
Abstract
Do personal experiences matter for public attitudes towards the role of the government? In the domain of healthcare, I argue that policies change the salience of personal experiences for government attitudes. Specifically, I expect that personal experiences matter less for government attitudes when healthcare is publicly financed, that is, when there is less emphasis on financing healthcare via market-based choices. Empirically, I link subjective and objective personal experiences from the International Social Survey Programme to macro-level policy indicators. The analysis provides strong support for the expectation and contributes to a growing body of literature interested in the underpinnings of government attitudes in a comparative perspective.
Public attitudes towards the welfare state is a cornerstone of policy developments in contemporary democracies. Accordingly, a large body of literature is interested in explaining citizens’ preferences towards the provision of welfare services (Andreß and Heien, 2001; Blekesaune and Quadagno, 2003; Kikuzawa et al., 2008; Lipsmeyer and Nordstrom, 2003). In the domain of healthcare, one of the most salient and popular domains of the welfare state, an understudied topic is whether people rely on their own personal experiences when forming their attitudes towards the role of the government (hereafter denoted as government attitudes).
The puzzle in the literature is understanding when personal experiences with healthcare policies matter for government attitudes. In brief, the research on whether healthcare policies matter has provided mixed evidence. In Norway, for example, Martinussen and Magnussen (2019) find that the existence of private health insurance is unrelated to government attitudes. In the United States, Barabas (2009) studies differences in two healthcare programmes and finds that different programmatic experiences matter for individualized healthcare coverage attitudes. These, and other studies reviewed below, illustrate that personal experiences might not translate into government attitudes in a homogeneous and universal manner.
In this article, I leverage insights from the policy feedback literature to provide one explanation that can, at least partially, explain why personal experiences only matter in some contexts. Building on research on the individual-level dynamics of government attitudes and the comparative policy feedback literature, I theorize how publicly financed healthcare crowds out the relevance of personal experiences. I thereby demonstrate how policies link personal experiences to government attitudes in a predictable manner.
The perspective outlined in this article shows that personal experiences are heterogeneously related to government attitudes across countries with different healthcare policies. Specifically, policies frame how the public should perceive an issue and, accordingly, whether personal experiences are relevant for their government attitudes. When healthcare is privately financed, people will be encouraged to consider different alternatives such as social insurance funds and private health insurance companies and thereby to a greater extent also rely on their individual experiences when forming their government attitudes. Countries that structure the financing of the healthcare system by public means, on the contrary, will make such considerations less salient and frame a logic of universalism that will make people’s own experiences disjointed from how they perceive the role of the government.
To examine this empirically, I combine country-level data on healthcare policies with individual-level survey data from 30 countries participating in the 2011 Health and Healthcare survey in the International Social Survey Programme (ISSP). The individual-level data provide multiple measures of personal experiences and the 30 countries provide substantial variation on how healthcare policies are financed, enabling a comparative test on how healthcare policies matter for citizens’ support for the government provision of welfare.
The results substantiate that people living in countries with privately financed healthcare rely on their personal experiences to a greater extent than people living in countries with publicly financed healthcare. These findings corroborate the policy feedback argument that policies structure how people link their personal experiences to political topics. In short, the findings show how policies can contribute substantially to our understanding of when personal experiences are salient for people’s government attitudes.
Personal experiences and government attitudes
There are profound reasons to expect that citizens rely on their own personal experiences when thinking about the welfare state. a personal assessment is, as Egan and Mullin (2012) argue, ‘directly accessible and requires little in the way of information search’ (p. 797). Put simply, personal assessments of welfare policies are crucial for citizens’ political attitudes (Calzada and del Pino, 2008; Gevers et al., 2000; van Oorschot and Meuleman, 2012). Previous research shows that personal experiences with political institutions are important drivers of various political outcomes (Calzada and del Pino, 2008; Kumlin, 2004, 2007; Kumlin and Rothstein, 2005; Soss, 1999; van Oorschot and Meuleman, 2012). Kumlin (2004), for example, explains that personal welfare state experiences ‘belong to a larger category of independent variables that are labelled government performance’ (p. 75).
Government performance matters for a series of outcomes, including how democratically satisfied citizens are (Sirovátka et al., 2019), and such perceptions of government performance can be negative, neutral or positive. In brief, on the basis of personal experiences, citizens gain direct insights into the performance of policies and form specific attitudes towards the role of the government.
Whether or not the government should be responsible for providing healthcare taps into a broader category of welfare state attitudes. Importantly, welfare attitudes are multidimensional in nature (Roosma et al., 2013), and people can have both good and negative evaluations of the actual performance of welfare policies that are unrelated to the role of the government (Roosma et al., 2014). Thus, the focus here will be on understanding how the nature of personal experiences matter for the role of the government.
A stable finding in the literature is that people are less likely to demand government responsibility to areas they are satisfied with (Calzada and del Pino, 2008; Gevers et al., 2000; van Oorschot and Meuleman, 2012). Specifically, people dissatisfied with welfare services see the current government involvement to be insufficient and prefer more involvement. People prioritize further government action to policies where they are dissatisfied, and the more dissatisfied people are, the more they expect the government to take responsibility. Accordingly, the expectation is that people dissatisfied with their healthcare experiences are more likely to prefer more government healthcare.
