
Abstract
Tailored and comprehensive psychotherapy options have been requested by individuals experiencing negative premenstrual change (PMC) – inclusive of premenstrual syndrome (PMS), premenstrual dysphoric disorder (PMDD) and premenstrual exacerbation (PME). Whilst some studies present psychotherapy programmes or interventions for PMC, few provide detailed descriptions of the session contents or the rationale behind them. Only a small number of studies have explored participants’ acceptability of these programmes, and none have been codesigned with individuals who experience PMC themselves. This paper addresses the need for practice-led research by outlining the development process and session content of a codesigned psychotherapy programme tailored to PMC: a person-centred programme involving internal family systems (IFS) aspects and arts-based therapeutic activities. A case study using a single participant who completed the programme is used to illustrate the sessions, and the rationale behind them is discussed.
Keywords
Introduction
Premenstrual change (PMC) refers to the cognitive, affective and physical changes experienced just before menstruation (the late luteal phase of the menstrual cycle). Many who experience significant disruption and distress related to PMC express a need for tailored and comprehensive psychotherapy options. Many of the extant interventions are not codesigned with those who experience PMC and are not adequately grounded in their actual experiences and needs. The work we present in this article was motivated by the need for practice-led, 1 codesigned psychotherapy for PMC and documentation of design and application so that such programmes can be translated into practice.
In this article, we present a novel codesigned psychotherapy programme grounded in feminist principles and tailored to PMC, using the case study of one of the participants for illustration. We use the case study to illustrate the programme design and positive outcomes for the participant. Beyond highlighting these individual outcomes, the case underscores the importance of collaborative and practice-led research in refining psychotherapy interventions for PMC, particularly, centring client's embodied knowledge and experiences in shaping such interventions. In doing so, the paper contributes to feminist psychology by demonstrating how psychotherapeutic support for PMC can move beyond pathologising frameworks and instead privilege participants’ own meanings, expertise and lived experiences. The following sections outline the programme's development through codesign, describe its theoretical and therapeutic foundations and illustrate its application through a detailed case example.
PMC
PMC – often also diagnosed as premenstrual syndrome (PMS), premenstrual dysphoric disorder (PMDD) or premenstrual exacerbation (PME) – refers to the cognitive, affective and physical changes experienced by people with female physiology during the late luteal phase of the menstrual cycle. Mood changes, anxiety, anger, depression, difficulties in concentration, fatigue, sleep disturbance, breast tenderness and bloating are common, affecting up to 98% of menstruating women/people worldwide (Direkvand-Moghadam et al., 2014; Rapkin & Winer, 2009). Within this group, 8% experience more severe changes that significantly impact daily life and are often diagnosed as PMDD (Hantsoo & Epperson, 2015).
Qualitative accounts of individuals who have experienced PMC capture narratives of desperation and distress. For example, from the pilot study of this programme of research, one participant said: ‘I want to be able to know that going into my next cycle, I’m going to come out alive’ (Buys, 2024, p. 296). The impact of changes diagnosed as PMDD specifically has been accounted for in the workplace (Hardy & Hardie, 2017; Hardy & Hunter, 2021; Loukzadeh et al., 2024), relationships and the home (D. Brown et al., 2024; Tutty et al., 2021; Ussher & Perz, 2011, 2013) and in experiences of seeking healthcare (Buys, 2024; Chan et al., 2023; Osborn et al., 2020). Across contexts, however, many report suffering in silence and feeling alone in their journey to find appropriate support (D. Brown et al., 2024; Chan et al., 2023; Habib et al., 2024; Osborn et al., 2020; Sveinsdottir et al., 2002).
Addressing this need, research on psychotherapy options for PMC is evolving. A recent scoping review (Buys, 2025b) identified 34 studies published in the past 25 years that investigate a psychotherapy programme or intervention for PMC. Of these, only six explored participant acceptability of the programme (Hunter et al., 2002a, 2002b; Mahmoodi et al., 2023; Shareh et al., 2022; Ussher & Perz, 2006, 2017), and none were codesigned taking into account the preferences of the participants or community. These findings suggest a critical gap in person-centred and feminist care (Burdett & Inman, 2022; Smith et al., 2022). The level of detail provided on the programme contents also varies. Only two studies discussed the programme contents in significant detail, offering comprehensive session structures (Citil & Canbay, 2024; Hojjati Najafabadi et al., 2023), and two provided significant details of the sessions elsewhere (Hunter et al., 2002a, 2002b, as cited in Ussher et al., 2002; Weise et al., 2019, as cited in Janda et al., 2015). 2 The limited number of studies that offer codesign and sufficient programme transparency highlights important questions around how closely existing approaches reflect lived experiences of PMC and how feasible they are to implement in real-world clinical contexts. Practice-led, codesigned research that can be translated into the clinical setting with ease is therefore essential. This forms the rationale for our PMC psychotherapy programme that took a person-centred approach and used internal family systems (IFS) aspects and arts-based therapeutic activities such as body mapping. We discuss each of these components in turn below.
