, employed, educated and ‘respectable’. ‘Typical’ male GPI patients in colonial New Zealand tended to be socially out of place in urban society and often lived in rural and isolated areas. These men (most GPI patients in nineteenth-century New Zealand were male) also battled financial hardship and the ever-present threat of starvation or malnourishment. These less than respectable traits, in the context of the nineteenth century, when understood in the light of the independence of most New Zealand mental hospitals from the judgemental clutches of charity funding, mean that concerns of respectability had far less influence than they may have done in the REA. This article also identifies the scarcity of connections made in medical and popular texts between prostitution and GPI.
Debauchery to spirochaete: medical theories about general paralysis of the insane
From early in the nineteenth century GPI had been linked to a variety of causes, including ‘debauchery’ (Haslam, 1809: 208–9), changes in brain physiology (Hare, 1998: 47), and in the late 1850s, the Danes Frederich Esmarch and Peter Willers Jessen wrote the first internationally published article to present syphilis as an aetiological factor in GPI (Esmarch and Jessen, 1857). By the early 1870s, ideas about the aetiology of GPI published in the BMJ mirrored contemporary class concerns, speculating that the causes of the condition in the ‘opulent classes’ were ‘intense and prolonged mental activity, carried on under emotional excitement’, along with ‘sexual excesses; and large quantities of wine and alcoholic stimulants’ (Hitchman, 1871). This was differentiated from the aetiology of GPI in working-class patients, for whom ‘heavy and prolonged labour, sustained by large quantities of ale or spirits, rather than by nutritious food and a due quantity of sleep’ were the identified causes. Dr Hitchman notes that the GPI population were ‘almost exclusively the male sex’, as well as typically aged over 30 years old and ‘among the upper classes of society’. However rare, female GPI patients existed in 1870s England and, despite comprising a small patient cohort, their numbers were sufficient for doctors to claim that female general paralytics were from ‘the poor, and the lower middle classes of society’ (Hitchman, 1871).
The role of heredity in the production of GPI is supported by patient case note extracts included in Hitchman’s article, in which he quotes a case note for a male patient, T.G., with a ‘special hereditary predisposition to insanity’, including a ‘mother of weak intellect’ who was ‘always in anxiety owing to the vices and caprices of her husband, who drank to excess and died of pulmonary consumption’. Furthermore, the patient’s grandfather, uncle and sister were all described as mentally deranged, and had died in lunatic asylums. Added to his ‘hereditary predisposition to insanity’, the patient had a personal history of excessive drinking, so that both heredity and vice appeared in the patient’s case note. But the defining statement in Hitchman’s published version of this case is his description of T.G. as a result of ‘a (probable) drunken procreative act; to gestation in a womb of a mother agitated by a thousand fears; to poor and irregular nutrition in infancy; to defective intellectual training; and the daily example of drunkenness or depravity in his father, and last, although not least, to intemperance on his own part’ (Hitchman, 1871). Tellingly, despite contemporary medical literature referring to the aetiological role of syphilis, in his article Hitchman did not refer to syphilis at all. 3
A larger examination of GPI cases was presented by Dr Julius Mickle, Superintendent of the Grove Hall Asylum in London, who examined GPI rates published in the Lunacy Blue Books for England and Wales, over a four-year period during the 1880s (Mickle, 1886). This analysis identified 3,374 male GPI patients and 910 female patients committed to English and Welsh mental hospitals during this time (Stoller and Emmerson, 1969: 607). Mickle also found a slight gender difference in GPI aetiology, with males becoming general paralytics because of ‘intemperance in drink, heredity, other bodily diseases, and adverse circumstances’, while for females ‘heredity, intemperance in drink, other bodily diseases and domestic trouble’ were the main causative factors (p. 607). 4 The most notable difference between the listed causes for each gender is that for female patients ‘domestic trouble’ replaced ‘adverse circumstances’, but this is possibly a fairly insignificant difference, as domestic trouble for women was perhaps equivalent to ‘adverse circumstances’ for many male patients. As shown below, male GPI patients admitted to the AMH tended to work in occupations with no guarantee of consistent employment, sometimes in isolated locations, where the threats of poverty and loneliness were ever-present, and to live in conditions that could be described as ‘adverse circumstances’. In contrast, the five female patients admitted to the AMH during the nineteenth century all lived in the domestic realm, so that ‘domestic trouble’ may be a fairly appropriate description of many of the difficulties they may have faced. As in the AMH patient cohort, there was a notable gender disparity for GPI admissions in England and Wales during the 1880s. Mickle (1886: 247) attributed this to the ‘greater moral shocks to which the male is subjected’ and a ‘greater liability to syphilis, injury and isolation’. Furthermore, male brains were said to be ‘innately more liable to organic disease’ than female brains. Mickle’s book shows how syphilis was incorporated into a variety of potential causes, not discounted altogether, but not elevated above any other cause.
