
Abstract
This study applies conversation analysis to an infant/caregiver activity, “getting vaccinated.” Here, an infant’s natural reactions (crying) to pain (inoculations) appear to function as inchoate social devices aiding the co-creation of an emerging proto-social interaction order. I argue and demonstrate that the infant’s cries comprise its (biological, as opposed to psychological) devices that contribute to the proto-interaction order, when systematically responded to by caregivers, and thus (inadvertently) employed as interactional resources. The caregivers’ responses to the crying demonstrate that the participants’ actions, including the infant’s, constitute resources for creating a proto-social-interaction order from the interacting normative and biological rule systems. Finally, since conversation analysis has not traditionally been applied to infant/caregiver interaction, I contrast relevant conversation analyses to developmental psychological studies.
Keywords
This research was motivated by my previous research (Berducci, 2010a, 2010b) and informal noticing that some type of order manifested in infant/caregiver interaction when caregivers caused pain in infants.
In this introduction I will first explicate my basic analytic motivation via Wittgensteinian thoughts on infant cries as natural reactions, on which, he claims, language learning is grounded. I follow with a biological and phonetic description of infant cries. Further, I invoke non-conversation-analytic infant studies in developmental psychology as counterpoint, to demonstrate how conversation analysis (CA) differs in analyzing infant/caregiver interaction. Finally, I invoke Goffman (1978) and Wilkinson and Kitzinger (2006)’s sociological work on surprise reactions, for comparison to infant cries as surprise reactions to pain.
Natural reactions
One fundamental idea underlying this project is Wittgenstein’s contention (1953) that infants’ natural reactions, such as infants’ pain-cries, through interacting with caregivers, later become refined into spoken language. For infants interacting in an American English context, a pain-cry could become refined into “Ouch!”, and later, more complex pain-formulations, for example “That really hurts,” and so forth. I expand Wittgenstein’s contention, and claim that through interacting with caregivers, infant cries, previous to becoming refined into mature social devices such as language, can be employed to ground those mature social devices employed in turn-taking, both preceding and setting the stage for language and other social devices, in addition to acquiring social (normative) rules.
An additional rationale for Wittgenstein’s relevance to this project is that one salient pain-cry attribute is their structural regularity (please refer to Figure 1), and their regularly being deployed in response to unexpected pain; essential since part of the definition of any type of rule-guided (normative) behavior is its regularity (Baker & Hacker, 2000, p. 44).
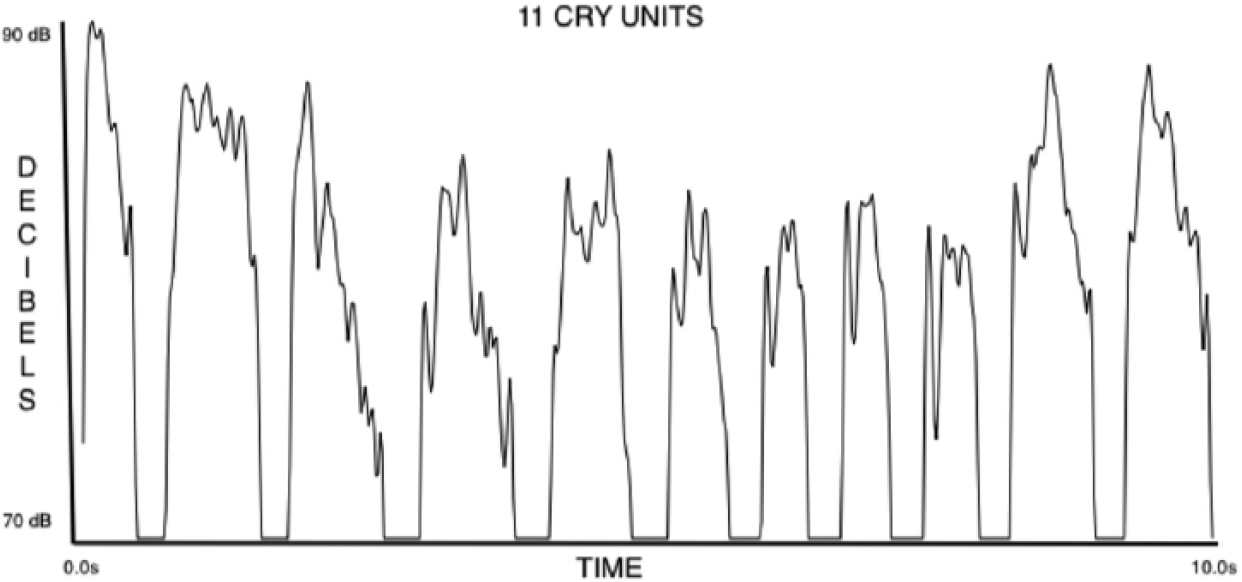
One cry event, comprised of 11 individual cry units.
Figure 1 depicts an example of a pain-cry intensity structure, in decibels (X-axis) and time (Y-axis), of the type of cries to be analyzed in this study. As can be seen, regularity in terms of intensity and duration manifests.
Additionally, pain-cries are caused reactions, whereas adult responses (not reactions) to conversational analytic turns are normative orientations to an other, for example, an infant. Thus, regularity, both structural and as infants’ regular reactions to pain, may serve as one criterion to begin to recognize proto-rule-governed behavior. Infants’ pain-cries are regular, yet not normative; they are caused reactions, and thus cannot be rule-guided as adult surprise performances are (Goffman, 1978), since infants cannot yet intentionally control their cries.
Thus, infant/caregiver interaction, if indeed ordered, would manifest order via categorically different means. Adult/adult interaction is ordered via normative rules; while infant/caregiver interaction may be, as I claim, initially at least partially ordered by biological “rules” (the biological capacity and need to cry in response to pain, and the necessity of in-breaths to fuel such cries); it follows that since infants normally become adults, then infant/caregiver interaction may serve as a foundation for adult/adult interaction insofar as infant/caregiver interaction precedes it, and is structurally similar.
Human caregivers, as homo sapiens, are also biologically equipped to perceive and respond to infant cries; to perceive and seemingly to expect, as I hope to demonstrate, the projected cry-endings—and may employ those endings in regularly responding to infants—again, thus creating a “proto-social-interaction” order.
