
Abstract
In this paper the hypotheses on differences among welfare state sectors with regard to decline and convergence are subject to comparative empirical tests focusing on healthcare. A diachronical cross-national analysis of healthcare services is performed, comparing developments with that of cash benefits. Contrary to previous claims we find that European healthcare systems are not particularly hit by retrenchment and that convergence is absent in key healthcare dimensions, namely coverage and provision. Convergence appears mainly in terms of the increased reliance on private healthcare financing. Our examination is based on Organisation for Economic Co-operation and Development (OECD) Health Data and institutional data on entitlement levels of major cash benefit programmes, providing both a descriptive analysis and multi-level regressions.
The slowdown of welfare state expansion since the 1970s has initiated an ongoing discussion about the stagnation and possible decline of social policy (for example, Pierson, 1996; Esping-Andersen, 2002), something that has given a new impetus to research on welfare state convergence (Brady et al., 2005; Starke et al., 2008). Healthcare has not been immune against such expectations of cross-national institutional conformity, often in the downward direction (Bonoli and Palier, 2000; Castilla, 2004; Wendt et al., 2005).
Hitherto welfare states have been rather resistant to major systemic change and in this regard the likelihood for changes within programmes seems to be greater. One example is cuts in major cash benefit programmes over the most recent decades (Korpi and Palme, 2003; Montanari et al., 2008; Nelson, 2008). Another example is the shift from public to private actors in state financed and regulated healthcare systems (Wendt et al., 2009). In an influential study Clayton and Pontusson (1998: 96) argue that retrenchment is most likely to occur in public social services, thus leading to an ‘anti-service bias of welfare state retrenchment’. One supposed reason for the greater vulnerability of services is the lower immediate visibility of cuts, in comparison to that in cash benefits. A further reason is the fear of European governments for so-called social tourism due to increased European integration.
The purpose of this paper is to subject the above hypotheses of welfare state decline and convergence to empirical tests with regard to healthcare. Does the restructuring of the European welfare states involve processes of convergence, whereby central dimensions of healthcare are becoming more alike? Is it possible to observe stronger cutbacks in European healthcare than in major cash benefits? With an institutional perspective three basic dimensions of healthcare are examined: financing, coverage and provision. Financing concerns the share of contributions coming from public and private sources, rather than expenditure levels. Coverage shows the extent to which citizens are eligible for healthcare, whereas provision relates to the content of services that are being offered.
The paper is organized in the following way. In the next section we review the retrenchment thesis of social services more generally, followed by an identification of the specific pressures toward convergence emanating from the EU. Thereafter, we discuss issues related to data and measurement. The results of the empirical analysis are then presented, followed by a concluding discussion.
The vulnerability of social services revisited
The thesis of greater vulnerability of social services for retrenchment can be questioned on several accounts. Since social insurance principles inform the organization of healthcare in most parts of Europe, there would be little need to decrease healthcare services in order to prevent social tourism. In healthcare services we find, in fact, a degree of resemblance with major contributory social benefit programmes, in which entitlement levels often depend on employment and earned income. In comparison, the problem of social tourism should be more evident for non-contributory and means-tested social assistance benefits, where EU legislation in part prohibits discrimination based on nationality. However, even in connection with social assistance, social tourism seems to be limited among the EU countries (Kvist, 2004).
The substantial shift that has occurred in the area of social reproduction, especially in the UK and parts of Continental and Southern Europe, where caring responsibilities have moved from the family to become production work in the market or the public sector, makes a presumed reversal of the consistent development in the size of social services even less likely (Gornick et al., 2003; Esping-Andersen, 2009; Montanari, 2009). In addition, the often strong popular support of healthcare should increase the risk of political backlash associated with disliked cuts (Blekesaune and Quadagno, 2003) and thus add to the resistance of healthcare to major change. Healthcare is an important component of the European welfare states, cherished by an overwhelming majority of the population, and also by political opponents to other forms of social policy. The limited degree of moral hazard and elimination of disease contagion are probably some reasons for the support of an effective healthcare among citizens in general. For policy-makers, healthcare may also be seen to guarantee a healthy workforce and thus to constitute an important component of the productive welfare state (Midgley, 1999; Freeman, 2002).
Finally it should be noted that the empirical evidence used by Clayton and Pontusson (1998) to support the vulnerability hypothesis of public social services is problematic. The decline of social service expenditure in Sweden and the UK, for example, is mostly due to the out-sourcing of service provision to private actors and to administrative reforms, rather than to restrictions in access and cuts in levels of service provision (Anell, 2005; le Grand, 2009). For the above reasons we do not expect European healthcare systems to have been particularly hit by retrenchment, as envisioned by Clayton and Pontusson (1998).
European integration and national healthcare reform
Despite the potential for strong public support and its prime position as a social investment, healthcare may of course be subject to changes. Several scholars have linked the recent development of European healthcare systems to the broader issues of welfare state convergence and European integration (Bonoli et al., 1996; Greve, 1996; Taylor-Gooby, 1996; Wendt et al., 2005). Pressures towards welfare state convergence are assumed to emanate from four distinct areas of EU regulation: The Broad Economic Policy Guidelines (BEPG), EU Competition Law, the Open Method of Coordination (OMC) and the European Court of Justice (ECJ) (McKee and Mossialos, 2006; Obermaier, 2009; Mossialos et al., 2010; Scharpf, 2010; Graziano et al., 2011). The BEPG include low inflation, balancing of national budgets and exposure to competition in every field. In this way the space for national differences in economic and financial policy is heavily circumscribed, something that indirectly may promote social policy convergence in a downward direction.
Competition law expresses the baseline of EU cooperation. Apart from cartel building and other anti-competitive behaviour among companies, restrictions apply explicitly to any public procurement in sectors such as transport, education and healthcare. Although the formulation and implementation of health policy still remains a task of national polities, the ongoing development of the internal market as established in EU treaties and driven by EU institutions and specifically the ECJ, is transforming the legal environment under which health systems contract employees, purchase goods, collect revenue and organize themselves (Lamping, 2005; Greer, 2010). Collectively organized and provided healthcare may in the EU be substituted by market production of the same services by outright sales or by auctioning-out of service production while maintaining state financing (for example, Clarke and Newman, 1997). Different forms of marketization of service production continue to develop along the process of European integration. In a longer time perspective, and given that patients and medical personnel are free to move around Europe demanding or offering healthcare services, competition is expected to result in a Europe-wide concentration of certain specialist healthcare services (McKee and Mossialos, 2006). We consider such development to be of less relevance for primary care services.