Kumlin and Rothstein (2005) show that personal experiences with healthcare policies, measured with perception of policy treatment, are significantly related to people’s level of interpersonal trust in Sweden. Bendz (2017) finds that different experiences with healthcare policies shape people’s attitudes towards privatization. In China, Im and Meng (2016) find that having health insurance matters for people’s attitudes towards government responsibility for the minimum standards of living but not for other issues such as healthcare.
Importantly, we do not know whether the relevance of personal experiences differs across countries and, if so, what might explain such cross-country differences. To better understand the relevance of personal experiences in a comparative perspective, I argue that the policy feedback literature can explain how and when personal experiences matter. In the next section, I outline how taking comparative policy differences into account can shed light on whether, and when, personal experiences are of greater importance for government attitudes.
Policy feedback and government attitudes
Policies are socially and culturally embedded institutions (Jæger, 2009; Larsen, 2008, 2019a), and to understand citizens’ government attitudes, a growing body of research has demonstrated how the structure of public policies matters for people’s preferences (Campbell, 2011, 2012; Fernandez and Jaime-Castillo, 2013; Fervers, 2019; Garritzmann, 2015; Larsen, 2019b; Mettler and Soss, 2004; Soss and Schram, 2007).
In contemporary welfare states, healthcare is one of the most salient policy areas (Hacker, 2004). As Jordan (2010) argues, people are likely to have numerous contacts with the healthcare sector across socioeconomic groups, making individuals ‘potentially more knowledgeable concerning the structure of the national healthcare system than any other sector of the welfare state’ (p. 870). In sum, healthcare policies are, while characterized by a large degree of complexity, visible and proximate (Beckfield et al., 2013).
Studies have examined how healthcare policies have implications for people’s government attitudes (Barabas, 2009; Campbell, 2011; Gevers et al., 2000; Jordan, 2010). Jordan (2010), for example, finds that the average support for national healthcare is higher in countries with hierarchically organized national healthcare systems compared to countries with more decentralized healthcare systems. In brief, hierarchically organized healthcare captures universal healthcare financed through general tax revenues, whereas decentralized healthcare builds on private health insurance and other means to ensure health coverage.
Recent studies have further examined how health expenditures directly shape attitudes towards the government responsibility for healthcare (Jordan, 2013; Missinne et al., 2013; Wendt et al., 2010). Wendt et al. (2010), for example, show that there is a high support for government responsibility in healthcare but substantial variation across Europe in the extent to which citizens are satisfied with their healthcare system. Related to this, studies have demonstrated that health expenditures matter for the overall satisfaction with the healthcare system (Popic and Schneider, 2018; Schneider and Popic, 2018). More generally, people have perceptions of the consequences of welfare policies that matter for how they perceive such policies (van Oorschot et al., 2012). This provides initial evidence for the interplay between assessments and attitudes, and thereby the importance of understanding how and when personal experiences with healthcare policies matter for government attitudes. However, while the studies provide evidence on the dynamics between healthcare policies and public opinion outcomes, they do not examine how healthcare policies shape how people’s personal experiences matter for their government attitudes.
The aim of the present study is to address the gap in the literature on how policies matter for the importance of such personal experiences. The focus in this setting will be on one of the most dominant properties that is expected to shape how citizens’ personal experiences matter for their government attitudes, namely, the financing (Cammett et al., 2015; Huber and Stephens, 2001; Jordan, 2013; Wendt et al., 2010).
The market plays a crucial role in relation to financing healthcare services (Moran, 2000), and while welfare policies can take a variety of different forms in different countries, the responsibility for the government to finance the healthcare system is a crucial policy design feature. As Cammett et al. (2015) argue, the share of private financing of healthcare is relatively obvious to individuals: private payments for health insurance premia, unofficial payments to doctors and hospitals in exchange for expedited care in nominally state-run systems, and out of pocket payments for medications and doctor visits are relatively visible to the end user. (p. 943)
Hence, the public share of the total healthcare expenditure serves as a defining feature of healthcare services (Cammett et al., 2015; Huber and Stephens, 2001; Jordan, 2013).
The macro-salience of healthcare policies: linking policies to experiences
People are limited in their abilities to consider more than a certain set of motivations at once. To explain what specific set of motivations people rely on in their government attitudes, and in particular whether personal experiences will be of importance, it is paramount to focus on the macro-salient nature of policies (Rohrschneider and Loveless, 2010). In short, policies emphasize some features with implications for the considerations people make. Rohrschneider and Loveless (2010) show, in the domain of the European Union, how the national contexts shape ‘the weight that citizens attach to economic and political considerations when evaluating the EU’ (p. 1032). Here, I apply these insights to the role of healthcare policies and thus incorporate the arguments into the policy feedback literature.
To explain the mechanism, these insights are inspired by framing theory (see Chong and Druckman, 2007), and they provide a theoretical framework explaining how specific policies affect the basis upon which citizens evaluate political objects. Two previous studies have utilized the concept of framing in relation to policy feedback effects on public opinion in the domain of healthcare. Jacobs and Mettler (2011), for example, use the concept of ‘structural framing’, and Zhu and Lipsmeyer (2015) argue that policies can frame individuals’ perceptions and thereby indirectly affect their preferences.
