
Abstract
Kahlbaum’s seminal approach to symptom complexes, as opposed to disease entities, is still relevant. Many psychopathologists have approached mental symptom complexes without prejudging them as necessary physical deficits or diseases, favouring a broader dimensional and anthropological view of mental disorders. Discussions of symptom complexes gained prominence in psychiatry in the early twentieth century – through Hoche – and in the period leading up to World War II – through Carl Schneider. Their works, alongside those of Kraepelin, Bumke, Kehrer, Jaspers and others, are reviewed in relation to the theme of symptom complexes, the mind, and mental disorders. A particular feature of symptom complexes is their relationship to aspects of the normal mind and how this affects clinical manifestations. It is further suggested that symptom complexes might offer a useful bridge between the psychic and the biological in theories of the mind.
Keywords
Introduction
Kahlbaum (1863) reviewed over 30 classifications of mental disorders that had been identified by his time. One of his conclusions was the existence of four basic nuclear symptom complexes: melancholia, mania, a type of mental weakness (‘Turbatio’) and dementia (‘Aphrenia’). These nuclear symptom complexes, which are not themselves diseases, comprise elemental symptoms disposed in a continuous centripetal–centrifugal physiologic flux (Figure 1).
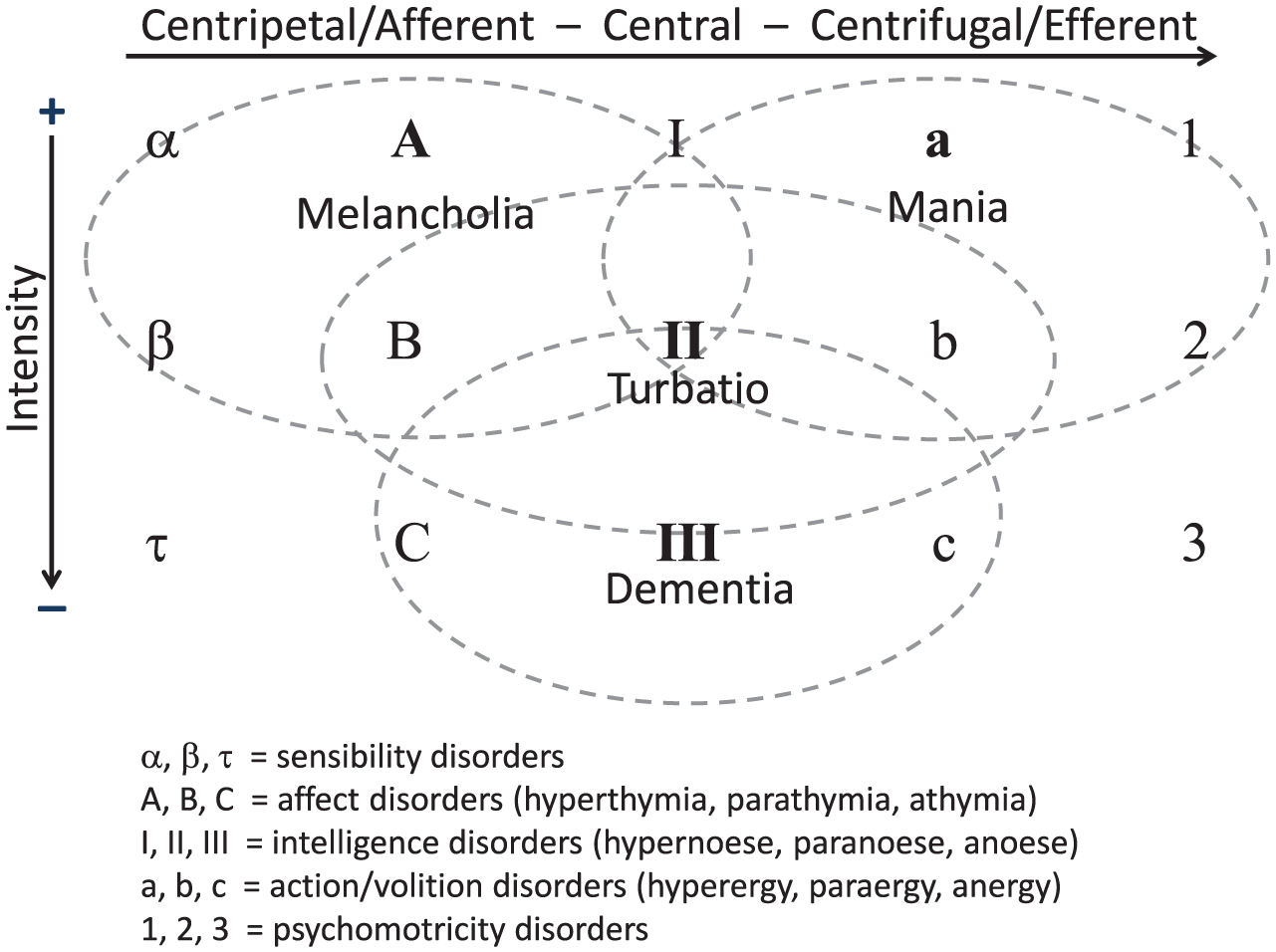
Elements (symptoms) and symptom complexes, adapted from Kahlbaum, 1863: 157.