The OMC, a new form of governance within the EU (Borrás and Jacobsson, 2004), promotes standards and benchmarks in various fields, such as education, employment, poverty alleviation and healthcare. Although the social policy agenda of the OMC principally regards the implementation of institutions in order to enhance social stability and prevent social tourism, the continuous exchange of expert-led best practices may lead to discursive consensus on institutional convergence (Schmidt and Radaelli, 2004). With regard to healthcare, the continuous benchmarking procedures and promotion of ‘best practices’ may have important future effects especially for new and aspirant Member States (McKee et al., 2004; Hervey, 2007).
The ongoing discussion about the role of EU integration for European healthcare systems has provided new insights concerning the driving forces of institutional change. Besides the general pressure of cost-containment, which may be reinforced by EU economic integration, changes in the private and public mix of healthcare financing have been recognized and linked in part to developments at the EU level (Wendt et al., 2009). Another example is provided by Sindbjerg Martinsen and Vrangbaek (2008), who link the market based principles of Danish healthcare to the ECJ’s decisions on patient mobility. The possible spatial concentration of specialist healthcare services noted above may also entail increased user fees at the patient level, thus contributing further to an increased share of private healthcare financing (Newhouse, 1992). The level of healthcare provision and especially health employment may have been affected as well, for example, by the judicial interpretation of the ECJ’s decision on the Working Time Directive (Sheldon, 2004). The OMC may also have had some imprint on national healthcare systems in parts of Europe where social development has been lagging behind. For example, the OMC invoked positive pressure on Spain to move towards nearly full coverage of primary healthcare services (Guillén and Álvarez, 2004).
Despite these testimonials of a relationship between European integration and the core dimensions of healthcare analysed in this paper, both the direction and the magnitude of the association can be questioned. European integration is only one of several factors that exert pressure on national healthcare systems. Moreover, patient and professional mobility within the EU remain relatively limited, despite the common market and rulings of the ECJ (World Health Organization, 2005). While recognizing potential spill-over effects of European integration on national healthcare systems, Marmor et al. (2005: 338) concludes that ‘there is as much evidence of continued difference (or divergence) in national arrangements for the finance, delivery and regulation of healthcare as there is of increasing similarity’.
Ideological orientations and institutional legacies are two supposed reasons for the continued diversity of European healthcare systems, despite the seemingly common objective pressures for policy change (Jacobs, 1998; Hacker, 2004). The former factor brings partisan politics back into the theoretical framework of welfare state reform (for example, Korpi, 1985), something that is important not only for the development of cash benefits, but also for the development of social services and healthcare policy (Huber and Stephens, 2000). Thus, in a similar way to the discussion on the retrenchment hypothesis above, we do not anticipate any univocal evidence of healthcare convergence in Europe.
Data and measurement
Comparative healthcare analyses involve major conceptual difficulties (Jordan, 2010). This concerns not least the analysis of potential trade-offs between governments’ capacity of cost-control and individual choice, areas that have been in focus for health economics over the last decades (Bevan et al., 2010). 1 Although we do not directly address the issues of horizontal and vertical equity, our institutional approach to the comparative analysis of healthcare systems draws attention to policy structures of relevance for health outcomes. 2
We have in this paper chosen to examine the development of healthcare in Europe in three core analytical dimensions, coverage, financing and provision. 3 Whereas coverage and financing for long have been important dimensions in comparative healthcare research (Organisation for Economic Co-operation and Development, 1987), the level of service provision has more recently come into focus (Moran, 2000; Bambra, 2005). Since countries tend to move in clusters with distinct combinations of scores on the various dimensions some scholars have asked for more systematic comparative analysis in this regard (Wendt et al., 2009). We do not expect the three dimensions of healthcare coverage, financing and provision to be linearly interrelated. 4 It is, however, beyond this study to propose any systematic classification or new model types.
Our empirical analysis of European healthcare systems is based on OECD Health Data 2008. Coverage refers to the number of citizens eligible for healthcare services financed by public funds, irrespective of whether the actual service provider is a public or private actor. For healthcare financing we distinguish between public and private expenditure for activities directly related to healthcare services. 5 In addition we analyse user fees; that is, private out-of-pocket financing paid directly by households after contact with the services. 6 User fees are of relevance for vertical equity in the ability to pay for services. Although parts of health expenditure are allocated from general tax revenue, payroll taxes, premiums and so forth, we do not analyse the pooling of pre-payments as such. Nonetheless, it should be recognized that the composition of pre-payments are important for various outcomes related to both the distribution of health resources and healthcare costs (Kutzin, 2010).
Healthcare provision is measured in terms of health employment, medical equipment and hospital beds, with all figures related to the size of total population. Healthcare employment includes the number of practising physicians and nurses. Medical equipment includes the number of computed tomography scanners, magnetic resonance imaging units, radiation therapy equipment, lithotriptors and mammographs. Hospital beds are measured both in total and in terms of acute care beds. Acute care beds are regularly maintained, staffed and immediately available for the care of admitted patients. Each country’s score in 2006 on the healthcare variables analysed below are shown in the appendix (Table 1A).
In order to analyse systematically whether in recent decades cash benefits or healthcare have suffered the most from welfare state stagnation and decline we use data on benefit levels from the Social Citizenship Indicator Programme (Korpi, 2009) and the Social Assistance and Minimum Income Protection Interim Dataset (Nelson, 2010). Our study includes 19 EU countries: Austria, Belgium, Czech Republic, Denmark, Finland, France, Germany, Greece, Hungary, Ireland, Italy, Luxembourg, the Netherlands, Poland, Portugal, Slovakia, Spain, Sweden and the UK. We restrict our analysis to the period 1980–2006, during which European integration has been significantly strengthened, both in content and space. Over this period the pressures for welfare state reform have also markedly grown, for example due to global economic developments and demographic shifts. This period therefore gives excellent opportunities to analyse whether governments in different countries follow the same pattern in the restructuring of healthcare.
Results
The growth of healthcare expenditure in recent decades has introduced a shift in financing responsibilities. Figure 1 shows changes in private and out-of-pocket health expenditures as percentages of total health expenditure in 19 EU countries 1980–2006. Due to the large amount of missing values, out-of-pocket expenditure is shown only from 1990 and onwards. The coefficient of variation is used to analyse cross-national differences. It is evident that private healthcare financing has become more prominent. Between 1980 and 2009 the share of private healthcare financing increased on average by about 22 percentage points. The decline around 1990 is due to breaks in the series and the subsequent inclusion of the Czech Republic and Poland in the analysis. Although public financing still accounts for the largest share of total health expenditure, the private part of healthcare financing is on average at a level of 24 percent. In absolute terms this share amounts to about 1.9 percent of GDP, which can be compared with 1.4 percent of GDP in 1980.
