
Abstract
Kurt Schneider’s insight nearly 80 years ago that schizophrenia could be demarcated from other psychoses by a small set of particular delusions and hallucinations powerfully influenced diagnostic practice. The theoretical status of such ‘first rank symptoms’ as a whole, however, has rarely been addressed. But if they are sensitive and specific to the condition, it is about time that their essential nature and potential origin be considered. This is the purpose of the present paper. I argue that these psychopathological phenomena are indeed relatively sensitive and specific to the condition, that their nature can be formulated within a Schelerian model of what constitutes a human being, and that their origin fits anthropological and neuropsychological notions of the make-up of contemporary human beings.
Introduction
The first publication in which Kurt Schneider mentioned first rank symptoms of schizophrenia (Symptome I. Ranges) is a monograph of 1939 entitled Psychischer Befund und psychiatrische Diagnose (roughly translated as ‘Mental State Findings and Psychiatric Diagnosis’). He described a selection of types of delusions and hallucinations which he considered were of critical importance in distinguishing schizophrenia from other psychotic conditions.
This was a watershed in the history of psychiatry for a number of reasons. First, Schneider eschewed Kraepelin’s reliance on the course of a condition as having any diagnostic value: ‘Die psychiatrische Diagnose grundet sich für uns grundsätzlich auf die Zustandsbilder, auf die Symptomatik und nicht auf den Verlauf. (Psychiatric diagnosis is in my opinion fundamentally based on the pattern of the mental state, on symptoms, not on the course of any condition.)’ (Schneider, 1939: 9). Second, he disputed Bleuler’s and others’ claims that the identification of an intrinsic disturbance of thinking could seal the diagnosis: ‘Leichtere Grade von Zerfahrenheit gibt es aber überall … in aufregenden Situationen, im Rausch, im Fieber. (Mild forms of thought disorder are widespread … in (normal) agitation, in drug-induced states, and during fever.)’ (p. 14). In fact, like his mentor Jaspers, Schneider was sceptical of any claim as to a specific psychological underpinning of schizophrenia.
Third, he was not troubled by the fact that the first rank symptoms he had described had no shared phenomenological basis. He offered them simply as a helpful pragmatic standard. This is expressed in subsequent amplifications of his 1939 monograph – in the various editions of his Klinische Psychopathologie and other articles. Here are his views on the matter from the fifth edition of Klinische Psychopathologie (1958) which was translated as Clinical Psychopathology (Schneider, 1959: 134):
We are far from being able to presume a common structure for all these symptoms of first-rank importance. Some can certainly be regarded as a group which represent the ‘lowering’ of the ‘barrier’ between self and the surrounding world … thought-withdrawal, passivity thinking, diffusion of thought, and all passivity experiences, whether feeling, drive or volition, may be involved. The characteristic hallucinations … and delusional perception, however, cannot be brought into this group without resorting to speculative constructions.
In an article in 1949, entitled ‘Notiz über Ichstörungen und Entfremdungen’ (Memorandum on disturbances of the self and alienation), Schneider discusses disorders of self-awareness in general and mentions the sense of Meinhaftigkeit (myness) and its psychopathology, but does not link any of this with his earlier identification of first rank symptoms. In 1957 Schneider (1957/1974) writes that first rank symptoms are: ‘not theoretical possibilities but are intended only for pragmatic diagnostic use’.
Fourth, for someone whose early academic theses were supervised by the philosopher Max Scheler (1874–1928), eulogized by Heidegger (1928/1992) as the greatest contemporary philosopher, it is odd that Schneider never attempted a proper theoretical account of them, never mind a philosophical formulation, even more so since he had attempted this very thing in the case of depressive illness in 1920 (Schneider, 1920).
To my mind there is something very unsatisfactory about all this, because although Schneider shifts the whole notion of schizophrenia in a specific direction – undermining the previous reliance on course as a diagnostic indicator, thought disorder as an essential element, and theoretical formulations of any sort – the value, nature and origin of the psychopathological markers which he promotes are not properly addressed. This situation has in no way been resolved in the intervening decades, which has led to the fact that first rank symptoms have been rather side-lined recently.
What seem to me to be the outstanding questions are: (1) Are first rank symptoms as diagnostically valuable as Schneider maintained? (2) If so, what is their nature, if indeed they do share a common phenomenological pattern, something that Schneider anyway denied? (3) If they do have a diagnostic value and a shared phenomenological essence, can they be traced back to their origin, whether in psychological, neuropsychological, anthropological or philosophical terms? The purpose of this article is to answer or attempt to answer these questions.
Diagnostic value of first rank symptoms
A handful of investigators in the 1970s and 1980s tackled the problem of whether first rank symptoms have a diagnostic value, singly or as a group, over other psychopathological markers. Four critical issues emerged, all interrelated: (1) the sensitivity of the symptoms to the condition, i.e. how frequent are they in schizophrenia diagnosed by other means; (2) their specificity, i.e. how often do they appear in other psychiatric conditions; (3) the variability in how a subject’s mental state is assessed with respect to their presence or absence, and how this impinges on sensitivity and specificity; and (4) their status as a gold standard for the diagnosis of schizophrenia vis-à-vis other psychopathological criteria.
(1) The frequency of first rank symptoms in schizophrenia diagnosed by the Research Diagnostic Criteria (Spitzer, Endicott and Robins, 1975), the forerunner of DSM, early DSM versions themselves, and other schedules, varied between 28% and 72%, averaging about 50% (Mellor, 1982).
(2) The frequency of first rank symptoms in psychotic depressives is very low – 4% (Wing and Nixon, 1975) – and in manics it averages around 10% (Mellor, 1982).
(3) There is considerable variation in how each first rank symptom is evaluated among authors (Koehler, 1979), particularly surrounding the role of self-alienation as the critical determinant. Of significance for the thesis to be developed in this article, the investigator who most emphasized the primacy of self-alienation – Mellor (1982) – found the highest rate of first rank symptoms in schizophrenia: 72%.
(4) There was a flurry of interest in the 1970s in the relative validity of the various diagnostic schemes in currency before DSM monopolized the field. Validity was assessed either by the extent of inter-correlations between individual first rank symptoms (Lewine et al., 1982), or by their persistence over time (Mellor, Sims and Cope, 1981), or by their ability to predict a poor social outcome (Silverstein and Harrow, 1978), which was and still is regarded as a benchmark of diagnostic validity despite Schneider’s censure. Some results of all this – poor symptom inter-correlation, mediocre prediction of social disadvantage – were interpreted at the time as undermining the value of first rank symptoms, even though other results – the persistence of the same first rank symptoms episode by episode – were a positive index of some intrinsic stability. Mellor in Britain and Koehler in Germany were enthusiastic advocates of their continuing value, whereas American psychiatrists were less convinced.
