
Abstract
This article revisits a little-known lecture by René-Théophile-Hyacinthe Laennec (1781–1826), best known as the inventor of the stethoscope, focusing instead on his reflections on mental illness—what he termed vesanias. Delivered at the Collège de France in 1823, the lecture predates modern psychiatry and offers a rare, nuanced view of mental disorders at the crossroads of clinical medicine, philosophy, and Enlightenment moral thought. Laennec distinguishes between five types of mental illness—hallucinations, monomania, mania, dementia, and idiocy—while rejecting the reductionist views of his contemporaries who sought anatomical lesions as the sole cause. His classification emphasizes gradation, subjective experience, and the blending of pathology with normal human faculties such as imagination, emotion, and belief. He critiques the dominant anatomical paradigm, notably the views of Broussais, and advocates for a moral and observational approach to mental care. His views prefigure modern biopsychosocial models and anticipate concepts such as shared psychosis and dimensional spectra in psychiatry. By refusing to isolate madness from social, cultural, or historical contexts, Laennec offers a deeply human and still-relevant vision of mental illness—one that challenges us to rethink psychiatry beyond biological determinism and diagnostic rigidity.
Introduction
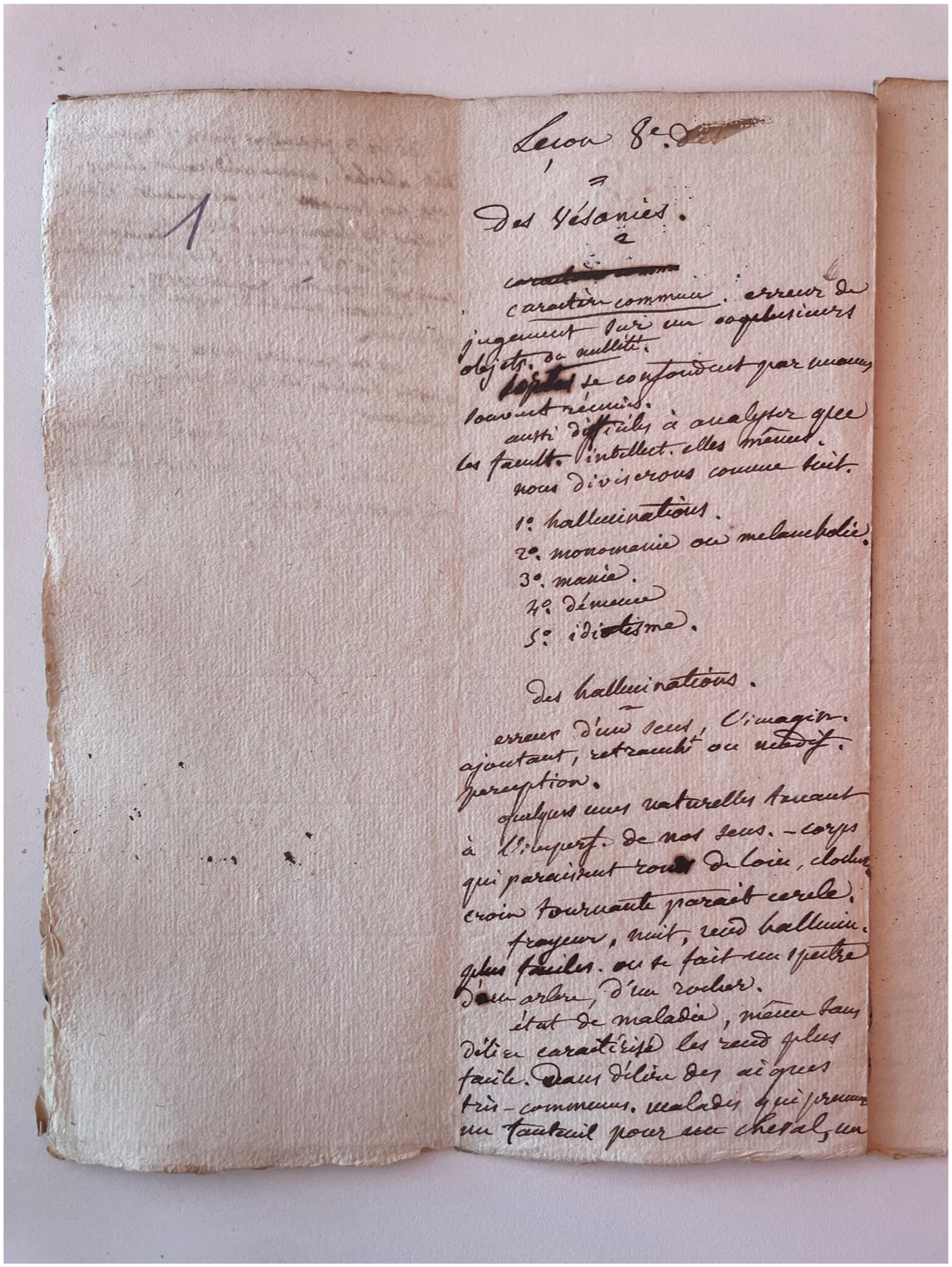
In medical imagination, René-Théophile-Hyacinthe Laennec (1781–1826) is primarily remembered as the inventor of the stethoscope and as a founding figure of modern clinical semiology (Drouin et al., 2023; Laennec, 1819). Yet a lesser-known dimension of his work deserves renewed attention: his reflections on mental illness, which he termed vesanias, developed in his lectures at the Collège de France between 1822 and 1824. The eighth lecture of the second year, delivered in late 1823 and revised in 1825 (Classeur 2aB, fols 171–176, Bibliothèque santé de Nantes), is devoted entirely to mental disorders and offers a rare window onto a moment of conceptual instability in early 19th-century mental medicine. This text has been known only to a limited circle of specialists since the pioneering works of Ackerknecht (1962) and Zins-Ritter (1993). More broadly, the period has been extensively studied by historians of psychiatry who have shown how French alienism emerged at the crossroads of moral philosophy, clinical