People’s government attitudes are the weighted sum of a series of evaluative beliefs. For personal experiences, there is a weight that shows the extent to which they relate to government attitudes. The policy, that is, the financing of healthcare, works as the salience weight, which structures the relevance of personal experiences. Thus, if the weight for a personal experience is zero, the personal experience will not matter for government attitudes, independent of how strong that personal experience is. In other words, a person might be completely dissatisfied with his or her experience with the healthcare system in a country, but whether this will be of relevance for the respondents’ government attitudes is a feature of the healthcare policy in place.
The design of a policy promotes certain logics that frame how people perceive and think about the policy. The argument presented here is that when a policy is financed via the market, such a policy will promote a logic where individual experiences are key to understanding people’s government attitudes. Specifically, the expectation is that privately financed healthcare policies will put an emphasis on the importance of personal experiences and the choice of alternatives on a market, for example, health insurance companies. Publicly financed healthcare will, on the contrary, promote a logic of universalism that will make the personal experience less entangled in selective services (Larsen, 2008).
Publicly financed healthcare builds on a logic of collective solidarity (Missinne et al., 2013: 234). When healthcare is financed by private means, this will foster questions related to the selection of services, that is, situations where people are more likely and even encouraged to rely on their level of satisfaction with their treatment. Accordingly, people’s personal experiences with the healthcare system will, in privately financed healthcare systems, be salient and thus shape their attitudes towards whether or not the government should provide healthcare services.
Data and method
The empirical strategy combines individual-level survey data with macro-level data on the share of public healthcare expenditures. The 30 countries included in the analysis are Australia, Belgium, Bulgaria, Chile, China, Croatia, Czech Republic, Denmark, Finland, France, Germany, Israel, Italy, Japan, South Korea, Lithuania, the Netherlands, Norway, Poland, Portugal, Russia, Slovakia, Slovenia, South Africa, Spain, Sweden, Switzerland, Turkey, the United Kingdom and the United States. The Philippines and Taiwan are not included in the analysis.
For the survey data, I rely on the Health and Healthcare survey data from the ISSP (ISSP Research Group, 2013). The ISSP is an annual programme of cross-national collaboration providing comparative survey data from widely different countries. The ISSP covers different topics from religion to gender roles, and the health topic was the focus in the 2011 round. The data were collected in the period from February 2011 to April 2013 (for further information on the data collection period and mode of interview in the individual countries in the ISSP, see Supplemental Appendix A).
For the outcome variable, respondents were asked whether they agree or disagree with the statement that governments should provide only limited healthcare services (for question wording on all variables, see Supplemental Appendix C). The variable is coded on a 5-point scale from ‘strongly disagree’ to ‘strongly agree’, where greater values indicate more positive attitudes towards the provision of healthcare services by the government. It is notable that the question wording is not similar to government attitudes in other ISSP surveys and, accordingly, it is not possible to examine how closely this measure correlates with other measures of government attitudes and thereby the degree of government involvement in healthcare.
For the main independent variables, that is, personal experiences with the healthcare system, the main challenge is to ensure measures of evaluations of personal experiences rather than generic evaluations of the healthcare system. Specifically, an overall satisfaction with the healthcare system reflects more than personal experiences (Busse, 2013; Busse et al., 2012). To accommodate this, I rely on subjective and objective measures of personal experiences.
For subjective personal experiences, respondents are asked to evaluate their most recent treatment by both the hospital and the doctor. For example, for the doctor evaluation, the question wording is as follows: ‘How satisfied or dissatisfied were you with the treatment you received when you last visited a doctor?’ Both of the subjective evaluations are measured on a 7-point scale (from ‘completely satisfied’ to ‘completely dissatisfied’), where greater values indicate a negative personal experience with the healthcare system.
For the objective personal experience, I use measures of whether the respondent was able to receive medical treatment during the past 12 months (from the date of the interview). Here, respondents are able to indicate that they did not receive medical treatment because the waiting list was too long, the treatment was not available in the area of the respondent, that they could not pay for it or that they could not take time off. I consider these reasons for not receiving medical treatment a negative personal experience. For example, previous research demonstrates that waiting times correlate significantly with hospital service satisfaction (Rönnerstrand and Oskarson, 2018).
In addition to the main individual-level variables of interest, I use a series of variables as covariates to take socio-demographic and socioeconomic characteristics of the respondent into account. First, I use information on gender, age, marital status, employment status and income (in quartiles to standardize across countries). Second, I use education, International Standard Classification of Occupations (ISCO-88) and healthcare insurance information to include as fixed effects in the models. For education, this is the highest completed education level. For ISCO-88, I use any category with more than 50 respondents in the full dataset and group the remaining categories into one (205 categories in total). For healthcare insurance, I control for nine categories from no health insurance to various combinations of public, private and employer/union-based health insurance (see Supplemental Appendix C for information on all variables).