In summary, the diagnostic value of first rank symptoms is not as dire as their reputation has been made out to be. A sensitivity of nearly three-quarters in two studies (Koehler, Guth and Grimm, 1977; Mellor, 1982) and an acceptable specificity (4% in psychotic depressives and 10% in manics) are impressive, and the supposed deficiencies in validity are themselves based on questionable measures of validity itself.
The nature of first rank symptoms: historical perspective
The nature of these symptoms as a whole was barely tackled. Schneider himself referred to a sub-set emanating from ‘Die eigenen Akte und Zustände nicht als solche eigene, sondern als von andern gelenkte und beeinflüsste erlebt werden (a person’s own acts and mental states are not experienced as their own, but as something controlled and influenced).’ (Schneider, 1971). But he could see no plausible explanation for the species of auditory hallucinations or delusional perception which he had linked with such experiences.
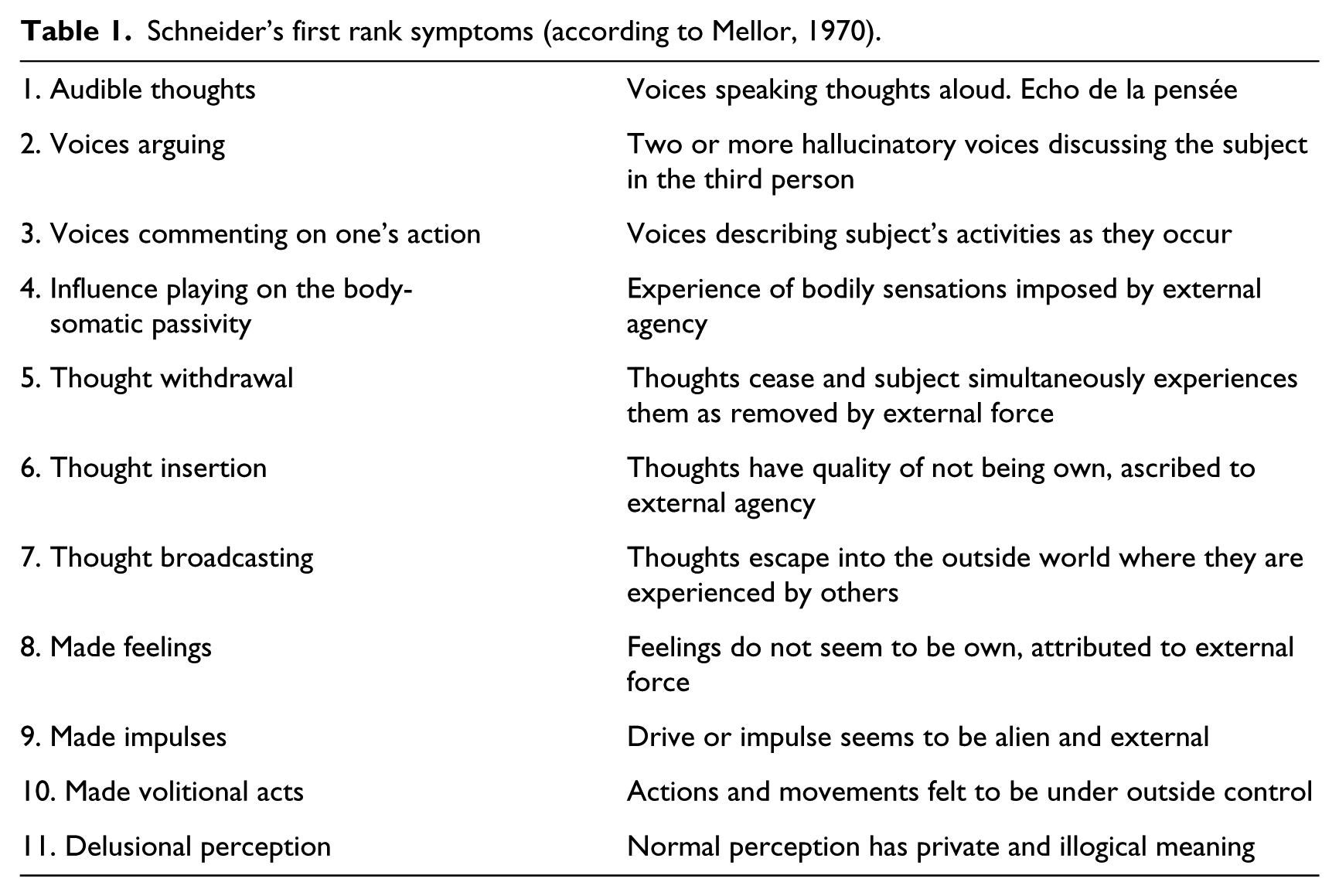
Sims (1991) was more adventurous, and proposed that all first rank symptoms – see Mellor’s (1970) rationalization of these in Table 1 – could be conceived of as varieties of Ichstörung (ego disturbances or lack of myness): the hallucinations resulting from leaky boundaries between self and non-self, and hence one’s thoughts became invested with an alien and objective quality; delusional perception illustrating the converse, with what was actually an external, neutral event being imbued with personal meaning.
Schneider’s first rank symptoms (according to Mellor, 1970).
If we now join all this up with another theme in the historical development of the schizophrenia concept, we can see that this notion of the schizophrenic as an anomalous self-experiencer is the culmination of a number of abortive attempts to portray the essence of the condition. All these are well known among psychopathologists but are worth summarizing and critiquing because of their blatant naiveté or over-generalized applicability.
Kraepelin’s view, reliably attributed by Gruhle (1929: 141), was that the sufferer from dementia praecox, the forerunner of schizophrenia, was lacking in some overall mental controller: ‘a weakening of those emotional activities which form the mainspring of volition … [in short] an orchestra without a conductor’. But it is doubtful if any normal person has such a controller. Look at case histories of subjects whose corpus callosum has been damaged; for example: ‘I came to the lobby because I wanted to smoke, but another vague desire occurred and prevented me from smoking … The more I wanted to move, the more I became frozen.’ (Nishikawa et al., 2001). Two competing volitional alternatives are exposed, and it can hardly be that a band of fibres is the overall controller.
Bleuler’s (1911/1950) suggestion was that the condition stemmed from a loosening of associations, a thesis that applies better to manics, whereas schizophrenics, according to Spitzer, Braun, Hermle and Maier (1993), are more alert to the dominant linguistic connotations of a word. Max Scheler (1928/2009: 18), moreover, whose critique of psychology was superbly acute, regarded an associative frame of mind as a feature of senility, and any deviation from this a sign of youth and vitality, hardly an apt description of the schizophrenic.
Minkowski’s (1927/1987: 193) basic formula for schizophrenia was a ‘loss of vital contact with reality’, and although some other suggestions of his about schizophrenia – morbid rationalization, pragmatic dementia – hit the nail on the head, in my view his core notion of a loss of vital contact with reality is too vague, and begs the question as to what is meant by ‘reality’ in this context. The normal and the schizophrenic must both have some vital contact with the physical, physiological, psychological and social tiers of reality, otherwise they would not survive. It is rather that each differs from the other in what actuality they engage and experience of all this, in which case we are back to square one.