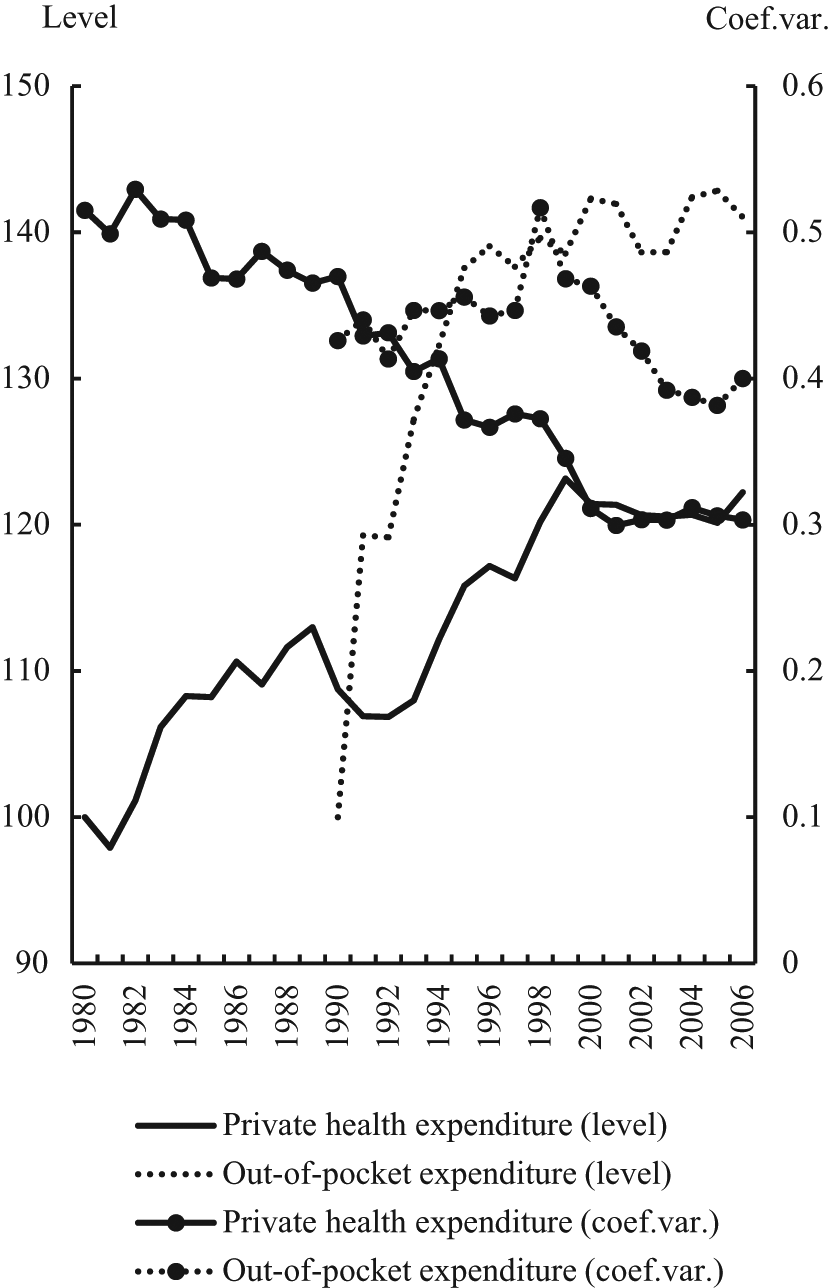
Private healthcare financing in 19 EU Member States 1980–2006. Private health expenditure and out-of-pocket expenditure and out-of-pocket expenditure as a percentage of total health expenditure. Levels index 1980=100(private health expenditure) and index 1990=100(out of pocket expenditure). Coef. Var., coefficient of variation.
All-country averages conceal differences between individual countries, which sometimes can be substantial. For example, private healthcare financing is about 30 percent of total healthcare expenditure or higher in Greece, Hungary, the Netherlands, Poland, Portugal, Slovakia and Spain. At the other end of the distribution, with levels of private healthcare financing below 20 percent, we find Denmark, Sweden, UK, the Czech Republic and Luxembourg: countries dominated by universal healthcare systems. Private healthcare financing has increased most dramatically in Sweden and the Central and Eastern European (CEE) countries. Between 1990 and 2006 private healthcare financing more than doubled in Sweden, from about 8 to 19 percent of total health expenditure. The share of private financing more than quadrupled in the CEE countries. Austria, Greece and Portugal show changes in the opposite direction, with the private share of health expenditure declining by about 13 percentage points, probably reflecting efforts in the 1980s and 1990s to make insurance-based healthcare systems more universal in character (Saltman and Figueras, 1997).
Several European countries are struggling with escalating public health expenditure. To control or reduce public expenditure countries have increased competition among health insurance providers and strengthened individual responsibility for user charges. User fees have in fact increased in most European countries, particularly in the early 1990s, but also at a more moderate pace in subsequent years. They constitute the lion’s share of private healthcare financing in most European countries, reaching an average of about 70 percent of private health expenditure in 2006. Its size in total health expenditure rose from about 11 to 16 percent between 1990 and 2006.
From an equity point of view the trend towards an increased reliance on out-of-pocket expenses is problematic, since they tend to be more regressive than private health insurance premiums, at least in Europe where private health insurance is mostly complementary to public financing sources. Conversely, public financing sources are mostly progressive in nature and thus of greater benefit to lower income strata (De Graeve and Van Ourti, 2003). Thus, in terms of financial fairness the increase of private health expenditure and especially out-of-pocket payments seem to be congruent with the expectation of welfare state decline in the social service sector referred to above. 7 The fees charged for doctor’s visits was also used by Clayton and Pontusson (1998) to assess the extent of cutbacks introduced to public social services in Sweden. However, it is important to point out that there is still substantial cross-country variation concerning the relative size of out-of-pocket expenditures. The share of out-of-pocket expenditure is particularly high in Belgium, Italy and Poland reaching more than 20 percent of total health expenditure and more than 80 percent of private health expenditure. At the lower end we find France and the Netherlands, with out-of-pocket expenditure of less than 10 percent of total health expenditure and less than 40 percent of private health expenditure. Despite noticeable differences between individual countries the general increase in private health expenditure in Europe is an indicator of convergence, whereas it is difficult to observe any clear overall trend concerning the dispersion of out-of-pocket expenditure. Similar results appear if the CEE countries are excluded from the analysis.