A Codesigned Psychotherapy Programme for PMC: Using IFS and Arts-Based Therapy
Codesign is a collaborative approach that involves all relevant stakeholders in designing and implementing solutions based on the principle of designing ‘with’ rather than ‘for’ the people who will use, deliver or engage with a service or product (Vargas et al., 2022). In the healthcare context particularly, codesign empowers users to shape the services and interventions that impact their lives through the sharing of power and decision-making (Slattery et al., 2020). This approach informed the development of the psychotherapy programme for PMC, which I (Megan) designed, run and evaluated as part of a broader research project.
The project employed an iterative design with multiple data collection methods to codesign and evaluate a psychotherapy programme. I (Megan) used an open-ended survey and one-to-one interviews to gather participants’ experiences and preferences to tailor the programme to their needs (Buys, 2025a). The data analysis indicated that participants wanted specific therapist competencies, namely validating, knowledgeable about PMC and ability to develop a strong therapeutic relationship. They sought therapy focused on self-compassion, integration and gaining control delivered through IFS and arts-based therapeutic activities. Participants were not asked to choose from a predetermined list of psychotherapeutic modalities; rather, they described the qualities, therapeutic goals and activities they wanted included in a PMC-specific intervention. The selection of IFS and arts-based therapeutic activities was informed by these preferences, as well as the alignment between participants’ experiences and the theoretical underpinnings of these approaches. In addition, the programme design itself was informed by participants’ input, ensuring that the structure, session content and activities reflected the priorities and experiences they had identified.
Drawing on these insights, I designed the psychotherapy programme under the supervision of the second and third authors, who offered academic oversight, manuscript review and ongoing reflexive discussion throughout the research process. As the lead researcher and developer of the programme, I engaged in ongoing reflexive practice throughout the study to consider how my social positioning, clinical background and personal experiences shaped the research process and interpretation of findings. As a white, Western, educated, middle-class woman with a family history of gendered inequality and violence, I recognised that I approached participants’ accounts with particular sensitivity to power, gender, embodiment and relational dynamics. My training in integrative, social-justice-informed psychotherapy also influenced how I developed the therapeutic programme, conceptualised distress and understood participants’ narratives. These influences shaped how I engaged with the topic by attending to experiences that may be overlooked, minimised or medicalised; how I engaged with participants by prioritising collaboration, curiosity and respect for their lived/living experience and expertise; and how I interpreted findings by viewing knowledge as co-constructed rather than objective or value-neutral.
The programme consisted of five therapy sessions, spaced fortnightly, and one introductory session where the programme and broader research project were outlined and the participants were able to share their personal experiences of PMC. All sessions were in an in-person, one-to-one format between the client and the clinician, all 60 minutes in length. The number and spacing of sessions reflect prior studies conducted on psychotherapy options for PMC (Busse et al., 2008; Han et al., 2019; Kleinstauber et al., 2012; Lustyk et al., 2009) and were also a codesigned aspect of the broader research project. The programme used IFS and arts-based approaches, specifically, body and parts mapping, as explained below. (The full psychotherapy programme outline is provided as supplemental material.)
IFS Therapy
IFS therapy was adopted based on participant preference for a nonpathologising approach that promoted self-compassion, self-understanding and integration. IFS was also selected because it offers a useful conceptual framework for understanding common experiences reported in PMC, including internal conflict, experiences of a ‘split self’, self-policing and self-silencing (Chrisler et al., 2014; Han et al., 2019; Shareh et al., 2022; Sweezy, 2023; Ussher, 2004a). Rather than viewing distressing thoughts, emotions or behaviours as symptoms to be eliminated, IFS conceptualises them as understandable responses that serve protective functions within an individual's internal system (Schwartz & Sweezy, 2020).
In this modality, the psyche is viewed as comprising distinct, sometimes conflicting ‘parts’ –each with its own perspectives, desires and roles – that interact dynamically within the individual. Some parts may take on extreme or rigid roles that create conflict within the internal system. The Self is viewed as the undamaged, innate centre of wisdom, compassion and leadership that exists beneath these parts, experienced as an inherent inner state of clarity, compassion and curiosity. Therapeutic work proceeds from a nonpathologising and trauma-informed lens, with the motto ‘all parts are welcome’. It involves facilitating ‘self-leadership’, understanding, integrating and harmonising the different parts. The therapist builds upon the strengths of the Self as a way of engaging with all parts by, for example, fostering self-compassion or curiosity (Schwartz & Sweezy, 2020, p. 59). Ultimately, the therapist assists the client in identifying and communicating with these different parts to enhance understanding of how they relate and to create more adaptive parts that support the system (Schwartz & Sweezy, 2020).