Two other great psychopathologists of the last century – Binswanger and Blankenburg – proposed variations on Minkowski’s theme: an immobilization of the flow of life with a compensatory theoretical take on everything (Binswanger, 1956/1987); and a fundamental flaw in common sense or natural attitude, which rendered, what in normals was an automatic attunement to life, in schizophrenics exaggerated, eccentric and artificial (Blankenburg, 1969/2000). Again, their insights are almost certainly correct, but too woolly to be translated into any diagnostic or robust theoretical framework.
We return to Kurt Schneider because the most prevalent notion as to the essence of schizophrenia in recent decades has been a variation on what he tentatively saw as a phenomenological principle underlying the majority of his first rank symptoms – a blurring of the individual’s sense of what was subjective and what objective. Parnas (2000), Sass (2003) and Stanghellini (2004) have all homed in on what they call a lack of ‘ipseity’ in schizophrenia – a ‘lack of myness’ (in English), a lack of Meinhaftigkeit or Ichstörung (in German), a loss of moiété (in French). The German psychiatrist Fuchs, who holds the chair in Heidelberg that Schneider once held, sees the schizophrenic as someone who is not bound to their bodily needs, but is detached from these as if their experience were now anybody’s (Fuchs, 2005).
In summary, there is something about the first rank symptoms of schizophrenia, at least some of them, which resonates with the contemporary notion of the condition as a detachment on the part of the subject from acknowledging the ownership of experience. Whose experience am I having? Is it my experience? Who is behind it all?
The nature of first rank symptoms – a critique
All we have to go on from our historical perspective is that some first rank symptoms of schizophrenia manifest the contemporary consensus among psychopathologists that the essence of schizophrenia is something to do with an attenuated ‘myness’ in experience. Sims’ (1991) proposal was that all of them could be brought under an umbrella of such dilapidation, but he had to distort the nature of the auditory hallucinations and delusional perception to achieve his aim, and by attributing the latter to an enhanced sense of myness he undermined the very notion of ‘lack of ipseity’ and its synonyms.
Looking at Mellor’s rationalization of Schneider’s first rank symptoms (Table 1), it is clear that seven of the 11 do involve a lack of myness: tactile experience is not mine, thoughts are hijacked by someone else, thoughts are simply not my own, thoughts are no longer private, and feelings, drives and actions all take on an alien quality. So far so good for lack of myness as an overarching explanation for schizophrenia.
But what about the three sorts of auditory hallucinations? They are not obviously anything to do with a lack of myness, despite what Sims claimed. What they have in common is rather an anomalous spatial disposition. What should be in the mind and, therefore, as Max Scheler (1913–16/1973: 417) said about the essence of anything psychic in this respect, possessing the quality of Ineinandersein (interwovenness), is no longer in the mind but projected outside, now possessing the spatial quality of Aussereinandersein (extensionality). Hoffman’s (1986) formulation of ‘voices’, to the effect that they are preconscious fragments of thought prematurely given actuality, also supports the notion that an anomalous spatiality essentially underlies them. The recent work of Stephane and colleagues (2010), demonstrating that schizophrenics who experience ‘voices’ blur external and internal space, as if the boundaries between these were porous, is further evidence of the central role of anomalous spatiality in these psychopathological phenomena. One is therefore drawn to the conclusion that schizophrenics, as well as suffering a disturbed sense of myness, are affected independently by an anomalous sense of spatiality. Moreover, as auditory hallucinations occur in around half of all schizophrenics (Cutting, 2003), if a loss of myness cannot satisfactorily explain them, whereas anomalous spatiality – a disturbed sense of whereness – can, this is the first nail in the coffin for the ‘lack of ipseity’ thesis as an overriding psychopathological explanation for schizophrenia.
The remaining first rank symptom to be considered in this critique is delusional perception. A man in the street is talking to another man and crosses his fingers. What he is in fact doing is explaining to his friend a building project that he is engaged in. A schizophrenic, however, looks at the man and sees a cross; the cross is meant for him; the schizophrenic concludes that he, the schizophrenic, is being summoned for some religious purpose. What of loss of myness here? Conrad (1958: 53) commented on one of his patients with delusional perception: ‘Wherever Karl B’s glance falls every component of his experiential field appears to stand in a special relation to him … His “world” becomes transformed into a situation specifically meant to test him.’ No lack of myness here; if anything, the complete opposite: a sense of heightened myness. Everywhere the man looked, everything was imbued with a meaning for him. Delusional perception is quite common too. In Conrad’s series of 107 subjects with early schizophrenia, almost all had delusional perception. So, if delusional perception cannot be explained within the confines of a ‘lack-of-myness’ concept, then schizophrenia itself is not comprehensively accounted for in this way either. (What delusional perception might be is considered later.)
We appear to be stumped, as was Schneider, in uncovering a single phenomenological principle behind first rank symptoms. But an acquaintance with the history of psychiatry sometimes reveals that what seemed by-ways and dead-ends at the time were, in retrospect, founts of insight. One such is the current psychopathological notion of delusional misidentification. Joseph (1986) is largely responsible for having brought together under this label a number of case reports in the early twentieth-century French literature with various names, e.g. Capgras syndrome (Capgras and Reboul-Lachaux, 1923), along with seemingly neuropsychiatric oddities such as reduplicative paramnesia (Pick, 1903), and more recent miscellaneous cases, e.g. the syndrome of subjective doubles (Christodoulou, 1978). A German literature on Personenverkennung should be added to this (Mojtabai, 1996). From our vantage point the particular syndromes and their status vis-à-vis others of the same ilk are not important. What is of interest, however, is the range of the psychopathological entity and how this guides any view as to its nature.
Vié (1944: 248), for example, described a man who had fought in World War I and who, years later, after a cerebrovascular accident, denied that the war had been a unique event in history. He did not repudiate the existence of the event nor his participation in it, but deemed it ‘une guerre d’expérience (an experimental war)’, and when asked about the carnage and devastation replied: ‘It is a custom every year to pay certain local authorities to put on a real exhibition of shooting in their district.’ Petho’s (1985) patient, diagnosed as schizophrenic, believed that everything that happened to her had happened before and, for example, when she and her husband were building a house, she would not allow one of the walls to be built in the planned place because ‘it caused trouble in my previous life’.
What the psychologists who have ventured into this area have failed to appreciate, and have hence come up with lame explanations invoking face perception deficits (Ellis and Young, 1990), is the enormous range of the entity, involving issues that are nothing to do with the psychological deficit proposed. There are even case reports of blind people with Capgras’ syndrome (Rojo, Caballero, Iruela and Baca, 1991; Reid, Young and Hellawell, 1993), which undermine such theses from the outset. What does ring true, however, is a suggestion from Cutting (1991) and Margariti and Kontaxakis (2006) that the common thread in all instances of delusional misidentification is a loss of the sense of uniqueness in experience. What has been ignored, which strongly supports the above, is the fact that the subject with delusional misidentification not only denies the identity of someone or something (or some time or some place) – and the focus can be Wellington boots, which is another blow to a face perception deficit – but deems the misidentified object one of several extant identical instances. In other words an X is not just non-X, which can call forth all sorts of psychological theories about why this might be so, but is an X multiplied indefinitely, which no purely psychological theory has any hope of explaining.
