
Abstract
This introductory article to the Special Issue ‘Social Dialogue in Care Services’ examines how European countries have addressed the ‘care trilemma’ – balancing service coverage, fiscal constraints, and job quality – in early childhood education and care (ECEC) and long-term care (LTC). Despite the expansion of care services across Europe over the past two decades, labour shortages have become widespread. Building on the care trilemma framework, the article investigates the institutional determinants of this paradox and the role of industrial relations in shaping labour market outcomes in the care sector. The analysis combines quantitative evidence from 22 European countries with qualitative insights from seven country case studies presented in this Special Issue. The findings show that most countries have addressed the care trilemma through ‘low road’ strategies: increases in public expenditure and service coverage have often been accompanied by stagnating or deteriorating job quality, reflected in low wages and high work intensity. Overall, the article shows that variations in the resolution of the care trilemma are explained less by levels of public expenditure alone than by the institutional configuration of industrial relations systems and care policy legacies shaping labour regulation in the sector.
Keywords
Introduction: Why we should care for care workers
There are several reasons to pay closer attention to employment in the care sector − particularly early childhood education and care (ECEC) and long-term care (LTC), excluding healthcare − within the industrial relations and comparative political economy literature.
First, employment in ECEC and LTC has expanded significantly in recent decades, driven by socio-demographic changes and welfare state transformation. Rising female labour market participation and population ageing have increased demand for formal care services. At the same time, the ‘Social Investment Turn’ has led many advanced economies to prioritise policies that promote labour market participation and human capital development (Busemeyer et al., 2018), thus transforming ECEC and LTC into key policy instruments supporting labour market participation among parents of young children and caregivers of older relatives (EC, 2023).
Second, a key feature of care work is the ambiguity surrounding its skill requirements. Because inadequately defined and weakly recognised competencies characterise care occupations in several European countries, the consolidation of a stable and institutionalised ‘professional jurisdiction’ (Abbott, 1988) is often hindered, thus undermining the definition of adequate working conditions. Moreover, the historical legacy of unpaid family care, traditionally performed by women, continues to shape distorted perceptions of appropriate levels of professionalisation and employment conditions (England, 2005).
Finally, the care sector provides a valuable lens for examining industrial relations institutions and trade union strategies in a branch of the service economy that differs from traditionally studied sectors, since care diverges from labour regulation frameworks in both the public sector (particularly in education and healthcare) and private services, whether low-end labour-intensive services or high-skilled knowledge-intensive services. This is due to its ‘hybrid’ systems of service governance, reflecting historically mixed public–private provision. While some countries retain largely public provision, most European systems combine public services with publicly funded private providers, whose role has expanded since the 1990s alongside the marketisation promoted by New Public Management (Hermann and Flecker, 2012). The literature shows not only that industrial relations institutions differ significantly between the public and private sectors (Di Carlo and Molina, 2024; Mori, 2017) but also that market mechanisms shape working conditions in public services: by exploiting regulatory differences between public and private sectors, governments might contain public expenditure while maintaining service coverage through lower labour costs (Grimshaw et al., 2015; Mori, 2017). In sum, the structurally ‘hybrid’ nature of the care sector has two implications. First, working conditions and their regulation can be influenced by the type of provider. Second, cross-country comparisons − and comparisons between ECEC and LTC within the same country − must account not only for the degree of provision hybridity in care systems but also for the capacity of industrial relations institutions to coordinate across the public–private divide (Mori, 2024).
Taken together, these developments reveal a puzzling pattern. On one hand, socio-demographic change and welfare reforms led, over the past two decades, to a significant expansion of care policies in terms of public coverage and funding − even during the harshest years of austerity − and especially when compared with other social policy domains that experienced retrenchment, such as healthcare and pensions. Thus, employment opportunities in care services have also grown substantially. On the other hand, this apparently virtuous cycle conceals a central paradox: despite continuous investment and rising demand, employment expansion in the care sector faces severe labour shortages across all EU member states (Kim, 2020; Read and Fenge, 2019). Although shortages affect several sectors, particularly after the COVID-19 pandemic, they are especially acute in ECEC and LTC and are expected to persist due to demographic trends (ELA, 2025; WHO, 2022). Thus, despite its employment potential, the sector remains chronically understaffed (Eurofound, 2020, 2023). How should this tension be interpreted? These shortages may reflect a temporary post-COVID labour market imbalance or a lag in labour supply adjustment to rapid sectoral expansion. Alternatively, they may point to deeper structural mechanisms underlying the shadow side of care policy expansion.
Building on this question, this article − together with the contributions in this Special Issue − pursues two objectives. First, it identifies the determinants of persistent labour shortages and the low occupational attractiveness of the care sector in Europe, with particular attention to working conditions and job quality. Second, it examines cross-national variation within the EU and the factors shaping similarities and differences, focussing on the configuration of industrial relations institutions and actors.
To address these questions, the article proceeds as follows. The next sections present the analytical framework, hypotheses, data, and methods, followed by the empirical findings and concluding remarks.
An analytical toolkit to study care labour markets: The care trilemma and its different solutions
Understanding labour market dynamics in the care sector – and in particular labour shortages – requires considering the key policy priorities that governments in advanced economies must address when making decisions about care provision. These concerns can be framed within a trilemma, which consists of three often conflicting priorities that governments must balance within each country-specific context (Esping-Andersen, 1999; Iversen and Wren, 1998; Pavolini et al., 2013).
First, due to growing demand and increased pressure from households for more state support − ranging from better regulation of care markets to expanded rights for benefits in cash or services − governments are compelled to increase the coverage of needs in ECEC and LTC, also through the expansion of service provision.
Second, since the 1990s, states’ decisions in public employment and social policy have been shaped by a ‘permanent austerity’ condition in public finances, limiting the ability of governments to provide and fund new initiatives (Pierson, 2001). This concept reflects the shift from the post-World War II era, when welfare states could expand more easily. Currently, expansion requires recalibration or restructuring of expenditures − allocating resources from one social policy area to another (Ferrera and Hemerijck, 2003). As a result, governments must carefully manage their budgets, balancing strict financial constraints with the need for greater cost-effectiveness. Moreover, the last decades (the temporal focus of this Special Issue) not only saw ongoing permanent austerity but also a specific and intense fiscal austerity following the 2007–2008 global financial crisis. Across Europe, governments increasingly turned to the public sector (and public employment) to pursue internal devaluations and fiscal austerity to achieve macroeconomic adjustment (Bach and Bordogna, 2016; Di Carlo and Molina, 2024).
Finally, job quality − particularly in terms of working conditions and wages − is a key issue in care labour markets for two main reasons. Attracting and retaining workers in the sector depends heavily on ensuring adequate working conditions (Armstrong and Braedley, 2023; OECD, 2023). Furthermore, given the labour-intensive and relational nature of care work, poor working conditions can directly affect the quality-of-service provision (Eurofound, 2023; OECD, 2020).
The care trilemma framework allows us to analyse not only the level and configuration of each pole but also their interrelations, the degree of tension between them, and the main actors associated with each one: households for the first, governments for the second, and workers, providers, and their representatives for the third.
From a labour market regulation perspective, the care trilemma can be addressed in three distinct ways. Each approach reflects a different configuration and leads to varying outcomes in terms of working conditions and job quality within the care sector.
First, a generalised improvement in working conditions − referred to as a ‘high road’ approach to care labour market regulation − can be pursued through different strategies. One option is to allocate additional public resources specifically to enhance wages and working conditions while maintaining existing coverage levels. Alternatively, governments may opt for a recalibration strategy, redirecting funds from other areas of the education or social protection systems (such as pensions or healthcare) to invest more heavily in the care sector and in its workers.
While the ‘high road’ approach focuses on improving working conditions, two alternative solutions represent different forms of a ‘low road’ to care labour market regulation.