This approach to psychopathological manifestations has often been used subsequently and indeed is also currently observed in psychiatry, for example in the symptom dimensions proposed by Häfner, Heiden and Maurer (2008: 95): depression, mania, psychosis and functional impairment, in addition to negative symptoms. These dimensional schemas recall the enduring discussion on categorical versus dimensional classification and diagnosis (Angst, 2002; Angst and Gamma, 2008; Möller, 2009). These schemas also contribute to subjecting the traditional medical model of disease to a disputable and rich debate in psychiatry and philosophy (Fulford, Thornton and Graham, 2006: 3–30, 111–38).
Kraepelin (1920: 25; also available in English: Kraepelin, 1992) considered such symptom complexes to be like pipe organ registers: their sounds vary depending on the exerted strength and expansion over them, but quite regardless of what type of action triggers their play. Symptom complexes are, then, preformed reaction patterns of the human organism to various possible influences or causes that lead them to move. Kraepelin conceded the possibility that ‘the affective and the schizophrenic manifestation forms of insanity do not represent, in themselves, the expression of certain disease processes, but merely reveal those areas of our personality in which they take place’ (Kraepelin, 1920: 27, italics added). He also mentioned Guislain as an ancient precursor of these thoughts (p. 24). Importantly, the ideas of Guislain had strongly influenced Griesinger, who disseminated the notion of a pattern of evolution for mental disorders in continuous symptom complexes (Griesinger, 1876), later called unitary psychosis or Einheitspsychose (Angst, 2002; Kumbier and Herpertz, 2010).
Many of the most important discussions regarding the significance of symptom complexes in psychiatry occurred from the early twentieth century to World War (WW) II. Some authors and aspects of these discussions are gathered in this work to explore possible relations between symptom complexes and the mind.
Distinguishing symptom complex, syndrome and disease
Syndrome, from the Greek syndromos, meaning ‘place where several roads meet’ or ‘a running together’ (Harper, 2017), is often used interchangeably with symptom complex or with disease; however, there are some important differences. Although this paper does not intend to probe too deeply into these concepts, Table 1 shows that, compared with syndromes, symptom complexes are more neutral or distant in relation to diseases.
Relations of symptom complex, syndrome and disease to aetiology and pathogenesis.
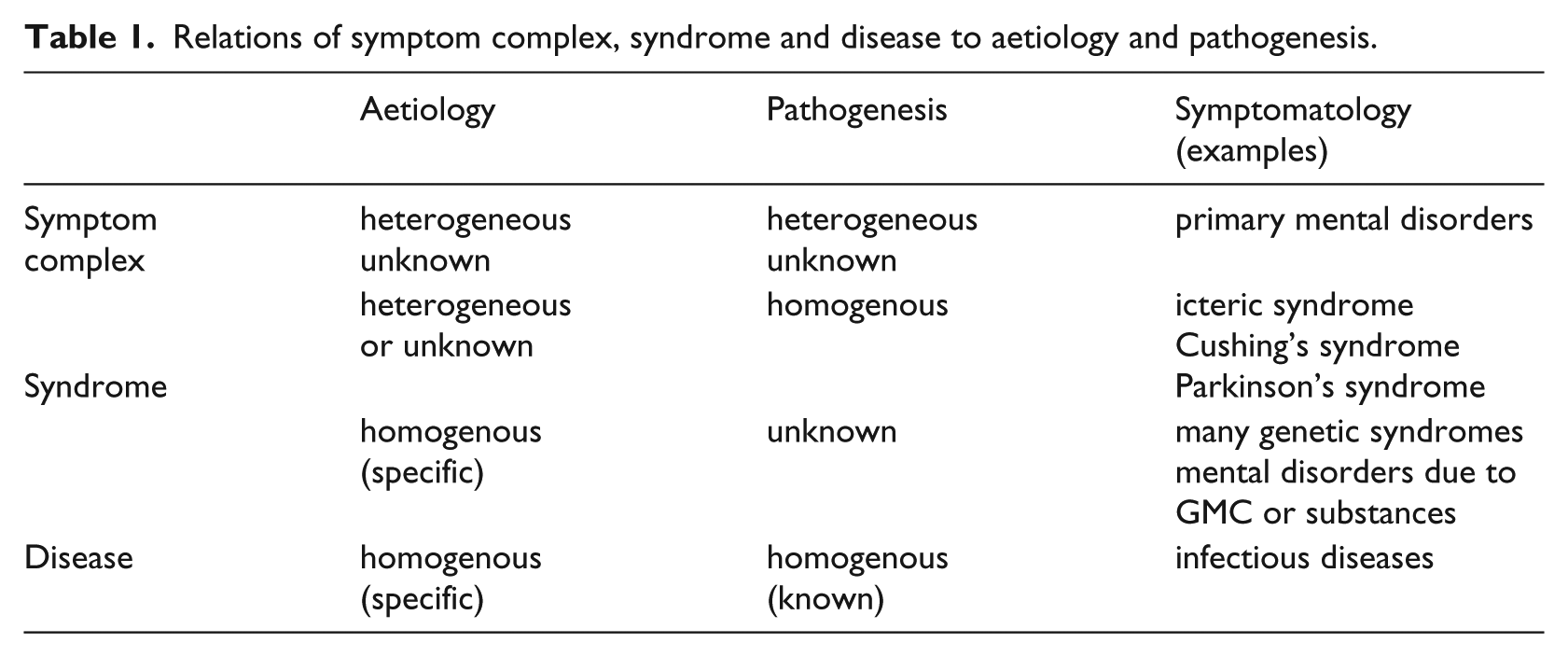
Indeed, the seminal study of symptom complexes by Kahlbaum was intended ‘at first, without regard to certain forms of disease’ (Kahlbaum, 1863: 141), and they were considered solely as a garment or vesture (Gewand or Habitus) of the inner disease. Jaspers also noted, Already, Emminghaus described as symptom complexes melancholia, mania, insanity [Whansinn], paranoia [Verrücktheit], dementia [Blödsinn], and it was said of symptom complexes as self-evident but completed forms, as the idea of the disease unit alone stood in the foreground of interest. However, in our days, it was again demanded in principle the investigation of these complexes: they should be studied in themselves, regardless of disease unit and disease processes, to investigate the regularity and needful togetherness that exist in them, and so to reach unities that would stand as in the middle between the elementary manifestations of all kinds and the disease units. (1913: 268)