Arts-Based Therapy, Body Mapping and Parts Mapping
Alongside IFS, the participants expressed a preference for art-based approaches. Art therapy is an expressive modality that uses art-making as a means of expression and communication to explore and address psychological and social challenges (Malchiodi, 2007). Art therapists facilitate the creation of art that is personally meaningful and relevant to their client's therapeutic goals, using a variety of media depending on the client's preferences and needs. We used two arts-based therapeutic activities alongside IFS, namely body mapping (De Jager et al., 2016; Dew et al., 2018; Ryan et al., 2022) and parts mapping (Neubauer, 2024; Schwartz, 2023; Schwartz & Sweezy, 2020). Parts mapping is (as discussed further below) a natural extension of IFS, but we chose body mapping as the primary arts-based activity due to prior use in research (Ryan et al., 2021, 2022) in which the technique was shown to support emotional expression and meaning-making, as well as its alignment with the embodied nature of PMC (Ussher & Perz, 2020b).
Body mapping comprises (a) a visual, life-sized body map, (b) a key to interpret the symbols on the map and (c) a first-person narrative detailing the body map (Gastaldo et al., 2012). Body maps can be completed in individual or group research and in community and/or therapeutic spaces (De Jager et al., 2016). The body mapping activity was informed by Gastaldo et al.’s (2012) facilitation guide. Specifically, we retained the guide's emphasis on creating a life-sized body outline; the use of symbols, imagery, colours and text to represent lived experience; the development of a legend/key to support interpretation; and the generation of a narrative account accompanying the map. Our participants completed these in individual sessions with me (Megan) in which they created life-sized representations of their bodies and overlaid these with personal narratives and symbolic imagery. Each therapy session was audio-recorded so that personal narratives and meanings were captured. The technique originated in postcolonial feminist research as an arts-based research tool to foreground the embodied experiences of marginalised communities (De Jager et al., 2016). In our programme, body mapping provided participants with a structured, creative means of externalising and exploring embodied experiences related to PMC.
Parts mapping is a foundational intervention in IFS, designed to help clients visually or conceptually organise their internal system of ‘parts’ (Neubauer, 2024; Schwartz, 2023). This process identifies the roles, relationships and interactions among various parts, offering a structured way to uncover internal dynamics and patterns (Schwartz, 2023; Schwartz & Sweezy, 2020). Therapists and clients often use creative approaches – such as diagrams, lists or drawings – to help make the client's internal system clearer and more accessible, and as a tool to foster curiosity about one's own experiences (Schwartz, 2023). In our programme, parts mapping was completed on large pieces of paper, again, with all the sessions audio-recorded to capture personal meanings.
Case Study
To demonstrate the application of the elements discussed above, we use the case study of a participant whom we call ‘Elenor’ in this article. This material is necessarily descriptive and illustrative and not intended to represent a formal qualitative analysis. We selected Elenor's case because she was the first participant to complete all sessions. Elenor (she/her) is a 25-year-old White Australian woman who describes her sexuality as queer, is in an intimate relationship, living with her partner and does not have children. She was diagnosed with PMDD by her general practitioner in 2025; however, now uses PMC to describe her experiences as a result of attending the therapy programme. When asked to what extent she found PMC distressing, she rated her experience as 8/10, with a 3/10 ability to cope. Elenor experiences premenstrual changes 7 to 15 days before beginning menstruation and describes her premenstrual experience as involving full-body physical pain and ‘intense bloating, pimples on the face, irritability, explosive rage, mood changes, depressive, teary [and] extra sensitive’. Her social relationships and self-care routines are impacted by this. We provide necessarily truncated descriptions of each session in what follows. A fuller, richer account of the therapeutic process, including extended dialogue and clinical detail, is provided in the Appendix.
Session 1: Authoring PMC
The first session focused on building a genuine connection and rapport with the client, providing a solid foundation for the therapeutic process. The psychotherapy programme and the modalities to be used, including IFS and arts-based therapeutic activities, were introduced. A biopsychosocial model was presented to help the client understand the multifaceted nature of PMC. The client was invited to share their personal story and experiences with PMC in a supportive and nonjudgemental space. Arts-based methods were introduced as tools for expressing thoughts, emotions or experiences that may be difficult to put into words while also encouraging new insights. Together, the client and therapist explored the experience of PMC visually through a body map, which supported self-reflection (Figure 1).