A comprehensive account of the possible retrenchment in European healthcare systems goes beyond an analysis of financing principles. Perhaps equally important for the distribution of healthcare and health-related outcomes is legislation governing access to the services. Most European citizens have access to healthcare and European healthcare systems thus have very high coverage rates. The rather small differences in healthcare coverage that exist in Europe are to a large extent related to the fundamental structure of healthcare systems; that is, whether eligibility is universal or insurance-based (Schieber and Poullier, 1987). Universal healthcare systems with full coverage were often established in Europe before the 1980s and it is difficult to find any clear evidence of restrictions being imposed on access to these services. This development seems to be markedly different from that of the major contributory benefit programmes, where Clayton and Pontusson (1998) note that access to entitlements have gone down due to the large increase of the non-working population. Since eligibility for healthcare in Europe is less strongly connected to employment than the major contributory benefit programmes, healthcare coverage is very stable among the countries here studied. Over the last two decades the share of eligible citizens in total population only fluctuates by a couple of percentage points around the 1980 baseline. In 1980 the average coverage rate of the 19 EU member states was 95.8 percent. The corresponding figure for 2005 is 97.0 percent. Over these years the dispersion of coverage rates across the EU member states is extremely stable, with changes only in the fourth decimal of the coefficient of variation for 1980 and 2005.
Reflecting developments in the Netherlands the average coverage rate increases to 98.9 percent in 2006, whereas cross-national dispersion goes down substantially. 8 The Netherlands used to be a European outlier in terms of healthcare coverage, with rates fluctuating around 60 percent between 1980 and 2005. As part of a major restructuring of healthcare, whereby citizens became required to purchase private health insurance, coverage was substantially extended (Palier and Martin, 2008). Nowadays almost all Dutch citizens are eligible for healthcare. Developments in other countries also deserve comment. Only Greece and Italy made the transition towards full coverage during the observation period. Greece went from a coverage rate of 88 percent in 1983 to 100 percent in 1984. For some people, however, full coverage in Greece simply means access to public hospitals, since public primary care facilities are far from meeting the demand (Cabiedes and Guillén, 2001). Italy achieved full coverage in 1980, a few years earlier than Greece. Portugal was the first among the Southern European countries to introduce universal healthcare and full coverage was reached already in the 1970s. Spain does still not have full healthcare coverage, although substantial extensions to eligibility were introduced in the 1990s. In Continental Europe we find countries moving in the opposite direction with strengthened insurance-based principles. In Germany, for example, healthcare coverage shows a slow but steady decline since the early 1980s, after a couple of decades associated with stable increases. Nonetheless, it should be recognized that Germany introduced compulsory health insurance with full coverage in 2009, which is not captured by our data. Reforms in the CEE countries were largely triggered by intense political pressure to replace elements of the previous authoritarian regimes, but progress has often been slow due to various financial and political obstacles (Saltman and Figueras, 1997). Nonetheless, both the Czech Republic and Hungary have full healthcare coverage. Together with Denmark, Finland, Ireland, Sweden and the UK full coverage is reached in about half of the 19 EU countries in 2006. In nine European countries with insurance-based healthcare systems approximately less than 5 percent of the total population lacks healthcare. Included here are Austria, Belgium, France, Germany (for 2006), Luxembourg, the Netherlands, Poland, Slovakia and Spain.
With the exception of the Dutch case, the stability of healthcare coverage in Europe since 1980 does not imply that European healthcare systems are immune against cutbacks. Whereas eligibility and coverage are closely related to the basic principles governing access to European healthcare systems, resulting in complete or nearly full coverage throughout Europe, more gradual reforms may have affected the level of services provided. One way to analyse this dimension of European healthcare systems in closer detail is to explore levels and dispersion of healthcare provision. Figure 2 shows health employment, hospital beds and medical equipment for the years 1980–2006 in the 19 EU countries. Due to the large amount of missing values, developments in medical equipment are analysed only from 1990 and onwards. Whereas health employment and medical equipment have increased almost continuously over the period, the number of hospital beds has declined. 9 The improvement of medical equipment reflects the fast and consistent growth of the biomedical and pharmaceutical industrial sectors (Clemente et al., 2008), being an important driver for increasing per capita healthcare expenditure (Okunade and Murthy, 2002).
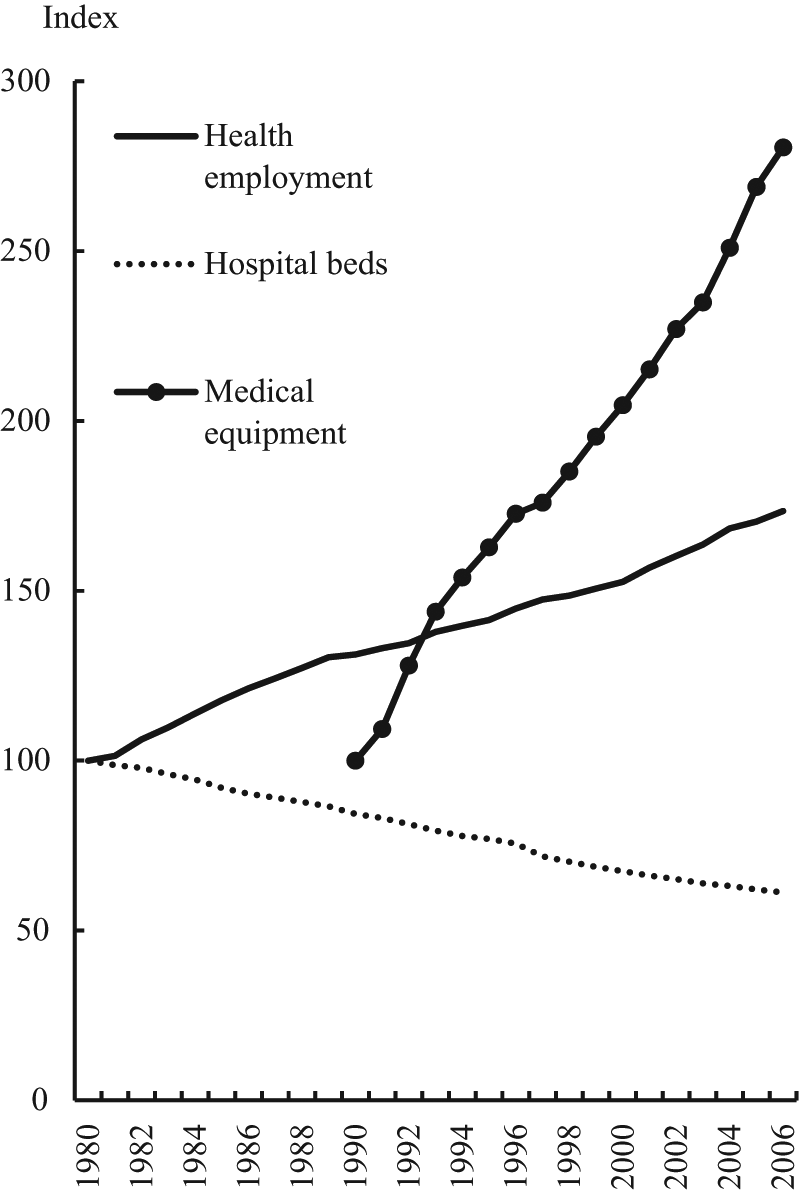
Levels of health employment, hospital beds and medical technology in 19 EU Member States 1980–2006, index 1980=100. Health employment includes practising doctors and nurses. Healthcare beds includes total and acute healthcare beds. Medical equipment includes computer tomograph scanners, MRI units, radiation therapy equipment, lithotriptors and mammographs. Healthcare provision is an additive index comprising health employment, healthcare beds and medical technology. Medical equipment is measured from 1990 onwards.