As quoted above, Kraepelin, who had searched for psychiatric disease entities and established the basis of our current psychiatric classification, turned his perspective to a seemingly less positivistic and linear approach. In his later writings, he reflected on the impossibility of satisfactorily delimiting schizophrenia from manic-depressive illness, which ‘leads us to suspect that our problem statement was flawed’ (Kraepelin, 1920: 27). In all the editions of Kraepelin’s textbook, he had espoused a strict medical model of natural disease entities or natural kinds (Hoff, 2015), with a direct correlation among causes, anatomo-pathological findings, and clinical manifestations of mental diseases: ‘this requirement I regard as the cornerstone of our scientific investigation of mental disorders’ (Kraepelin, 1910: 14). Thus, from careful study of the clinical manifestations, which he believed to be more feasible, knowledge of anatomo-pathology and aetiology would emerge more easily. However, in the chapter on the causes of mental disorders in the editions of his textbook, he also mentioned the difficulties of relating clinical manifestations to causes, what he coherently called a ‘contradiction with the basic natural scientific laws’ (Kraepelin, 1909: 15). Indeed, since his first edition, Kraepelin was aware of the difficulties of relating causes to clinical manifestations in psychiatry: The great majority of the causes of insanity, however, have a very different effect, both in terms of duration and intensity of their actions as in terms of the constitution of the organism that they hit; further, they rarely act individually, mostly in combination, so that the causal relationship of the singular manifestations can almost never be seen with that clarity such as in the course of an infectious disease. (1883: 189)
His work of 1920 appears to be an attempt to resolve these puzzles, in addition to being stimulated or provoked by the works of Bonhoeffer, Birnbaum (both mentioned in Kraepelin, 1920), Hoche (see below), and others. Kraepelin proposed that symptom complexes arose from anthropological and genetic origins, with the mechanisms lying in phylogeny and personal inherited characteristics (Kraepelin, 1920: 25). Accordingly, these symptom complexes are not directly related to some specific disease causes, as he once believed, but arise from ‘preformed apparatus of the human organism once and for all fixed … general human properties … general properties of the psychic life … gear of our personality … our inner gear’ (pp. 13, 15, 27). Kraepelin proposed three anthropogenetic groups of symptom complexes, presented in involutional stages: (1) delirious (clouding of consciousness, similarity to dreams), paranoid, affective, hysteric and impulsive manifestation forms; (2) schizophrenic and perhaps auditory hallucinatory forms; and (3) encephalopathic, idiotic and spasmodic forms.
Hoche, Bumke and Kehrer
Hoche’s ‘Die Bedeutung der Symptomenkomplexe in der Psychiatrie’ (The meaning of symptom complexes in psychiatry) (1912; also available in English: Hoche, 1991) broke away from the perspective or ideal of establishing disease entities in psychiatry as natural kinds. In his words: Underlying all these strenuous efforts [to find disease entities] is the indestructible belief that it should be possible also in psychiatry to find particularly defined, pure, single forms of disease, a belief that again and again is nourished from the analogy to somatic medicine, without thinking that the nature of the relationships between symptom and anatomical basis, as they are here and there, cannot be compared at all with each other. (1912: 542)
The psychic, according to Hoche, represents an entirely new category, obeying its own laws, not commensurate with material processes, comparable to music as it relates to a musical instrument. All of this resulted in his famous statement that the search for disease entities in psychiatry is a hopeless and exhausting hunt for ghosts (p. 551).