Second, a dualisation of working conditions. In this scenario, public funding is primarily directed toward expanding service coverage, while overall financial resources for wages and working conditions remain stable or even decrease. However, instead of applying uniform standards across the sector, policymakers – and the social partners − may choose to prioritise job quality protection in certain segments of the care workforce while sacrificing it in others. This form of dualisation can occur through various mechanisms, including (i) increasing of services through private provision, leading to poorer employment conditions in the private sector compared to the public one; (ii) the development or reinforcement of informal or non-regular care markets (e.g. reliance on family caregivers or domestic workers instead of trained professionals); (iii) clear segmentation within the care workforce, where more professionalised roles (e.g. nurses and kindergarten teachers) enjoy stronger protections than less recognised and/or less qualified roles (e.g. personal care workers and nursery educators); (iv) regional disparities in working conditions, particularly in countries with federal or highly decentralised administrative systems.
Third, a generalised sacrifice of working conditions. In this scenario, improving coverage becomes the sole priority, and working conditions are broadly downgraded. This can occur either in a context of stable public expenditure or, in compliance with fiscal balance constraints, when increased funding is directed toward expanding the number of care beneficiaries, without any parallel investment in job quality or employment standards.
How countries solve the care trilemma: Two hypotheses
Over the past decades, all EU countries have been confronted with the challenges of addressing the care trilemma. This article − and the whole Special Issue − focuses on the first two decades of the 2000s, a period characterised by significant expansion in both ECEC and LTC sectors. Rather than offering an exhaustive mapping of national cases, the analysis identifies broader patterns and dynamics in the evolution of job quality and working conditions in care services across Europe, to assess the extent to which these trends reflect the structural determinants underpinning the current, acute labour shortages. Particular attention is given to the configuration of industrial relations institutions and actors.
Hypothesis 1. We expect that, during the first decades of the 2000s, countries addressed the care trilemma by (partially) sacrificing wages and working conditions in favour of the other two goals. This reflects a predominance of what we defined as ‘low road’ solutions. The growing demand for care services increased public intervention in service provision. At the same time, after the 2008–09 economic crisis, fiscal consolidation became a central priority for many EU countries (Bach and Bordogna, 2016). In this context, European and national institutions often introduced measures to reduce public sector service costs, seen as the quickest route to restoring public finances.
However, cuts to public investment in care services can face strong resistance from citizens acting as users, taxpayers, and voters. As voters, they may pressure governments to expand service coverage and penalise agendas that reduce investment. By contrast, actors directly involved in the third dimension of the care trilemma − job quality − often exert a weaker influence. This is particularly the case for trade unions representing ‘weak’ labour market segments, such as care workers, who in many countries are characterised by low-to-medium professionalisation, limited institutional support, and high replaceability due partly to medium-low educational entry requirements. These workers are typically represented by large, encompassing unions (Olson, 1965), which must reconcile and prioritise their interests alongside the diverse demands of a heterogeneous membership base, often spanning the entire public sector (Bordogna, 1994).
As a result, care workers’ structural power is comparatively weak, especially relative to other professional groups in the same sectors (such as physicians, teachers, and, to some extent, nurses) whose representative bodies − typically professional associations and craft unions − exercise greater bargaining power by organising a highly qualified, narrow, and relatively homogeneous workforce through structures resembling ‘special interest groups’ (Bordogna, 1994; Olson, 1965). We therefore expect the ‘job quality’ pole to be more compromised than the others, reflecting the weaker political voice of those advocating for it and their logic of representation.
Hypothesis 2. Different institutional traditions − especially those related to employment relations − shape how each country addresses the care trilemma, influencing not only the choice between ‘high’ and ‘low’ road strategies but also the specific form that a ‘low road’ approach takes. On the industrial relations side, we hypothesise that two key dimensions shape whether countries follow a ‘high-road’ or ‘low road’ approach: the nature of the employer and the existence of intra-sectoral and cross-sectoral (public/private) coordination mechanisms.
Comparative industrial relations research highlights structural differences between public and private sector labour regulation, which generate divergent outcomes in wages and working conditions (Mori, 2024). Public sector employers operate under different constraints and logics from private actors, and employment relations in the public sector follow distinct regulatory frameworks (Bach and Bordogna, 2016; Di Carlo and Molina, 2024). As widely documented, employment conditions are generally higher and better protected in the public sector than in the private sector for comparable positions within the same sector (Mori, 2017).
However, the presence of intra-sectoral (within public or private sectors) and cross-sectoral (between public and private sectors) coordination mechanisms can reduce − or even eliminate − these disparities by aligning working conditions across the broader labour market. Legal or administrative provisions for the erga omnes extension of sectoral collective agreements ensure not only high collective bargaining coverage but also uniform working conditions across the care sector, regardless of whether employment is public or private. Conversely, the absence of such mechanisms can produce fragmented and uneven conditions across different segments of the sector. Likewise, highly coordinated employment relations systems − characterised by cross-sectoral encompassing bargaining structures, such as pattern bargaining or inter-sectoral regulatory coordination − are expected to promote higher job quality and greater uniformity of working conditions across the care market, irrespective of the nature of the employer.
On the social policy side, the expansion of care policies in recent decades has occurred across different welfare regimes. Saraceno and Keck (2010) identify three main approaches to ECEC and LTC policies that have traditionally distinguished European countries: familialism by default, supported familialism, and defamilialisation.
In the familialism by default model, public policies do not acknowledge a right to care support, leaving the full burden of care on households, with little or no state involvement. As a result, governments do not promote the development of professional care services, limiting job creation and investment in this sector.
In supported familialism, households receive financial assistance − cash transfers and parental (typically maternal) leave − while close relatives are still expected to provide care. This model also limits the expansion of professional care services, as public support is directed toward enabling informal care, often reinforcing traditional gender roles.
By contrast, defamilialisation occurs where public policies directly support households through the provision of formal care services. Here, governments invest in the development of professional care infrastructure, fostering formal employment, better working conditions, and the institutionalisation of care as a labour market sector.
As noted above, the growing expansion of care services in recent decades has led countries that previously followed familialism by default or supported familialism models to (partially) shift away from approaches that relied primarily on informal household care. However, according to a path dependency approach, the pace and trajectory of this shift can vary depending on the original model (Streeck and Thelen, 2005). Countries with a previous defamilialisation approach might have placed greater emphasis on regulating and improving working conditions (for LTC, see Arlotti and Neri, 2023). In contrast, those transitioning from the other two models might have focused more on expanding the care workforce in quantitative terms than on enhancing job quality.
Factors associated with ‘high road’ and ‘low road’ approaches to the care trilemma.