observation, institutional reform, and political concerns (Goldstein, 1997; Pigeaud, 2001; Weiner, 1999). More recent scholarship has further emphasized the social, cultural, and political dimensions of madness in the 19th century (Hewitt, 2020; Murat, 2011), as well as the historical construction of diagnostic and affective categories such as nostalgia (Dodman, 2018). At the same time, Delille (2017) has cautioned against the uncritical use of the notion of ‘precursor’ in the history of psychiatry, reminding us that retrospective filiations often obscure the specific epistemic configurations of past debates.
Within this historiographical landscape, Laennec occupies an ambiguous and marginal position. He was neither an alienist in the strict sense, like Philippe Pinel (1745–1826) or Jean-Étienne Esquirol (1772–1840), nor a purely somatic clinician indifferent to questions of the mind. Rather, he stood at the intersection of clinical medicine, pathological anatomy, moral philosophy, and a broad humanistic culture. The present article does not aim to present Laennec as a heroic founder or a straightforward ‘anticipator’ of modern psychiatry. Instead, it seeks to situate his lecture on vesanias within early 19th-century debates and to show how his clinical, anthropological, and epistemological stance both overlaps with and diverges from that of his contemporaries. The central claim defended here is that Laennec’s most distinctive contribution does not lie in the invention of new diagnostic categories, but in his insistence on gradation and continuity between normal and pathological states, combined with a form of epistemic humility regarding the causes of mental disorders. By systematically blurring the boundaries between error, passion, imagination, and delusion, he articulated a view of madness that resists both rigid nosological compartmentalization and crude anatomical reductionism. In this respect, his lecture can be read as a clinical and philosophical experiment situated at a crossroads rather than as the foundation of a new discipline. This article has a threefold objective: first, to contextualize Laennec’s lecture within the debates of early 19th-century mental medicine; second, to offer a critical reading of his classification of vesanias in comparison with that of Pinel and Esquirol; and third, to confront his views with contemporary psychiatric knowledge, without projecting anachronistic categories onto his work.