Body map of Elenor's experience of herself, her body and PMC (name redacted) from Session 1.
After discussing the programme and her typical premenstrual experiences, including reaching a ‘peak’ of distress where she would end up ‘on the floor of the shower crying’ following conflict with her partner, I invited her to create a body map of her premenstrual experience. Although initially hesitant, Elenor identified an anxious part she called ‘Fat Elenor’, who simply wanted to be acknowledged before beginning. As she worked on the map, she described feeling ‘dark’, tearful, puffy, inflamed and bloated during the luteal phase. Reflecting further, she reconsidered the name of the anxious part, renaming it ‘Fatphobic Elenor’ to capture the internalised judgements that emerged more strongly premenstrually. She represented this part by circling her lower stomach in black while describing self-critical messages about being ‘fat’, ‘big’, ‘puffy’ and ‘lazy’.
As the map developed, Elenor drew a yellow and orange ‘Core Sun’ in the centre of her body, representing her ‘authentic self’, and added a range of other parts, including Fatphobic, Judgmental and Lazy Elenor below the Sun; and Authentic, Spiritual and Embodied Elenor above it. She described a dynamic tension between these parts, explaining that during the luteal phase ‘the flood takes over the Sun’, leaving her disconnected from her Core. Together, we identified a ‘dam wall’ of resistance preventing her Core from connecting with the more vulnerable lower parts of her body. She also drew a moon shape outside her body to represent her sense of disconnection from her menstrual cycle. At the end of the session, Elenor reflected that although the process had initially felt confronting, ‘it feels like me … I feel like I just unlocked something’. The introduction of a Core ‘Sun’ alongside conflicting parts illustrated the programme's foundational assumption that multiple internal experiences can coexist, and that distressing states are meaningfully connected to, rather than separate from, the Self.
Session 2: Meeting Parts
The second session introduced an IFS-informed approach, offering a new lens through which to understand and work with PMC. The client was guided to conceptualise PMC as involving parts of their internal system, helping them to externalise and engage with these experiences in a compassionate way. Together, the therapist and client explored and mapped these parts through a visual representation, including their relationship to the Self (Figure 2). This process supported the development of a collaborative conceptualisation of PMC from an IFS perspective, laying the groundwork for deeper therapeutic exploration in subsequent sessions.

Parts map (with name removed) from Sessions 2 and 3.
Reflecting on the previous week, Elenor shared that she had experienced a premenstrual ‘peak’ but had responded differently by giving herself permission to let the experience ‘take over’ and asking her partner for validation rather than remaining silent. After discussing some apprehension about the session, we agreed to finish with a grounding exercise and began creating a parts map, using her body map from Session 1 as a reference. Elenor immediately drew the ‘Core Sun’ from the previous session in the centre of the page, representing Self, and surrounded it with words such as ‘Warm’, ‘Embodied’, ‘Whole’, ‘Centred’, ‘Fun’, ‘Play’, ‘Spirituality’ and ‘Values’.
As she mapped her internal system, Elenor identified ‘Brain Fog’ as a prominent part, represented by a grey cloud. Exploring its role led to the emergence of additional parts, including ‘Control’, which was frustrated with Brain Fog and trying to keep everything organised; and ‘Exhausted’, a part she recognised was often ignored. As she added these parts, Elenor commented that ‘there's a bit more room’, describing a sense of relief in seeing them externalised. Further exploration identified ‘Judgmental’, ‘Anxious’ and ‘Insecurity’ (previously, ‘Fatphobic’) parts, with Judgmental positioned as critical of the others. Revisiting the ‘Resistance’ identified in Session 1 revealed it to be a panicked protective part guarding a more vulnerable aspect of herself, leading to the emergence of a distinct ‘Vulnerable’ part. At the end of the session, Elenor reflected that the completed map ‘feels nicer’ and gave her ‘a sense of control’. She also repositioned the Moon from her first body map beside the Core Sun, explaining that although she wanted it to be touching it, it remained ‘a little further away’, symbolising a growing but incomplete connection with her menstrual cycle.
Session 3: Meeting the System
The third session focused on deepening the IFS-informed approach. Building on the parts map from the previous session, the client explored the relationships between their parts and how they interacted. Table 1 outlines the relationship between Elenor's parts and Self. PMC experiences were framed as valid and protective, fostering greater self-compassion. External influences on PMC were also explored, providing a broader context for the client's experiences and insights into how these factors interact with their internal system.
Relationships between Elenor's Parts and Self.