To capture variation in healthcare policies, I leverage cross-national variation across the 30 countries in the financing of the healthcare system. Specifically, I use data on the public share of total health expenditure (public health expenditure (PHE)) for each country as used in the literature to measure salient policy differences in healthcare (Huber and Stephens, 2001; Jordan, 2013). While this measure does not fully capture all relevant characteristics of the public–private mix in healthcare, it is a reliable and valid measure of healthcare policies. Jordan (2013) uses this measure to capture differences between hierarchical and decentralized healthcare systems, and more specifically, this measure ‘distinguishes between highly centralized systems in which direct government spending dominates the healthcare market and decentralized systems where multiple payers including social insurance funds and private health insurance companies are more significant’ (p. 139).
The macro-level data stem from the World Development Indicators. To take into account that countries participate in the ISSP in different years and that respondents within the same country are not in all cases interviewed in the same year, I match each respondent to the relevant country-year PHE data. PHE ranges from 48.5 percent in the United States to 84.8 percent in Norway. The mean is 71.7 percent (standard deviation (SD) = 11.11) and the median is 72.2 percent (all values are available in Supplemental Appendix D).
Due to the limited number of countries, I rely on health expenditures as a percentage of gross domestic product (GDP) as the main macro-level covariate. This variable addresses the fact that a country might spend a lot on healthcare without saying anything meaningful on the public–private mix. In robustness tests, I further include hospital beds (per 1000 people), out-of-pocket healthcare expenditure as well as absolute (GDP) and relative (inequality, Gini) wealth.
I present the evidence both in the form of aggregate correlations between countries and in a series of hierarchical models with individuals nested within countries. Specifically, for the latter step, I estimate varying intercepts hierarchical models with cross-level interactions between personal experiences and PHE with the Level 1 variables group mean centred (Enders and Tofighi, 2007). All models include the covariates outlined above. To ensure an identical number of cases across the different models, I conducted multiple imputations with multivariate imputation by chained equations. All analyses were conducted in R 3.5.2.
Results
I begin by examining the degree to which citizens’ personal experiences are related to their government attitudes in the 30 countries. If the political context is irrelevant for the impact of personal experiences on government attitudes, we should find no variation across different countries in the extent to which personal experiences matter for government attitudes.
Figure 1 shows that there is substantial variation in the correlations between the 30 countries. First, the results replicate the main finding in the literature, that is, that people more dissatisfied in their personal experiences on average have stronger preferences for the government to provide healthcare. Second, in some countries, we find notable correlations between personal experiences and government attitudes (with correlations between close to .2), whereas in other countries we find no correlation between personal experiences and government attitudes. Third, the correlations are slightly stronger for the subjective evaluations (doctor evaluation and hospital evaluation) than the objective experience measure.
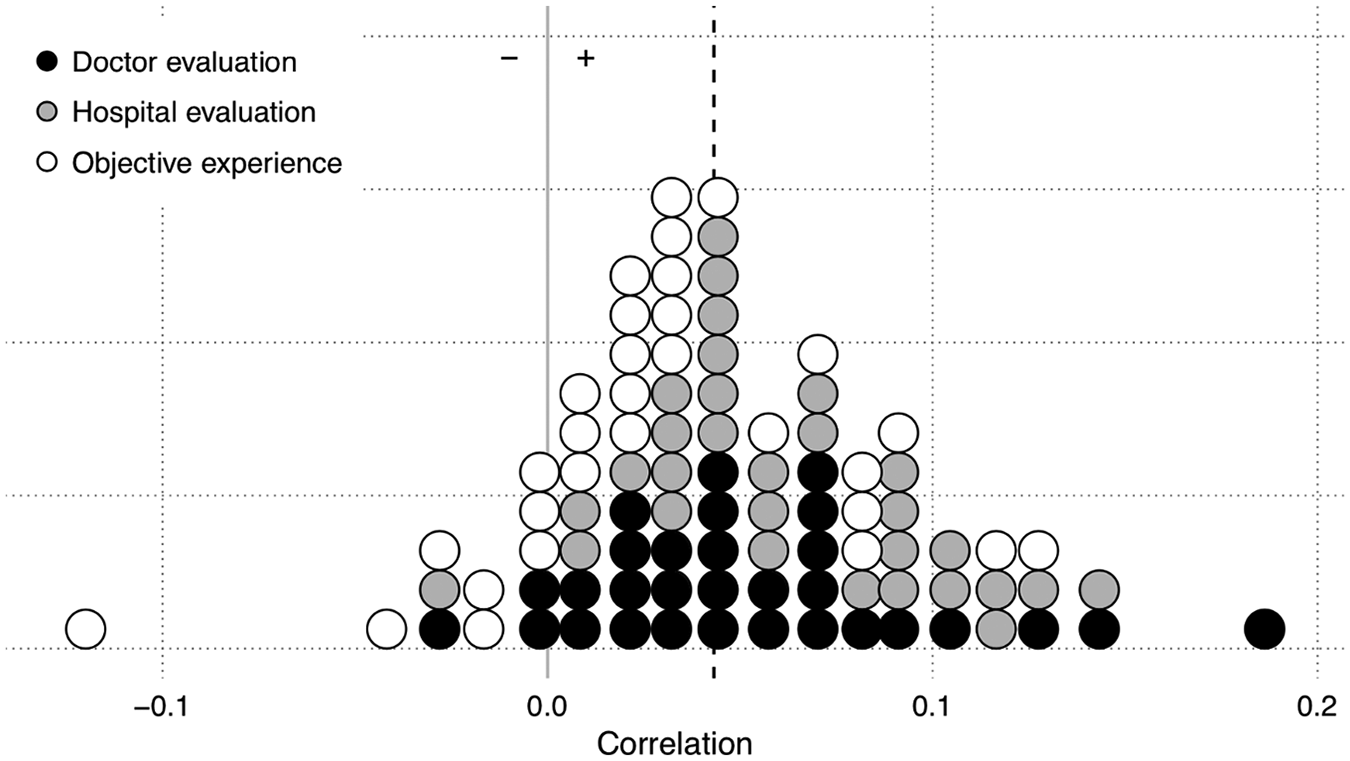
Correlations between personal experiences and government attitudes, 30 countries.