This new approach was obviously a more flexible approach than the previous rigid Kraepelinian view of mental disease. Hoche introduces an anthropological-personal perspective into psychopathology: symptom complexes are preformed or lie ready in the normal psyche (as well as in those predisposed to mental disorders), constituting in part ‘what we call a man’s character’ (p. 549), and in part – in case of special pathogenic influences – they define the characteristic reaction-form of that particular personality.
Such symptom complexes are observed in mental disorders that appear to be only a strengthening of certain morbid dispositions such as melancholia, mania or chronic paranoia, but are also brought forth by organic processes (p. 549).
By 1909, Bumke had already clearly pronounced the inner relation of symptom complexes within a normal psyche: There is, in fact, a common characteristic of these endogenous, functional diseases, which is that they repeatedly provoke psychological interpretations. They do it because their symptoms mean nothing new in principle, but are connected by a smooth transition with the manifestations of healthy mental life, so closely related that in individual cases, the decision ‘healthy or sick’ can be just impossible. The mood changes of manic-depressive, inhibition and excitation, the suggestibility and hypochondriacal inclination of hysterics, the struggle desire of grumblers, and so many other things that belong here are all things with healthy analogues in their own consciousness, and one can only because of this – depending on personal disposition of more of this, more of that tendency – understand and feel them. (1909: 397)
In 1924, he went on to say: These dispositions are in fact connected with normality by way of indefinite transitional stages: we are apparently dealing with truly quantitative deviations from normal mental processes, such as are continually being produced anew by the mechanism of heredity, and which always bear the stamp of this origin from the earth and soil of the normal psyche. . . . We should certainly assume that there are deviations in the function of the brain tissue, but these deviations will rise from the normal somatic disposition in just the same way as their mental counterparts are related to normal behaviour. Mental disorders which are ‘functional’ in this sense can and must shade off into normal human psychology. (Bumke, 1993/1924: 134)
However, with respect specifically to schizophrenia, Bumke did not fully agree with the views of Bleuler and Kretschmer regarding a functional continuum with normality. Bumke was critical of them for perceiving ‘nothing in dementia praecox but a morbid condensation of normal mental reactions’ (Bumke, 1993: 134). In any case, psychiatry began to pay more interest to normal psychic aspects, as noted by Mayer-Gross (1929: 40): ‘We no longer hold everything that the patient produces in an uncommon way for the immediate expression of the disease itself, we want to recognize the detours and substitute formations thoroughly, in order to find out the functions and their disturbances’.
Kehrer (1925) addressed the theory of symptom complexes. He critically noted that what Hoche said about disease entities applied to classifications in all branches of medicine as well as in biology; that is, we would always be chasing phantoms because of the infinite variability of forms in living organisms, as seen through time in Darwin’s theory of evolution. He suggested that the term ‘disease types’ might be more appropriate than ‘disease entities or units’; however, ‘type’ already signals a possibility or an approximation, not necessarily something real. Kehrer argued that what we call ‘natural’ classification systems, for example for botany and zoology, are in fact artificial, at least in part. What then would render symptom complexes so different from diseases? Why favour one term ahead of the other? Of relevance would be a classification according to the features and knowledge of a scientific field, in favour of reaching its specific practical purposes. Furthermore, he questioned what is meant by talking about ‘preformed’ entities in biology. What is not somehow already in the organization of the organism? ‘Preformed’ is perhaps simply a synonym for predisposition (Kehrer, 1925: 443–4).
In addition to his noteworthy critical evaluation of Hoche’s work, Kehrer also makes several positive remarks and contributions. He congratulated Hoche for being sufficiently brave to fight on two leading battlefronts: the model of disease entities represented by Kraepelin and the psychodynamics of Freud. Kehrer welcomed ‘the displacement of an elementary psychology strange to life through a matter of lived personality within psychiatry’ (Kehrer, 1925: 433), which is also a warning against rigid schematizing. ‘Preformed’ or ‘to lie ready’ should, then, be understood as disposition, which manifests itself either in the permanent mental constitution or in the readiness for mental disorders. Kehrer, drawing on work by Bonhoeffer, suggested that, when confronted with a suitable (somatic or psychogenic) aetiology, the dispositions act as a ‘pathogenetic intermediate constituent’ between that aetiology and the manifestation. However, Kehrer differed from Bonhoeffer in believing that a proper investigation could distinguish between symptom complexes, for example mania and melancholia, caused by an external factor and those deemed endogenous.