Infants’ biology/phonetics
Above, I alluded to infants’ biology in terms of their capacity to cry when reacting to pain. By definition, infants are not yet fully persons; thus knowledge of infants’ biological limitations may help demarcate the difference between normative actions (such as turn-taking) and biological reactions (pain-cries).
To accomplish what I wish to do here, entails one to be aware of some infants’ biological capacities, because it is assumed that such capacities act as temporary and foundational proxies for mature social interactional devices such as conversation analytic turns. For anyone to interact at all entails use of basic perceptual abilities accomplished through the five senses. However, a newborn human’s perceptual abilities differ from an adult’s and require explanation to aid in understanding their more limited role in infant/caregiver interaction. I here outline infants’ lack of some biological interactional capacities.
A technical explanation may clarify infants’ lack of self-control, specifically the lack of the ability to voluntarily produce pain-cries. Phonetic research has determined that very young infants cannot regulate sub-glottal air pressure via neural control of their intercostal muscles or any other means (Lieberman, 1986, p. 246). This finding means infants cannot neurally control the cry-intensity-contour shape (see Figure 1) of their pain-cries, entailing: minimal intensity-contour variation (detailed below) resulting in regularly structured pain cries. The resulting regularity thus concomitantly increasing the possibility of caregivers’ accuracy of projecting cries’ endings. Projecting endings, as I will attempt to demonstrate, is essential for creating a proto-social order.
Additionally, in relation to projectability of infant cries, the cries’ fundamental frequencies (F0), usually fall at cry-unit endings, when infants run out of air that powers their cries (Lieberman, 1986, p. 247). F0 falling in the same position (at cry endings) exemplifies that cries are regular and thus their endings are projectable, and further, they are directly analogous to the structure of adult turn-ending intonation, that is, falling F0 at the end of many adult turns.
Human infants of course cannot produce articulated linguistic phenomena, for example, “Daddy.” However, it has been well established that infants, and even fetuses, possess passive abilities of perceiving and differentiating such linguistic phenomena, for example, human-voice sounds (Mampe, Friederici, Christophe, & Wermke, 2009). Infants thus are able to recognize adult vocalizations, and employ them as resources to form their cries. As evidence of this assertion, fetuses in-utero have been found to be able to sense speakers’ intonational contours and mimic them in their early cries. It was found that in line with their soon-to-be mother tongues, when crying, “French newborns preferred to produce rising melody contours, German newborns more often produced falling contours” (Mampe et al., 2009, p. 1994). Infants possess this ability because prosodic, rather than phonetic features are salient for the human fetus since prosodic features do not distort when passing through the mother’s abdominal barrier (Mampe et al., 2009, p. 1994).
As Mampe et al. (2009) have demonstrated, an infant’s cries are not randomly contoured, rather they may share some phonetic commonality with most languages in the sense that “the terminal intonation contour whose acoustic correlates area falling F0 and amplitude thus is the cue that signals the end of a declarative sentence or phrase in most human languages” (Lieberman, 1986, p. 247). The intensity contour (calculated via Praat speech analysis software; Boersma & Weenink, n.d.) of infants’ cries may also be relevant to mature turn-ending intonation. As we can see in Figure 1, the cry-unit contours manifest an intensity structure most of us are aurally familiar with from experience—in many types of infant cry, intensity moves from low to high to low, and followed by an, at times, audible in-breath. It is indicated that infant cries may possess a universal phonetic structure, and that because of their universally predictable structure, infant cries, for caregivers, can be easily recognizable and projectable, and thus a handy tool, employable by caregivers to create an interaction order.
The biological capacity infants possess to perceive and reproduce intonation contours of languages that infants have experienced in- and ex-utero, is essential to this study since this finding may constitute one fundamental reason to view newborns as being primed to actively participate in some way in proto-turn-taking; rather than being viewed as passive recipients, again without positing the existence of any innate social cognition (Fiske & Taylor, 2008).
Additionally, it has very recently been found that infants can aurally detect specific words in the womb and remember them in the days immediately after birth (Partanen et al., 2013).
These capacities to perceive and mimic sound while in-utero or soon after birth supplement the frequent claim that “the learning of language seems to begin in the womb. This may be why infants appear to be able to recognize their mothers’ voices at birth. … This learning all precedes the dramatically accelerated learning that begins after we emerge from the birth canal” (Everett, 2012, p. 187). I would like to highlight that one of my claims here is that pre-linguistic infants in interaction with caregivers learn not only language per se, but simultaneously have the (turn-taking) stage set for them to learn language and deploy it correctly (normatively) in mature interaction. Thus, infants learn some basic aspects of social interaction even as they develop intrauterinally, for example voice prosody, caregivers’ reactions to voices, to loud noises, and so forth. Thus, fetuses, in relation to their “overhearing” conversation and other sounds, can, in a special sense, not only be said to be language/social learners, but can be said to be co-present, non-participating recipients in social interaction, and thus be simultaneously inadvertently trained in same.
In sum, humans thus appear to be born with a variety of biological capacities that prime them, that enable them soon after birth to participate successfully in interaction (not interactional capacities per se) at some attenuated level. Fundamentally, the lack of self-control of cries decreases their variability, virtually all pain cries end in F0, cry-contour is constrained by mother-tongue, and infants learn in utero (so become able to produce cries, for example, relative to their interactional contexts).
Infants’ cries and other types of vocalizations are at times naturally structured into what I term “cry units” (see Figure 1), consisting of a continuous vocalized outburst, powered by one in-breath, and can be depicted in terms of its decibel intensity (Y-axis) versus time (X-axis): rise, followed by peak or plateau, then descent followed by an in-breath, which marks the (biologically necessary) ending and beginning of each cry unit. Each of the 11 cry units in Figure 1 manifest an inverted “U” shape. Each valley between the cry units denotes an infant in-breath. As displayed, it is common for infants to repeat cry units followed by in-breaths, refueling each cry unit, creating the cry event (multiple cry units).
Developmental psychology infant studies
Moving now from infant biology to infant research in Developmental Psychology, it would appear, ostensibly, that this field would be strongly relevant to my current endeavor, especially since that field’s methodological orientations often imply existence of transcriptions of infant–caregiver interaction. However, it seems that in developmental psychological studies individuals in interaction are depicted as pinging turns back and forth, rather than as individuals interacting and creating an emergent interactional order.