Overall, we find that there is substantial variation across countries and the next step is to shed light on whether the relevance of personal experiences varies in a systematic manner according to the healthcare system. Figure 2 shows the correlations between the personal experience measures and attitudes towards government healthcare at different levels of PHE. Across the three measures of personal experiences, we see that there is a stronger impact of personal experiences in countries with lower PHE. In most of the countries where healthcare is primarily financed by the government the correlations are statistically insignificant. For the United States, the correlations are around .1, whereas the countries with high PHE values, such as the Scandinavian countries, depict correlations not statistically or substantially different from zero.
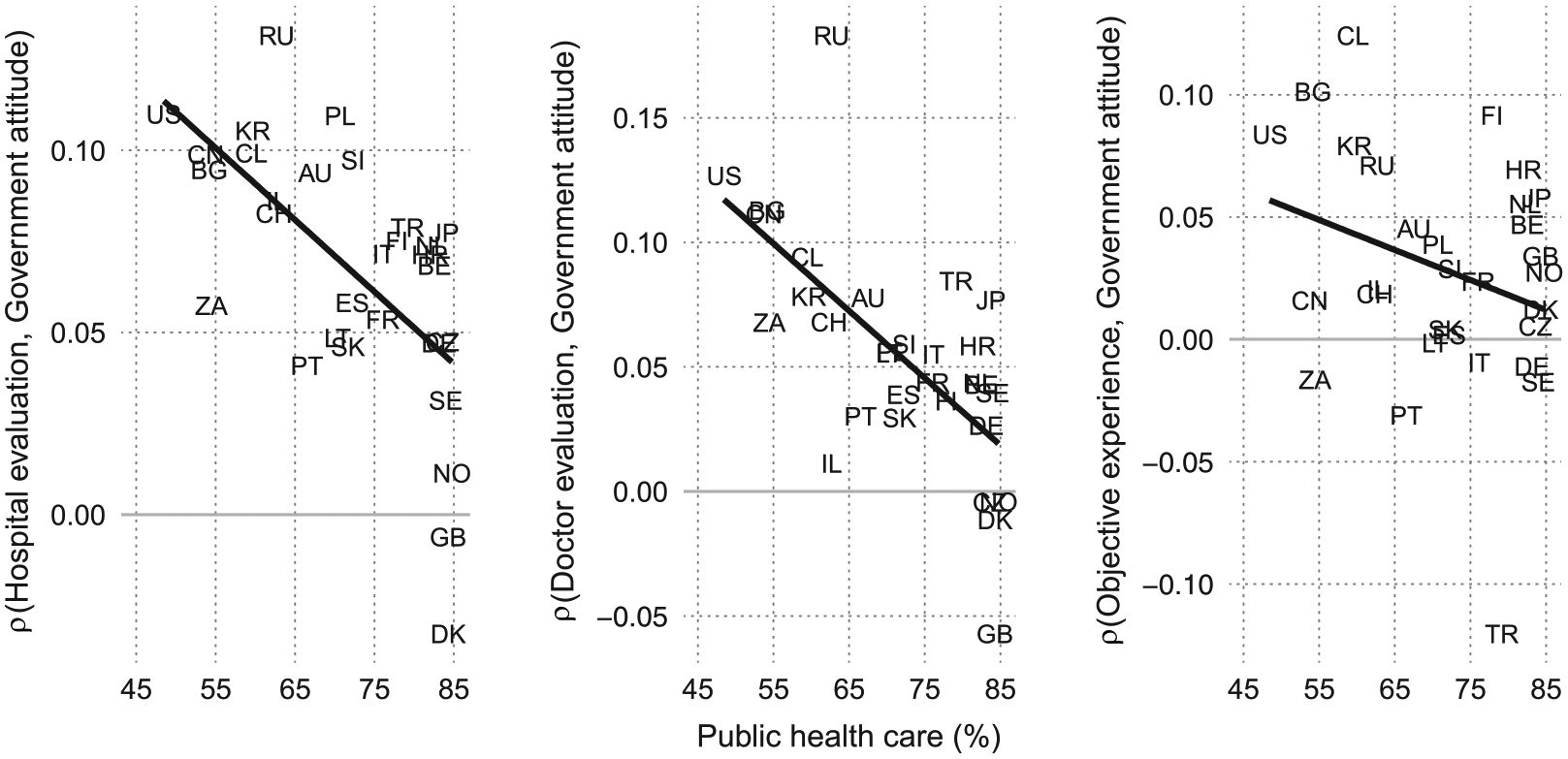
Personal experiences, public healthcare and government attitudes, macro-level evidence.