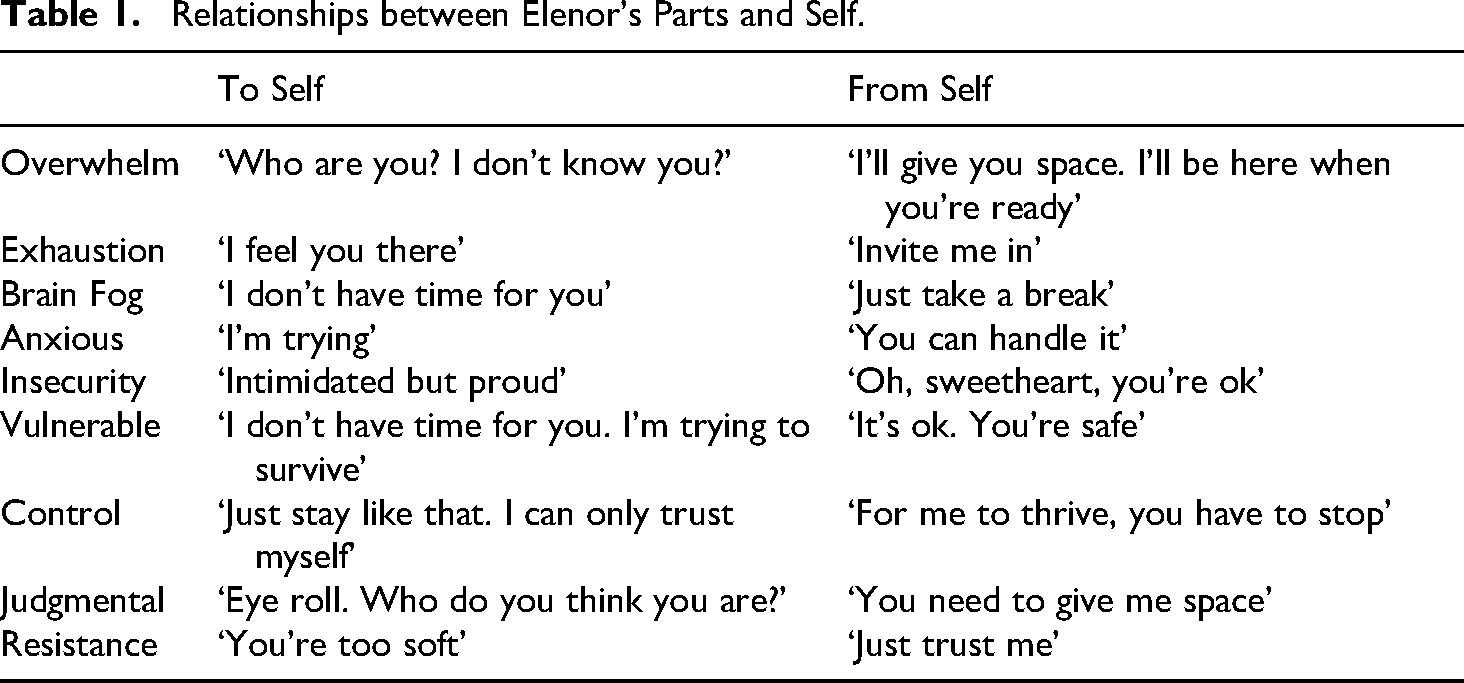
Revisiting her parts map, Elenor expanded the descriptions of several parts and reflected on the strong connection between her Anxious and Control parts. She described how feelings of being out of control during difficult premenstrual experiences could trigger both anxiety and self-blame, noting that ‘maybe that goes into Judgmental a little bit as well’. To further explore these relationships, Elenor drew arrows between parts, including a message from Control to Anxious that read, ‘Just stop it’. We then mapped how each part related to her Core Self and how Self related back to each part, creating a fuller picture of her internal system. Together, we identified three broad groupings within her system: control-oriented parts (Control, Judgmental, Resistance), vulnerable parts (Vulnerable, Insecurity, Anxious) and overwhelmed parts (Overwhelm, Exhausted, Brain Fog). Through discussion, Elenor recognised a recurring cycle in which the control parts worked hard to protect Vulnerable, but in doing so often contributed to Overwhelm and Exhaustion.
Toward the end of the session, the Moon was further reconceptualised as representing cyclical change rather than disruption. Elenor reflected that her Judgmental part still struggled to accept the Moon and what it represented about her menstrual cycle, while another part recognised that ‘the point of the Moon’ is that it moves through phases.
Session 4: Speaking With Parts
The fourth session continued the IFS-informed approach, focusing on fostering dialogue with the client's parts through a guided meditation process. The client was guided to connect with and understand her different parts, particularly those associated with her PMC experience. Together, we explored the roles and needs of these parts, gaining insight into their dynamics and underlying motivations. Through this process, the session encouraged self-compassion by fostering a deeper understanding of each part and began the work of integrating these parts to create a more harmonious internal system.