Historical and medical context
At the turn of the 19th century, mental medicine in France underwent a profound transformation. The Enlightenment legacy—its interest in the passions, its moral psychology, and its faith in observation—combined with the emergence of hospital-based clinical medicine and new forms of medical authority. Philippe Pinel is conventionally credited with having founded French psychiatry by promoting ‘moral treatment’ and by proposing a classification of mental disorders—mania, melancholia, dementia, and idiocy—within the broader category of vesanias (Pinel, 1801). His work, as historians have shown, cannot be reduced to a simple humanitarian gesture: it also participated in a broader reorganization of medical knowledge, institutions, and social control (Goldstein, 1997; Weiner, 1999). Jean-Étienne Esquirol, Pinel’s student, refined and expanded this framework by introducing the concept of monomania, a partial delusion that became a central category of French alienism and played a major role in medico-legal debates (Esquirol, 1838). Together, Pinel and Esquirol helped stabilize a new medical specialty devoted to mental disorders, grounded in clinical observation, classification, and institutional practice. At the same time, this period was marked by intense efforts to identify anatomical or lesion-based correlates of madness. Many alienists and clinicians hoped that pathological anatomy would provide the key to mental disease, even though results remained fragmentary and often disappointing (Goldstein, 1997; Luauté, 2020; Weiner, 1999). The award of the Esquirol Prize in 1825 to Camille Bouchet (1801–1854) and Jean-Baptiste Cazauvieilh (1801–1849) for their studies on the links between epilepsy and mental alienation epitomized this orientation (Bouchet and Cazauvieilh, 1825–1826). Delasiauve would later criticize these works for their excessive reliance on pathological anatomy and their narrow explanatory scope.
Laennec, appointed to the chair of medicine at the Collège de France in 1822, was not an alienist by training. He was, however, a central figure of Parisian clinical medicine and a sharp critic of speculative or monistic systems. His opposition to François Broussais’s inflammatory doctrine, which sought to reduce all disease to irritation and inflammation, is well documented (Braunstein, 1986; Duffin, 1998). In the domain of mental medicine, this scepticism translated into a refusal to accept that vesanias could be explained by constant or specific organic lesions. Like Pinel, Laennec classified mental disorders among the ‘neuroses’, understood as functional disturbances that generally leave no anatomical trace after death. In this respect, he did not break with the dominant framework of his time. As Finger (1994) has emphasized, Pinel himself already resisted crude reductionism and insisted on the moral and psychological dimensions of madness. Laennec therefore did not introduce a radical epistemological rupture. His originality must be sought elsewhere: in the way he rearticulated these themes within a clinician’s reasoning shaped by pathological anatomy on the one hand, and by a broad historical and philosophical culture on the other (Aretaeus of Cappadocia; Hippocrates; Plutarch; Pascal; Rousseau) (Arétée de Cappadoce, 2000). This intermediate position explains both the proximity and the tension between Laennec’s views and those of contemporary alienists. He shared with them a commitment to observation and classification, but he remained wary of the institutional and theoretical closure that was gradually taking shape within early psychiatry.
Laennec and his classification of vesanias
In the eighth lecture, Laennec distinguishes five major forms of vesanias: hallucinations, monomania (or melancholia), mania, dementia, and idiocy. At first glance, this taxonomy closely resembles that of Pinel and Esquirol. However, a closer reading reveals significant differences in both scope and intention. Laennec defines vesania in very broad terms as an ‘error of judgment’, a formulation that deliberately blurs the boundary between delusion, illusion, and socially deviant or eccentric behaviour. This definition already signals a shift in emphasis. Whereas Pinel’s nosology, though flexible in practice, tended to reserve vesania for more clearly delusional or disabling states, Laennec repeatedly insists that pathological and non-pathological states are connected by imperceptible transitions. In his own words, ‘vesanias blend through nuances’ (Laennec, Classeur 2aB, fols 172r–173v, Bibliothèque santé de Nantes). Pinel’s classification aimed at distinguishing relatively discrete forms of alienation—mania, melancholia, dementia, and idiocy—in order to guide clinical practice and institutional management (Pinel, 1801). Esquirol’s introduction of monomania further refined this compartmentalization by isolating partial delusions as a specific entity (Esquirol, 1838). Laennec, by contrast, uses similar categories but constantly undermines their rigidity by multiplying borderline cases, transitional states and examples drawn from ordinary life. Hallucinations, for instance, are not presented as the exclusive mark of insanity. Laennec emphasizes that perceptual errors can occur in healthy individuals, in dreams or under the influence of strong emotions, and that all senses may be affected. Monomania is treated as a partial delusion centred on a dominant idea—guilt, persecution, imaginary illness, erotomania—but illustrated through a wide range of historical, literary and clinical examples, from Pascal to Don Quixote. Mania is described not only as furious agitation but also as a state that may coexist with relatively preserved reasoning. Dementia and idiocy represent more global impairments, yet even here Laennec insists on variability of causes and presentations.