The increase of health employment and medical equipment can to some extent be interpreted in qualitative terms and as improvements in healthcare provision, although we lack data on the distribution of services. It is, however, more difficult to judge whether the trend towards fewer hospital beds is a sign of retrenchment. As part of major restructurings of healthcare, most EU countries have reduced the number of acute care beds almost continuously since 1980, at least, and increased the number of patients subject to specialized nursing care. Alternatively patients are treated at home with the assistance of community-based health and social care services. There are several reasons for this re-organization of healthcare services, including both cost-cutting pressures and changes in treatment and care options, such as the availability of new prescription drugs (Healy and McKee, 2002).
Although the three indicators of healthcare provision have developed quite differently over the years, the overall trends do not correspond to Clayton and Pontusson’s (1998) claim for welfare state decline and greater vulnerability of service provision. Since we also have data on the generosity of cash benefit schemes, we can here systematically compare developments in both benefit levels and service provision. Figure 3 shows indices of healthcare provision, social insurance replacement rates and social assistance benefit levels 1980–2005. It is evident that healthcare provision has not necessarily suffered from more serious retrenchment in recent decades than cash benefit programmes. In fact, we observe quite the opposite. Between 1980 and 2005 the index of healthcare provision increased by about 25 percent, even though during the 1980s we find primarily a state of stability or even of a slight decline. Much of this increase is due to the exceptional development of medical equipment since 1990. If medical equipment is excluded from the index of healthcare provision the increase is more modest (about 16 percent since 1990). The slight decline in healthcare provision in the 1980s disappears when medical equipment is excluded. Thus, healthcare provision does not seem to be particularly prone to cutbacks. Rather it is cash benefits that have suffered from retrenchment in recent decades, quite contrary to previous claims. Social insurance replacement rates have declined on average by about 10 percent between 1980 and 2005. The decline is somewhat larger for sickness benefits and even more so for social assistance. Based on the empirical evidence presented here on healthcare provision, Clayton and Pontusson’s (1998) hypothesis of greater vulnerability of social services cannot be substantiated.
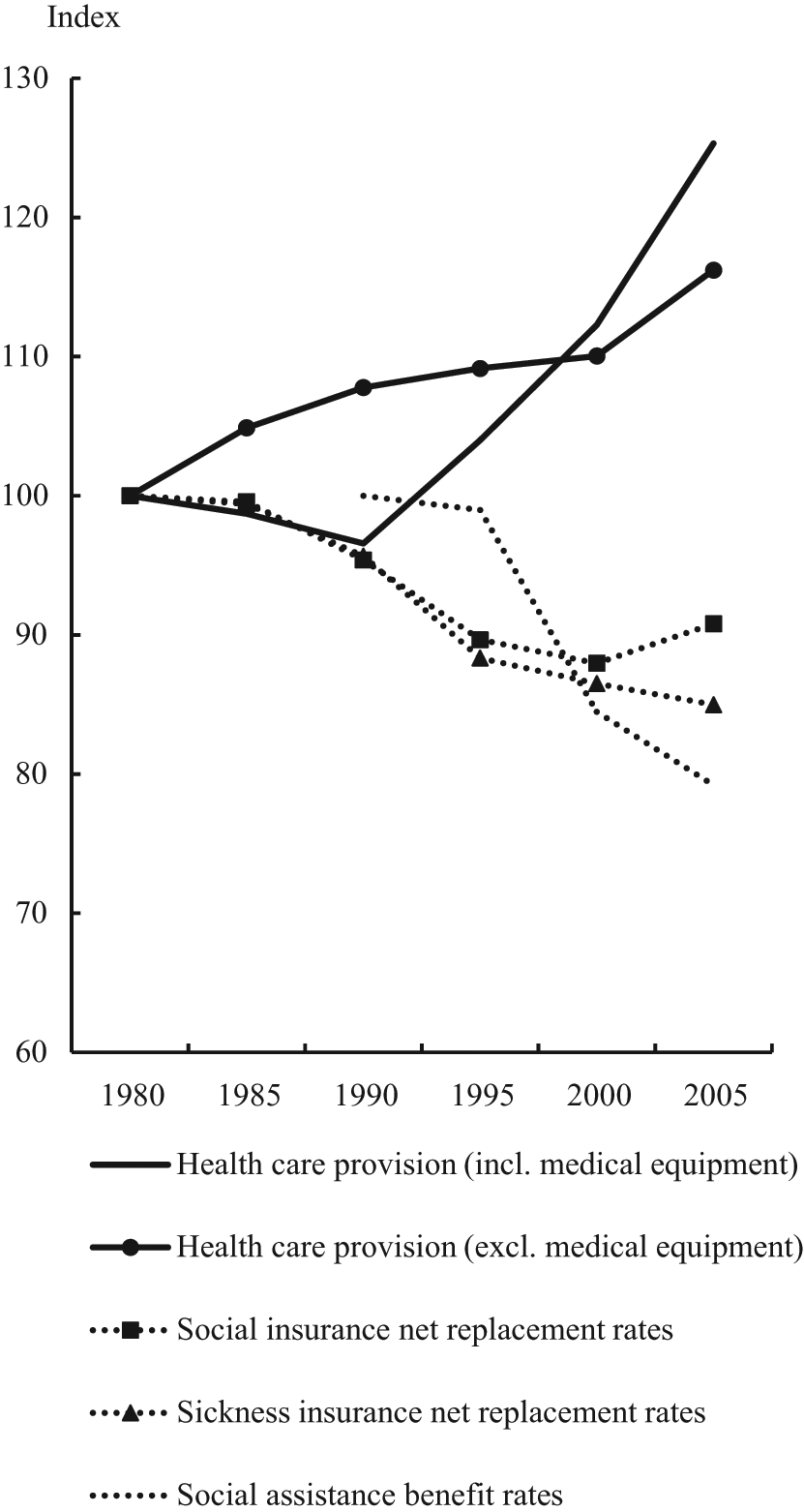
Index of healthcare provision, social insurance net replacement rates and social assistance benefit levels in 19 EU Member States 1980–2006, index 1980=100. Index of healthcare provision includes health employment, hospital beds and medical equipment. Social assistance is indexed according to 1990 levels.