Kehrer agreed with Jaspers that the symptom complexes should be further investigated, and defended the idea of an ordering among them: they are not simply beside others by chance, but ‘one after another or from another, and above all in static cross section with a lawfully up-and-down, through and together, eventually even against each other’ (Kehrer, 1925: 453). If we only think of complexes lying side-by-side, then it is impossible to understand Hoche’s work (p. 454). As an example of such ordering, he mentioned the ‘anthropogenetic ordering in stages’ proposed by Kraepelin, as quoted above and further investigated by other authors. He believed that without a dynamic view of such an ordering, even if tacit, it would no longer be possible to adequately approach psychopathology. According to Kehrer, for example, it is reasonable to think that obsessive-compulsive symptoms emerge from affective or schizophrenic disorders, but not vice versa. Further, he sought an answer to the question of why, in each case of different exogenous agents, this or that symptom complex can be set in motion and not another. Again, he mentioned Bonhoeffer and his predilection type (Prädilektionstypus), that is, some variability in the response is expected: there is not a pathognomonic response to all the exogenous agents, but a certain uniformity, due to a transformation and synthesis of the different agents through the pathogenetic mediation (Kehrer, 1925: 446, 447). Kraepelin’s original hope of a linear correlation between causes and manifestations is here contrasted by Kehrer (p. 447).
Kehrer indicated that it is not possible to reach nomothetic proof and a satisfactory categorical classification of such dynamic, interchangeable or continuous symptom complexes characteristic of a living human being in a state of constant adaptation to the environment. However, Kehrer concluded with the hope that a better knowledge of the symptom complexes or syndromes, together with their physiopathology, would evolve into a nosology of all cases of diseases as in other branches of medicine. It is not clear here whether he was thinking again about diseases in terms of a continuous variability of forms; he most likely was (p. 456).
Carl Schneider
According to Jaspers, Carl Schneider turned the symptom complexes into the epicentre of psychiatry, ‘just as atoms are central unities in physics and chemistry’ (Jaspers, 1946: 491). Jaspers (pp. 490–5) dedicated five to six dense pages to Schneider’s work on symptom complexes in schizophrenia.
Carl Schneider diverged clearly from Kraepelin’s conception of disease entities in psychiatry with its linear correlations between aetiology, anatomo-pathological findings and clinical manifestations: Indeed, Kraepelin believes that he has hereby established a basic requirement of psychiatry as a science, without even suspecting that he was, however, engaged in unrestrained observation with the fetters of a basic philosophical conception, which psychiatry has not yet abandoned. (1942: 5)
Drawing from his empirical work on schizophrenia, he described three symptom complexes or associations (Symptomverbände): ‘thought retreat’ (Gedankenentzug), ‘jumpiness’ (Sprunghaftigkeit) and ‘drivel’ (Faseln). These associations were also investigated throughout the life span. He suggested that more such associations should be identified for all disorders in psychiatry.
The point of interest in the present work is Schneider’s emphasis on a dynamic correspondence between symptom associations and normal function associations (Funktionsverbände): ‘the couplings of symptoms which are present in the symptom associations are not first produced by the schizophrenic process but are already formed in the norm … which for differentiation are better named function associations’ (1942: 142). Indeed, in this way, the symptom complexes can assist our knowledge and understanding of normal function associations: Given the great fluidity of the internal mental and external physical changes in the normal, it is difficult to recognize without further ado the connections. In the symptom associations, on the other hand, a conclusion concerning the norm is, above all, possible because the pathological disorder highlights, in isolation, the connections in question. … the new doctrine leads to an in-depth description of the pathological processes of life as well as the normal functions of the organism. (pp. 237, 243)
It is important not to regard the identified associations as static constructions in the sense of a rigid categorization, but as expressions of an ever-fluid process of life with dynamic effects and changeable responsiveness (p. 194).
Schneider employed a wide scientific ‘biological’ concept: a general concept of life comprising the ‘psychobiological’ and ‘somatobiological’ (mind and body), ‘whose laws go beyond both alone’ (p. 17). Thus, the mind is not simply an epiphenomenon of the body, as noted by Jaspers when commenting on Schneider: ‘Functional associations are the elements of all body-soul life’ (Jaspers, 1946: 491). This can be perceived in the following excerpt: Each of these ‘functional associations’ is the result of a biological differentiation process in the whole organism, and like the ‘symptom associations’, spreads across psychological and somatic manifestations in an orderly way, since it, in each case, picks out certain psychic and somatic functions from the totality of the remaining manifestations, and unites them in itself. (Schneider, 1942: 237)
Schneider speaks of ‘wholeness’ or ‘totality’, concepts with which many psychopathologists were concerned when approaching personality and mind at that time. Minkowski, in his 1933 book (reprinted in 1968), referred to the ‘whole living personality’ as he delineated his notion of ‘generating disorder’ (Minkowski, 1968: 208, original italics). According to him, psychiatry as a branch of medicine is supposed to address symptoms and syndromes but the psychic reality poses special problems. This is because we tend to view psychic manifestations in the context of the whole person. Thus, mental syndromes are not conceived to be simple associations of symptoms, but the ‘expression of a profound and characteristic modification of the whole human personality’ (p. 211). He also suggested that the psychic manifestations should, at first, be considered ‘different’, arising from a different person, rather than ‘sick’: in contrast to sickness, diversity is not in principle a negative characteristic (p. 233). Henri Ey (1952) considered this aspect of wholeness in psychiatry – ‘in the sense of a pathology of consciousness, or a pathology of the personality, that means then the overall organization of “being-in-the-world”’ (p. 198) – as its fundamental difference from neurology. Psychiatry implicates a global dissolution of the consciousness, whereas neurology involves a local dissolution in the periphery of the ego, that is, it involves a local and basal dismantling process, a disintegration of isolated functions that constitute the apparatus of psychic activities. Schneider advised that it was important to keep the totality of the picture in mind when investigating the more elementary facts of the clinical picture, also arguing that being constantly conscious of the influence of the whole in the analysis of the elementary facts does not mean falling into pure metaphysical abstractions (Schneider, 1942: 227–8).