Many transcripts in developmental psychological works that exist typically do not supply interactional detail, which conversation analysis deems necessary to understand the operations of that interaction. Additionally, even when interaction is relevant to the study and comprises part of the title, for example in “Mother–Infant Face-to-Face Interaction,” (Cohn & Tronick, 1988), transcriptions were not included in the manuscript.
For example, the transcripts of Kaye and Charney (1981, p. 37) would be considered inadequate according to Conversation Analysis. In particular, all sessions were transcribed in that paper as in the following example (compare to detailed conversation-analytic transcripts in the Data Analysis section): Mother Child (1) (points to picture) What is that one? (2) kitty cat”
A conversation-analytic transcription of those same two turns, may look something like this (details created):
And the analysis something similar to: in turn 01, mother points to the picture with her left hand and simultaneously “[ ]” gazes and poses an information question to the infant, ending the mother’s turn with downward, turn-ending intonation “↓”. The infant responds immediately “=”, demonstrating her understanding of the question by answering correctly, i.e., the picture is of a “kitty cat,” then subsequently directs her gaze to the mother.
Additionally, developmental psychologists many times employ narrative descriptions in lieu of a transcript. A case in point: Trevarthen, an extremely prolific and influential researcher in the field, narratively describes a series of still photos of an infant interacting with caregivers: A 4-week-old infant captures and tracks with her eyes an object that is moving from right to left of her body. She coordinates her whole body and makes two reach and grasp movements with her right arm and hand, and a fast, fisted movement of her left hand. … Integrated activities of this kind can be seen with healthy and alert newborns immediately after birth. (Trevarthen, 2011, p. 126)
This narrative adequately describes individual infant movements for some purposes, but a conversation analyst would be interested in the moment-to-moment emergence of the interactional sequence created by that interaction. The original conversation-analytic transcript of such interaction would be published in its journal article, and through its detail would answer such questions as “When and how does the infant track the object?,” “What is the caregiver doing while the infant is tracking the object?,” “Is there a delay in the infant’s tracking?,” “If so, how much, and does the caregiver orient to that delay?,” “When does the infant coordinate her body and reach/grasp?,” “After the object has stopped?,” and so forth.
Further, differing from conversation analysis, developmental psychologists often employ a pre-existing analytic coding scheme. Conversation analysis does not do so, but rather examines how what is being done in the interaction is understandable to the participants, and out of the participants’ understanding, analytic categories emerge.
I do not suggest that developmental psychologists do conversation analysis, but rather that conversation analysis would be useful in at least supplying a new analytic dimension to analysis of infant/caregiver interaction and the socialization of infants into mature social members, as well as caregivers being socialized into interaction with infants.
In addition to possibly inadequate transcripts, the influence of Bruner, Piaget, and their followers continues in developmental psychology. Many of these followers generally explicate infant interaction and development in terms of intra-individual factors: accommodation, assimilation, impulse control, learning, genetic predisposition, cognitive representation, and similar phenomena. A number of (non-conversation-analytic) interaction studies are performed by this group, but here, interaction is reduced solely to the role that it plays as an influence on, again, intra-individual development factors. On the other hand, a conversation analysis discovers, in a sense, how individuals lose their individuality, and come to perform as individual-in-interaction. However, though I generally oppose the analytic orientation of Bruner, Piaget, and so on, their work is partially applicable to my project, in that portions of it provide details of infant biological capacities employed to cooperate with a caregiver in co-creating the interaction. For example, as alluded to, from that research orientation it has been found that previous to 6 weeks of age, infants cannot clearly see objects—a biological fact which would affect functional attributions to infant gaze, a fundamental social device in the conversation-analytic literature.
Though I generally oppose their methodological orientation, some earlier work in developmental psychology is partially consistent with what I am attempting here. For example, Kaye (1982) examined infant/caregiver interaction in relation to the rhythmic biological capacities of infants—in particular, sucking at a nipple. In that study, infants were found to suck in bursts and patterns, and such phenomena appeared to be related to ordering interaction with caregivers. So far so relevant, however, in that work in particular Kaye concluded that mothers interacting with infants merely create the illusion of their “inter-co-ordination” by responding within “gaps” of the sucking bursts, and thus that infant/caregiver interaction merely mimics coordinated dialogue.
In my analysis below, I attempt to demonstrate that infant/caregiver interaction is orderly (dialogic), and not illusory, but I hope to demonstrate that some type of orderly (coordinated) interaction manifests, which I term here “proto-social-interaction.”
In response to Kaye’s assertion of turns being illusory in infant/caregiver interaction, is the work of Reddy (2010), who evokes some developmental psychological research that he deploys to question Kaye’s findings: “Is such turn-taking really illusory? Are the infant’s responses not responses at all, but independent acts? It was to answer this sort of question that three separate labs (Trevarthen, Papousek, and Tronick’s) developed what have become known as ‘perturbation experiments’” (p. 11). Reddy reported that those labs found what he labels “genuine turn-taking” (2010, p. 11).
I would claim here that the infants in those experiments did take turns with their caregiver, but could not have taken conversation-analytic turns, since the latter are normative. I would claim that those infants took biological proto-turns (natural reactions), which will (under normal circumstances) become mature (normative) turns through interacting with caregivers. In my study here I argue and demonstrate, through explicating the infant/caregiver transcripts below, that these infant turns, because they are natural reactions to pain, are turns that caregivers employ to co-create orderly interaction.
Further, consistent with my orientation, Reddy (2010) evokes Wittgensteinian ideas, yet does not seem aware that these ideas could be employed in conjunction with conversation-analytic methodology to solve Wittgenstein’s problem: Ludwig Wittgenstein showed that if you assume that representation [cognition] precedes communication, you cannot explain communication at all. You have no way of explaining how the shared meanings originated in the first place. A meaning must be public – or shared – in order for it to be used in conversation or communication. (p. 18)
A conversation analysis demonstrates how meanings are “public” and “shared,” and how those meanings are employed in interaction. Further, Reddy in that same paper (2010) advocated a Wittgensteinian solution: “If we accept Wittgenstein’s solution the question becomes: What meanings does the infant share with adults? When and how do these meanings emerge? If communication is taken as primary (i.e., if we accept the ‘hermeneutic circle’ in this question) the paradox disappears” (p. 18). Through conversation-analytic methodology, I take communication as primary.