Since European integration has not resulted in substantial decline of healthcare services we cannot expect to observe any downward convergence in healthcare provision. Instead the development may translate into upward convergence, whereby countries with less elaborate healthcare systems are catching up on countries ranked higher in the welfare league. This is the type of healthcare convergence envisioned by McKee et al. (2004) and Hervey (2007) due to the introduction of the Open Method of Coordination (OMC). If the opposite applies, a fanning out pattern occurs, showing divergence in healthcare provision, where countries with a more elaborate welfare state introduce more improvements in healthcare than countries in the lower ranks.
Figure 4 shows cross-national dispersion in the index of healthcare provision for the 19 EU countries in 1980–2006. Also included in the figure are separate series for health employment, hospital beds and medical equipment. Contrary to common expectations about the convergence of European welfare states, the period of improvements in healthcare provision since 1980 is associated more with divergence. The EU countries are becoming less similar on all three indicators of healthcare provision. Medical equipment varies most extensively across countries, followed by hospital beds and health employment. The inclusion of the Czech Republic and Poland around 1990 makes the index of healthcare provision rise sharply. Even though the dispersion in the index of medical equipment describes somewhat of a rollercoaster pattern, the overall trend is an increase in the coefficient of variation between 1990 and 2006. The provision of hospital beds shows the clearest and most stable pattern of divergence. In particular developments in the 1980s made countries more different in terms of the number of hospital beds; something that continued to characterize cross-national variation also during subsequent years, albeit with weaker signs of divergence. Health employment shows more diversified long-term changes. In the 1980s health employment converged, whereas the following years are characterized by divergence.
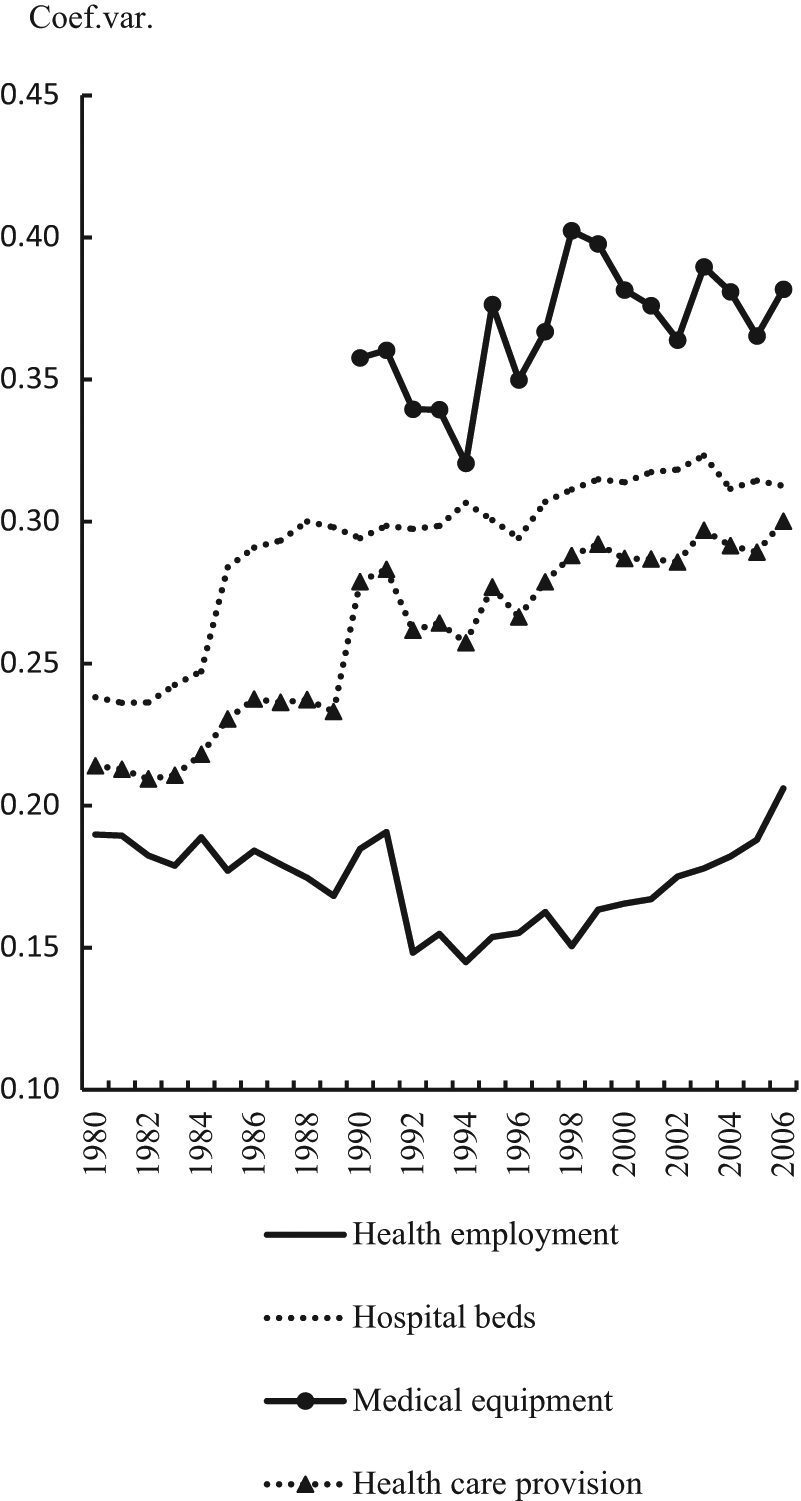
Dispersion of healthcare provision in 19 EU Member States 1980–2006. Health employment includes practising doctors and nurses. Healthcare beds includes total and acute care beds. Medical equipment includes computer tomograph scanners, MRI units, radiation therapy equipment, lithotriptors and mammographs. Healthcare provision is an additive index comprising health employment, heathcare beds and medical equipment. Coef. var., coefficient of variation.
The descriptive analysis of healthcare systems above shows that the hypotheses of welfare state decline and convergence of European healthcare are not fully supported. Of the three dimensions of healthcare analysed in this paper, only private healthcare financing shows clear signs of convergence for the period 1980–2006. Increased out-of-pocket expenditure does, however, not translate into greater similarities in the financing of European healthcare systems, nor is it possible to find any convergence tendencies in healthcare coverage. Neither could we observe downward convergence in all aspects related to healthcare provision.