Mickle’s work on GPI was set against a background of considerable debate about the significance of heredity and vice, including sexual and alcoholic intemperance. At the 1884 Congrès Périodique International des Sciences Medicales in Copenhagen, Frenchman Valentin Magnan maintained that at a Parisian hospital 300 GPI patients were admitted annually, of which only 30–40 per cent were diagnosed with syphilis (Magnan, 1886: 476). Rather than syphilis, Magnan argued that a ‘hereditary condition predisposition’ was essential, as ‘syphilis, chronic alcoholism and excesses of any kind are only determining factors’ (p. 479). In this example, heredity trumped vice in the hierarchy of causes of GPI, reflecting general patterns in contemporary theories about insanity, particularly towards the end of the nineteenth century; these theories, by emphasizing the role of heredity or a pre-existing tendency to mental illness, sought to reduce state culpability in the aetiology of what were often incurable cases of mental illness. Mexican historian Cristina Rivera-Garza (2001: 66) suggests that towards the end of the nineteenth century the Mexican government promoted heredity as a cause of mental illness, rather than the influence of ‘modern life’, in a deliberate attempt to minimize government responsibility and blame for the insane, in a country blighted by economic inequality.
The disagreement among the international medical community regarding the cause of GPI was further demonstrated at the Section on Psychological Medicine at the Ninth International Medical Congress in the late 1880s, which included several papers contributed by British doctors on the link between syphilis and insanity (Anon., 1888). Puzzlingly, a paper contributed by one of these authors to the BMJ in 1890 denied this simple and clear connection, by presenting GPI as a ‘degeneration’ initiated by ‘possibly drink, extravagance, restlessness, and sexual excess alone or combined’ (Savage, 1890: 777). In the same article, Savage characterized GPI patients as ‘middle aged married men, inhabitants of cities, and flesh eaters’. Savage’s GPI patient cohort formed the core of the ‘respectable class’.
Other significant articles about GPI contributed to the BMJ during the 1890s label the condition as a ‘disease of civilisation’ or provided statistics of GPI cases admitted to mental hospitals (Savage, 1894). 5 The depiction of GPI as a ‘disease of civilisation’ sits well with other attempts to construct GPI patients as men of the world, who had succumbed to the condition due to overwork and over-indulgence in the fruits of their labour. It also lends an air of inevitability or of a lack of culpability for GPI patients, perhaps suggesting that it was not their own vices or misdeeds that made them so unwell, but that it was simply an expected consequence of life in modern times. Other medical journal articles promoted the role of syphilis, including an 1890 survey of medical literature that included a review of a German doctor’s analysis of the causes of GPI. This analysis involved 200 GPI cases and demonstrated that the condition was ‘due to syphilis and syphilis alone’, arguing that, while in 19 per cent of those 200 cases the patient had no history of syphilis, patients had ‘probably suffered from it unknowingly’. In contrast, heredity could only be traced in 11 per cent of cases in the sample (Anon., 1896a).
The reluctance of some psychiatrists to attribute GPI entirely to syphilis is shown by the degree of proof of this relationship that many doctors sought before they were willing to discount other causes. At the 1893 Annual Meeting of the BMA, Denmark’s Dr Jacobsen blamed the unwillingness of doctors working in mental hospitals to support the doctrine of a syphilitic aetiology on the fact that ‘no one has yet been able to definitely trace the syphilitic infection to every case of general paralysis’ (Anon., 1893a). Perhaps it was the value-laden nature of tainting all GPI patients with a sexually-transmitted disease that ensured that doctors required such conclusive and definitive evidence, before lending their support to the idea of a syphilitic aetiology. Scottish historian Margaret Thompson’s research into patients admitted to the REA in the late-nineteenth and early-twentieth centuries shows that while Scottish doctors were concerned about a correlation between ‘alcoholism and promiscuous sexuality’, they failed to ‘recognise the causative relationship between syphilis and general paralysis of the insane’ (Thompson, 1988).
Clouston, who treated many of the patients mentioned by Thompson, considered syphilis and GPI as distinct diseases, and cited a number of causes of GPI, including ‘brain exhaustion, irritation, excesses in drinking, sexual excess, over-work, over-worry, syphilis or injuries’ (Thompson, 1988: 326). Thompson argues that the role of syphilis as a ‘necessary precursor’ to GPI placed doctors like Clouston in a professionally and socially difficult position, because of the large number of patients under his care who could be branded ‘promiscuous or dissipated’ (p. 329). She also suggests that Clouston feared that financial supporters of the REA, drawn from Edinburgh’s respectable elite, would be uncomfortable with the realization that many patients at the asylum were mentally ill as a result of syphilis, and would consequently be unwilling to pay for the care of the sexually dissolute. In view of this concern, Clouston (1895) preferred to link GPI to ‘hard work under conditions of excitement and responsibility’, a connection possibly more palatable to those professionally and financially associated with the REA. His reference to the syphilitic origins of GPI, as shown in the passage at the beginning of this article, also endorsed other causative factors, suggesting that heredity and vice, even non-sexual vice, continued to be significant to medical theories about GPI at the end of the nineteenth century. Clouston was a prolific author of articles published in the BMJ and the JMS, the first Lecturer in Mental Diseases at the University of Edinburgh and a hugely significant influence on doctors working in New Zealand mental hospitals in the late-nineteenth century (Davis, 2008: 55; Dawson, 2013: 71).