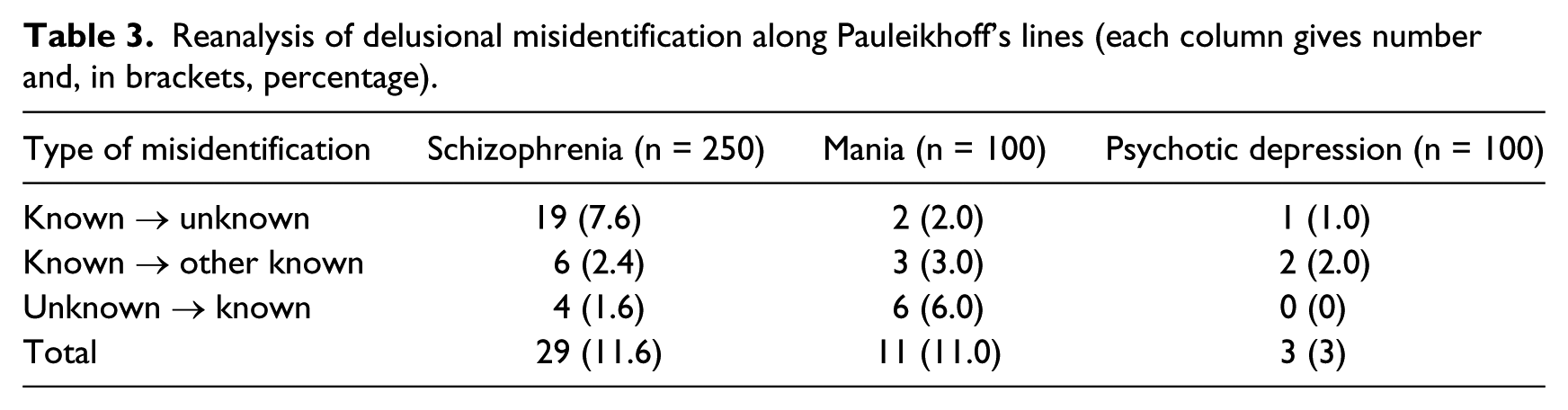
Luckily, some German literature on the issue can help us out here. In a forgotten article by Pauleikhoff (1954), a colleague of Schneider in Heidelberg, the nature of Personenverkennung is discussed. Pauleikhoff believed that there were two sorts of Personenverkennung, one in which a known person’s knownness was denied, and another in which an unknown person was deemed known. Pauleikhoff claimed that the former was a ‘first rank symptom’ of schizophrenia, the latter an accompaniment of a variety of psychiatric disorders. This is an extraordinary claim, particularly since Schneider and all the other great psychopathologists of the twentieth century showed little interest in delusional misidentification. But, despite Pauleikhoff giving no data to support this claim, an analysis of some data by Cutting (1997) strongly supports his thesis and, in my view, should add ‘delusional misidentification of a known person as unknown’ to the list of first rank symptoms. Table 2 shows the proportion of delusional misidentification of any sort in the three psychoses – schizophrenia, mania and depressive psychosis – from Cutting’s data, and, although depressives rarely experience this, schizophrenics and manics do so to equal degrees. But when one re-analyses the data according to Pauleikhoff’s suggestion (Table 3), the truth of his insight becomes clear. Even allowing for a third version of delusional misidentification, where a known person is mistaken for another known person, the schizophrenics are now overwhelmingly contrasted with the other two diagnostic groups by their experiencing a known person as unknown, i.e. sensing a lack of whoness about someone else.
Incidence of delusional misidentification of any sort in psychosis.

Reanalysis of delusional misidentification along Pauleikhoff’s lines (each column gives number and, in brackets, percentage).
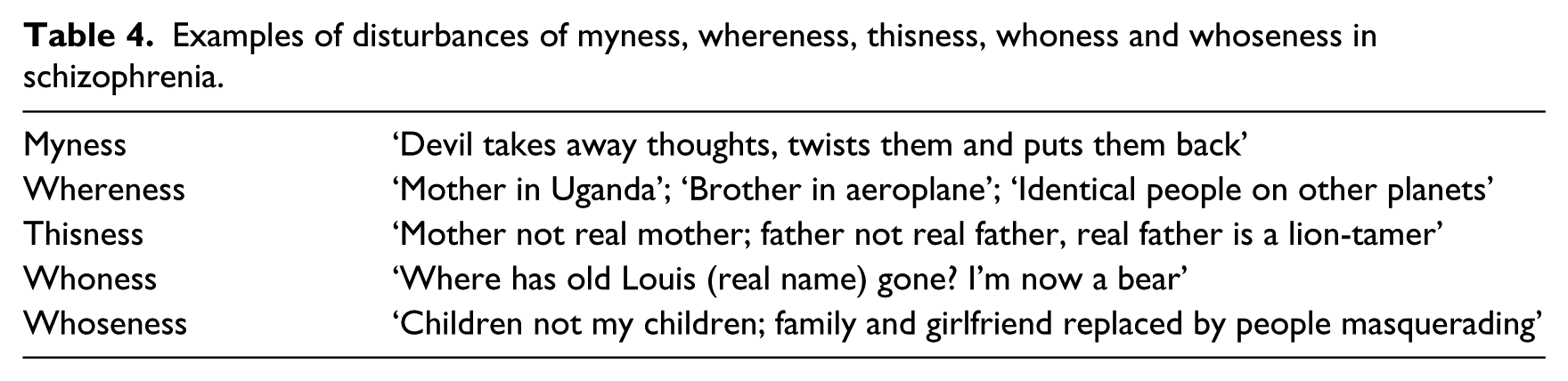
Warming to our theme, we can say that not only are there disturbances in the experience of myness and whereness in schizophrenia, but also in the sense of uniqueness, which, depending on whether the object being experienced is a thing or a person, we can refer to as disturbances in the experience of thisness, whoness and whoseness. Examples from Cutting’s (1997) psychopathological data are given in Table 4.
Examples of disturbances of myness, whereness, thisness, whoness and whoseness in schizophrenia.