In this article, I take the more prudent orientation, more consistent with conversation analysis: we are biological beings and, as I hope to demonstrate, that proto-social-interaction order is based on, neither reduced to nor caused by, our biological capacities, and that the demonstration of any interaction order need not posit any innate infant psychological processes that are putatively coterminous with or precede communication.
I agree here that there are structural similarities between infant/caregiver and mature interaction, but I, to connote their foundational character, again would posit “proto-conversation” comprised of “proto-turns” as alternatives to the posited “conversation” and “turns” of the developmental psychologists cited by Reddy (2010). In the forthcoming analysis, I hope to demonstrate that Kaye’s (1982) “gaps,” may be analogous to proto-TRPs (see below); and if so, would have been essential to the “mimicked” interaction order Kaye found.
Any theoretical implications of my study, if correct, would dissolve and demonstrate as unnecessary, any innate-cognition perspective, such as those cited in Reddy (2010, p. 8), Trevarthen’s (1998) “innate intersubjectivity,” where “representation precedes communication” (Reddy, 2010, p. 18), and those of many other infant researchers and cognate research orientations, in regard to infant cognition driving infant behaviors to function proto-socially in interaction with caregivers.
Finally, and maybe most importantly, it appears that in both conversation analysis and developmental psychology little or no work has focused on one object of this study—where (if anywhere), within the phonetic structure of infant cries, caregivers initiate their response turns, and relate this potential proto-social phenomenon to the creation of a type of proto-social order of infant/caregiver interaction.
Sociological infant studies
Here I explicate a group of studies that are similar to what I propose, yet differ enough to enhance my findings in infant/caregiver interaction. From a more sociological standpoint, interaction studies in the infant/caregiver field is occupied by those who do analyze infant/caregiver interaction, but (a) do not apply conversation-analytic methodology and regard cognition as essential to interaction in the form of Theory of Mind (ToM); (b) studies that take an interactional perspective but do not employ conversation analysis, for example Bateson (1975); (c) those that employ conversation analysis and argue against a sociological explanation of how people become social, for example Durkheim (1901/1938), but did not investigate very young pre-linguistic infants, for example, Wootton (1997); and (d) employ conversation analysis, yet regard innate cognition as an internal process necessary for interaction to ensue, such as Filipi (2009), Levinson (2006), and others. Through my analysis, I would like to rectify and fill in any lacunae created by these four research classes. I will now expand on each of these four categories.
Tomasello’s work (1999, 2003) related to Theory of Mind (ToM) is currently in vogue and influential in Developmental Psychology. According to him, human infants possess a special form of social cognition, ToM, which is “the [innate] ability of individual organisms to understand conspecifics as beings like themselves who have intentional and mental lives like their own” (Tomasello, 1999, pp. 5–6). This claim can possibly be explained away by conversation analysis. In conversation analysis, recognizing another’s intention, for example, is embedded in turn-taking sequences, rather than theorizing what the other speaker is doing. For example, if interactant A in turn 1 hits B, then B in turn 2 can claim that A did so intentionally without imputing any ratiocination on A’s part; though reasons for the hitting can be stated by both A and B. Actions such as B’s blaming A (turn 2), are sequentially organized to take account of what happened (Wootton, 1997).
An additional conversation-analytic related argument against ToM has also been supported by non-conversation-analytic infant interactional researchers Mauritzson and Säljö (2001), whose results demonstrate “that whether or not children ‘are able’ to adopt other people’s perspectives is very much a situated [non-cognitive interactional] affair” (p. 213).
Finally, a logical argument against ToM according to Sharrock and Coulter (2004) is here applicable—in sum, they argue that we (researchers) must avoid confusing mastery of cognitive concepts, with possession of a ToM (p. 587). Mature humans come to recognize so-called cognitive processes in others through interactional experience and the learning of concepts, and how concepts are employed in interaction. Tomasello’s and others’ search is for mental processes that “precede communication” and determine/influence our actions, rather than the search for normative rules which manifest in our communicative actions.
M. C. Bateson’s (1975) infant observations are consistent with mine, yet she did not employ conversation-analytic methodology. She concludes that the moments when infants and caregivers “seemed to be conversing with each other occurred like rare gold nuggets between long sections of other types of material” (p. 102), and in infant/caregiver pairs, “social interaction similar to conversation were recognizable for all pairs before [infants of age] 3 months” (p. 102). Since she did not employ conversation analysis, she was not able to describe rigorously how she came to conclude that infant and caregiver interaction was conversational as I endeavor to do.
Next, the traditional Durkheimian (1901/1938) social-scientific response to the problem I am posing, was that all adult/child interaction constituted a caregiver imposing on the child, ways of seeing and acting which, they would not have arrived spontaneously (Wootton, 1997). Following Durkheim’s formulation, caregivers would explicitly teach infants social rules and infants would consequently build up a cognitive store of social knowledge, which they would access when needed. Further, implicit in Durkheim’s assertion, is that infants could and would know when to correctly apply that knowledge in multifarious social contexts.
One effective response to Durkheim’s research, and true to the conversation-analytic tradition, has been Wootton’s (1997) work. He found Durkheim’s formulation of the problem to be invalid in the sense that a caregiver need not provide an infant explicit rules related to social behavior on every interactional occasion. Rather, young children come to participate in the interaction by acting strategically so as to take account of what has happened in any given encounter.
The results of Wootton’s (1997) research seem to have resolved the problem engendered by Durkheim’s earlier putative solution of the traditional research question “How do infants become social?” Problems however linger. Wootton’s results are essentially consistent with what I have found in other infant/caregiver interaction research. However, he studied a child aged 1 to 3 years old, who already possessed some measure of mature turn-taking ability. It has not yet been determined, by Wootton or others, in what turn-taking ability is grounded. Thus, the success of Wootton’s research in mitigating Durkheim’s argument, begs the question “Is interaction ordered between caregivers and children younger than 1 year, and if so, how?”
Another recent conversation-analytic study (Filipi, 2009) is again on the surface similar to and consistent with my project. Filipi deftly employed conversation analysis to study infant/caregiver interaction; however she focuses only on infants’ linguistic development between 9 and 18 months—older than the infant in my study, and does not focus on turn-taking origins, and contrary to the implicit tenets of conversation analysis, succumbs to the psychological tack—by conceiving of infant intention as an inner phenomenon, à la Tomasello and Levinson (among others), rather than intention being interactionally organized.