Davis (2008: 200) queries Thompson’s examination of Clouston’s work on GPI, arguing that Thompson exaggerates Clouston’s moral dilemma. Instead, Davis suggests that Clouston’s denial of the role of syphilis in the aetiology of GPI was due to ‘a lack of statistical evidence to support what was at that time a major reformulation of the syphilitic domain’ (p. 200). However, by the end of the nineteenth century there was growing evidence of the role of syphilis as the sole cause of GPI. This is particularly evident when contrasting the increasing certainty of the medical profession about syphilis as a significant factor in most GPI cases, as noted in the BMJ (Anon., 1896b: 296), with the plateau, if not decline, in the importance attached to the role of intemperance in alcohol or ‘modern life’. While counter-arguments to the aetiological role of syphilis remained at the end of the nineteenth century, it is noteworthy that a doctor as esteemed as Clouston refuted the importance of syphilis.
Davis’s objections to Thompson’s work have merit. Yet Davis has somewhat understated the fact that many other influential figures in British psychiatry in the late-nineteenth century were fairly insistent in attributing GPI to syphilis, and were unwilling to ascribe the condition to anything else. For example, Dr Alfred Campbell wrote a lengthy article in the BMJ in 1899, concluding that although it was only in the 1880s that the significance of syphilis in the aetiology of GPI had been recognized, all previously gathered statistics were ‘valueless’ (Campbell, 1899). Campbell argued that this was because all the previous patient histories on which the statistics had been based were obtained by asking questions only until answers such as ‘alcoholism, overwork, trauma’ were given, at which point questioning had then ceased, as, ‘in accordance with former doctrines, this would be immediately entered as sufficient cause for the attack’ of GPI (p. 705). 6 So a GPI patient’s history of syphilis might never be suspected or enquired about. Importantly, even Campbell’s apparently scientific monologue about GPI was tinged with ideas about morality, as he claimed that most GPI cases came from ‘localities where the traffic in immorality is greatest’, which he deduced accounted for claims that GPI was a ‘disease of urban and industrial communities’, rather than in rural areas (p. 705). This suggests that Campbell connected prostitution to GPI through a syphilitic consequence of prostitution. While still somewhat opaque, this is one of the more explicit connections made between GPI and sex workers in either the BMJ or the JMS. International medical discourse about prostitution and syphilis favoured stronger and wider controls on prostitution in civilian society, as demonstrated by the role of several prominent British medical personalities, including Ernest Hart, editor of the BMJ, psychiatrist Henry Maudsley, and surgeon Berkeley Hill, in leading a Society of the Extension of the Contagious Diseases Act to the Civil Population (Brown, 2006: 68). Despite this connection between syphilis and prostitution, discussions in medical discourses about the possible connection between prostitution and GPI were notably absent during this period.
Knowledge about general paralysis of the insane in the colony
General paralysis of the insane was referred to in non-medical texts in nineteenth-century New Zealand in several ways, from newspaper articles speculating on the cause of the condition, to articles discussing medical theories about it, to references to well-known GPI patients. There was no mention of syphilis in any of the publications referring to the aetiology of GPI. The newspaper articles analysed here are from regional and local newspapers from around New Zealand, and many of these publications were based in the same area as the AMH. Despite some regional differences and difficulties in communication between locales, as discussed earlier, newspaper articles were often reprinted in other publications, creating a ‘national’ discourse of sorts, and in some instances these articles were reprinted from foreign newspapers, suggesting an international aspect to these non-medical texts. This analysis of newspapers published in New Zealand between 1868 and the end of 1899 shows that while international ideas about GPI were endorsed, the significance of syphilis as a cause of GPI was virtually ignored.
Mirroring the uncertainty in medical circles about the causes of GPI, non-medical discourses were vague about the aetiological details of the disease. For example, a report of an inquest conducted on an AMH patient published in the Auckland’s Daily Southern Cross stated that ‘from the evidence given it appeared that the deceased had been suffering for some considerable time from general paralysis’ (Anon., 1871). 7 According to the press report, the coroner found that the deceased had ‘died from natural causes’. Yet, this report omits any information about the nature of GPI itself or its causes. This may be because such information was not thought to be appropriate for a lay publication, because it was not considered newsworthy, or because it was taken for granted that New Zealand’s newspaper-reading public already knew what the cause of GPI was or knew that it was still unconfirmed. Hurn (1998: 92) has speculated on this in her doctoral thesis, using the publicity surrounding the death of Lord Randolph Churchill as an example of the lack of press coverage given to syphilis as a cause of GPI, as late as the 1890s.