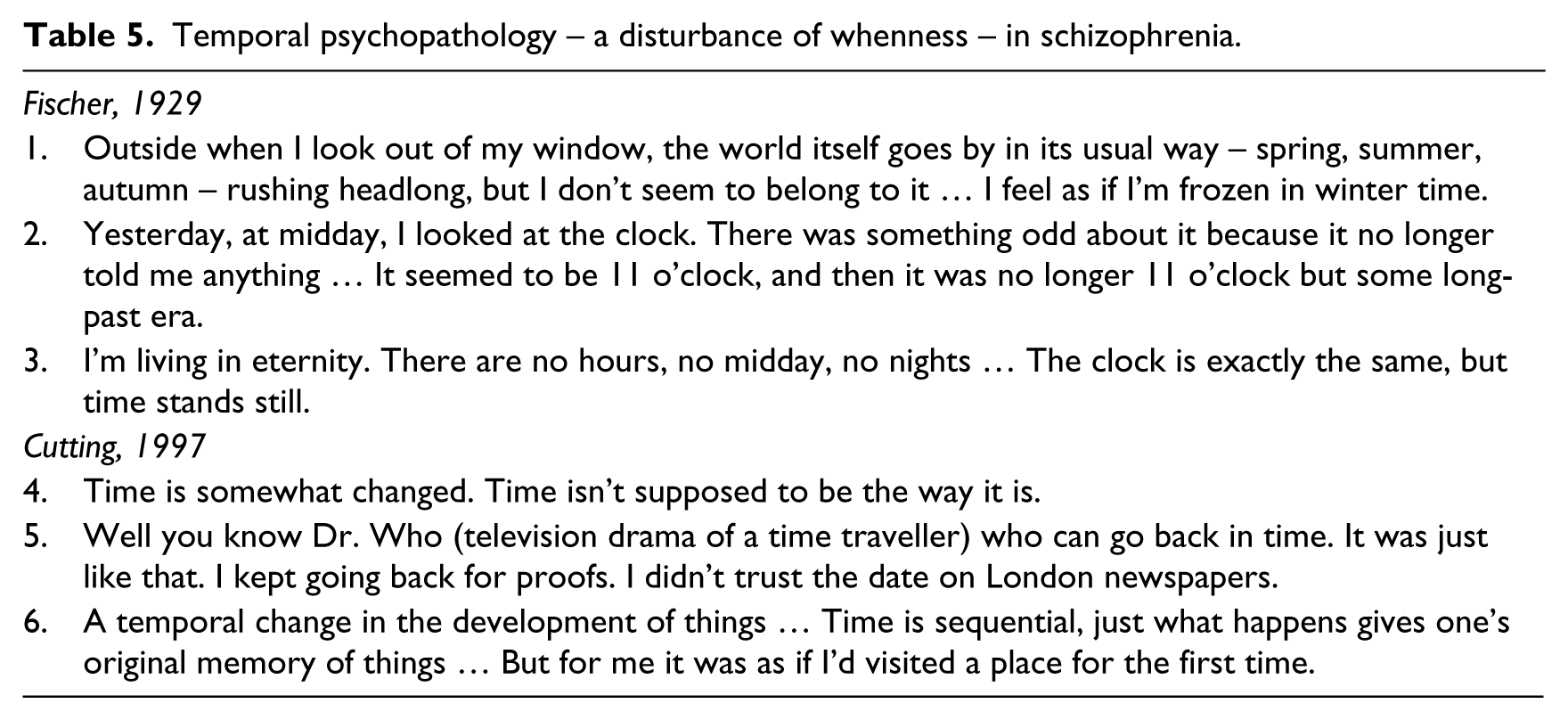
The last issue germane to the developing theme is the extraordinary breakdown in temporality that pervades some schizophrenic’s experience. This too is something that only someone with a curiosity for the history of psychiatry could know, because it appears in none of the various diagnostic systems that jostled for recognition in the 1970s and 1980s and is absent from any version of DSM. Indeed, apart from Minkowski, who fashioned his psychopathological oeuvre around anomalous temporality, no other great psychopathologist was struck by the peculiarity. Such experiences are admittedly uncommon, but those that have been reported (Table 5) are quite specific to the condition in my experience and are different from the anomalous temporality of manics and depressives. There is a strange breakdown in the entire temporal structure of existence: subjective and objective time completely out of kilter (case 1), clock time unreliable (case 2), time stopping (case 3), a general sense of time being awry (case 4), contemporary measures of time being doubted (case 5) and temporality itself dissolving (case 6). What these experiences indicate is that a disturbance of whenness occurs in at least some schizophrenics, and that this should be added to our list of other disturbances, myness, whereness, thisness, whoness and whoseness.
Temporal psychopathology – a disturbance of whenness – in schizophrenia.
Delusional perception has not been forgotten in all this, but its nature is somewhat different from all the other first rank symptoms and can only be properly appreciated, I would suggest, after a consideration of the matters in the next section.
In summary, the official first rank symptoms of Schneider, and others that could have been graced with this label, have been shown to have an underlying substrate of miscellaneous deficits in how a human being grasps the particularity of their world.
The nature of first rank symptoms: philosophical perspective
We have built up an array of seemingly unrelated anomalies in schizophrenic experience, some of them purporting to explain all but one of Schneider’s first rank symptoms, and others possibly underlying first rank symptoms that Schneider missed or did not care to include (Pauleikhoff’s first form of Personenverkennung, a certain sort of anomalous temporality). What we now discover, if we turn to the writings of the philosopher Max Scheler, who has already featured in this article, is that the apparent heterogeneity in our array of disturbances of myness, etc., is indeed only apparent and that they actually constitute a shared conceptual domain.
In his late works (e.g. Scheler, 1924–27/2008: 401–2; 1927–28/1995), Scheler again and again portrayed the human being as something that possessed over and above any other living being the facility of Geist (notoriously difficult to translate into English but best rendered as mind, with connotation of spirit; I shall leave it untranslated in the ongoing discussion). What Geist provided, among other things, was the faculty to grasp the Wassein (whatness) or Wesensein (essence) of something over and beyond any mere happenstance of that something’s here and now existence. The latter, which he called zufälliges Sosein (something’s co-incidental or accidental being-so), was a perspective which the human being shared with other living beings. If you look at any object whatsoever, a distinction between these two viewpoints should strike you straightaway. Take a glass: what it is, its essence, is to be a glass; but it is also an object in a spatial matrix of other things, it is here now in time, it is a unique exemplar of numerous sorts of glasses, it belongs to someone and hence has a whoseness, and it has entered my experience. (If the object is a person the question of who it is can be put.) Whereness, whenness, thisness, whoseness, myness and whoness comprise the zufälliges Sosein of some object with a fixed essence.
The failure to recognize this fundamental dichotomy between the whatness or essence of something and its accidental qualities, along with the human being’s unique facility in respect of the former (unique vis-à-vis all other types of being except God, Scheler thought), was something Scheler held against all modern philosophers, even Heidegger; Scheler (1927–28/1995) criticized the latter for construing a human being in terms which made it no more special in the scheme of things than whatever colour hair it had, or some other such accidental quality. A higher animal can recognize its owner or mate (myness or whoseness), birds have a superb sense of spatial awareness (whereness), and all animals are locked into a web of seasons and diurnal phases (whenness). But, according to Scheler, they do not grasp the essence of anything.