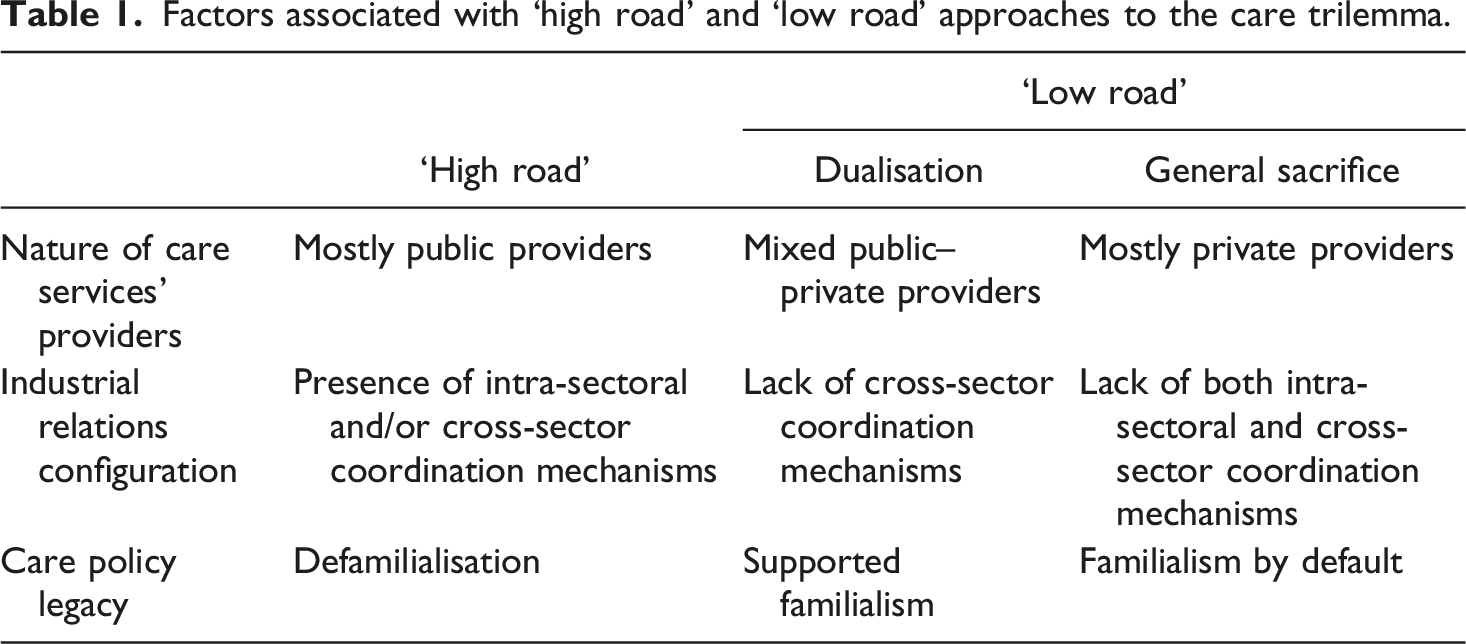
We expect that a ‘high road’ solution is more likely under three conditions: the presence of mostly public care providers; the presence of intra-sectoral and/or cross-sector coordination mechanisms; and a previous policy legacy based on care defamilialisation.
We expect that a ‘low road’ based on a dualisation of working conditions path is more likely under three conditions: a mixed public–private provision, the lack of cross-sector coordination mechanisms, and a care policy tradition based on supported familialism.
Finally, we expect a ‘low road’ centred on a general sacrifice of working conditions to be more likely under three conditions: a mostly private provision; the lack of both intra-sectoral and cross-sector coordination mechanisms; and a care policy tradition of familialism by default.
Data and methods
The empirical section of this study draws on two main sources of information and methods: a quantitative analysis and a qualitative case study-based one.
We used quantitative data from various sources, primarily Eurostat, the OECD, and the European Commission. The quantitative analysis includes 22 European countries: the United Kingdom and all EU member states, except for the three Baltic states (Estonia, Latvia, and Lithuania), Croatia, Cyprus, and Malta. These countries were excluded due to data limitations.
To operationalise the three dimensions of the care trilemma − expenditure, coverage, and working conditions − we used the following indicators.
Public expenditure. Public spending on LTC and ECEC, expressed as a share of GDP.
Needs’ coverage. For LTC, the proportion of people aged 65+ receiving home or residential care. For ECEC, participation rates for children under 3, and for children aged 3 to the minimum compulsory school age, calculated as the share of children in each age group enrolled in formal services.
Working conditions and job quality. For LTC, hourly wages of LTC care workers as a share of the national average wage and LTC workforce density (number of LTC workers per 1000 people aged 65+). For ECEC, wage levels of pre-primary school teachers and professional educators (for those countries that do not employ school teachers at this level) as a share of earnings for full-time, full-year workers with tertiary education and ECEC workforce density, expressed as the child-to-staff ratio in services for both age groups (under 3, and 3 to minimum compulsory school age).
Data were collected at two points in time: the mid-2000s (typically 2005 or 2007) and the most recent available information (with most data referring to 2022). For the UK, the most recent available data refer to 2019. The results of this quantitative analysis are presented in Section 5.
We also conducted a comparative and synthetic analysis of the core findings from the other contributions included in this Special Issue. This qualitative assessment not only complements our empirical investigation but also serves to introduce and contextualise the contents of the individual articles. The timespan covered by such qualitative assessment reaches more recent years than the quantitative one (in particular, the end of 2025). The results of this part of the analysis are presented in the next section.
Findings: A quantitative overview of the solutions to the care trilemma in Europe
This section presents the empirical analysis based on quantitative data covering a broad set of European countries. The analysis is organised in three steps. First, we present a classification of national care models based on levels of public expenditure and service coverage in ECEC and LTC across European countries in the early 2020s. Second, we offer an examination of how these care models perform in terms of wages and working conditions, depending also on the nature of employers and the presence of coordination mechanisms in labour regulation. Third, we show a diachronic analysis of the evolution over time of the configuration of the three poles of the care trilemma within these models.
A classification of care models based on public expenditure
The care models: public expenditure and coverage rates in LTC and ECEC.
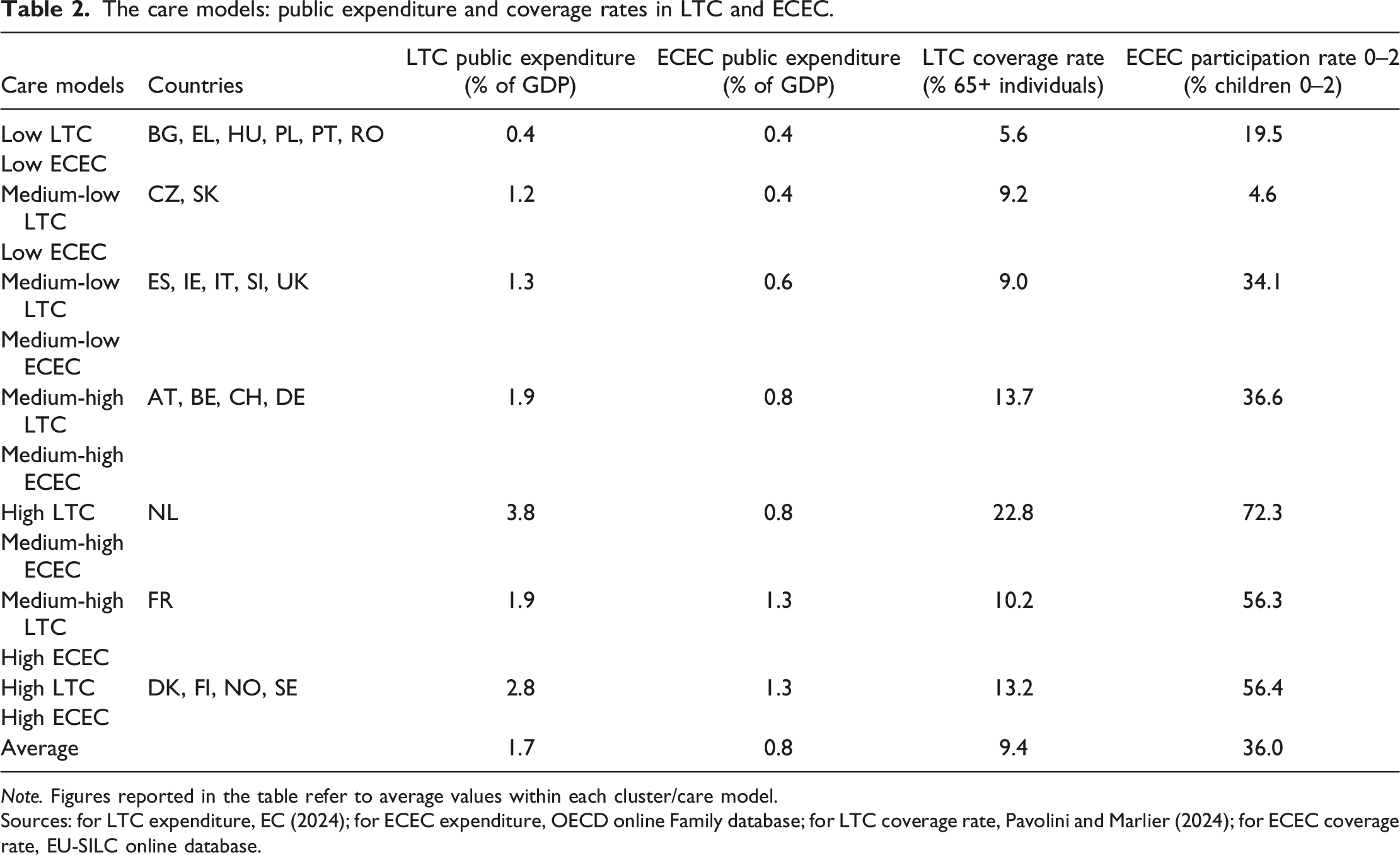
Note. Figures reported in the table refer to average values within each cluster/care model.