What is at stake, therefore, is not merely a list of categories, but a conception of mental disorder as a continuum rather than as a set of sharply delimited entities. This point is crucial for understanding what distinguishes Laennec from Pinel. Although Pinel himself acknowledged the complexity and variability of mental illness, his classificatory project tended toward stabilization and differentiation. Laennec, by contrast, places gradation at the very centre of his conceptual framework. In this sense, and in this sense only, his approach can legitimately be described as ‘dimensional’, even if the term is anachronistic (van Os et al., 2009). This insistence on continuity between ordinary passions, imagination, and pathological states constitutes one of the most original features of Laennec’s lecture. It also explains his persistent reluctance to assign mental disorders to fixed anatomical causes. Rather than seeking a definitive localization or lesion, he treats vesanias as variable disturbances of judgment, perception, and emotion—disturbances that differ in degree more than in kind from normal psychic life.
A clinical and anthropological approach to madness
One of the most striking features of Laennec’s eighth lecture is the constant intertwining of clinical observation, historical erudition, and moral reflection. He does not limit himself to describing symptoms or arranging them into a static nosology; instead, he mobilizes a wide cultural repertoire—Aretaeus of Cappadocia, Hippocrates, Plutarch, Pascal, Rousseau, and Horace—alongside contemporary clinical cases to illuminate the many faces of vesania. This mode of reasoning situates his discourse at the intersection of medicine and what might be called a moral and historical anthropology of mental life. Such an approach was not without precedent. As historians have shown, the late 18th and early 19th centuries were marked by a strong interest in the passions, imagination, and the social circulation of beliefs and affects (Goldstein, 1997; Pigeaud, 2001; Weiner, 1999). More recently, Dodman (2018) has demonstrated how nostalgia emerged as a powerful medical and political category in the context of war and empire, while Hewitt (2020) and Murat (2011) have highlighted the deep entanglement between psychiatry, politics, family structures, and social order in 19th-century France. Laennec therefore did not ‘discover’ the emotional or social dimensions of madness. What distinguishes his position