Schneider concluded that psychiatry was a specially suitable field in which to develop his dynamic and broad biological views: It is no accident when such enterprise starts just from psychiatry. For in it, the question of the body-, soul-, and wholeness-structure of the human individual and his whole life is deepened and turned into a methodically solvable problem, and it is clear that in order to face such a task, the endogenous psychoses offer right the most favourable start; indeed their symptomatology reaches all spheres of living events, and their course lamentably lasts usually a lifetime. (p. 247)
One of Jaspers’ criticisms concerning Carl Schneider’s research on schizophrenia was that he tended to highlight insight into the structure of the mind rather than into schizophrenia itself. ‘The investigation thus leads to a new hypothesis of the structuring of mental life …’ (Schneider, 1942: 156). However, Jaspers’ interest in Schneider’s work could be linked to his statement elsewhere that the study of psychology is to psychopathology what physiology is to pathology, without clear limits from one side to another (from normality to pathology), and that psychology remains unable to offer the knowledge of ‘normal’ that psychopathology could take advantage of. In this sense, he envisaged a ‘psychology of broad horizon’ (Jaspers, 1946: 2, 3).
Conceptual stasis
After the work of Carl Schneider and Jaspers’ analysis of it, the concept of symptom complexes did not appear to advance beyond WWII. Why did the theory not continue to evolve? The theory itself has no relation to the National Socialist ideology: quite the opposite in the author’s view, because of its openness to normality and consequent tendency to de-stigmatization, compared, for example, with the concept of degeneration. However, for other reasons, some of the authors, as well as much of mainstream psychiatry of that time, were linked to that ideology, which brought tremendous harm for those considered insane. Not surprisingly, after WWII, psychiatry moved away from its genetic and physical or biological murky side in favour of psychodynamic and phenomenological-existential approaches (Hoff, 2009), if not to overt anti-psychiatry. Then, psychotropic drugs appeared on the scene, leading rapidly to an epoch of renewed hope and a search for disease entities, that is, to a neo-Kraepelinism, but in the sense meant by Kraepelin before 1920. Recently, however, the more dimensional or spectrum-orientated Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5) again attenuated the strict medical concept of disease entity: Because the previous DSM approach considered each diagnosis as categorically separate from health and other diagnoses, it did not capture the widespread sharing of symptoms and risk factors across many disorders that is apparent in studies of comorbidity. (American Psychiatric Association (APA), 2013: 12)
An additional historical difficulty is that since WWII, the prevailing English-speaking psychiatry had little access to authors and key papers about symptom complexes. Even Jaspers’ work was not translated into English until 1963.
Summary of the historical and conceptual investigation
Some points from the study above merit emphasis:
Disease entities in psychiatry do not exist in the strict sense of disease, that is, with a direct relation among causes, anatomo-pathological findings and clinical manifestations.
Clinical psychic manifestations are relatively uniform reactions or expressions of the human organism through symptom complexes.
In addition to integrating symptoms, symptom complexes are integrated into themselves, indicating a natural order among them, recalling the idea of unitary psychosis.
Despite their relative uniformity, symptom complexes must be seen dynamically in space and time, and in mind or in the living person as a whole.
Symptom complexes, in addition to their endogenous-genetic or physical roots, are intimately intertwined with the normal mind or mental functions and can provide clues to the investigation of the mind.
Altogether, the theory of symptom complexes appears to foreshadow a ‘biological’ (in the sense of C. Schneider) anthropological matrix that seems to be an important piece of the puzzle concerning a model of the mind. The mind–body problem reveals itself in many points throughout the present study.
Psychiatry and the mind–body problem
Notwithstanding the known difficulties or challenges surrounding this ‘big question’, it is undeniable that the mind–body problem is crucial in psychiatry. Our view of psychiatry, with all of its consequences, is closely connected to the manner in which we conceptualize mind and body (Fulford et al., 2006: 613–66). Therefore, a few words regarding the mind–body problem merit mention here, adding important elements to the discussion in this study.