Another relevant researcher, Levinson (2006), employs conversation analysis, but his ideas on intention as a cognitive process that develops in infants comprises his main tool for explaining human action. Though Levinson employs CA, Coulter (2005) cautions us that if any Cartesian (dualistic) residua remain in sociological analyses of interaction, we (non-cognitively oriented social science researchers) should abandon our work, since we would not be accessing social interaction fundamentals—social interaction would merely be an effect of cognition. In short, Levinson has allowed psychological mechanisms into his work that, for him, account for action. However, in ordinary conversation, and in infant/caregiver interaction, from my project’s point of view, these mechanisms are not necessary. Cognition is not one general process necessary to explain social action, rather it consists of myriad phenomena, as was detailed by Anscombe (1963). Her work of course was not explicitly interactional, but she argued convincingly that putative cognitive processes (intentions in particular) are public acts performed in and recognized through various interactional contexts.
Turn-taking and conversation analysis
Mature conversation-analytic turns consist of actions (verbal or non-) that comprise interaction. Mature turns are made of grammatical units, for example, sentences, phrases, lexical items, and so on, including intonation. Of course infants cannot yet produce such items. Conversation-analytic research has verified in many languages and cultures, that in interaction, as a speaker comes to complete his/her turn, the transition to next speaker becomes relevant. The transition to next speaker can be accomplished “with the immanence of possible complete as the ‘transition-relevance-place’ [TRP, see below].” (Schegloff, 2007, p. 4). Next-speakers are normatively allowed to initiate a turn if chosen by the present speaker, or can self-select within a TRP.
Conversation-analytic turn-taking appears to be universal and biologically based since according to Sacks’ (1992) claim concerning conversational turn-taking, “If you get that kind of stability [turn-taking order], across fantastically different languages, then the social sciences and the biological sciences come to some close relationship” (Sacks, 1992, pp. 98–99). This claim strongly suggests that turn-taking is grounded in human biological capacities, but the claim has never been tested. Thus I proceed to demonstrate the how of same.
To do so, I employ a conversation analysis to the infant/caregiver activity “vaccinating an infant.” For adult/adult interaction, the original conversation-analytic researchers (Sacks, Schegloff, & Jefferson, 1974) have discovered fundamental interactional rules: conversational overlap is avoided; speakers change; size and ordering of conversational turns vary; among others. These findings beg various questions in applying conversation analysis to infant/caregiver interaction, since the infant is not an adult, and relevantly, infants and caregivers’ interactional skill sets are vastly asymmetrical; yet the potential for the grounding of a mature interaction order is seemingly inherent in infants’ biological capacities.
Conversational overlap and TRPs
Above, in Figure 1, I structurally described cry units, their endings, manifested as intensity (decibel) declination, preceded by an in-breath. I now attempt to relate them as analogues to conversation-analytic TRPs where transition to next speaker becomes relevant (Schegloff, 2007; akin to Kaye’s, 1982 “gaps”).
In adult/adult interaction, “Terminal [end-of-turn] overlap occurs at a point where a turn in progress is for all practical purposes completed; where what is being said is all over but for the final noises” (Jefferson, 1983, p. 14). Jefferson’s finding would suggest that caregivers should, if they are to at all, initiate their turns at the infant’s cry-unit endings which are “for all practical purposes completed” (p. 14), as indicated by their downward intensity.
Mature TRPs, alluded to above, are places at which it is normatively correct for turn recipients to initiate a turn (Jefferson, 1983). Posited here are infant (immature) TRPs, henceforth, proto-TRPs (pTRPs), places towards the projected cry-unit endings or beginnings, adjacent to or within in-breaths between cry units, that I hope to demonstrate are functionally analogous to mature TRPs (places where transition to next speaker can normatively occur). Please note I am not advancing the claim that cry-unit endings equate to mature TRPs, but rather that they are TRP-like, and thus may ground the formation of mature TRPs, and consequently an adult interaction order.
In conversation analysis, if an adult recipient responds previous to a TRP, that is, too early, it could be seen by speaker as an interruption; after a TRP, that is, too late, and the time between the turn-ending and incoming turn could be viewed as a lapse (non-response) by speaker. Thus TRP durations are co-created and vary according to interactional context. In short, TRPs are phenomenological.
In adult/adult interaction, it has been found that the first possible TRP in any speaker’s turn is marked at its beginning by immanence of possible turn completion through projecting its own end as do, I claim analogously, infant pain cries.
Surprise in interaction
It may be beneficial to compare and situate infants’ pain-cries relative to Goffman’s (1978) response cries, and further with the surprise reactions of Wilkinson and Kitzinger (2006). These two papers provide us with structure and information with which we can compare to enrich the analysis at hand and contextualize our understanding of infant cries as surprise (biological, non-normative) reactions that may ground future adult normative surprise responses, such as “wow,” “gosh,” and so forth.
The following from Goffman (1978) seems an accurate description of infant crying in reaction to pain: “Significantly, we have here [infant cries for example] a form of behavior whose very meaning is that it is something blurted out, something that has escaped control” (p. 799).
Wilkinson and Kitzinger (2006) build on Goffman’s work. They employed a conversation-analytic approach to investigate a subset of adult response cries in interaction, those which perform surprise (p. 154), as contrasted to infant cries which are “blurted out.” In their analysis, adult surprise responses are interactionally achieved by being prepared for several turns in advance. Adults performing surprise are “responsive to an interactant’s prior talk [prior interaction], and not [emphasis added] to direct sensory impressions of the world” (p. 156). Thus, as is ordinarily thought, surprise responses do not need to be, for adults, visceral eruptions of emotion, as are infant pain-cries. Rather, surprise responses (“wow,” “gosh,” and so forth) are deployed by those mature enough to be versed in surprise language games; to perform as-if surprise (Wilkinson & Kitzinger, 2006, p. 153). I here claim that “wow,” “gosh,” and so forth are analogous to “ouch,” that is, they are Wittgensteinian refinements of visceral surprise reactions to the unexpected, such as pain cries. They are performances of viscerality (p. 161), not viscerality itself, as are the infant’s cries in this study. These adult surprise performances are normative, and, I hope to have indicated, must be grounded in visceral reactions, such as the pain cries in this study.