Heredity was also discussed in non-medical publications in New Zealand, through references to the family trees of GPI patients. In 1873 the Nelson Evening Mail, a newspaper from the South Island, published by request an extract from Dr Maudsley’s Body and Mind, which included Benedict- Augustin Morel’s research into the ‘family history of a youth who was admitted into the asylum at Rouen’ (Anon., 1873). Morel’s work described the youth’s family as consisting of a first generation of ‘immorality, depravity, alcoholic excess and moral degeneration’; the youth’s great-grandfather, who was killed in a bar room brawl, belonged to the second generation of this family, featuring ‘hereditary drunkenness, maniacal attacks, ending in general paralysis in the grandfather’. This ‘general paralytic’ grandfather produced a sober ‘but hypochondriac’ son, who then fathered a child of ‘defective intelligence’ which transformed into ‘complete idiocy’. The requested inclusion of this family tree in a lay-press newspaper suggests that the connection between vice, through ‘immorality, depravity and alcoholic excess’ and GPI in subsequent generations was of considerable interest to the newspaper-reading New Zealand public, along with the idea of hereditary influences on GPI. Such ‘family trees’ made heredity more visible as a cause of GPI and of insanity in general.
Other traces of non-medical theories about GPI are evident in a report on medical testimony given in a manslaughter trial that mentioned a woman who had died of ‘general paralysis from chronic alcoholism’, which the medical witness claimed ‘would indicate long indulgence in drunken habits’ (Anon., 1883). Syphilis was not considered part of the aetiology of GPI in this case. In a similar vein, an article written by a medical doctor but published in a popular newspaper, held alcohol responsible for the decline of man to ‘the lower ranks of the living creation over which he was born to rule’, a state which the author defined as ‘general paralysis’, adding that ‘our asylums contain an immense number of examples of this general paralysis, produced by alcohol’ (Richardson, 1884). The attribution of GPI to alcohol can be explained by the number of similarities between GPI patients and patients admitted to mental hospitals suffering from chronic alcoholism. The advent of the Wasserman test in 1906 and the discovery of the syphilitic spirochaete in the bloodstream of syphilis patients made it possible to distinguish between patients with GPI and patients suffering the effects of alcoholism and delirium tremens. Until this time, medical doctors based their diagnoses on observation of patient behaviour, speech patterns, gait and other physical characteristics, with some patients suffering from alcoholic insanity sharing many of these behaviours and characteristics with general paralytics (Davis, 2008: 108).
Discussions about GPI in the press persisted into the 1890s and continued to involve the publication of medical theories to be read by the general public, both of which referred to gender-based theories about the causes of GPI, as well as stress due to city life (Anon., 1892; Anon., 1893b). In some instances, vice was represented by intemperance, perhaps because this was a more palatable form of vice than sexual impropriety (Anon., 1898a). Another possible explanation is that alcohol abuse may have been more visible than syphilis would have been at certain stages of the condition, added to the fact that symptoms of GPI were often reminiscent of symptoms of sustained alcohol abuse.
Men with GPI were often constructed in the press as being vulnerable to the disease as a result of their own otherwise commendable work ethic, or as falling victim to GPI due to excesses which enabled men to keep up a high work rate (Anon., 1892). An article published in a South Island newspaper referred to GPI as a condition virtually exclusive to men, and was brought on by ‘overwork, overindulgence in alcoholic beverages, tobacco or narcotics, and other excesses’ (Anon, 1889). In this same article, GPI patients were defined by gender and occupation, as men who ‘insist on working sixteen hours a day, and who employ stimulants to keep up their strength instead of getting natural rest, a cohort consisting of a majority of bankers, lawyers, editors, actors, playwrights, and even doctors’ (Anon., 1889).
GPI was also rendered visible in newspapers through celebrity patients. Along with reports about Lord Randolph Churchill, an obituary of a renowned Dunedin merchant and ‘former Provincial Treasurer’ identified both the deceased and his cause of death, suggesting that in New Zealand at this time there was no shame attached to a GPI diagnosis (Anon., 1894a; Anon., 1894b). If syphilis was known to be the cause of the condition, the man’s family might have encouraged the press to be a little more discreet about the cause of death.
In 1898 the Christchurch-based Star newspaper reported on the attempted suicide of a male GPI patient living in Auckland. As with previous press articles referring to GPI there was no information included about the illness itself. It was reported that the man had ‘some time ago sustained an attack of general paralysis, and latterly has developed paralysis of the brain. He has a wife and children. Formerly he was a commercial traveller’ (Anon., 1898b). The inclusion in this report of a reference to the man’s wife and children is particularly relevant, as a medicalized connection between sanity and family had been published earlier in the decade, when New Zealand newspapers reported on a double murder in Victoria, Australia (Anon., 1891). In this double murder case the accused murderer was judged by several ‘medical men’ to be suffering from ‘general paralysis of the brain’. But several other doctors who examined the accused did not believe him to be a general paralytic, with one of the doctors quoted in the article as saying that ‘if he were a householder with a wife and children, and were brought before me for commitment to Kew, I would not sign the warrant, I am so satisfied of his sanity’ (Anon., 1891). This testimony suggests that doctors working in the nineteenth century tended to equate mental illness, including GPI, with certain personal and economic circumstances, and that GPI was perceived to be incompatible with family life.