Perhaps because of an ignorance of the above Schelerian dichotomy, no one has fully appreciated the psychopathological principle that if a set of potential attributes or qualities of something is no longer accessible to a knower then the experience that the knower will have of the object will be radically and pervasively transformed, not just missing whatever is unavailable in an otherwise unaltered, premorbid image. Minkowski (1927/1987), among the great psychopathologists, was most aware of the issue, having read and digested Bergson’s notion of a dual facility at the core of the human being for representing the same matter either temporally or spatially with concomitant change in the quality of experience. In the recent neuropsychological and neuropsychiatric literature, there is a growing realization of this, in the form of what Kapur (1996) called ‘paradoxical functional facilitation’ in cases with focal brain damage: another healthy part of the brain, which carried out premorbidly a parallel or complementary sort of function to that of the area of brain now damaged, has now taken on sole charge for tasks which were under dual control hitherto. Braun and Suffren (2011) also saw that delusional states consequent to brain damage could arise in this way, through a combination of deficit in a brain-damaged area and compensation in the healthy homologous area, akin to Jackson’s (1884/1958) celebrated notion of positive and negative symptoms. But only Scheler (1924–27/2008), remarkably in a thought-experiment rather than ‘in vivo’, saw the full gamut of what would happen if a human being were bereft of that part of it which was responsible for both the genesis and the perception of zufälliges Sosein as a whole, which Scheler called Drang (another virtually untranslatable word, but meaning the vital being or animality of the human). Scheler realized that a human being in this artificial state would be running only on what Geist can provide in the way of knowledge, and that would include, as mentioned above, seeing essences or whatnesses of things rather than their co-incidental qualities. (We are, of course, extrapolating his findings to a schizophrenic’s proposed compromised ability to grasp zufälliges Sosein, or some part of it.)
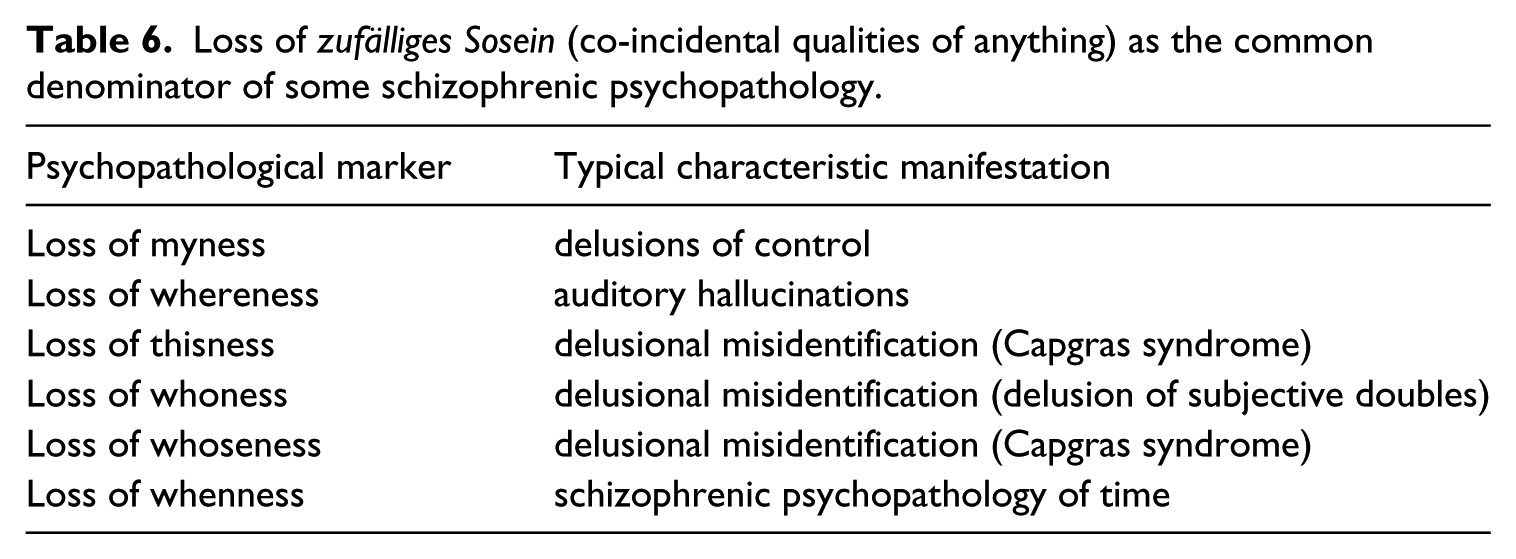
We are now closing in on our enigmatic subject. Table 6 illustrates the sorts of schizophrenic psychopathology stemming from a loss of the sense of zufälliges Sosein. However, the following extracts from two autobiographical accounts by schizophrenics clearly show that each is experiencing a world populated by things stripped of their zufälliges Sosein and displaying their bare whatness or essence: ‘ a round grey stone’ without function; a jug without name, function or meaning. These two schizophrenic patients illustrate the standing out of the essence of something and the falling away of co-incidental qualities.
I am a fascinating creature. I move in no stultifying ruts. There’s no real yoke of custom on my shoulders … My mind goes in no grooves made by other minds … When I look at a round grey stone by the roadside I look at it not as a young woman, not as a person, not as an artist, nor a geologist, nor an economist, but as Me – as Mary MacLane – and as if there had not before been a round grey stone by a roadside since the world began. (MacLane, 1917: 176) Things looked smooth as metal, so cut off, so detached from each other, so illuminated and tense that they filled me with terror. When, for example, I looked at a chair or a jug, I thought not of their use or function – a jug not as something to hold water and milk, a chair not as something to sit in – but as having lost their names, their functions and meanings: they became ‘things’ and began to take on life, to exist. (Sechehaye, 1950/1970: 40)
Loss of zufälliges Sosein (co-incidental qualities of anything) as the common denominator of some schizophrenic psychopathology.