Sources: for LTC expenditure, EC (2024); for ECEC expenditure, OECD online Family database; for LTC coverage rate, Pavolini and Marlier (2024); for ECEC coverage rate, EU-SILC online database.
Assessing care models in terms of working conditions
Care models and working conditions.
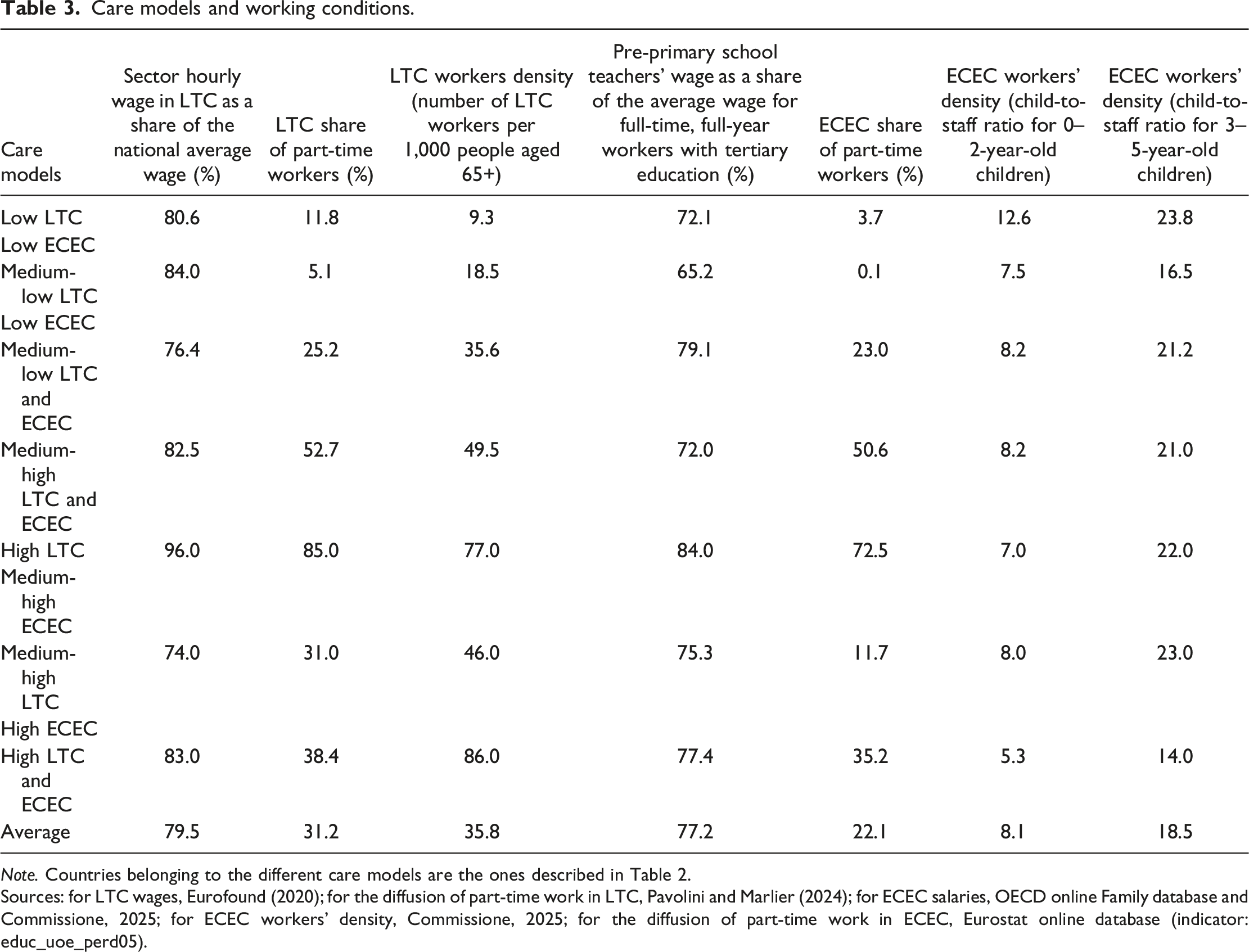
Note. Countries belonging to the different care models are the ones described in Table 2.
Sources: for LTC wages, Eurofound (2020); for the diffusion of part-time work in LTC, Pavolini and Marlier (2024); for ECEC salaries, OECD online Family database and Commissione, 2025; for ECEC workers’ density, Commissione, 2025; for the diffusion of part-time work in ECEC, Eurostat online database (indicator: educ_uoe_perd05).
Moreover, a high incidence of part-time work is observed in many countries. The combination of low hourly wages and widespread part-time employment increases the risk of in-work poverty for many care workers. For example, while the Netherlands records the highest hourly wages in the LTC sector, the near-universal prevalence of part-time contracts results in relatively low monthly earnings. When wage levels and part-time employment are considered jointly, countries typically fall into one of the two groups: those offering low wages overall (e.g. many CEE countries) and those offering higher hourly wages (sometimes comparable to national averages, as in the Netherlands) but with widespread part-time employment.
Differences among care models are more pronounced regarding workload. Here, a clearer relationship emerges between public expenditure levels and staffing ratios. Countries with lower care spending tend to have higher staff-to-beneficiary ratios − suggesting heavier workloads per worker − whereas Nordic countries, which invest more in care, exhibit lower ratios and thus lighter individual workloads.
Nature of employers and the role of collective bargaining in the care sector.