These newspaper articles demonstrate that there was no direct connection made in non-medical or medical discourses published in the popular press between prostitution, as a source of syphilis, and GPI. Historians Joseph Melling and Bill Forsythe (2006: 132) have noted that the connections between ‘sexual infection, legal regulation, and social purity campaigns’ were a ‘context in which mental illness was understood’. However, my analysis based on a variety of texts shows that this was not very explicit, and reveals that there are very few references to a connection between prostitution and GPI in historiography of the disease. Davis (2008) refers to prostitution just once in her book The Cruel Madness of Love, Sex, Syphilis and Psychiatry in Scotland, 1880–1930, and while Brown (2006: 213) discusses prostitution, he does not link it explicitly with GPI. Thompson (1988: 337) queries how Scottish doctors dealt with the inference that patients with GPI were likely to have had direct or indirect sexual contact with prostitutes, and argues that Clouston was particularly slow to accept the role of sexual vice in the aetiology of GPI, choosing instead to embrace ‘mental hygiene’ once the role of syphilis could not be denied any longer. However, analysis of contemporary medical texts shows that while Clouston was at times reluctant to acknowledge the role of syphilis in GPI, he was by no means the only medical professional to make this omission. Furthermore, his reluctance to openly declare syphilis to be the sole cause of GPI prior to the development of the definitive Wasserman test was countered by a number of sternly phrased articles and addresses referring to morality and the cost to mental health of ignoring such principles (Beveridge, 1995: 139). Clouston’s application of ideas about mental hygiene and racial fitness was mirrored by growing public concern in the late-nineteenth and early-twentieth centuries about social hygiene, which included concerns about sexually transmitted diseases and the consequences of ‘profligate men visiting their sins upon their wives and children’ (Brandt, 2001: 572).
The role of prostitutes in the spread of syphilis concentrated public debates about venereal disease and the need for government legislation to minimize the spread of this medical and moral contagion from sex workers to a wider and ‘innocent’ society (Brandt, 2001: 572). In a New Zealand context, women suspected of being prostitutes were subjected to genital examination and sometimes imprisonment (Brickell, 2009: 469). The strengthening medical links between syphilis and GPI could have prompted an acknowledgement of the significance, or even the pre-Wasserman potential significance, of prostitution to the development of GPI in medical or popular texts. Government control of prostitution, framed as a public health concern, depended on a degree of public panic about syphilis and resulted in a gender-driven policy that targeted prostitutes, the perceived ‘source’ of syphilis, rather than those who potentially ‘carried’ the disease to homes and families. In line with a number of British colonies and England itself, New Zealand introduced its own Contagious Diseases legislation, although it diverged from legislation in other locations through its intent to ‘suppress prostitution rather than to limit the spread of venereal disease’ (Macdonald, 1986: 16).
Published references to GPI in New Zealand in a non-medical context examined the disease in a somewhat limited way during this period. Newspaper articles included minimal information about the causes of GPI and, when aetiology was raised, it was intemperance in alcohol that was the most commonly identified factor. Other articles blamed heredity or natural causes for GPI. Non-medical texts also discussed idealized gender behaviour and contagious diseases legislation, at times combining the two by targeting female prostitutes, blaming them for the spread of syphilis in male populations. Like medical discourses, these popular texts did not relate prostitution to GPI. Other medical sources, such as the mental hospital records interrogated in the next section, demonstrate that syphilis became a more dominant but not yet universal aetiological factor in GPI as the nineteenth century drew to a close. Moreover, references to prostitution in discussions about GPI continued to be omitted.
The causes of general paralysis of the insane in the Auckland Mental Hospital
Sixty-eight patients were admitted to the AMH with GPI between 1868 and 1899. These patients were overwhelmingly male, mostly aged between 35 and 50, and were likely to be married. They had a variety of occupations, but were generally mariners or sailors. Only a small percentage of these 68 GPI cases were attributed to heredity, but the proportion of cases said to be caused by vice increased noticeably towards the end of the period, although in these cases vice did not strictly refer to syphilis. Table 1 shows the number of patients admitted to the AMH with GPI each year, and illustrates the cause to which each GPI case was attributed. The table shows that no GPI cases admitted up to 1879 referred to heredity as a cause of illness, and only four of these cases, out of a total of 21 admitted mentioned vice. Examples from these cases mentioned vice in ways such as ‘a drinking propensity appears to have been the cause of his malady’, and patient has ‘been a rather hard drinker’ (YCAA 1048/1: 178). Aside from intemperance in alcohol, there were no other specifically identified causes of the condition for the GPI patients admitted during this period.