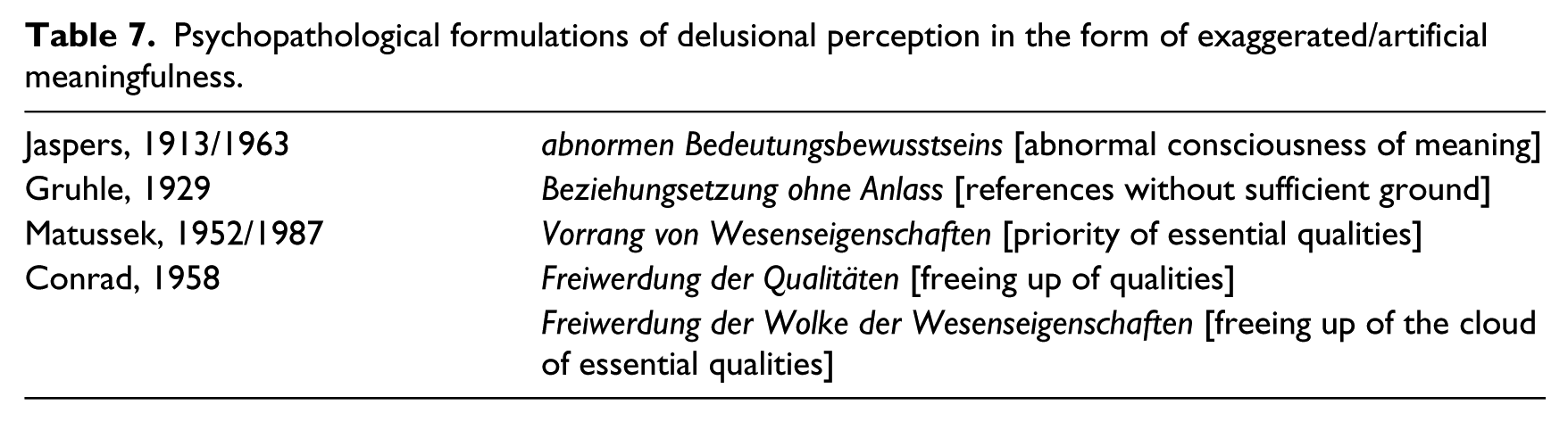
We are also finally in a position where delusional perception sheds its cloak of ‘un-understandability’. This is not to say that earlier psychopathologists were not on the right track. They were, as can be seen by their remarks, shown in Table 7. But they had no theoretical framework in which such comments made much sense. Matussek and Conrad did try to recruit Gestalt theory in its genesis but they were rather half-hearted about this, and rightly so because the essence of delusional perception cannot be derived from any psychological model of the human being, but only within a philosophical framework such as Scheler’s.
Psychopathological formulations of delusional perception in the form of exaggerated/artificial meaningfulness.
Delusional perception, within a Schelerian framework, is indeed a freeing up of the essence of something, which can be a quality, for example colour, as in this brilliantly illustrative case of Blankenburg (1965/2012: 165–76):
He was feeling unwell with various bodily symptoms which the medical attendant who first saw him thought were neurological in origin, and referred him to a neurologist in the neighbouring town. (He may well have been in a prodromal state at this point.) While walking from the station to his appointment with the neurologist he happened to look in at the window of an art shop, and was captivated by a painting in blue, which he did not perceive as perceptually awry in any way, but as a marvellous specimen of ‘art’, a topic he had barely thought about before – he was a Mercedes Benz worker. From then on he became quite preoccupied with this picture, particularly its blue colour, and this led him to profound thoughts about the nature of art.
It can be an object, such as a stone, as in MacLane’s (1917: 176) experience. But whatever it is, it is the freeing up itself that constitutes the ‘new’ experience, and this freeing up is the consequence of a new balance between the zufälliges Sosein and the Wassein of anything, with the balance tilted in favour of the latter.
In summary, we have shown that the apparent miscellany of particular qualities of objects in the world that seem to be picked off in schizophrenia, giving rise to many of their first rank symptoms, are in fact no miscellany at all but part of a fundamental perspective of human beings to grasp the unique nature and qualities of things necessary for our animal survival. Yet other schizophrenic phenomena, in particular delusional perception, are the flip side, as it were, of this deficient know-ledge, and represent a human being who is, now preoccupied with what anything is, shorn of its here and now relevance to ‘my’ life.
The origin of first rank symptoms
The final section of the article is speculative, but no more speculative than the handful of proposals by the few brave souls who have ventured into the area in the past few decades: Jaynes (1976), Hare (1983), Sass (1992), Crow (1993) and others. What they all saw in common, from quite different perspectives, was that schizophrenia can only properly be understood within a historical perspective of the development of the human being. Jaynes actually saw the condition as an atavistic return to the situation of the ancient Greeks, who, according to him, had no real consciousness of themselves, and no real ‘analogue – I’, as he called it, which could stand back and create a domain in which actions as they happened could be analysed. Instead, all actions were attributable to an outside source, one of the Gods; schizophrenic hallucinations, according to Jaynes, reprised this historical phase. Sass (1992) took a diametrically opposite view, though still placing schizophrenia in a non-contemporaneous context: for Sass, schizophrenics resembled avant-garde artists such as De Chirico and Artaud in being ahead of the crowd, not behind it. Hare’s (1983) and Crow’s (1993) theses were not anthropological in this sense, but nevertheless appreciative of the fact something had happened to the human being at some stage in history: for Hare it was in the seventeenth and eighteenth centuries, possibly a virus; for Crow it was a genetic event at the very beginning of the advent of homo sapiens out of its hominid ancestors.
My contribution to the debate is to provide a theoretical grounding for my particular anthropological suggestion. Jaynes’ notion was largely based on a supposed similarity between auditory hallucinations in schizophrenia and poetic accounts of what drove the Greek heroes. Sass’s formulation rested on a number of psychopathological similarities between avant-garde art and schizophrenia, but was, like Jaynes’, a simple phenomenological exercise. Hare’s evidence was epidemiological and Crow’s anatomical and genetic, but the clinical component was also phenomenological. My advantage, I would suggest, is that I have gone beyond mere phenomenological analyses to achieve some philosophical underpinning of what schizophrenia is, particularly in respect of first rank symptoms. Nevertheless, I hail all such attempts as the foregoing as welcome additions to the run-of-the-mill approach to schizophrenia, which is to see it as some psychogenic or sociogenic disturbance in a contemporary human being, conceived of entirely in contemporary psychological terms.
If the schizophrenic, on the other hand, is someone who has a dilapidated sense of zufälliges Sosein and is overly captured by the Wesensein or essence of everything in their environment and world, and it was the tracking down of the nature of first rank symptoms which first gave a clue to this, we might find analogies of this same state of affairs in an anthropological or neuropsychological setting, which might help to nail the very origin of schizophrenia itself. There are indeed remarkable similarities in this respect, first in the philosophical anthropology of Max Scheler and his contemporary Ernst Cassirer (1874–1945) on the mentality of early human beings vis-à-vis contemporary humans, and secondly in some astonishing experiments carried out by Soviet psychiatrists on the role of the two hemispheres in fashioning the perspective that we contemporaries assume is a single take on anything. It is not surprising that anthropological and neuropsychological data should be helpful guides here, as the other contributors to the debate about the origin of schizophrenia relied heavily on these: Jaynes (1976) invoked the supposed mental state of a normal ancient Greek along with what each of their hemispheres might be doing; Sass (1992) at least analysed the avant-garde; Crow (1993) was sensitive to the anthropological thesis as well as holding views on the change in hemispheric structure at his proposed moment of ‘speciation’; Hare (1983) had a hunch that some organic event was responsible for the advent of schizophrenia in the seventeenth or eighteenth century.