is rather the way he integrates these dimensions into a clinician’s epistemology that remains wary of both speculative system-building and anatomical reductionism. When he discusses religious melancholia, for example, he does not simply denounce superstition or credulity; he analyses how an imagination ‘left to itself’ can generate fixed ideas of guilt, persecution, or demonic possession, while also acknowledging that religious frameworks may sometimes contain or channel such excesses. Similarly, in his discussion of nostalgia—particularly among enslaved Black people or soldiers—he does not present it as a mysterious or purely moral entity, but as a state in which sorrow, memory, and bodily decline become inseparably intertwined (Dodman, 2018). Here again, Laennec’s insistence on continuity is central. The same faculties—imagination, memory, belief, and emotion—that structure ordinary human experience may, under certain conditions, become the vectors of vesania. Madness is not a foreign substance invading the mind; it is a distortion, amplification, or fixation of capacities shared by all.
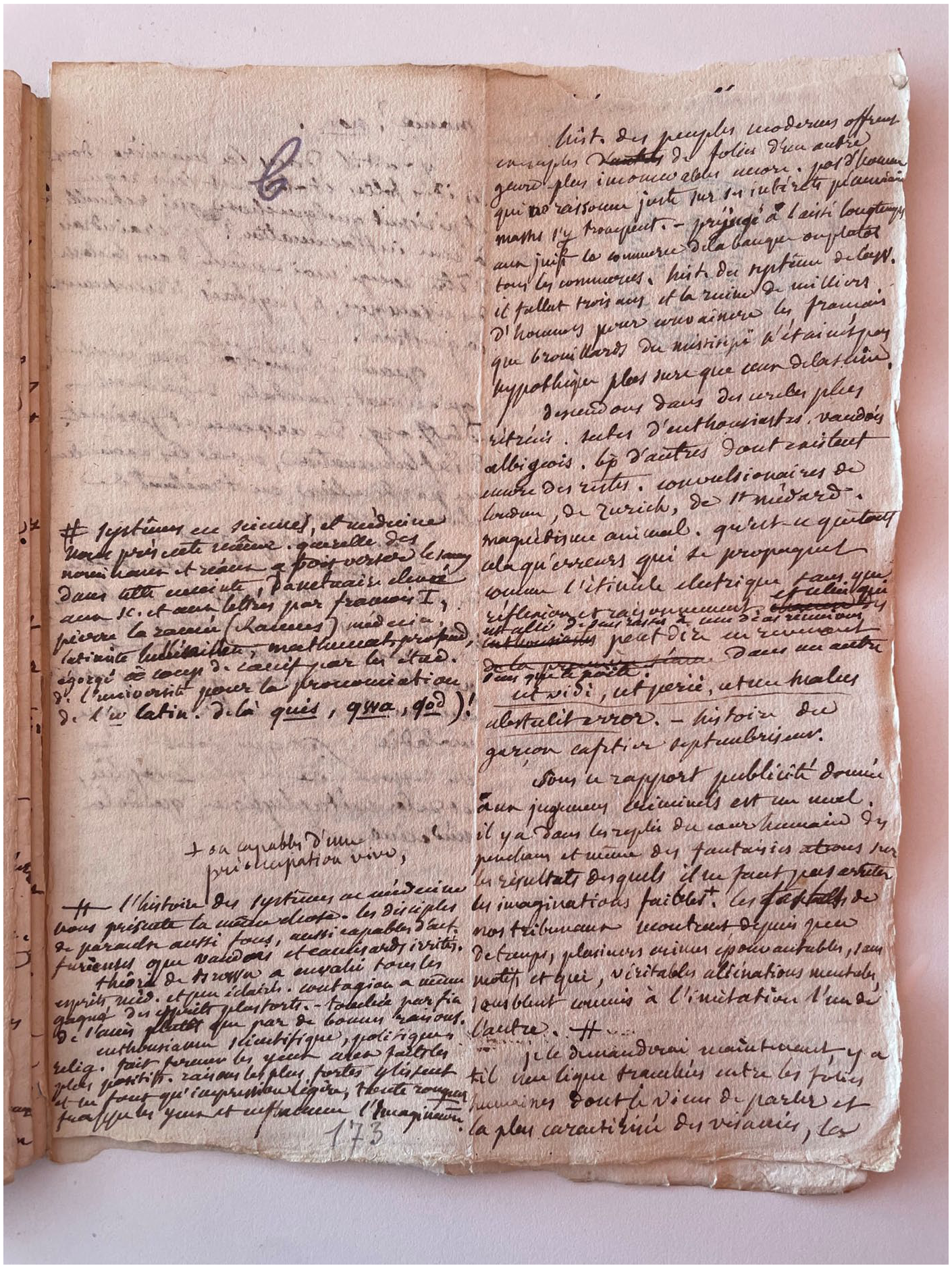
This perspective resonates with, but should not be confused with, later psychological or sociological theories of madness. It remains firmly embedded in early 19th-century medical culture, even as it resists its most rigid compartmentalizations. Laennec extends this reasoning to what he calls collective or epidemic forms of vesania: crusades, revolutionary fervour, financial delusions, and animal magnetism. Once again, this theme was not unique to him, and it would later be elaborated in more systematic ways by authors such as Le Bon (1895) or Freud (1921). Yet Laennec’s interest lies less in constructing a theory of crowds than in illustrating, through historical examples, the permeability between individual and collective passions. For him, these phenomena confirm that error, enthusiasm, and delusion circulate along the same psychological pathways, differing more in scale and intensity than in nature. In this sense, his approach can be described as ‘anthropological’ not because it anticipates modern anthropology, but because it constantly situates mental disorder within a broader reflection on human faculties, history, and social life. It is precisely this refusal to isolate madness from the rest of human experience that gives his lecture its particular tone and enduring interest.
What, then, is original in Laennec?