The guided meditation began with Elenor connecting with what she called her Core, described as warm, centred, curious and embodied. From this grounded place, Elenor identified Insecurity as the part most present, describing Insecurity as shy, lost and uncomfortable, yet noticed that she felt sympathy rather than criticism toward it. As the dialogue continued, Anxious and Vulnerable parts also emerged. Although initially overwhelmed by having these parts present, Elenor was able to reconnect with her Core, describing it as having a reassuring ‘mum’ quality that ‘has got it’. From this place of self-energy, she invited the parts into a supportive circle, offering them comfort, inclusion and reassurance. She described both her parts and herself as feeling ‘peaceful’, and concluded the session reflecting on the experience as something entirely new, characterised by ‘a huge sense of relief’ and a feeling of ‘transcendence’ associated with self-leadership.
Session 5: Embracing Parts and Reauthoring PMC
The fifth session provided an opportunity for the client to reflect on her journey and the evolving understanding of her PMC experience through the creation of a new body map (Figure 3) to reflect shifts in her perspective. The original body map was then revisited and laid side by side to the new map, where each were discussed. The session explored any changes in the client's narrative of PMC, highlighting progress and new insights. Finally, the focus shifted to integrating therapy insights into the client's daily life, with a discussion on strategies for ongoing self-support and postprogramme resources to maintain and build on therapeutic outcomes.

Body map of Elenor's experience of herself, her body and PMC from Session 5.
Elenore began our session by describing a significant shift in how she understood her menstrual cycle, explaining that during the luteal phase she no longer felt separate from her Core. To integrate her experiences across the programme, Elenor created a second body map. At its centre, she drew a large yellow and orange spiral representing her Core, with radiating lines extending throughout her body. Unlike her original map, where the Core had felt blocked and overwhelmed, she described this new image as representing flow, connection and openness: ‘It doesn’t feel like this [the Core] is stopped anymore … There's more flow’. Previously split-off parts were now represented as integrated within the body. The Moon, initially external, was depicted as connected to the Core, reflecting a reauthored understanding of PMC as cyclical and meaningful: ‘I’m not separate from her [Core]. I’m just waxing or waning’.
Comparing the new map with the original, Elenor noted that her Core was much larger, the previous barrier between the upper and lower parts of her body had disappeared and her parts now felt ‘at home’ within her. Reflecting on the Moon's progression across the three maps (from outside her body to beside her Core to connected with it), she concluded, ‘They know each other a bit better now. They’re a bit closer’. This progression illustrates the programme's overarching aim: supporting movement from fragmentation and self-pathologising toward integration, self-leadership and an agentic relationship with premenstrual experience.
Discussion
Research exploring a psychotherapy programme or intervention for PMC is limited, with few studies detailing the contents of the sessions and rationale in depth (Janda et al., 2015; Kues et al., 2014; Ussher et al., 2002), despite a need for practice-led research on novel and tailored approaches to PMC (Chan et al., 2023; Funnell et al., 2024a, 2024b; Habib et al., 2024; Hantsoo et al., 2022). The present paper addressed this gap by detailing the sessions of a codesigned psychotherapy programme tailored to PMC. The programme was integrative and collaborative in nature, drawing from a range of psychotherapy modalities aligned with a feminist framework and the needs identified by the participants in the codesign process. Modalities included IFS, arts-based therapeutic activities and feminist elements, each sharing similar philosophies: that truth is not objective but rather multiple truths may coexist at once; that reality is constructed through language and social discourse, and also through visual and embodied means; and that the therapist is not an external expert, with the client–therapist relationship being one of cocreation rather than hierarchy (Brown, 2018; De Jager et al., 2016; Malchiodi, 2007; Schwartz & Sweezy, 2020; White & Epston, 1990). The aim of supporting participants in the process of ‘moving from an abject to an agentic subject position, without positioning her as needing to be managed, or her body as an unruly vessel that needs to be contained by experts’ (Ussher & Perz, 2020a, p. 225) was upheld throughout the present programme. The following discussion expands upon the programme's rationale and details the programme's main tenets.