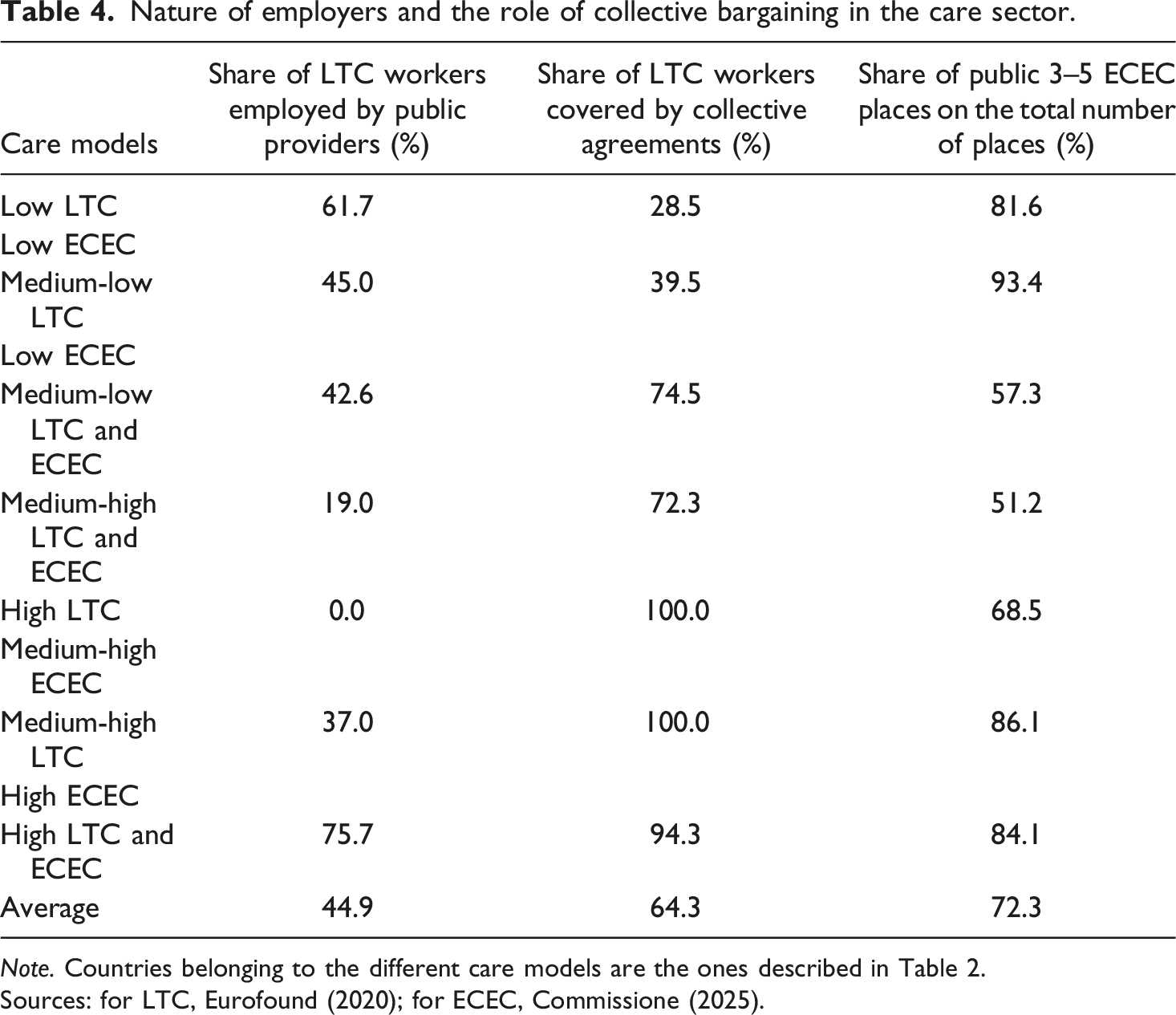
Note. Countries belonging to the different care models are the ones described in Table 2.
Sources: for LTC, Eurofound (2020); for ECEC, Commissione (2025).
Data on collective bargaining (CB) coverage are available only for LTC workers. Here, a distinct pattern links care models with levels of CB coverage. The latter is lowest in CEE countries, moderate (though not universal) in models characterised by medium-low or medium-high public expenditure, and highest in countries with high levels of care expenditure. These findings underscore the role of CB institutions in shaping job quality and working conditions.
The diachronic evolution of the three poles of the care trilemma
Public expenditure, coverage, and working conditions in the care sector over time in Europe.
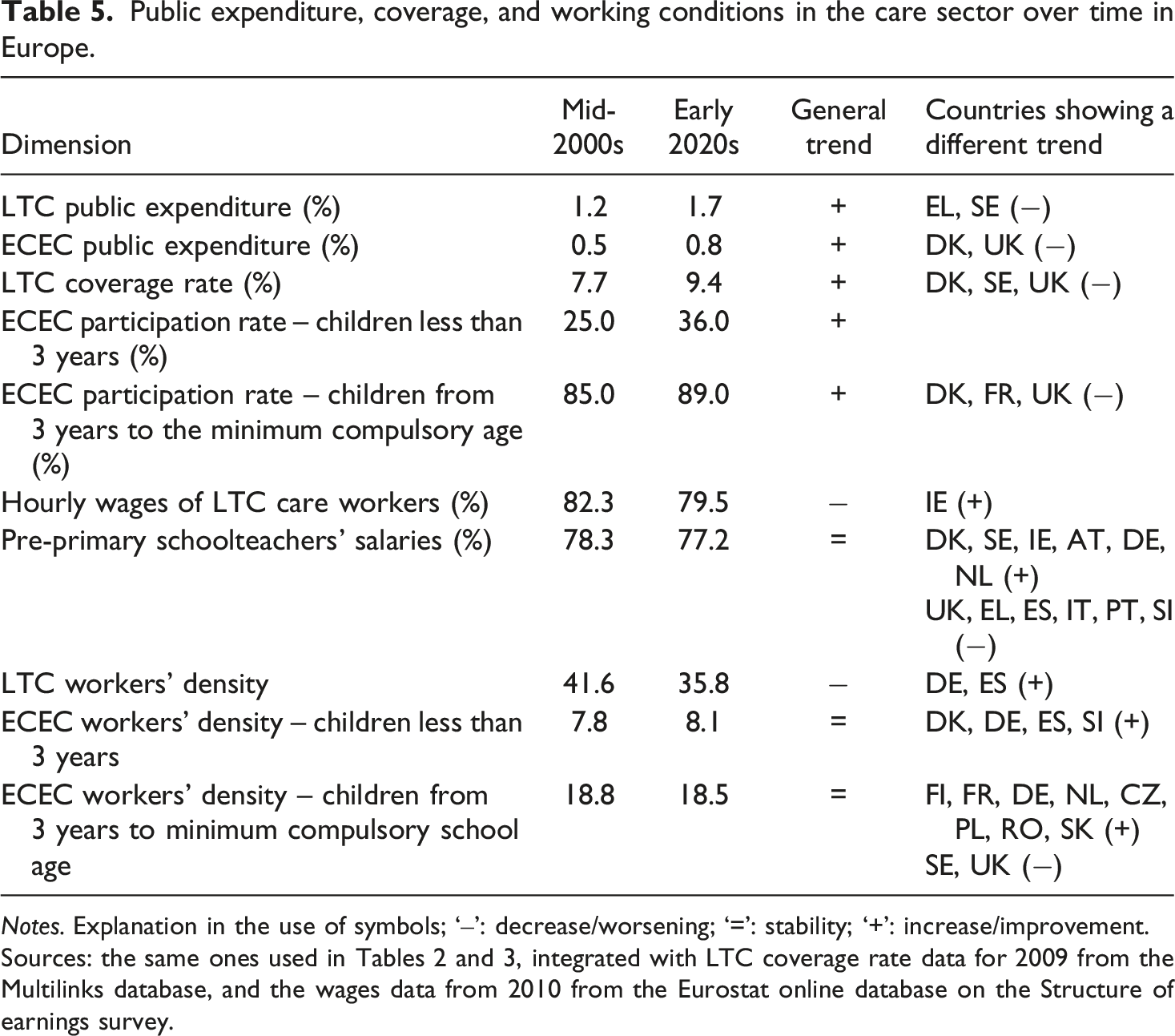
Notes. Explanation in the use of symbols; ‘‒’: decrease/worsening; ‘=’: stability; ‘+’: increase/improvement.
These features of the care labour market were consistently observed in the LTC sector across care models and countries, with very few exceptions. By contrast, working conditions in ECEC services followed a more heterogeneous trajectory across Europe. In other words, the sub-sector itself seems to play a significant role in shaping how the care trilemma has been addressed over time. While a ‘low road’ approach has been the predominant outcome in LTC across most models, the ECEC sector presents a more varied picture. Some countries have followed a ‘low road’, while others − mainly those associated with medium-high or high levels of public expenditure on ECEC − have witnessed improvements in working conditions.