As already stated by Griesinger, there is nothing truly analogous to the psychical agent in the rest of the world, and he asked the following: If we knew all that is also going on in the brain in its activity, if we could see through all chemical, electrical, etc., processes down to their last detail – what would be the use of it? All oscillations and vibrations, everything electrical and mechanical are but still not a state of mind, no ideation. How can that become this – the enigma will probably remain unsolved until the end of time, and I believe that if an angel came from heaven today and told us everything, our understanding would not be able to realize it! (1876: 6, 7)
Jaspers compared the mind–body problem to the investigation of an unknown continent from its opposite edges, wherein the traveller-investigators from both sides never meet: ‘We know of the causal chains between psychic and physical only the end links’ (1946: 4).
Reputable contributions from philosophy and science have been further developed since then, but none is without its pitfalls. Fulford et al. (2006: 613–66), in their chapter on the mind–body problem and mental health, advise that modesty is called for, and remembered: A brain state can be the state it is independently of what happens outside the skull, but mental states are relational and world involving and thus cannot be found simply within the skull. And while brain states stand in nomic relations of cause and effect, mental states stand in rational relations. (p. 664)
Berrios agrees with Jaspers on the necessary plurality of methods in psychiatry, which he considers a hybrid discipline rooted in both natural and human/social sciences, proposing a regional epistemology proper to psychiatry and able to dynamically integrate different methods (Marková and Berrios, 2012).
Discussion
The present work rescues a historical chapter of psychiatry that, similar to many others in its rich history of ideas, maintains a valuable background and inspires current interest. Many psychiatrists will agree that the theory of symptom complexes presented here speaks to crucial points of our specialty, and many scientists and philosophers addressing the mind may be interested in the approaches dedicated by those psychopathologists to mental disorders.
A crucial question is whether the theory of symptom complexes takes us further into the continent than the explorers in Jaspers’ analogy. Figure 2 provides a quite simple – but complex to explain – view, or conceptual map, of general psychopathological and mental dispositions, which appears to conform to the notion of symptom complexes.
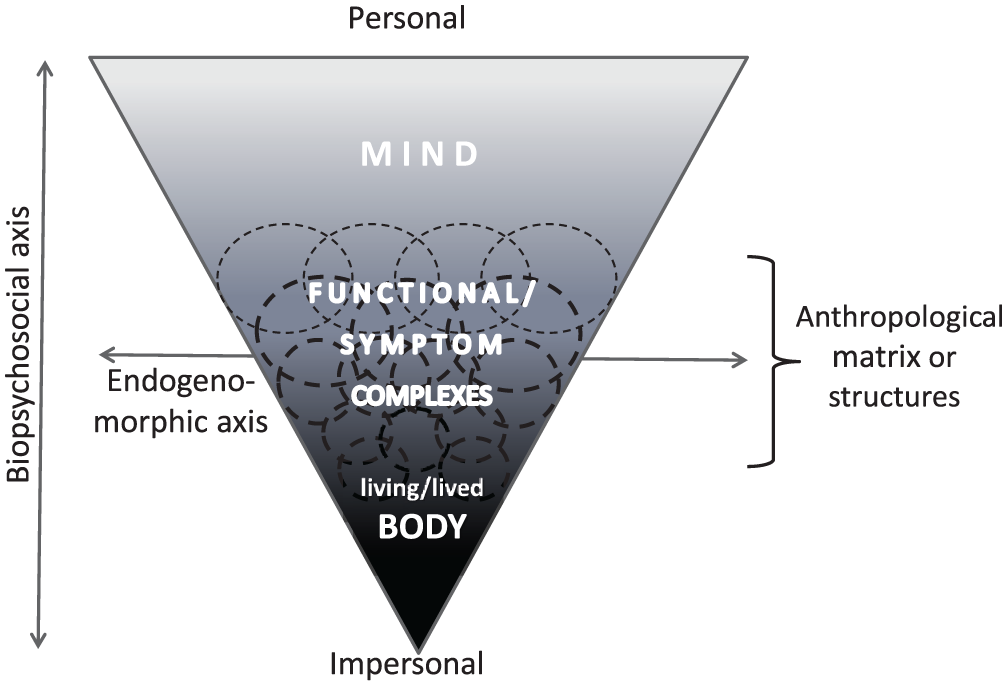
A conceptual map including symptom complexes intertwined with normal functions between mind and body.
The foreshadowed anthropological matrix remains mostly a matter of speculation. To what extent will empirical hard data or other kinds of knowledge contribute to it? In this regard, the author sympathizes with the idea of non-linear dynamic systems, at least used metaphorically, such as Ciompi’s (2015) affect-logic conception or Maiese (2016), who considered the dynamics of living organisms, body and mind. Symptom complexes would be attractors in such systems.
Not reaching quite that far, symptom complexes may be exemplified as the more homogeneous and identifiable colours in a light spectrum, particularly if we imagine a sort of multidimensional (not only from one side to another) spectrum. These relative homogeneities may be considered polarities, prototypes, ideal types, habitual forms, phenomenological structures, basic psychopathological forms, attractors, etc., provided they are conceived to be related to one another or pertaining to a whole, to a system, to a spectrum, to a continuum – the principle of unitary psychosis. As summarized above, as symptoms appear to be bound by certain rules in symptom complexes, so are symptoms complexes among themselves.