A Person-Centred, Feminist Approach to Therapy
Taking time to hear the client's experience without interruption or judgement and viewing the client as the expert of their own experience are central to person-first, feminist therapy (Ussher, 2006), shown predominantly in the first session and then continued throughout the programme. Ussher (2008), in an evaluation of a ‘woman-centered psychological intervention’ – a narrative therapy-informed cognitive-behavioural therapy (CBT) programme for premenstrual symptoms – outlines that hearing and validating the clients’ stories in a nonjudgmental way was reported by participants to be one of the most positive aspects of the intervention, allowing clients to feel ‘understood, rather than pathologised and dismissed’ (p. 38). Discussing this necessary aspect of support for PMC further, Ussher (2004b), notes: ‘For clinicians, the most important thing is to validate the woman's feelings, to be empathic and understanding, to reassure her that she is not unusual or abnormal, and to avoid any notion of blame’ (p. 104). Giving ‘“ownership” to women over their PMS, is therefore essential’, reports Kancheva Landolt and Ivanov (2021, p. 1289) in a review on CBT options for PMC. Hearing the client's narrative of PMC solidifies this suggestion, alongside developing a collaborative conceptualisation of PMC in the following sessions of the programme, where the client is valued as an expert of their own experience (White & Epston, 1990) and an ‘expert coper’ of PMC (Ussher & Perz, 2014).
Elenor's first session offers a concrete illustration of this feminist, person-centred orientation in practice. When she arrived ‘full steam ahead’ and then disclosed hesitance about the body-mapping activity, the therapist did not proceed regardless; instead, she checked in with Elenor's feelings, named the part carrying the anxiety and reassured her that all activities were optional and could proceed at her own pace. This moment of pausing to ask what the hesitant part needed enacts the principle of validating the client's experience before asking anything of her, and positions the client as the authority on what she requires in the therapeutic encounter. Hearing Elenor's full narrative of her premenstrual experience before any intervention and building the session around her spontaneous engagement with the body map further demonstrated the collaborative, nonhierarchical relationship that is foundational to feminist and person-centred approaches.
Reauthoring PMC
In exploring participant acceptability of the ‘woman-centered psychological intervention’ offered, Hunter et al. (2002a) found that ‘developing a different perspective’ on PMC was a helpful aspect within the programme. Shifting the narrative of PMC as an internal pathology or ‘irrational thinking’ (Lustyk et al., 2009, p. 95) is therefore a continual theme of the present programme (Buys, 2024; King & Ussher, 2012; Nordlander, 2018; Ussher & Perz, 2014; Ussher et al., 2014). In the ‘woman-centered psychological intervention’ (Hunter et al., 2002a, 2002b; Ussher et al., 2002), PMC is framed as an experience shaped by interactions between a person's biological, social and psychological worlds, rather than a pathology or personal flaw (Ussher, 2004b). Within this model, the cause of distress is not located ‘within the woman’ but instead ‘within her environment – her understandable response to life stresses and relationship conflict – exacerbated by unrealistic self-expectations that originate in broader cultural discourse about what it is to be “woman”’ (Ussher & Perz, 2020a, p. 196). In the present programme, the common view of the premenstrual experience as an ‘unruly force that is other to [the client] and feared because it is out of control’ (Ussher, 2008, p. 41) is examined and repositioned through an IFS-informed approach, by seeing the premenstrual part or parts as an understandable aspect of the client that has its own needs and desires that can be attended to. This viewpoint contrasts with the dominant narrative of PMC as a force either fully engulfing or abject to the Self and naturally attends to the phenomenon of the split-self common in PMC (Buys, 2024; Chrisler et al., 2014; Loshny, 2004; Ussher, 2004a, 2008).
The trajectory of Elenor's engagement with her body maps across the programme illustrates the reauthoring process as it unfolded in practice. In the first session, she described her premenstrual experience as a ‘flood’ that overwhelmed and displaced her Core, positioning PMC as a force external and threatening to her sense of self. By the fifth session, she had reconceptualised this relationship: the Moon was now drawn as directly connected to her Core, and she described the phases of her cycle as ‘waxing or waning’ rather than as a periodic annihilation of self. The renaming from ‘Fat Elenor’ to ‘Fatphobic Elenor’ in the first session is itself a microinstance of reauthoring: the shift locates the problem not within Elenor's body but within an internalised critical stance toward it, moving from self-pathologising to social critique. These moments demonstrate how the programme's IFS-informed and arts-based approach actively supported clients in constructing new, agentic narratives of their premenstrual experience.
No Longer Self-Silencing
Reframing the premenstrual phase as a time when the PMC experiencers may need to attend to their own needs and ask for support has been found to be a necessary aspect of psychotherapeutic support for PMC (Ussher, 2008). This emphasis is reflected in the present programme by using IFS-informed parts dialogue to attend to the needs of the client's parts, which may have been previously ignored or silenced. Self-silencing, the suppression or denial of one's feelings of distress due to maintaining relational dynamics or believing such emotions or needs are invalid, is understood to be integral in the maintenance of PMC (Chrisler et al., 2014; Ussher, 2003, 2004a, 2006). Self-silencing also refers to practices of self-policing and self-surveillance (Ussher, 2004a, 2008), where a part who silences and a part who is silenced may be active. An IFS-informed approach creates space for all parts to be heard (Schwartz & Sweezy, 2020). Parts who have been split off from the self, or form a process of abjection, are able to be acknowledged and understood; again, lessening this intrapsychic divide (Ussher, 2004a).