The infant of the age in this study (approximately 2 months) cannot, sensibly, have self-control attributed to them, for example infants of that age cannot withhold their cry-response to pain, thus cannot design the pain-cry as a social performance. Wilkinson and Kitzinger (2006) found “that the expression (and withholding) of surprise is thick with culture” (p. 178). These sociological findings stand in contrast to Darwin’s (1872) organismic view, that surprise is an innate, adaptive, uncontrollable product of an individual’s physiology. The organismic view describes the infant’s cry reactions to inoculations.
For many social scientists, adult emotions, such as surprise reactions, are completely social, but what they seem to have ignored is that emotional outbursts are ultimately biologically based (Averill, 1974), a connection I hope to make here, and further, that adults did not lose the ability to viscerally respond to “direct sensory impressions of the world [such as painful inoculations]” (p. 156), and still on occasion “blurt out.”
Data analysis
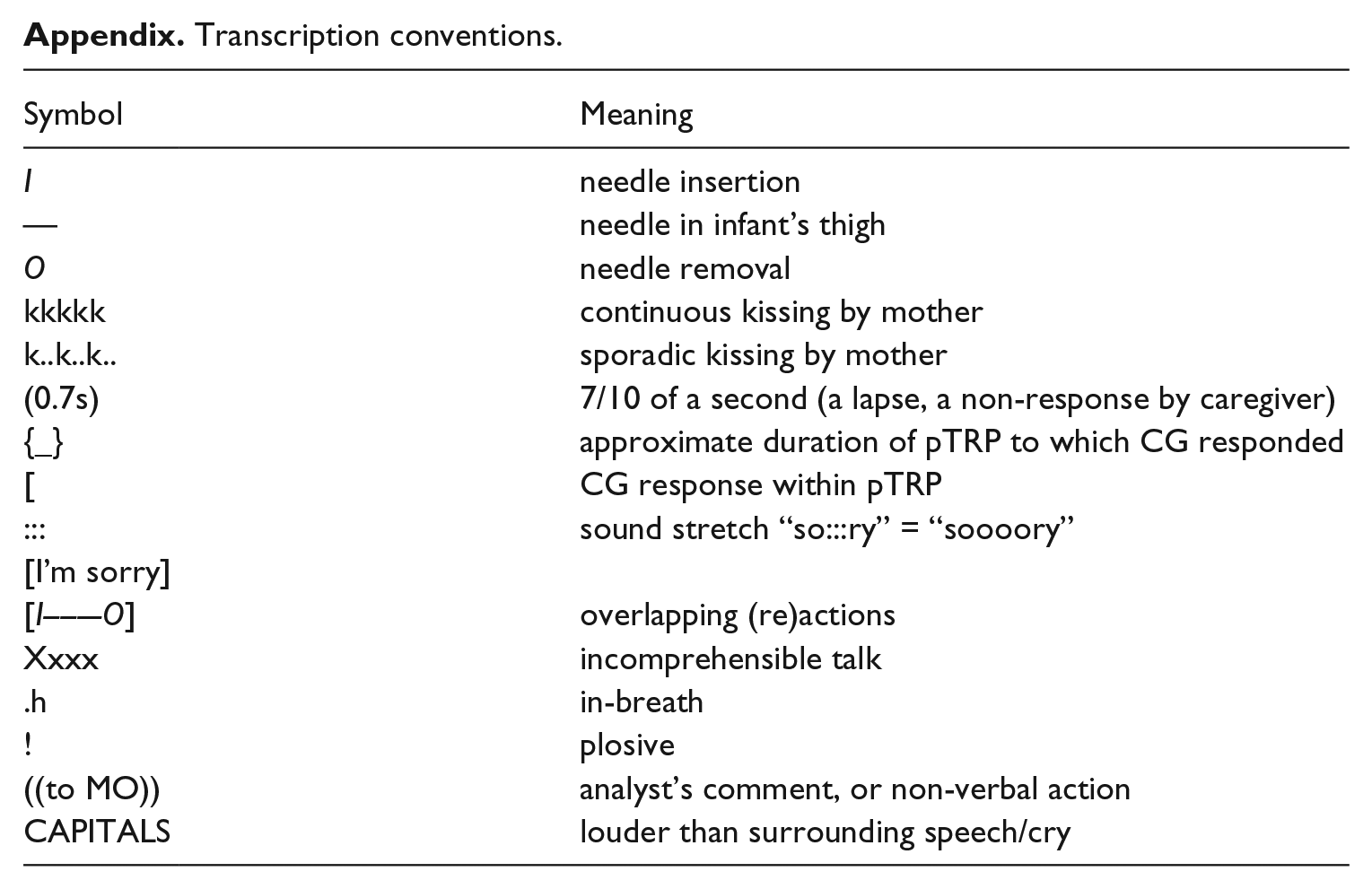
Following is a conversation-analytic transcript of five vaccination inoculations. The analysis focuses on the interrelated timings of inoculations, infant’s (IN) pain-cry reactions, the nurse’s (NU) apologizings, and the mother’s (MO) comfortings. In these fragments, the infant is lying on its back, while the mother, positioned at the infant’s head, continually steadies the infant by holding its arms. The nurse is positioned at the infant’s feet and injects serum into the infant’s thighs. I divide the data transcript into five fragments, one for each inoculation (please see Appendix for transcription conventions).
First inoculation
The video fragment begins with the first inoculation; the syringe has already been inserted into the infant’s thigh in line 01, “—-”. It is removed at the end of line 01, “O”, followed by cry units in lines 02 and 03, that is, the infant reacting to the inoculation.
The nurse initiates line 04, an apology, within “[‘, the pTRP ‘{
Second inoculation
With line 07, the infant continues the cry from the first fragment (line 06), initiates and ends another cry, followed by an in-breath, then initiates a second cry unit “EH::::::::::::” at the end of line 07. It is previous to the initiation of the second cry unit of line 07, within the pTRP, that the nurse in line 08 initiates talk directed to the mother, simultaneously overlapping insertion “I” of the syringe in line 09.