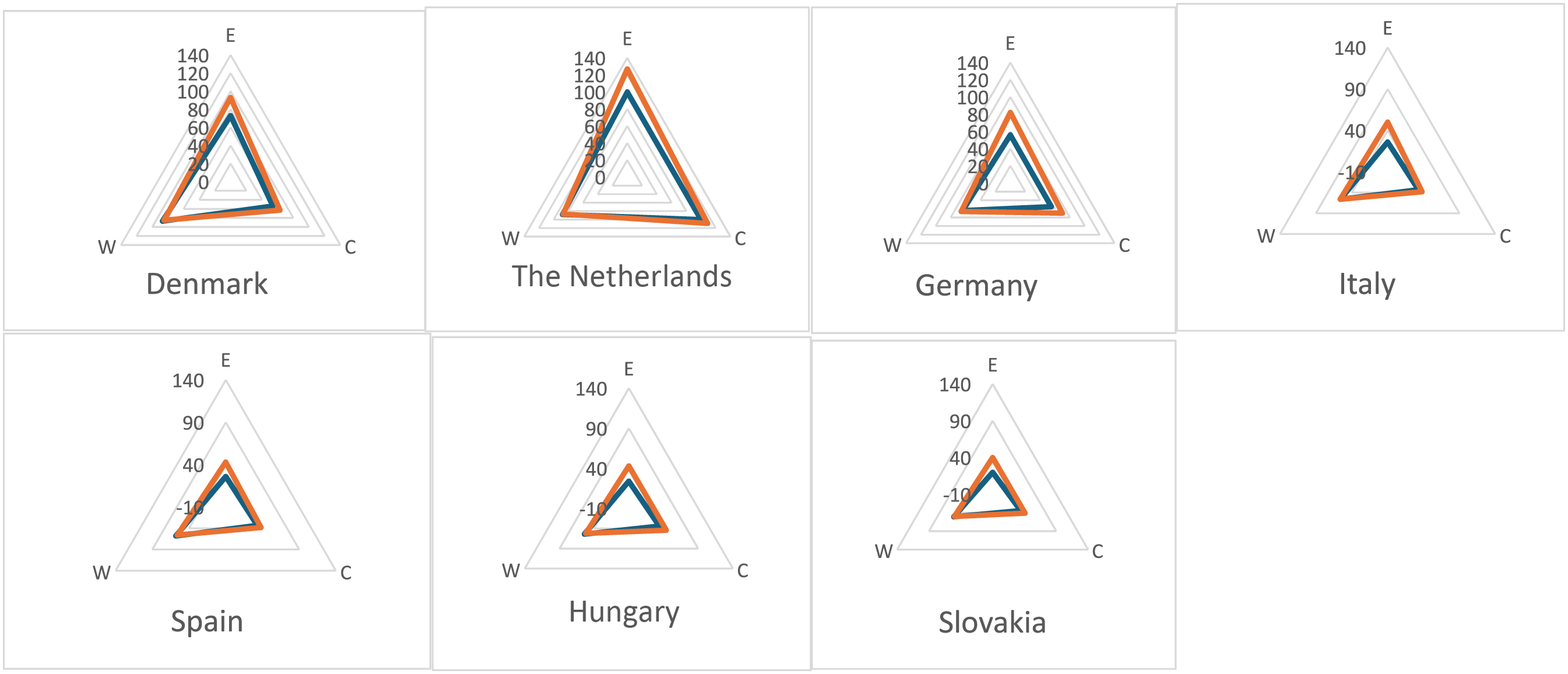
Figures 1 and 2 summarise for the seven countries involved in this special issue how the trilemma was squared, respectively, in LTC and ECEC over time. All countries’ values reported in Tables 2, 3, and 5 (expenditure, coverage, and working conditions – expressed in terms of salaries and workload) have been standardised in a 0–100 scale for 2005. 100 has been assigned to the country with the ‘best performance’ in 2005 (e.g. the highest LTC coverage rate among the countries included in Table 2). As it can be seen, practically most countries increased coverage and, often, expenditure, but working conditions did not improved or, eventually worsen. Squaring the trilemma in LTC over time. Squaring the trilemma in ECEC over time.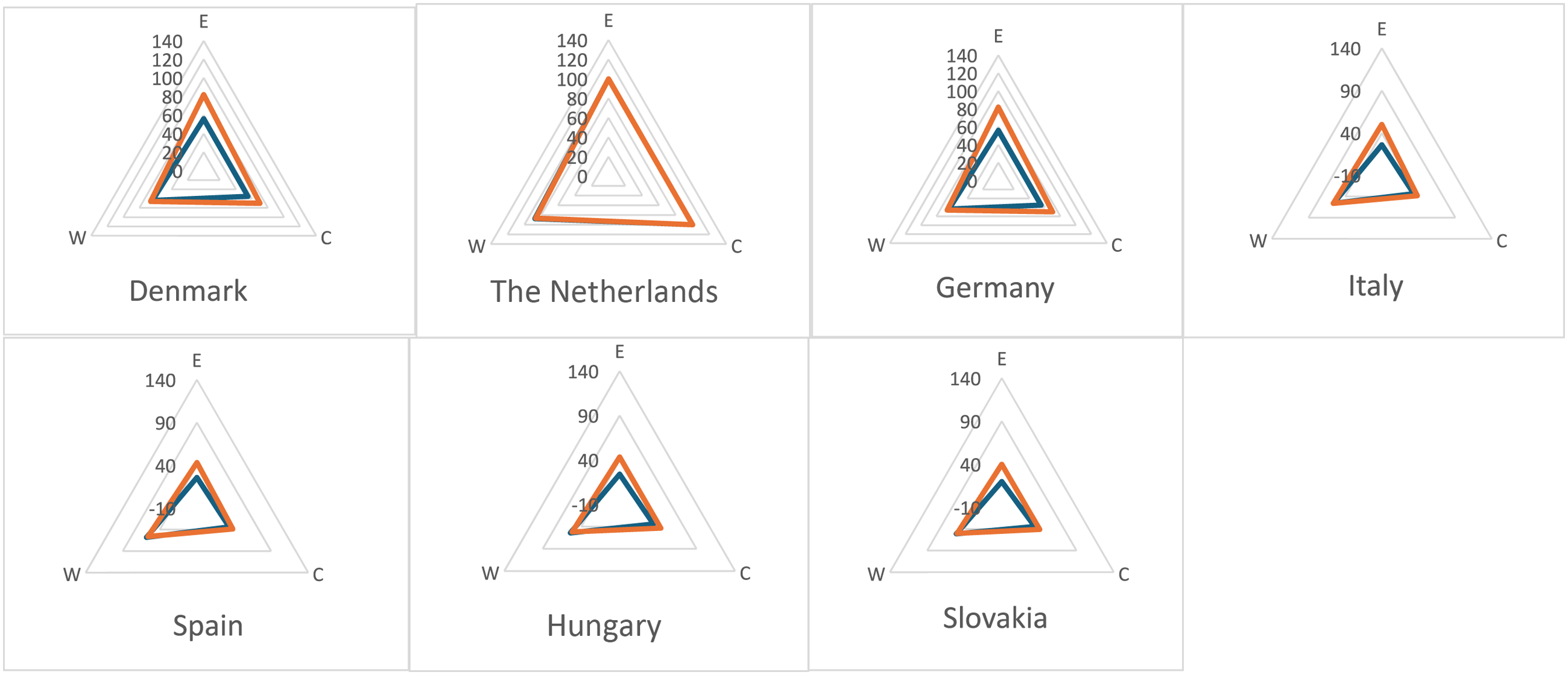
Findings: Evidence from the country in-depth case studies
The analysis presented in the previous section supports the hypothesis that the care trilemma has been resolved primarily at the expense of working conditions, following a ‘low road’. This finding reinforces our argument that poor job quality − particularly in terms of workload and wages − constitutes a key driver of both the growing labour shortages and the persistently low occupational attractiveness of the care sector in Europe. However, the quantitative analysis leaves two core questions unresolved. First, what explains both the commonalities and the differences in the trajectories of job deterioration across countries and care sectors? While we advanced hypotheses on these dynamics, the available quantitative data did not allow us to test them directly. Second, what type of ‘low road’ characterises different countries: a dualised trajectory or a more generalised deterioration in working conditions? And which factors account for these divergent pathways?