In order to provide formalized evidence of healthcare developments we will also apply a multilevel analyses based on repeated data. Table 1 shows the core results from a series of multi-level random slope regression models using healthcare financing, provision and coverage as dependent variables and a time variable as an independent variable. 10 We are particularly interested in two distinct parts of the models. The first is the fixed effect of the time variable, which shows whether the overall trend is increasing or decreasing. The second is the covariance between the intercept and the slope of the time variable across countries, which provides crucial information concerning cross-national differences (Twisk, 2003). Convergence is observed if the two estimates have opposite signs. Similar signs reveal divergence. 11 The results confirm the findings from the descriptive analysis above, since patterns of convergence tend to disappear when we move from financing to provision. Contrary to common expectations of convergence the developments in central dimensions of healthcare provision have thus introduced greater institutional diversity in Europe. The exclusion of the CEE countries does not affect the analysis to any larger extent.
Multilevel regression of healthcare financing, provision and coverage in 19 EU Member States, 1980–2006
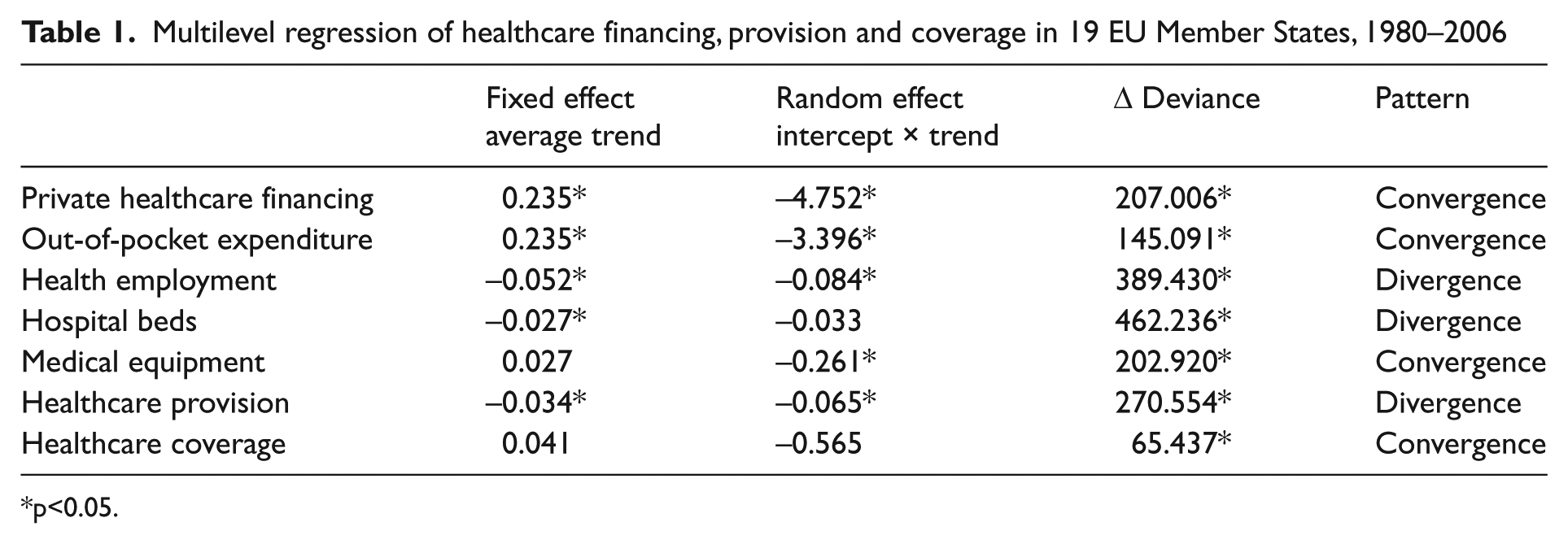
p<0.05.
Discussion
In this paper we have analysed healthcare developments in a large number of EU Member States, subjecting hypotheses of decline and convergence to empirical tests.
Three core dimensions of healthcare services were examined: financing, coverage and provision. In comparison with cash benefits, where retrenchment has been observed, we did not find any stronger evidence for decline in healthcare coverage and provision. Clayton and Pontusson’s (1998) argument concerning the greater vulnerability of public social services is thus not supported by our empirical data. Nor did we observe any strong convergence in the organization of healthcare. Countries have only become more similar in terms of increased private healthcare financing, whereas other dimensions such as healthcare provision has tended to diverge. Thus, there is not enough empirical evidence showing that European integration has lead to greater institutional conformity in core healthcare dimensions.
It is doubtful that the evidence presented here is the result of any systemic changes, possibly with the exception of the transition from social-insurance based systems to universal healthcare systems in a few countries, something that has strengthened access to the services and sometimes even resulted in complete healthcare coverage (Wendt et al., 2009). Internal changes of levels in the core healthcare dimensions have been easier to discern. Apart from the increased share of private financing, the changes introduced to healthcare seem to have been more diversified, contributing more to divergence than convergence. The extent to which these policy changes have reinforced previous categorizations of European healthcare systems into different institutional types needs to be analysed elsewhere.
The framework for an institutional analysis of European healthcare systems presented in this paper shows promising results and gives topical interest to alternative explanations for European policy reform. Nationally embedded driving forces in particular deserve explorations, such as the role of partisan politics. The regulation of the medical profession is another factor of interest, something that concerns the qualifications of medical personnel and the conditions of professional performance (Moran, 2000). In the long-term perspective the independence of members of the medical profession has gradually been eroded through political intervention circumscribing the range and forms of exercise. However, the privatization of healthcare provision especially in countries with tax-financed healthcare is reversing this trend (Ameringer, 2008), something that may influence the political setting of priorities and service distribution, both geographically and socially. The introduction of purchaser-provider splits, or quasi-markets, in healthcare provision may also be of relevance in this regard, especially concerning equity in access to healthcare (Shafrin, 2009). Precise contractual regulation and adequate payment methods are recommended to prevent escalating healthcare expenditure as well as cream-skimming on the part of private providers.
The above discussion illustrates the great need for continued analyses of European healthcare systems and the creation of comparative benchmarks against which individual countries can be evaluated. Such work should entail analyses based on institutional comparative data of the sort applied in this study and theoretical assessments of the latest claims concerning the direction and magnitude of institutional change. This study clearly shows that large-scale comparative welfare state research can fruitfully be broadened to encompass not only developments in cash benefits, but also the evolution of social services.