Number (N) of patients admitted to the AMH between 1868 and 1899 with the diagnosis of GPI, and stated cause of condition.*
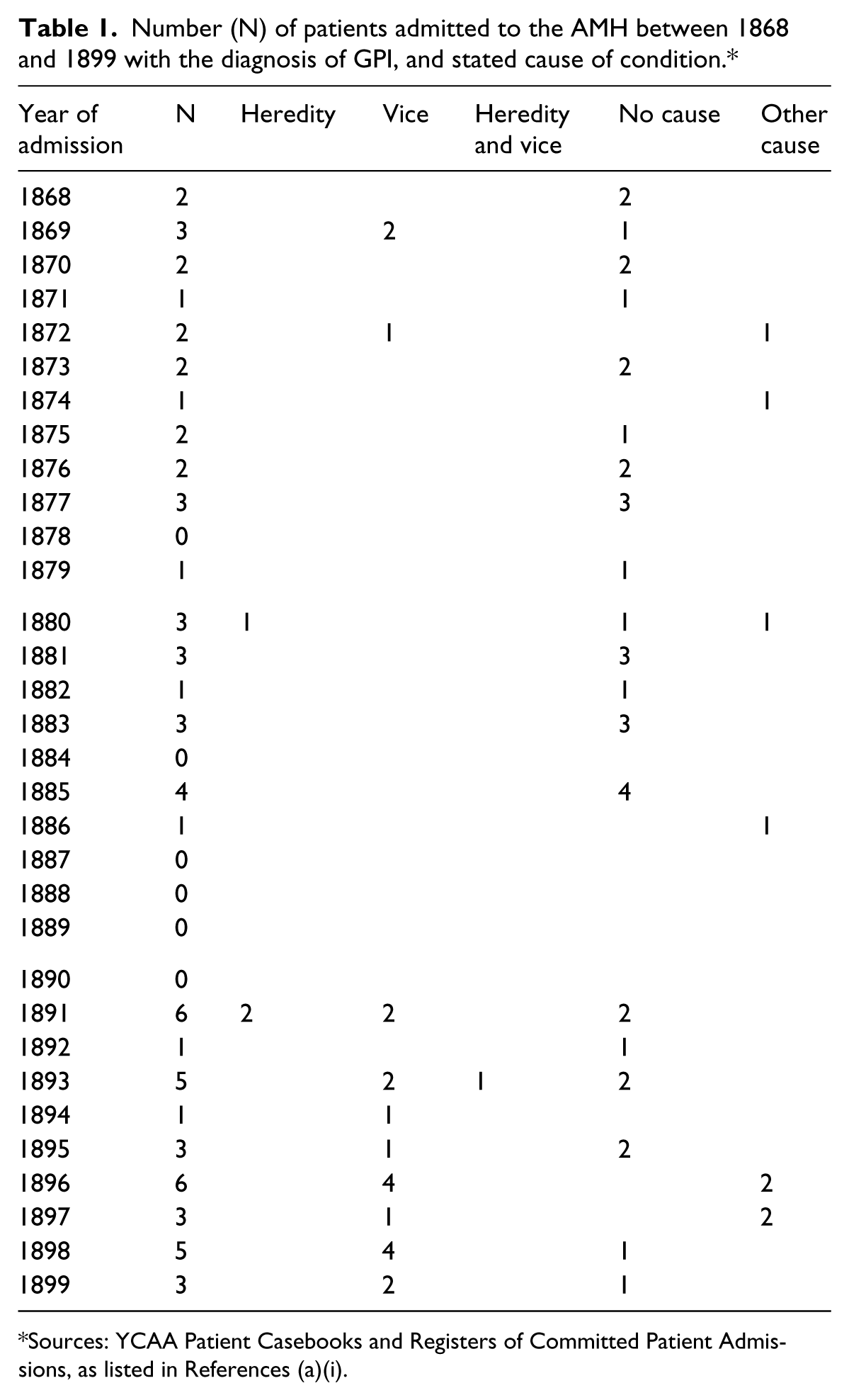
Sources: YCAA Patient Casebooks and Registers of Committed Patient Admissions, as listed in References (a)(i).
This table also shows that 11 patients were admitted to the AMH with a diagnosis of GPI during the 1880s. Once again, these patients were all male, and there were few explicit causes suggested for the development of the condition. The occupations of these patients was quite different the from occupations of GPI patients referred to in the Tuapeka Times (Anon., 1889), as it comprised labourers, painters, gum diggers and carpenters, and was a far cry from the highly educated, middle class men discussed in the press and by Dr Savage (1890: 778). Instead, these GPI patients conformed more closely to the traditionally constructed ideals of masculinity in nineteenth-century New Zealand, a world characterized by gold rushes and itinerant and often immigrant men, part of James Belich’s ‘crew culture’, attracted to distant and dangerous places by promised riches (Belich, 1996: 428–32).
One patient, shown in the ‘Other cause’ box for 1880, was described in his case notes as living ‘a sober and industrious life’, but had previously fallen on his head, which had prompted a fit, at which time he had ‘got queer and becoming uncontrollable and dangerous’ (YCAA 1048/3: 107). The initial reference to a sober and industrious life implies that a history of drunkenness would be the immediately suspected cause of GPI, justifying the need to discount it. Another patient, represented in the ‘Heredity’ box for 1880, was admitted to the mental hospital with no other explanation given for his condition other than that his brother was a former AMH patient, who had committed suicide (YCAA 1048/3: 162). Apart from this, there were no references to heredity evident in the GPI patient case notes from the 1870s or 1880s. The sole reference to vice that did not imply it was the cause of the patient’s condition related to a patient who ‘eats gluttonously’, and asked for ‘fourteen gallons of beer, fourteen gallons of whiskey, or fourteen he does not know what of tobacco’ (YCAA 1048/5: 195). The only other GPI patient with an assigned cause of his condition was a man suffering from ‘Worry and anxiety about having a wife and large family, and being out of work, owing to dull times’, indicated in the ‘Other Causes’ box for 1886 (YCAA 1048/4: 215). Patient case notes at the AMH during the 1880s were dedicated to recording the patients’ symptoms, and only rarely speculated as to the cause of the patients’ conditions. Those causes that were recorded in no way referred to syphilis, any sort of venereal disease, or sexual impropriety and excess. This is in contrast to a number of articles in British medical journals, and may be due to the nature of patient case notes, which were perhaps more conservative than an article in a medical journal. Articles in medical journals provided a forum for doctors to forge their reputations among peers and potential employers, so they may have written about patients and GPI in a more controversial or provocative way than in a non-public medium, such as patient case notes. The discursive differences between medical journals and patient case notes may also be attributed to differences between New Zealand asylum medicine and its British counterpart, as perhaps those working in New Zealand mental hospitals were genuinely less concerned about aetiology than those working in Britain were. Another possibility is that doctors working at the AMH simply did not know why GPI patients had become ill and were unwilling or unable to speculate on the cause, due to the inherent overcrowding, underfunding and understaffing of public institutions in this period.