In sum, there is a negative trend in the correlations between personal experiences and government attitudes, indicating that this correlation is smaller in countries where the healthcare system is publicly funded. In other words, the trend suggests that there are systematic differences in the relation between personal healthcare evaluations and government attitudes in line with the theoretical expectations derived above.
To test this in a systematic manner, Table 1 shows four models. The first model provides a model with all the covariates to examine the direct effect of PHE on government attitudes. Here, we can see, in line with findings from the policy feedback literature, that people living in countries with greater PHE are more supportive of the government providing healthcare.
Personal experiences and government attitudes, hierarchical models.
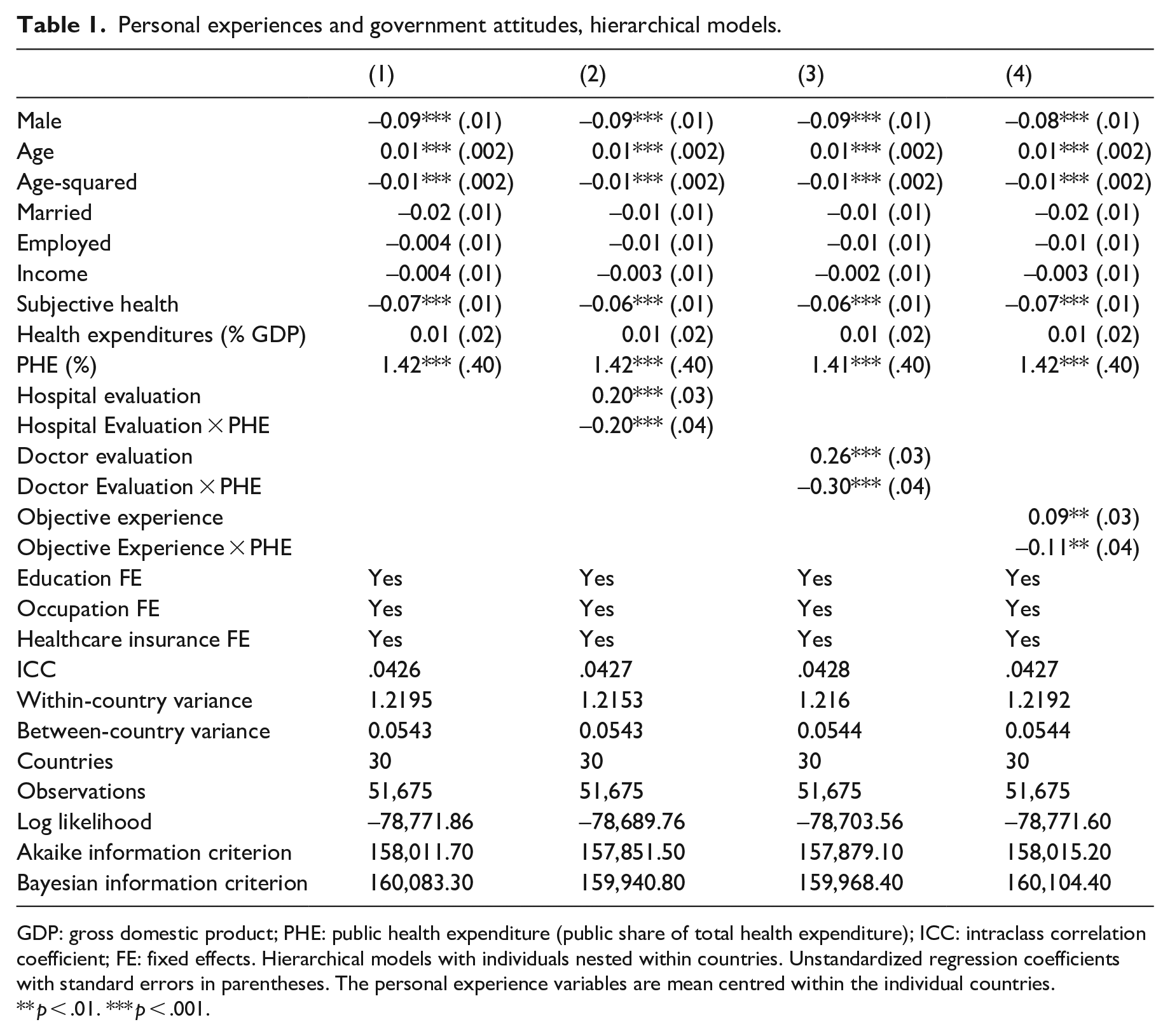
GDP: gross domestic product; PHE: public health expenditure (public share of total health expenditure); ICC: intraclass correlation coefficient; FE: fixed effects. Hierarchical models with individuals nested within countries. Unstandardized regression coefficients with standard errors in parentheses. The personal experience variables are mean centred within the individual countries.