Footnotes
Appendix
Values on the dependent variables in 19 EU Member States, 2006
| Country | Private health expenditure (percent total health expenditure) | Out-of pocket health expenditure (percent total health expenditure) | Healthcare coverage (percent total population) | Health employment (percent total population) | Hospital beds (percent total population) | Medical equipment (percent total population) | Healthcare provision |
|---|---|---|---|---|---|---|---|
| Austria | 23.8 | 16.5 | 99.0 | 0.52 | 0.95 | 0.60 | 0.69 |
| Belgium | 26.0 | 20.9 | 99.0 | 0.79 | 0.75 | 0.72 | 0.75 |
| Czech Republic | 11.8 | 11.5 | 100.0 | 0.54 | 0.93 | 0.41 | 0.63 |
| Denmark | 15.8 | 14.3 | 100.0 | 0.70 | 0.46 | 0.50 | 0.55 |
| Finland | 24.4 | 18.7 | 100.0 | 0.47 | 0.67 | 0.60 | 0.58 |
| France | 20.0 | 6.7 | 99.9 | 0.51 | 0.73 | 0.28 | 0.51 |
| Germany | 22.6 | 13.2 | 89.5 | 0.58 | 1.00 | 0.44 | 0.68 |
| Greece | 38.5 | m.d. | 100.0 | 0.60 | 0.6 | 0.91 | 0.70 |
| Hungary | 28.9 | 22.6 | 100.0 | 0.43 | 0.92 | 0.22 | 0.52 |
| Ireland | 21.3 | 12.4 | 100.0 | 0.71 | 0.56 | 0.42 | 0.56 |
| Italy | 22.2 | 20.2 | 100.0 | 0.51 | 0.51 | 0.78 | 0.60 |
| Luxembourg | 9.6 | 6.5 | 99.5 | 0.72 | 0.72 | 0.51 | 0.65 |
| Netherlands | 37.1 | 8.0 | 98.7 | 0.57 | 0.51 | 0.38 | 0.49 |
| Poland | 30.6 | 25.6 | 99.3 | 0.33 | 0.77 | 0.33 | 0.48 |
| Portugal | 29.4 | 22.8 | 100.0 | 0.43 | 0.45 | 0.57 | 0.48 |
| Slovak Republic | 32.4 | 25.9 | 96.3 | 0.49 | 0.80 | 0.42 | 0.57 |
| Spain | 28.6 | 21.5 | 98.3 | 0.51 | 0.41 | 0.34 | 0.42 |
| Sweden | 18.5 | 16.3 | 100.0 | 0.61 | 0.35 | m.d. | 0.48 |
| UK | 13.1 | 11.76 | 100.0 | 0.57 | 0.39 | 0.26 | 0.41 |
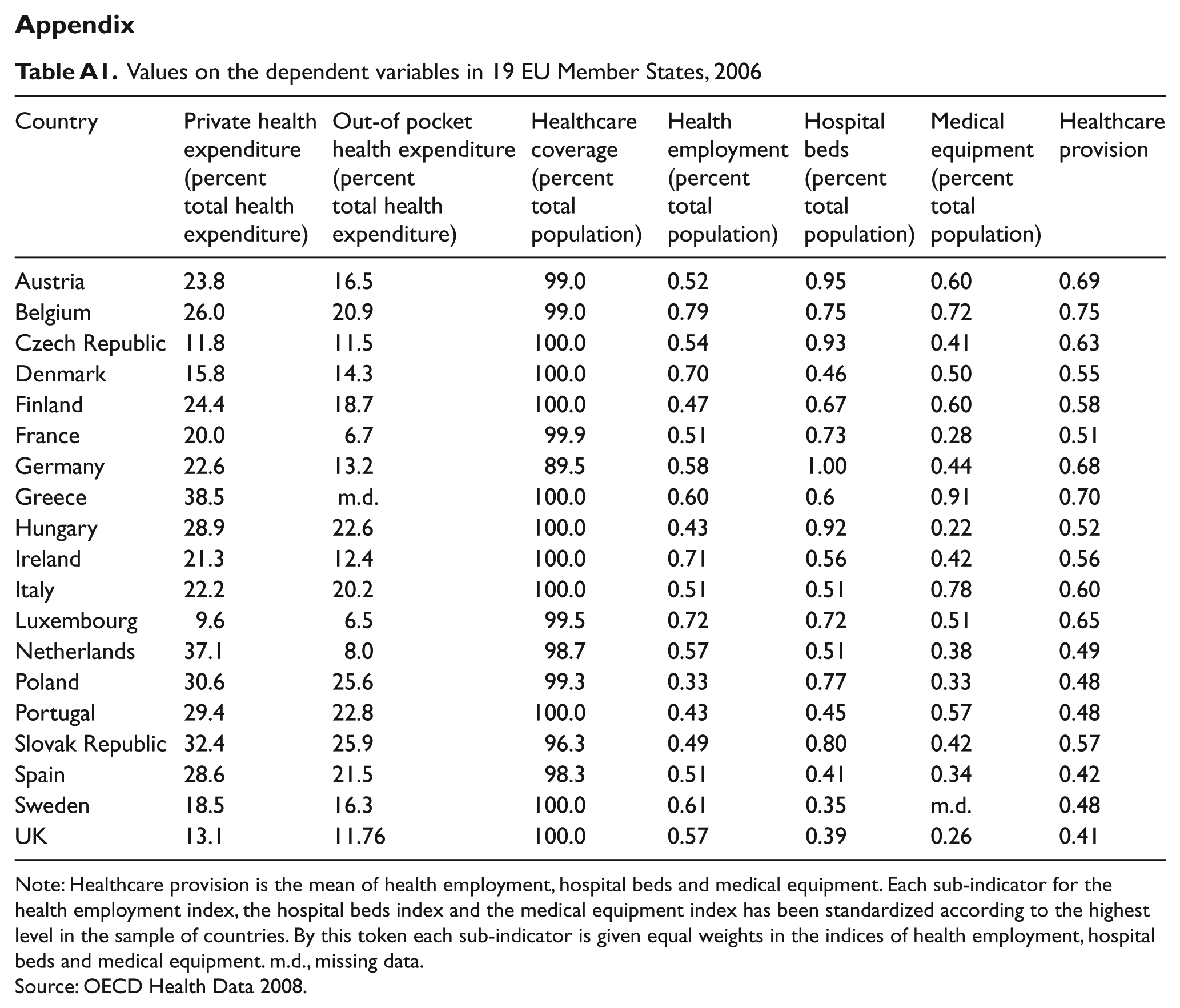
Note: Healthcare provision is the mean of health employment, hospital beds and medical equipment. Each sub-indicator for the health employment index, the hospital beds index and the medical equipment index has been standardized according to the highest level in the sample of countries. By this token each sub-indicator is given equal weights in the indices of health employment, hospital beds and medical equipment. m.d., missing data.
Source: OECD Health Data 2008.
Acknowledgements
We would like to thank Julia S. O’Connor at the University of Ulster, Joakim Palme at Uppsala University and Walter Korpi at Stockholm University for their valuable and insightful comments on earlier drafts. The advice of the editors and the anonymous referees are also gratefully acknowledged. This article has received funding from Riksbankens jubileumsfond and the Swedish Council for Working Life and Social Research.