But any claim about Laennec’s novelty must be demonstrated rather than merely asserted. Laennec did not invent moral treatment, nor did he discover the social or emotional dimensions of madness, nor did he oppose anatomical reductionism more radically than some of his contemporaries. His originality is therefore neither spectacular nor revolutionary. It is, however, conceptually precise and historically significant. First, Laennec consistently places gradation and continuity at the centre of his conception of vesania. While Pinel and Esquirol certainly acknowledged the variability and complexity of mental disorders, their classificatory efforts aimed at stabilizing distinct categories for clinical and institutional purposes (Esquirol, 1838; Pinel, 1801). Laennec, by contrast, repeatedly emphasizes transitional states, borderline cases, and the imperceptible passage from ordinary passions to pathological fixations. This insistence on a spectrum of mental disturbance—rather than on sharply delimited entities—constitutes one of the most distinctive features of his lecture. Second, Laennec adopts a stance of epistemic humility toward the causes of mental illness. He explicitly acknowledges the failure of pathological anatomy to provide consistent explanations for vesanias and refuses to replace one dogmatic system with another. Against Broussais’s inflammatory doctrine, he maintains that the absence of constant lesions is not a temporary gap in knowledge to be filled at any cost, but a structural limit that should caution physicians against premature theoretical closure (Braunstein, 1986; Duffin, 1998). In this respect, his position differs not only from reductionist anatomism, but also from more confident forms of moral or psychological systematization. Third, Laennec maintains a form of pluralistic causality. Mental disorders, in his view, may involve bodily conditions, emotional shocks, social circumstances, habits of imagination, or moral conflicts—often in combination. This pluralism does not amount to a coherent theory of causation, but it does function as a practical safeguard against explanatory monism. Taken together, these elements define Laennec not as a founder of psychiatry, but as a clinician-philosopher occupying a position at a crossroads. His lecture resists both the closure of rigid nosology and the seduction of single-cause explanations. In this sense, his contribution is less a matter of new doctrines than of a distinctive intellectual posture—one that privileges caution, gradation, and attention to the complexity of human mental life.
In light of contemporary psychiatric knowledge
More than two centuries later, how should Laennec’s lecture on vesanias be read? Any attempt to answer this question must avoid two symmetrical pitfalls: anachronistic celebration and antiquarian dismissal. Laennec’s conceptual framework belongs to early 19th-century medicine, shaped by vitalist physiology, moral philosophy, and the limits of pathological anatomy. Yet some of the problems he grapples with—classification, causation, the boundary between normality and pathology—remain central to contemporary psychiatry. At a descriptive level, several of his categories loosely correspond to present-day clinical entities. Hallucinations occupy a central place in psychotic disorders; melancholia evokes what is now termed major depressive disorder; mania recalls bipolar disorder; dementia refers to what are now classified as neurocognitive disorders; and idiocy overlaps with what would today be called severe intellectual disability. His notion of monomania, understood as a partial and circumscribed delusion, resonates with modern descriptions of delusional disorders or certain obsessive and related conditions (Fink, 1999; Rush et al., 2006). These resemblances, however, should not obscure the profound differences in theoretical background, diagnostic criteria, and investigative tools.
One of the most striking convergences concerns Laennec’s insistence on continuity between normal and pathological states. Contemporary research has increasingly challenged strictly categorical models of mental disorder, especially in the field of psychosis and mood disorders, and has proposed dimensional or spectrum-based approaches (Goodwin and Jamison, 2007; Kendler, 2005; van Os et al., 2009). Laennec’s repeated emphasis on gradation, transitional states, and borderline cases can be retrospectively seen as compatible with such perspectives. Yet it would be misleading to portray him as a direct ancestor of these models: his reasoning was grounded not in epidemiology or neurobiology, but in clinical observation and philosophical reflection on human faculties. Similarly, Laennec’s refusal to reduce vesanias to a single cause—whether anatomical, moral, or social—finds an echo in contemporary biopsychosocial approaches, which stress the interaction between biological vulnerability, psychological processes and social context. His pluralistic attitude toward causation functions less as a theory than as a methodological safeguard against explanatory monism. In this respect, his scepticism toward overly confident neurological or inflammatory explanations appears surprisingly modern in tone, even though it was formulated within a very different scientific landscape.
At the same time, important divergences must be stressed. Laennec’s framework remains embedded in vitalist physiology and in a conception of disease that predates modern genetics, neuroimaging and molecular psychiatry. Today, certain forms of dementia, epilepsy-related psychoses or schizophrenia can be associated with structural, functional, or genetic abnormalities detectable through contemporary techniques (Insel and Cuthbert, 2015; Le Bihan, 2015; Owen et al., 2016). The absence of consistent lesions that Laennec observed reflected the limits of 19th-century pathology rather than a definitive argument against biological involvement. Moreover, some of his claims—particularly regarding gender and the frequency of simulation—clearly bear the mark of the social and medical prejudices of his time (Ehrenreich and English, 1973; Showalter, 1987). Finally, following Delille’s (2017) warning about the ‘misuses of the notion of precursor’, it is methodologically preferable to resist the temptation to cast Laennec as a simple forerunner of modern psychiatry. His lecture belongs to a specific epistemic configuration, in which clinical observation, moral reasoning and limited anatomical knowledge were in constant tension. The interest of his text lies less in what it allegedly ‘anticipates’ than in the way it illuminates an alternative manner of thinking about madness—one that foregrounds continuity, uncertainty, and the limits of medical knowledge.