To address these questions, this section systematises the findings from the national case studies included in this Special Issue through a comparative perspective. The selected countries cover almost the full range of care models identified in the previous section: Hungary and Slovakia represent cases of low expenditure; Italy and Spain medium-low; Germany medium-high; and the Netherlands and Denmark high expenditure in both sectors. We first provide a qualitative overview of the main developments in working conditions and job quality across the seven countries, offering a more nuanced cross-country and cross-sector comparison than the quantitative analysis. The focus is on three core dimensions: wage levels, horizontal wage dispersion, and workload. Second, we examine the factors accounting for the cross-national and cross-sectoral variations observed in the resolution of the care trilemma, with particular attention to the extent to which working conditions are compromised.
The working conditions in LTC and ECEC
Changes in working conditions in the LTC and ECEC from the mid-2000s to 2025.
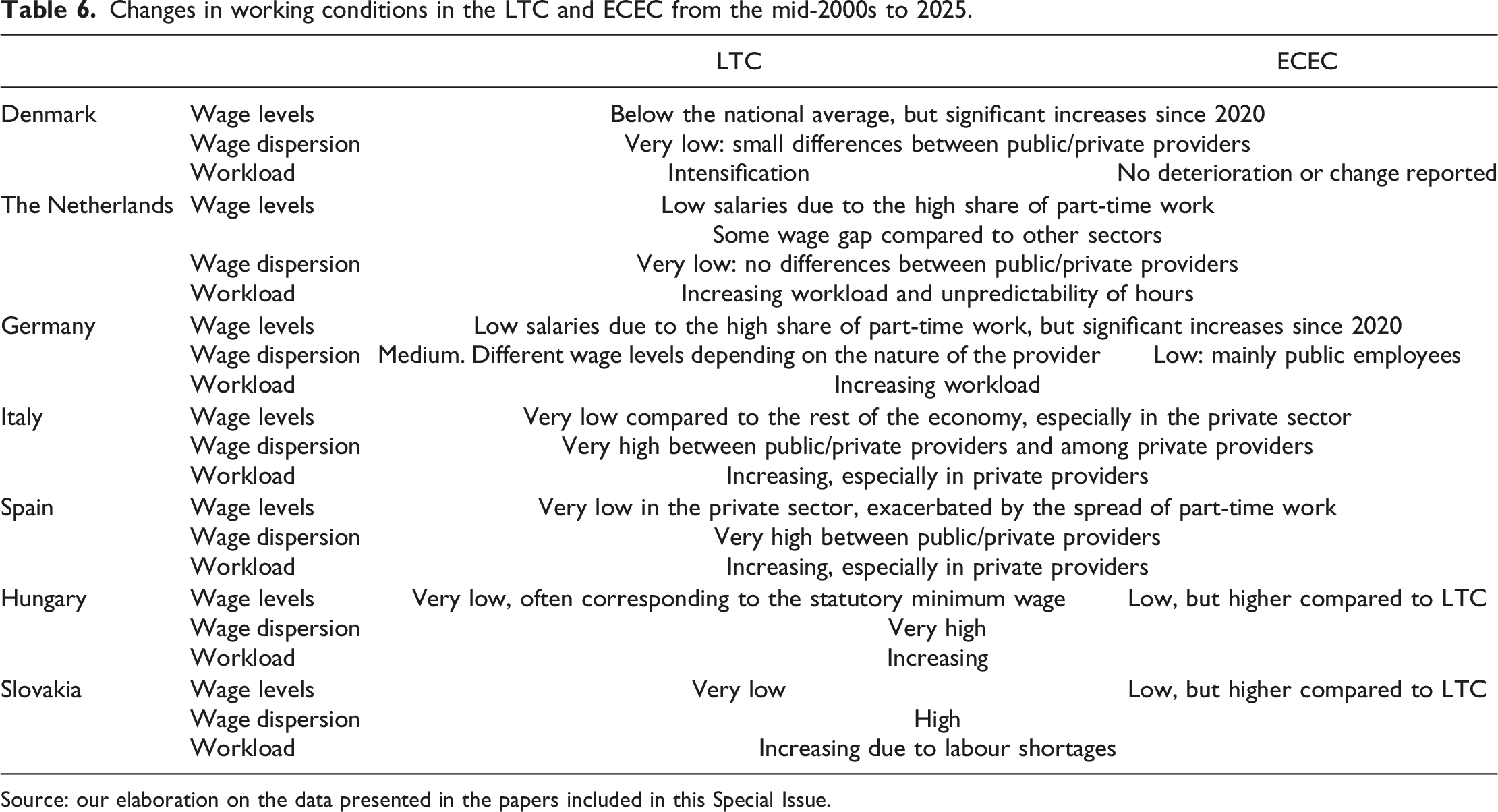
Source: our elaboration on the data presented in the papers included in this Special Issue.
Nevertheless, the case studies also reveal important differences between ECEC and LTC, with the latter consistently exhibiting, comparatively, poorer working conditions. Table 6 reports qualitative evidence for the seven countries examined that is not captured by the quantitative indicators, shedding light on the nature and direction of recent changes in working conditions. A common trend in most of the countries is a more severe weakening of working conditions in LTC compared to the ECEC. A key driver of this deterioration is the intensification of workloads that occurred over the past decade for several reasons. Labour shortages constitute an important factor of such intensification: recruiting and retaining staff has become increasingly challenging, and those who remain in the sector must absorb the additional workload. As illustrated by the Danish case, this situation is compounded by the entry of less-trained LTC workers, which further increases the pressure on more experienced staff (Mailand et al., 2026). Another factor contributing to poor and worsening working conditions in several countries (e.g. the Netherlands, Spain, and Italy) is the widespread adoption or strengthening of public procurement practices in LTC, in contrast to ECEC (Molina et al., 2026). The increasing marketisation of LTC services has intensified price competition among providers, leading to continuous work intensification and a deterioration of working conditions − particularly in terms of wage levels.
The configurations of industrial relations systems and the different ‘low roads’ solutions to the care trilemma
Factors associated with the type of ‘low road’ followed.