Table 1 also shows that the GPI population at the AMH increased substantially in the 1890s, compared with previous decades. Patient case notes included greater detail than those recorded in the 1870s and 1880s, and provided causes of the condition and background of patients’ lives. GPI patients admitted during the 1890s had a variety of occupations, ranging from those similar to the ‘bankers, lawyers and editors’ discussed in the Tuapeka Times, such as capitalists, clerks and insurance agents, to the less reputable categories of prisoners, paupers, bushmen and makers. This greater detail was inconsistent, and a cause of the patient’s condition was not always included. Causes related to vice featured fairly frequently by the 1890s, with one 1890 patient’s case note simply stating that the patient ‘was caught in the act of masturbation in the police cell. Dr Callan’s (admission) certificate is to the same effect’ (YCAA 1048/5: 437). Another patient’s case note stated bluntly: ‘supposed cause masturbation’ (YCAA 1048/5: 619). Other patients’ conditions were blamed on purely physiological causes, such as ‘kidney failure’ or ‘insomnia’, both of which may have masked the role of syphilis in the development of GPI (YCAA 1048/5: 569; YCAA 1048/6: 381). The table also illustrates that by the 1890s heredity was recognized as a supposed cause of GPI at the AMH. One ‘heredity’ case was that of John S, admitted in 1891, who was diagnosed with ‘all the symptoms of a general paralytic in a marked degree’ which was ‘probably hereditary (his brother is said to have committed suicide)’ (YCAA 1048/5: 677). Alfred T, a married cheese-maker from Waharoa, a small rural township in the Waikato region of New Zealand, was admitted to the AMH in 1895 with a diagnosis of GPI. According to his wife, who is quoted in Alfred’s case note, none of his relatives was insane and he had always been temperate in habits (YCAA 1048/6: 439). But other relatives testified that Alfred’s sister had been ‘subject to epileptic fits for years’ and that Alfred himself would ‘drink heavily’ on occasion (YCAA 1048/6: 439), as indicated in the ‘Vice’ box for 1895. Coleborne (2010: 82–4) provides further examples of interactions between families of patients and doctors working in mental hospitals.
Vice was a more frequently cited cause of GPI in the 1890s than heredity. Patient Bryan H (see ‘Vice’ box for 1893) was diagnosed as a general paralytic ‘probably caused by injury, a fall in a lift a few years ago’, and Bryan’s wife was quoted in the case note as saying that there was ‘no hereditary taint of insanity, [he] was not addicted to drink or other vices’; however, the case note also documented comments made by the police that Bryan was ‘a heavy drinker, this is corroborated by others’ (YCAA 1048/6: 77). This somewhat peripheral reference to vice was fairly typical of those case notes that mentioned vice at all. One particularly interesting case note is from Pourari K, a ‘halfcaste’ patient from a small settlement near Kawhia, on the Waikato coast, shown in the ‘Heredity and vice’ box (YCAA 1048/6: 141; see also Barry and Coleborne, 2011: 285–301). Pourari’s GPI was attributed to ‘a land court case and religious excitement’ (YCAA 1048/6: 141). Several members of his family were described in his case note as ‘hard drinkers, as also was the patient til he joined the Salvation Army’ (YCAA 1048/6: 141). There are no further details provided about the land court case or the patient’s religion, but the reference to both heredity and vice, in that both Pourari and his parents drank, matched published British medical theories and popular ideas expressed in New Zealand newspapers. Family history was mentioned in just three other GPI cases from the 1890s, and these references were consistently to the effect of there being ‘no history of insanity in the family’, so is not recorded in the ‘heredity’ column of the table (YCAA 1048/7: 77). In many GPI cases admitted to the AMH there was no family history provided at all, even as late as the 1890s. This may indicate that family history was no longer considered significant to a patient’s condition or – perhaps more likely – there was no family history provided due to the isolated lifestyles of many GPI patients, away from family or anyone able to provide a family history to asylum doctors. This is sustained by the occupations of the patients, as discussed earlier, many of which promoted an itinerant lifestyle (Belich, 1996: 428–31; Phillips, 1996: 19–26). One example of this is Christopher C, admitted to the AMH in 1894 and shown in the ‘Vice’ box for that year. Christopher was born in Greece and had worked as a seaman (YCAA 1048/6: 267). While his condition was attributed to masturbation, his case note reveals that there was no consideration of heredity or family history as being a cause of his condition, as ‘no one seems to know anything of his history, and he is quite unable to give an intelligent account of himself’ (YCAA 1048/6: 267). Sailors such as Christopher, as well as miners and others employed in ‘frontier’ occupations, lived in a world that historians have described as a hotbed of binge drinking, gambling, prostitutes and other vices. Australian medical historians Alan Stoller and R. Emmerson (1869: 608) speculate that higher incidences of GPI in the 1880s and 1890s were the aftermath of the gold rushes, and the associated ‘residuum of unattached migrant males’.