Conclusion
The eighth lecture from 1823 to 1824 by René Laennec on vesanias is of considerable interest on several levels: historical, epistemological, clinical, and anthropological. To reread this text today in light of contemporary psychiatric knowledge is not merely a historical exercise, but a genuine invitation to rethink the very foundations of how we approach madness, normality, and medical practice itself. While Laennec’s psychiatry owes much to Pinel, he frequently contradicts his mentor throughout the lecture. The course ends with a brief but sharp polemic against the prize-winning papers submitted for the Esquirol Prize, which claimed mental illness had organic causes. Laennec retorts: ‘There is no greater ignorance than believing oneself informed about something one does not truly understand’ (Ackerknecht, 1962).
First and foremost, the text bears witness to a pivotal moment in the history of mental disorders. Laennec inherits a medical and philosophical tradition oscillating between humoral explanations, clinical observation and moral speculation. Unlike Pinel, who laid the foundations of institutional psychiatry, or Esquirol, who sought to classify madness into rigid diagnostic categories, Laennec maintained a flexible approach that gives the lecture its richness. He did not claim to explain everything, much less cure it all. He observed, described, and suggested. He acknowledged the failure of anatomy in explaining vesanias but did not despair of their understanding. He never gave up on observation, clinical intuition, or moral reflection. In his view, mental illnesses were primarily distortions of judgment and concern not just the physician, but also the philosopher and moralist. Physicians address functional disorders and organic lesions—yet neither is consistently found in these cases. This is why, he argued, medical treatment is of limited use, whereas ‘moral’ treatment may prove more effective. He found it scandalous that some were now claiming mental illness resulted from organic lesions or, worse still, inflammation, as proposed by Broussais (Braunstein, 1986; Duffin, 1998).
Secondly, the lecture represents an attempt to understand madness not as a radical break from reason, but as an intensification or deviation of universal human faculties. Hallucinations, fixed ideas, judgment illusions, grandiose or depressive delusions are not seen as absolute anomalies but as pathological forms of normal psychic activity. Imagination, love, guilt, religiosity, sadness, anger, or even jealousy—under certain conditions—may become the matrices of vesania. In this way, Laennec offers a deeply human portrait of madness, free from reductionism and hasty pathologization of behaviour. This vision—one might call it anthropological—resonates strikingly with contemporary approaches to mental health, which emphasize the continuity between normal and pathological, the multifactorial nature of psychiatric disorders, and the need to consider the patient’s subjective experience (Kendler, 2005; van Os et al., 2009). Laennec’s cautious voice still rings as a call for epistemic humility. His lecture is also valuable for its critical dimension. He firmly rejects organic reductionism, which still persists in some branches of neuropsychiatry, and opposes the idea that vesanias must always have a cerebral lesion. While he concedes that some forms of idiocy or dementia may be accompanied by visible brain damage, he insists that most mental illnesses have no anatomical support and must therefore be approached with other tools: psychology, morality and philosophy. The lecture reveals Laennec’s will to think independently, outside prevailing trends—a mark of his great intelligence.
Perhaps the most important aspect of this lecture lies in its clinical and moral depth. Laennec never isolates mental illness from history, culture, or society. He sees in popular movements—the Revolution, crusades, religious sects, and animal magnetism—collective forms of vesania, illustrating the contagion of passion and mass irrationality (Freud, 1921; Le Bon, 1895). This perspective, striking in its lucidity, anticipates later research on social psychology, mass psychosis, and the construction of irrational belief systems. All of this reminds us that madness is never purely biological, nor solely medical—it involves the whole person: body, mind, language, emotions, and historical context. Reading Laennec is not a return to the past, but a way to draw on a broad, rigorous, and humane form of thought—one that remains a vital resource for understanding mental health in the 21st century.
Footnotes
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Project ‘Laennec writing the clinic’ supported by Grant No. ANR-24-CE27-2197-01.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.