The mother in line 10, responds to the nurse’s line 08 “just take xxxx” within the mature TRP at the end of line 08, with a questioning, “huh?” overlapping the needle removal “O”. Line 11 is the mother’s continuing her own turn of 10, overlapping the cry unit of line 12. Next, the infant in line 12 delivers a complete, contoured, inverted-U pain-cry.
Again in line 14, the nurse responds within the pTRP of line 13, with a routine, clinical apology. Simultaneously, and within the same pTRP of line 13, the mother in line 15 initiates a continuous kiss, “kkk,” initiated and ending simultaneously with the apology of 14, and the ending of the pain cry of 16.
The infant produces two cry units in line 17. And again, the nurse in 18 initiates an apology within line 17’s pTRP. In line 19, the infant produces a non-pain cry, and in line 20, the mother responds within line 19’s pTRP, and again responds in line 21’s pTRP (non-pain vocalization) with line 22.
Third inoculation
In line 23, the nurse inserts the syringe “I” within the mature TRP created by the mother’s talk of 22. The infant initially reacts to the injection with a low intensity pain cry at the beginning of line 24, while the nurse overlaps with clinical empathy towards the end of the second cry unit with line 26, 0.4s after the in-breath of 24, after the pTRP. This drawn out low intensity cry (vocalization) does not project an ending, thus no pTRP needed to be filled.
In lines 27 and 28, the infant reacts with three more cry units (pain-cries). The mother’s continuous kiss, “kkk,” on the infant’s right cheek, is initiated at the very beginning of the first pain cry of line 28, within the pTRP, and continues to the end of the third pain cry and into the next fragment.
Fourth inoculation
The fourth inoculation, is initiated “I” within the pTRP created at the end of line 30. In 32, the mother continues the kiss from the previous inoculation fragment, followed by a “sh:::::::” which ends simultaneously with the removal “O” of the needle in line 31. In 33, the infant performs “pre-cry vocalizations” “eh h! .h!” before initiating a complete cry unit, responded to by the mother in 34, at the pTRP created at the end of line 33.
The next pTRP is that created at the end of line 37, filled by the nurse in line 38 and simultaneously by the mother’s continuous kiss in 39.
Fifth inoculation
The fifth and final inoculation is initiated “I” within “[”—the pTRP created by the first cry unit of line 40. The nurse’s turn “I’m do:ne” is deployed within the pTRP of 42, and after that talk, mother repeats and upgrades “I’m do:ne,” by inserting an affection term “hon” in 44. The initiation of nurse’s turn 47 can be explained in two ways. One is that she missed the pTRP created at the end of line 45, or two, because of the flatness of the cry unit in 45, no pTRP was perceived by the nurse. This situation requires further study.
The mother’s line 48, releasing hold on the infant, is initiated within the mature TRP created by the nurse in line 47 (mature TRPs occur twice in this data set, and are not considered part of the analysis).
Finally, the nurse in line 50 deploys an apology within the pTRP created by the end of line 49.
Data summary
In sum, the caregivers responded to 16 out of the possibly available 18 pTRPs created by the infant’s cries. I use “possibly” out of caution since the two pTRPs that the caregivers did not respond within were weakly projectable, in the third and fifth inoculations, that is, the intensity contour was relatively flat, and hence the endings (pTRPs) of these cries may not have been projected, and thus not perceived as legitimate (normative) places for the caregivers to take a turn.
Third inoculation:
Fifth inoculation:
In both of these cases (lines 24 and 45) where the caregiver did not fill the available pTRP (lapses), the cries’ intensity contours were relatively flat “::::::::”. However, both ended with implosive in-breaths “.h!” which are associated with pTRPs. Thus it would seem that caregivers orient more towards the falling intensity of the cry units rather than the in-breaths as cues to initiate their turns.
Also, please note that not all pTRPs offered by infants need to be filled. One point under consideration here is where in the infant’s cry unit caregivers responded. Do they orient to the endings of previous turns (in this case proto-turns) as they do in mature social interaction? It appears they do.
Discussion
The infant/caregiver interaction in this analysis acted as a species of natural experiment regarding the organization of turn-taking, in that the infant’s cries, the proto-turns (as I hope to have demonstrated), manifesting a regular, predictable inverted “U”-shaped intensity structure, are employed by caregivers as aids to organizing the activity. Infant cries (surprise-pain reactions), regularly deployed after inoculations, manifest neither syntax nor semantics, but rather could be described as regularly structured vocalizations, thereby projecting their ends, and thus providing a space (pTRP) where caregivers could normatively respond.
Both the nurse and the mother oriented to the infant’s cries within what I have termed pTRPs. As we have seen, all but two of these proto-transition places were located towards the endings or within the following in-breath, when interactional work (inoculating, comforting, apologizing) had to be done. The two cases where caregivers did not respond within seeming pTRPs were those where the prior cry unit manifested a relatively flat intensity structure, thus did not project any (normatively) legitimate place for caregivers to respond.
It is important to note again that the cry units as surprised reactions, were caused by the inoculations. The timings of the cry units were controlled by the nurse, coordinated with the regularity of previous cry units, and the comfortings of the mother. The cry units comprised one structuring principle for the infant/caregiver interaction. It was thus possible for caregivers to perceive and orient to cry unit endings (downward intonation), and employ them as interactional resources (pTRPs); again without any necessity to posit any cognitive phenomena to afford such ordering.
In relation to infants’ cries it has been found that “The acoustic and linguistic analysis of cry and speech production in infants and young children demonstrates that human linguistic behavior is structured by physiological mechanisms” (Lieberman, 1986, p. 257). This finding directly relates to the findings here. Reformulating and expanding Lieberman’s findings to directly relate them to my project, I would assert that the acoustic analysis of cry units into intensity contours employed in interaction with caregivers possesses a possibility to demonstrate that all human social interactional devices (not merely linguistic) deployed in turn-taking, are ultimately grounded in and structured by, yet not reduced to, infants’ natural reactions (as Wittgenstein posited).
I would like to emphasize that this research in no way constitutes an attempt to reduce social order to biological mechanisms. One goal was to explicate and defend the claim that one human infant biological capacity could ground a type of interaction order. A quote from Ryle (1949) may clarify: the fact that there is no contradiction in saying that one and the same process, such as the move of a bishop [in chess], is in accordance with two principles of completely different types [causal/biological and normative] and such that neither is “reducible” to the other, though one of them presupposes the other. (p. 65)
Mature turn-taking is a second-order (normative) ability grounded, as I hope to have shown, on the first-order biological (causal) ability of crying in response to pain.