The most significant difference between GPI patients admitted to the AMH in the 1890s and those admitted in earlier decades is the noted presence of syphilis in the 1890s case notes: of the 33 patients admitted with GPI, six had GPI due to syphilis or ‘sexual excess’ (YCAA 1021/1,2,3). This change over time suggests that practices at the AMH, and perhaps in New Zealand medicine more generally, were beginning to keep pace with changes in medical theories about GPI operating overseas. As well as these six patients, vice in the form of intemperance in alcohol or masturbation was an identified contributing factor in an additional 11 cases. However, other causes persisted in the patient case notes, as Wilhelm F, a married storekeeper represented in the ‘Other Causes’ box for 1897 was diagnosed with GPI due to ill health, phthisis and ‘business worries’ (YCAA 1048/7: 98), while George W’s GPI was blamed on ‘heat of sun and want of food’ (YCAA 1048/7: 101). The various causes cited at an institution such as the AMH mirror the reluctance of doctors working at mental hospitals in other countries, such as the REA, to fully embrace a syphilitic aetiology. This is significant given that the AMH was so distant from Clouston’s place of work and those of other doctors who contributed to the BMJ and the JMS. Perhaps more significantly, there were no obvious moral or financial reasons for doctors working at the AMH to deny whether a patient had syphilis in their case notes, such as the reasons proposed by Thompson in the context of the REA in nineteenth-century Scotland.
The content of AMH patient case notes for GPI patients shows further continuities with Scottish mental hospitals. In the Scottish examples presented by Davis, ‘thickness of speech’ was considered so characteristic of general paralysis patients that patient case notes often referred to a patient as having ‘speech like a GPI’ (Davis, 2008: 91). There was also a shared notion of typical ‘general paralytic’ handwriting (p. 92). Both handwriting and speech were frequently remarked on in AMH case notes for GPI patients, to a far greater extent than for other diagnoses.
The existing climate of concern about prostitutes and syphilis in popular and medical sources, and the strengthening connection between syphilis and GPI in medical discourses, makes the absence of female prostitutes from the AMH records, as GPI patients, remarkable. 8 The five women who were admitted to the AMH with GPI between 1868 and 1899 appear to have been members of the ‘respectable classes’, and included an ‘old woman’, a housewife and a widow (YCAA 1048/1: 132; YCAA 1021/1). The much larger number of male GPI patients than female, as discussed by Mickle (1886), fits the pattern at the AMH, and the even broader gender imbalance at an antipodean institution may be explained by New Zealand’s overall gender imbalance in the mid- to late-nineteenth century. 9
Conclusion
The aetiology of GPI was a strongly disputed topic in nineteenth-century medicine, in particular the roles of syphilis, alcohol and the effects of ‘modern life’. Alcohol was originally suggested as a likely cause of the condition, although this may have been as a result of confusion and misdiagnosis between alcoholic insanity and GPI. Even as syphilis became more popular in medical thought as a cause of GPI, the condition remained completely detached from prostitution, which had long been acknowledged as a leading ‘cause’ of syphilis in both medical and more general discourses. Furthermore, despite a reportedly greater prevalence of GPI in ‘port cities’, known as strongholds of prostitution, there was a notable reluctance by doctors to seize on this connection.
Thompson (1988) and Davis (2008) have contemplated the seeming selective awareness of developments around the syphilitic aetiology of GPI in Scotland, and have focused on the predicament Clouston faced due to a formal association of GPI patients with sexual vice. Clouston was not alone in his reluctance to embrace the causative role of syphilis, nor was it the sole domain of Scottish and English asylum medicine. While doctors working at the AMH were exposed to many of the same ideas as their British brethren, through medical journals and their origins or training, they too were reluctant to identify syphilis as a cause of GPI in patients under their care, without encountering many of the pressures that Clouston faced.
This article has adopted a form of analysis based on a variety of textual sources, some of which were intended to be read by the public and by medical practitioners, others which merely sought to record medical ‘facts’ about individual patients. Analysis of these sources has revealed underlying concerns about heredity and vice in nineteenth-century medicine and wider society, by using a single diagnostic category to examine how ideas about heredity and vice were implicated in nineteenth-century medical theories, and to demonstrate the ways that medical ideas could become mobile and were shared between very distant locations, in a number of ways.