** p < .01. *** p < .001.
Model 2 in Table 1 shows the results for government attitudes regressed on the cross-level interaction between hospital evaluations and PHE. Here, we see a significant cross-level interaction, indicating that the effect of the personal experience differs systematically conditional upon the public share of total health expenditure. In brief, personal experiences in the form of hospital evaluations matter less at greater values of PHE. Model 3 shows the same results for doctor evaluations. Here, results are identical to the hospital evaluations. Last, Model 4 shows the results for the objective experiences. While the results are statistically significant, as in Figure 2, they are not as strong as for the subjective experiences.
The models show, as expected from the theory above, that citizens’ personal experiences with the healthcare system are related to their attitudes towards government provision of healthcare to a significantly larger extent in countries where healthcare is financed by private means. To visually evaluate the effects of the personal experiences at different levels of healthcare expenditures, I calculated the marginal effects of each of the personal experience measures. Figure 3 shows the marginal effects that, substantially, mimic the findings in Figure 2, that is, that public healthcare crowds out the relevance of personal experiences in explaining government attitudes towards healthcare. Thus, the marginal effect shows that the impact of personal experiences is greater in countries with privately financed healthcare.
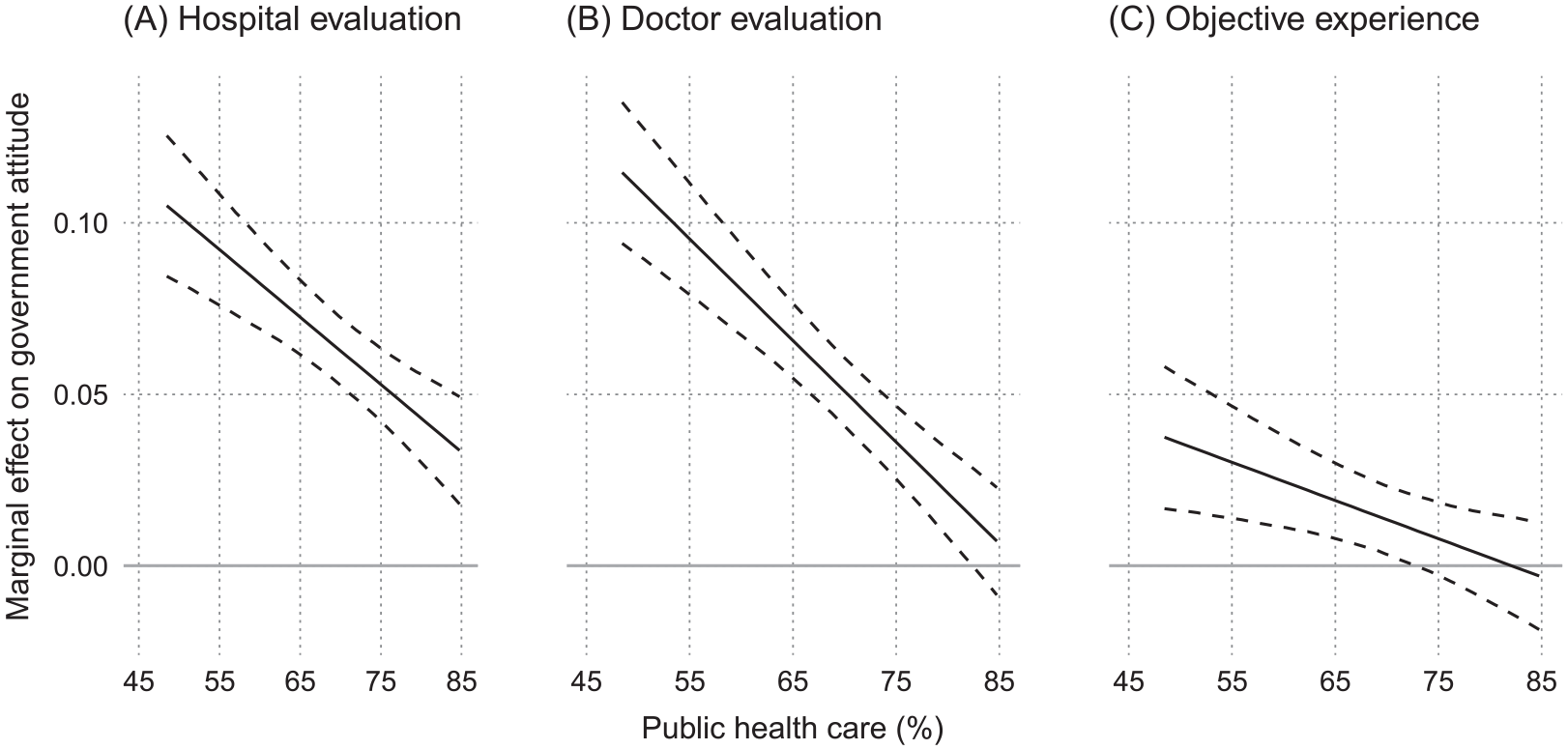
Marginal effects of personal experiences on government attitudes.
This lends support to the idea that how people’s experiences matter for their government attitudes is not consistent across policy contexts. Personal experiences with the healthcare system are significant predictors of government attitudes in a variety of countries, but mostly in countries where healthcare is financed by private means.