The infant’s reactions (not responses) were orderly in the sense that they were regular and predictable, but the order was biological rather than normative. Outside of the pain-cries as surprise reactions to the inoculations, the infant was not found to respond to the adult’s actions in an orderly manner. For example, the infant did not respond within the TRPs of the caregivers’ talk, nor was expected to. The pain-cries were (biologically) normal reactions to pain, and they occurred in the (non-normatively) correct position, that is subsequent to the injections. The caregivers’ responses to the infant on the other hand were normative, in addition to administering inoculations, the apologizings and comfortings were well timed, attuned to both talk and pain-cries, manifesting the conversation-analytic rule, “one person talks at a time to avoid overlap.”
As mentioned in the introduction, emotional outbursts in adults have been demonstrated to be social performances (Goffman, 1978). However in those demonstrations, researchers avoid mentioning that such outbursts are grounded in biological capacities (Averill, 1974), such as infant cries in response to pain. I attempted here to rectify that state of affairs.
Though Wilkinson and Kitzinger (2006) found adult surprise to be designed to appear spontaneous, the infant’s pain-cries in this study were spontaneous insofar as the infant could not socially perform. Infants of this age (2 months) cannot yet control biological reactions, such as pain cries, to intentionally employ them for social ends. They are not yet “thick with culture” (Wilkinson & Kitzinger, 2006, p. 178). The infant’s cries remain so far “thin with culture,” but appear necessary to form the ground of adult surprise performances.
The nurse, on the other hand, displayed what she expected by her not deploying surprise responses when she surprised the infant (with the inoculations); she designed the needle insertions, the when and how of the inoculations, in cooperation with the infant, and synchronized with the infant’s cries. She was the recipient of the expected infant’s visceral (non-performance) surprise reactions (pain cries).
According to Wittgenstein, any infants’ cries (as natural reactions) will be refined into normative response tokens, such as “wow,” “ouch,” and so forth. “Ouch” could be an adult performance if prepared in advance: an adult understands the context “getting a shot,” visits a physician, sees the doctor prepare a syringe, receives the inoculation, and is able to produce a normative surprise performance, for example, “ouch,” an as-if surprised-by-the-injection response. The infant, though prepared for the coming inoculations similarly: visiting nurse, lying on the table, and so forth, cannot yet perceive the preparations as preparations, cannot yet conceive of the language game “getting inoculations,” does not yet possess normative abilities, and thus is not able to intentionally perform surprise, but rather blurts out pain-cries. And again, it is this “blurting out” that grounds future normative turn-taking in general, and surprise performances in particular.
Here we saw fundamentally (non-rule guided, non-social, non-normative) natural infant reactions, pain-cries, being responded to by caregivers as if they were social resources in a socializing context, co-creating a proto-interaction order. The structure of such cries (downward intonation/intensity at their endings) in such interactions appear to be both logical (grounding phenomenon à la Wittgenstein) and empirical (in light of caregivers initiating turns at regular positions of the cry units) candidates employed by caregivers to help create a proto-interaction order, grounding a more mature social order.
Furthermore, I believe I have thus also demonstrated the utility of conversation analysis to the field of developmental psychology in a few ways. First, conversation analysis is a naturalistic methodology that affords its practitioners to examine infants’ cognitive, physical, and emotional development, and so forth, in one setting, in enormous detail, in context, indispensable to detect the most minute candidates (such as proto-TRPs) for developmental change.
Conversation-analytic methodology would be useful for developmental psychology since according to Lerner (1989), the latter ignores previous literature related to interactions of organisms in context, and that “this previous literature has demonstrated the logical traps, theoretical dead-ends, and empirical vacuity of attempting to treat organism and context as independent, non-transactive entities; that is, as parallel vectors or as main effects [caused] in a world of additive, linear combinations” (p. 167). Insofar as Lerner’s claims are valid, conversation-analytic methodology can help alleviate such methodological problems. ten Have (2011) lists, in a detailed summary of reasons to employ conversation analysis that are directly relevant to developmental psychology: CA [Conversation Analysis] operates closer to phenomena than other approaches. … it can take into consideration details and subtleties of human interaction that are lost in other practices [such as Developmental Psychology] and that have proven to be important for participants. … CA’s perspective on human interaction is organizational and procedural: When people talk with each other this is not seen as a series of individual acts, but rather as an emergent collectively organized event; the analytic purpose is not to explain why people act as they do, but rather to explicate how they do it. (pp. 9–10)
Finally, here I have shown that infant/caregiver interaction is orderly in that the infant and caregivers served as environments for each other, and that these participants were co-dependent transactive entities, from whose interaction, a co-created proto-social order emerged, a recognizable order developing from the interaction of two rule-systems (biological and normative), without the need to invoke any type of cognition. I have demonstrated how this order was achieved through the detailed conversation-analytic transcription of when the infant reacted (cried after injection), and when caregivers responded in accord with those cries (within the pTRPs, downward intonation of the cries). This demonstrated the claim that “talking together is basic to the social life of humans” (ten Have, 2011, p. 10), and adult “talking together” is grounded in infant/caregiver interaction.
Footnotes
Appendix
Transcription conventions.
| Symbol | Meaning |
|---|---|
| I | needle insertion |
| — | needle in infant’s thigh |
| O | needle removal |
| kkkkk | continuous kissing by mother |
| k..k..k.. | sporadic kissing by mother |
| (0.7s) | 7/10 of a second (a lapse, a non-response by caregiver) |
| {_} | approximate duration of pTRP to which CG responded |
| [ | CG response within pTRP |
| ::: | sound stretch “so:::ry” = “soooory” |
| [I’m sorry] | |
| [I——-O] | overlapping (re)actions |
| Xxxx | incomprehensible talk |
| .h | in-breath |
| ! | plosive |
| ((to MO)) | analyst’s comment, or non-verbal action |
| CAPITALS | louder than surrounding speech/cry |
Acknowledgements
I thank Aug Nishizaka of Chiba University, Tokyo, the anonymous reviewers of this journal, and my 2011 fellowship colleagues at the Konrad Lorenz Institute for Cognition and Evolution research, Vienna, Austria, for helpful comments and suggestions.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.