Beginning with the anthropological evidence, Scheler and Cassirer, independently, through vast reading of anthropology, concluded that the early human being was in the thrall of the happenstance of their surroundings. Cassirer (1925/1955: 43) wrote:
Mythical thinking is … distinguished from a purely theoretical world view … Anything can come from anything because anything can stand in temporal and spatial contact with anything … The mythical consciousness applies its ‘why’ precisely to the particular and unique … Inability to conceive of an event that is in any sense accidental has been called characteristic of mythical thinking. [italics added]
Scheler (1927/1973) said:
If we inquire into the origin of the idea of causality, the answer is that it is primarily given in our own spontaneous acting upon things … In my discovery that a project has been realized after a time by me and my action … The question ‘why?’ appears among primitives and children only when the customary and immediate connection of expectations about what will happen is broken … A further characteristic of the primitive causal question is indicated by the form his question takes: ‘who is responsible?’ … The causal concept became objective in the history of the spirit only very slowly. In place of ‘who is responsible?’ the question increasingly became ‘what is responsible?’ [italics added]
Whenness, whereness, uniqueness, myness and whoness are the only terms of reference known to the early human being. The ‘what’ question is a later advent (Scheler) and the failure of the early humans to conceive of the accidental (Cassirer) is because everything they experience is accidental – zufällig – measured against our contemporary viewpoint where things can be both essential and accidental. The early human does not experience the essential at all.
The schizophrenic, from everything we have considered earlier, is he or she who is in thrall to the essential, more so than the contemporary normal person. This is therefore against Jaynes’ view and supports Sass’s thesis that the schizophrenic is further along the trajectory of human development than even the contemporary human being.
What of a neuropsychological setting for this? Consider now the following experiments by Deglin (1993) and his collaborator Chernigovskaya (1993). Rarely translated, and even then usually in obscure publications, the experiments were carried out on patients with schizophrenia and depressive illness in the immediate aftermath of having had electroconvulsive therapy (ECT), applied either to the right or the left hemisphere, and who were, in essence, in a uni-hemispheric mode of cognition. (The subjects had previously been given the same task as they were now asked to perform after ECT, and so there was a normal or bi-hemispheric control state for comparison.)
Experienced thingness. Subjects were shown famous pictures by Monet, among others, depicting weather scenes, e.g. Waterloo Bridge in London under fog or a storm brewing (Chernigovskaya, 1993). They were asked to describe the picture and give the time of day and the weather portrayed. Under conditions of left hemisphere suppression (right hemisphere alone viable), subjects described the pictures with exactitude, much better than when their right hemisphere was suppressed, and better even than when in a normal bi-hemispheric state. For example, on seeing the Monet, one said, ‘Morning, fog’, and, on seeing a Siskin, said, ‘There is a storm brewing’. Moreover, they gave precise accounts of the colours and nuances of light and shade.
Under conditions of right hemisphere suppression (left hemisphere alone viable) the same subjects gave ‘drastically impoverished’ accounts, relative to when their right hemisphere was functioning alone, and even relative to their bi-hemispheric state. One subject, for example, on seeing the Monet, said, ‘I cannot make out any image whatsoever; it’s an abstract representation’. Another said of the same picture, ‘I can only say that it is something like the surface of the earth, or material of some sort, or even another planet.’ Yet another said that the surface looked convex or hollow. Several, however, tried to classify the picture as belonging to this or that school of art or historical period.
Mode of symbolic representation. Another experiment (Deglin, 1993) required subjects to comment on whether some object, e.g. ‘brother’ or ‘bread’, was appropriately named, or whether another name could be given it, e.g. respectively ‘sister’ or ‘meat’ or even whether a completely made-up word would do. Under conditions of left hemisphere suppression (right hemisphere alone), subjects replied, for example, ‘Bread is called bread because it’s white and tastes good. Bread fills you up. Why should anyone call it anything else?’ Or, ‘Brother, that’s someone who’s a blood relation and that’s why it’s a brother. You can’t call it anything else.’
Under conditions of right hemisphere suppression (left hemisphere alone) subjects replied that ‘bread’ or ‘brother’ could easily be called something else. Deglin concluded: ‘The right hemisphere does not know that a verbal sign is arbitrary and conventional. It appears, in fact, that for the right hemisphere the verbal sign is as firmly attached to the object, indeed part of the object, as is its form, colour or smell.’ What we see here is that the right hemisphere’s modus vivendi is to be concerned with the uniqueness of some object in the world. Its imagistic repertoire portrays a vivid scene with a time and a place, and its linguistic faculty further links a word with a definite thing. The left hemisphere, on the other hand, can barely provide images of anything definite, even though it can adequately construe what sort of thing it is presented with. Its semantic network plays to rules which ignore the uniqueness of what it presumes to denote.
In summary, we have presented philosophical anthropological and neuropsychological comments and experimental results to the effect that the zufälliges Sosein, which we had earlier argued was dilapidated in schizophrenia, is also a defining feature of the world and environment of early humans and largely subserved by the right hemisphere. Contemporary human beings have moved away from an over-reliance on zufälliges Sosein and can additionally grasp the essence of something as well. The schizophrenic, I propose, is he or she who is further distanced from being in the thrall to the zufälliges Sosein, and is further wrapped up, more so than his or her contemporary ‘normal’, in sensing and being constrained by the essence of anything.
Conclusions
In brief, Schneider’s introduction of the notion of first rank symptoms of schizophrenia was a stroke of genius, in my opinion. Their reputation for poor sensitivity, poor specificity and unsatisfactory predictive validity is not deserved. Adding other phenomena such as a certain sort of delusional misidentification and a particular kind of anomalous temporality might make them even more sensitive, specific and predicatively valid.
I think they have spearheaded the way to a formulation of schizophrenia itself, which, in the opinion of several of the most insightful contemporary psychopathologists, has to do with a disturbance in the ‘myness of experience’, which no less than seven of Schneider’s 11 first rank symptoms can be shown to illustrate. Further analysis of the remaining first rank symptoms which do not obviously display such lack of myness – certain sorts of auditory hallucinations, delusional perception – shows that there are other sorts of deficit, and compensatory psychopathology in response to this deficit, which can explain them. The investigation into the nature of schizophrenia as a whole, however, has been well served by Schneider’s original observations.
I go much further than Schneider in formulating a philosophical account of first rank symptoms and schizophrenia in general along the lines of certain late thoughts of the philosopher Max Scheler. I further maintain that this Schelerian enterprise allows certain unresolved issues about schizophrenia to be properly addressed, for example: is schizophrenia an atavistic mental state? (as many psychopathologists have maintained – Jaynes is the one selected in this context but Freud, Kretschmer, Storch and others could be included). Or is schizophrenia the complete opposite: an omen of the future, selectively given to those few who are deemed schizophrenic by their ‘normal’ contemporaries? Sass (2003) is the only person, to my knowledge, to have stuck his neck out on this issue, and I wholeheartedly support him in the thrust of this paper.