To further assess the robustness of the results, I estimated a series of additional models. First, the models were estimated with a series of extra macro-level covariates (available in Supplemental Appendix F). Second, the models were estimated with the removal of outliers and with the omission of individual countries (available in Supplemental Appendix G). Third, I replicated the models with the share of the population that are covered by public healthcare (available in Supplemental Appendix H). This policy measure shows the extent of general access provided by the public healthcare system (Bambra, 2005). Overall, the results from these tests do not affect the results or the interpretations presented here.
Discussion and concluding remarks
This article integrates insights from institutional and individual-level theories on political behaviour to study the joint role that healthcare policies and personal experiences play in shaping support for the government provision of healthcare. While citizens make assessments in relation to public policies that matter for their government attitudes, there is no reason to believe that the importance of such factors is homogeneous across different countries. On the contrary, the impact of personal experiences can be conditional upon specific policy features of salient policies.
While there is growing empirical evidence that the political context matters for the impact of individual-level characteristics on social welfare attitudes (e.g. Gingrich, 2014; Gingrich and Ansell, 2012), surprisingly limited attention has been devoted to empirically demonstrate how differences in the structure of policies matter for the importance of personal experiences. Zhu and Lipsmeyer’s (2015) study is a noteworthy exception as they study the impact of healthcare policies in shaping how people’s risk of unemployment matter for preferences towards government provision of healthcare. While the study provides important insights to how risk profiles matter for political attitudes, it cannot inform us on when and how personal experiences matter. This has been the primary goal of this study.
The argument tested in this article is that policies make specific features of the political environment salient with implications for how citizens’ personal experiences with healthcare policies are related to their government attitudes. More specifically, the findings are consistent with the expectation that policies condition how people align their personal experiences with their government attitudes.
In privately financed healthcare systems, features related to private choices and experiences are made salient at the macro level, and thus people will rely on such considerations and experiences when they form attitudes towards the role of the government. In a comparative perspective, this relation becomes weaker as the healthcare is financed by public means.
Overall, the findings presented here speak to the existing literature in different ways. First, it provides evidence on how healthcare policies matter for the impact of personal experiences on government attitudes in contemporary societies. Second, the theoretical and methodological implications are that we cannot solely understand people’s support towards welfare policies without taking the political context into account. In other words, an inherent limitation in looking at personal experiences in one context is that it is not sufficient to establish whether personal experiences might be of relevance or not outside this context.
Third, and most importantly, the findings contribute to a growing body of literature interested in policy feedback effects on political attitudes in a comparative perspective utilizing cross-national variation in public policies (Larsen, 2019b). More specifically, the findings stress the importance of integrating the political context with citizens’ experiences with policies. To fully understand the dynamics between public opinion and public policies, one needs to understand how existing policies frame how citizens link their personal experiences to concrete attitudes.
Future research on policy feedback effects should therefore devote close attention to how the policy context can shape the relevance of personal experiences. The correlations between 0 and .15 observed here in the different countries are representative for the effects normally observed in policy feedback studies on mass publics, and to explain the different effect sizes, the findings suggest that the political context is one important factor to take into account.
Beyond the direct implications, there are three noteworthy limitations in the present study that should guide future research as well. First, the empirical strategy does not allow for the study of time dynamics and is thus not a strong test of the causal arrows between personal experiences, government preferences and healthcare policies. While the results suggest that policies and personal experiences jointly shape government attitudes, the question of causality has yet to be answered. In sum, one should be cautious in drawing causal inferences based on the reported results.
Second, the countries studied here provide important variation in healthcare policies in different countries, but the extent to which the findings are generalizable to other countries not included in the analysis remains an important topic for future research. Most research on policy feedback dynamics has a Western bias in general and a US bias in particular, and while the study includes countries such as China and South Africa, additional evidence is needed in order to establish the external validity.
Third, as noted above, the measure of government attitudes is not identical to that available in other rounds of ISSP or other comparative surveys such as the European Social Survey and the World Values Survey. The advantage of the data used here is the data on personal experiences with healthcare policies, but replications with other measures tapping into other measures of government attitudes are encouraged. Furthermore, healthcare policies are complex in modern welfare states, and while focussing on the financing ensures the comparability across several different countries, the financing is only one measurable aspect related to the design of the healthcare system, and publicly funded healthcare can be used for private healthcare (Hacker, 2004; Jensen, 2011). Such dynamics might have implications for the experiences citizens have with the healthcare system and, consequently, their attitudes beyond what has been assessed here.
On a concluding note, as existing policies have implications for how the public perceive political issues, policies are important study objects if we are to understand basic political processes at the level of mass attitudes. The findings presented here emphasize that to fully understand the relevance of personal experiences for government attitudes, we need to take existing policy arrangements into account.
Supplemental Material
Larsen_supplementary – Supplemental material for Personal politics? Healthcare policies, personal experiences and government attitudes
Supplemental material, Larsen_supplementary for Personal politics? Healthcare policies, personal experiences and government attitudes by Erik Gahner Larsen in Journal of European Social Policy
Footnotes
Acknowledgements
For useful feedback on previous versions, I thank Paul Marx, Jane Gingrich, Christian Albrekt Larsen, Michael Baggesen Klitgaard, Robert Klemmensen, Christoph Nguyen, Simon F. Haeder, Peter Starke, Melike Wulfgramm, Paul Manna, Jochen Rehmert as well as the editor and anonymous reviewers.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.