The parts-dialogue work in Sessions 2 through 4 makes visible how self-silencing operates and can be interrupted. In the second session, Elenor herself observed that her Exhausted part was ‘not listened to’ and was largely ignored, while the Control part maintained pressure to ‘keep on top of everything’. This dynamic, a manager part suppressing distress in order to maintain function, maps directly onto the self-silencing and self-policing processes common to PMC. The IFS-informed approach created a structured space in which both the silencing part (Control) and the silenced part (Exhausted, Vulnerable) could be acknowledged. By Session 4, when Elenor imagined offering Control and Anxious a resting place in a forest and a lake, the relief she described (‘They wouldn’t have to try so hard’) suggests that attending to these parts’ needs, rather than overriding them, meaningfully shifted her relationship to her own internal experience. The embodied nature of this process as felt in posture, facial expression and a reported sense of peace underscores that the shift was not merely cognitive but whole-body, consistent with the feminist and embodied orientation of the programme.
Outside of the Therapy Room
In exploring participant acceptability of the psychotherapy programme offered, Hunter et al. (2002a) found that ‘being in control’ and ‘handouts’ were two helpful aspects of the programme, expanding on Kancheva Landolt and Ivanov's (2021) suggestion to prioritise the client's ‘ownership’ (p. 1289) over PMC. Beginning the present programme by allowing the client to fully express their narrative and experience of PMC exemplifies the aspect of being in control, as well as the trauma-informed approach of continually asking permission from the client before beginning activities or questions (Grewal et al., 2024; Kulkarni et al., 2022). Tangible homework activities that support developing control and problem-solving skills are also offered in each session, as Han et al. (2019) who, in a meta-analysis of psychological and psychosocial interventions for PMC, found that coping skills were more effective than psychoeducation or social support. The homework allows the client to reposition PMC as a valid reaction and reflection of their ‘true feelings’ (Ussher & Perz, 2020b, p. 226) toward particular aspects of their lives that may be impacting them negatively, legitimising the client's experience of PMC (Ussher, 2008).
Elenor's experience between sessions illustrates how the programme supported the transfer of therapeutic insight into everyday life. At the start of Session 2, she reported that following the previous meeting she had experienced a ‘peak’ premenstrual episode, but that on this occasion she had ‘given permission’ for the experience to take over and actively chose to ask for validation from her partner rather than remaining silent. This shift from involuntary overwhelm to deliberate, self-compassionate response to her own needs reflects the programme's aim of repositioning PMC as a valid signal that can be attended to, rather than a force to be managed or suppressed. The language Elenor used (‘gave permission’) suggests an emerging sense of agency and ownership over her premenstrual experience, consistent with the goal of supporting clients as ‘expert copers’ (Ussher & Perz, 2014) whose knowledge of their own needs is the primary resource for navigating PMC outside of the therapy room.
Implications and Conclusions
The psychotherapy programme presented in this paper offers a person-centred and integrative approach to supporting PMC, codesigned with participants experiencing premenstrual changes. Beyond individual outcomes, the programme underscores the importance of collaborative and practice-led research in refining psychotherapy interventions for PMC, particularly, centring clients’ embodied knowledge and experiences in shaping such interventions. The subsequent phase of the broader research project has explored participants’ experience and construction of the programme, providing emerging insights into its acceptability and feasibility. Future research should continue to honour these voices, combining qualitative and quantitative methods to evaluate the programme while remaining attentive to the contexts, needs and agency of those it aims to support.
Supplemental Material
sj-docx-1-fap-10.1177_09593535261464231 - Supplemental material for Mapping the Body, Meeting the System: The Development of a Codesigned Psychotherapy Programme for Premenstrual Change
Supplemental material, sj-docx-1-fap-10.1177_09593535261464231 for Mapping the Body, Meeting the System: The Development of a Codesigned Psychotherapy Programme for Premenstrual Change by Megan Buys, Raquel Peel and Denise Buiten in Feminism & Psychology
Supplemental Material
sj-docx-2-fap-10.1177_09593535261464231 - Supplemental material for Mapping the Body, Meeting the System: The Development of a Codesigned Psychotherapy Programme for Premenstrual Change
Supplemental material, sj-docx-2-fap-10.1177_09593535261464231 for Mapping the Body, Meeting the System: The Development of a Codesigned Psychotherapy Programme for Premenstrual Change by Megan Buys, Raquel Peel and Denise Buiten in Feminism & Psychology
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.