Each of these symptom complexes contains its peculiarity, each different from another from a static point of view (different colours). From a dynamic perspective, however, moving or evolving in time and space, their relations appear one after another or from another, up and down, through and together, or against one another, as Kehrer would say; between them are mixed states. Each person would contain in him/herself, at least potentially, the entire spectrum or system, but with his/her own variability and uniqueness. Hence, a continuum in time is observed through an indefinite number of individuals or persons (think again of Darwin’s theory of evolution through time – the continuous variability of forms). Thus, it is not required or expected that all considered symptom complexes must manifest in a single person, even less so at the same time, to say that there is a continuum between them. This paper addresses a dynamic approach, which is more adequate for living beings in many aspects – and particularly for the mind – than a static mosaic-form approach.
Carl Schneider regarded such individual variation as fundamental in medicine, considering the ‘biology’ of the organism. The varieties and multiple possible combinations of the functional associations in the course of inheritance would be a stratagem of nature to connect the stability of material, morphological and functional general laws in an overwhelming malleability of the individual life responses (Schneider, 1942: 247).
We might illustrate these considerations by analysing the contrast or basic polarity between schizophrenic and depressive symptom complexes. This polarity is a result not purely of Kraepelin’s nosological dichotomy, but also of persons’ contrasting worldviews, for example between the notions of schizoidism and syntony – which in the ambit of normality, are clearly complementary – and between some phenomenological-anthropological approaches to these worldviews. For example, Cutting perceives a contrast between schizophrenia and depression with regard to this-ness, who-ness, whose-ness, my-ness, where-ness and when-ness (Cutting, 2013: 27–9). Using whose-ness as an example, on one side there is the delusion that one is under the control of someone else; on the other side there is an over-involvement in someone else’s social situation or commitment to social norms, to the extent of delusions of guilt (exaggerated my-ness).
What if the schizophrenic or depressive, for example, were restricted to only one component of what was a dyad for the ‘sane’? Further, what if the difference between the world-views of schizophrenic and depressive consisted precisely of which member of the pair was viable or deficient in each case?’ (p. 15)
These dimensions are helpful in terms of getting away from a model that forces a dichotomy between deficit/insanity on the one hand and normality on the other. In this sense, Messas, Tamelini and Cutting (2017) differentiate a fixed existentialism, wherein a basic deficit is presumed, from a dialectical existentialism that sees an imbalance among anthropological characteristics.
As well as schizophrenia and depression in the spectrum of our possible anthropological matrix, the more cohesive delusional paranoia symptom complex or pole would sit above schizophrenia, and above depression would remain the pole of mania. Further above would be hysteria or dissociation (linked particularly to schizophrenia and mania?) and obsession (linked to depression and paranoia?). Analogous to schizoidism and syntony, all of the polarities complement themselves in the range of normality. Around them, some persons would be fixed or rigid in a certain position, indicating personality disorders. The wide range of normal mind would occupy an area of broadly complementary, malleable and adaptable dynamic equilibrium.
It is worthy of note that Hoche did not include dementia or other traditional organic symptomatology in his theory of symptom complexes as other authors have, for example Kraepelin (also to be excluded would be the more severe cases of schizophrenia if proven organic in a traditional sense). This reflected his concern to perceive such symptom complexes as closely bound to the normal psyche or to ‘a man’s character’ or person. Accordingly, many phenomenological psychopathologists, as observed by Minkowski, preferred to speak first of differences instead of seeing diseases overall. For example, Kraus distinguishes ‘phenomena’ from ‘symptoms’: if the two terms are used synonymously, the real sense of phenomenology is lost. The phenomenon presents itself in our lived experience without theoretical preconception, whereas a symptom is already bound to the medical concept of disease (Kraus, 2013: 71, 72). Thus, even without ever intending to neglect the hard reality of mental diseases and psychiatry as a medical specialty, another term for ‘symptom’ may be preferable when discussing some aspects of the theory of ‘symptom’ complexes, as did Kraepelin regarding his ‘manifestation forms’ and Carl Schneider with his ‘functional associations’. Kahlbaum had already referred to ‘habitual forms’, Jaspers meant ‘ideal types’, while others referred to phenomenological structures and so forth, according to each approach.
Conclusions
Because the history of psychiatry is primarily one of ideas rather than discoveries, much of that history maintains a kernel of truth and a current heuristic value. The theory of symptom complexes – which evolved between the work of Hoche and that of Carl Schneider in particular – can be considered a remarkable historical chapter. Without the interruption of World War II, this theory would most likely have generated further significant contributions. Those psychopathologists uncovered a special pathogenesis in psychiatry, which differs from the usual medical approach that is primarily directed towards physical deficits. In this pathogenesis or psychophysiology, symptom complexes play a role in the normal mind rather than being detachable or unnecessary contingencies. Is psychiatry here moving closer to its own regional epistemology?
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.