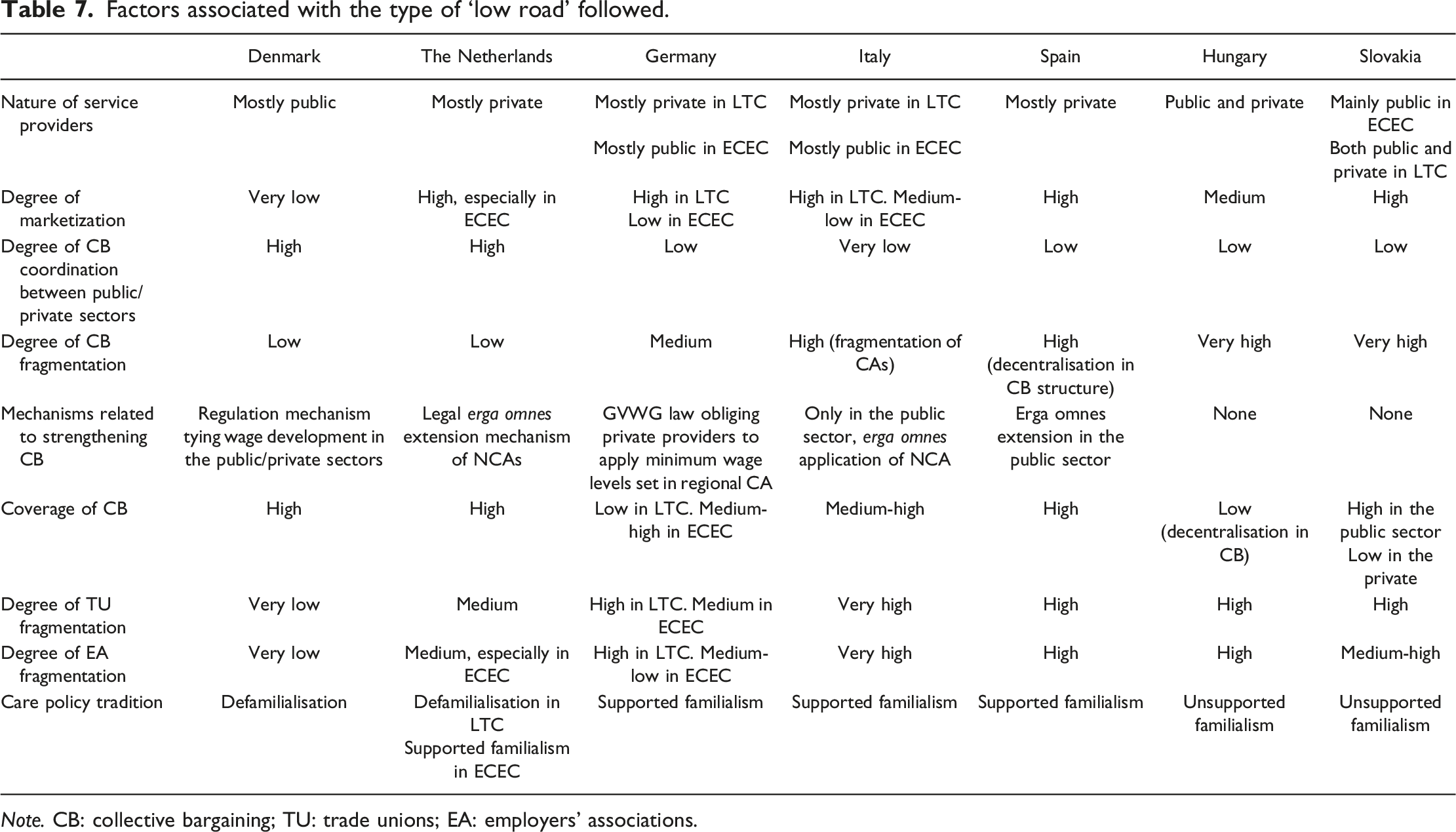
Note. CB: collective bargaining; TU: trade unions; EA: employers’ associations.
The configuration of industrial relations in this sector plays a crucial role in shaping the specific ‘low road’ trajectory pursued, and, consequently, the extent to which groups of care workers experience deteriorating working conditions. More specifically, encompassing, centralised, and coordinated collective bargaining systems − such as those in Denmark and the Netherlands − matched by a defamilialisation care legacy (especially in the former country), mitigated overall the deterioration of working conditions in care services (Mailand et al., 2026). These systems, associated with a relatively low level of marketization (especially in Denmark), ensured a comparatively robust level of protection and prevented the emergence of pronounced dualisation between the public and private sectors. This trend was facilitated by the low fragmentation in collective representation on both the union and employer sides (particularly in the Danish case), which contributed to ensuring a relatively uniform level of protection and representation. Nevertheless, even within these institutional settings, the pressures associated with the other two poles of the trilemma − budgetary constraints and service coverage − still resulted in a degree of deterioration in working conditions, albeit to a lesser extent than in other countries. They experienced a marked intensification of workloads, with wage levels that remain systematically below national averages, albeit with recent wage increases, as in the case of Denmark. Contrary to our hypothesis, which envisaged that coordinated and centralised industrial relations configurations embedded in welfare systems characterised by a defamilialisation care policy orientation would follow a high-road trajectory, our findings show that the care sector deviates from this expectation. Instead, it appears to be moving along a ‘low road’ path, albeit in a milder form compared to other countries.
The situation differs markedly in countries where there is, on one hand, a supported familialism care legacy, and on the other hand, collective bargaining institutions that are centralised, but less coordinated and less encompassing, as in Germany, Italy, and Spain. In these institutional contexts, the coexistence of distinct institutional frameworks regulating labour in the different segments of the care market − public, private, and, in the German case, also faith-based providers − combined with the absence of strong mechanisms for intersectoral coordination and the limited extension of collective agreements, fostered deep dualisation in working conditions (Abramowski, 2026; Molina et al., 2026 in this Special Issue). This ‘dualised “low road”’ trajectory, in line with our hypothesis, was further exacerbated by the marked fragmentation in collective representation among both workers and providers, which hindered the development of coordinated and uniform protection and representations across the care market. In contexts where care work is broadly devalued relative to the rest of the economy in terms of wage levels, the specific structure of collective bargaining, combined with a high degree of marketization, contributed to institutionalising a segmented care labour market in which labour standards in the private sector are systematically lower and less protected than those in the public sector.
A second ‘“low road”’ trajectory – the one characterised by a general sacrifice of working conditions − emerges in countries with a unsupported familialism care legacy, and industrial relations systems characterised by fragmented, highly decentralised, and weakly coordinated collective bargaining structures, in which trade unions − being poorly recognised − play only a limited role, particularly at the national and sectoral levels, defined largely at the local level in the absence of adequate mechanisms for both intra-sectoral collective bargaining coordination (among municipalities or regions) and inter-sectoral coordination (between public and private providers). This is the case of Hungary and Slovakia, where working conditions have proven to be particularly critical across the care sector, thus confirming our hypothesis of a pronounced general deterioration associated with the ‘low road’ trajectory pursued (Bors et al., 2026 in this Special Issue).
Conclusions
The analysis presented in this article shows that the severe and persistent labour shortages affecting European care systems are closely linked to how governments address the care trilemma. By examining the evolution of public expenditure, service coverage, and job quality, we show that since the turn of the XXI century, the trilemma has been resolved predominantly through ‘low road’ strategies. Across Europe, policy expansion in ECEC and LTC has prioritised the first two poles of the trilemma − service coverage and fiscal sustainability − while systematically sacrificing the third, namely, job quality. Albeit with some caveats across the two subsectors, service expansion has consistently outpaced investments in wages, staffing levels, and professionalisation, resulting in low occupational attractiveness and increasing work intensification. As a result, labour shortages in the care sector should not be interpreted as a temporary labour market mismatch or a delayed supply response to growing demand. Rather, they reflect the institutional equilibrium through which the care trilemma has been managed, in which care work has been persistently undervalued.
At the same time, our findings highlight important cross-sectoral differences in how the care trilemma was resolved. While the ‘low road’ trajectory is particularly pronounced in LTC, developments in ECEC appear more heterogeneous. Although wages remain below those of comparable occupations and workloads have intensified, some countries registered improvements in staffing ratios and salary levels over the past decade. This suggests that the institutional configuration of the sector itself – particularly in terms of care policy legacy, level of public expenditure, and degree of marketisation − plays an important role in shaping how the trilemma is addressed.
Furthermore, the analysis shows that countries do not follow a single ‘low road’ trajectory in resolving the trilemma; instead, two distinct patterns emerge. In some countries − particularly those with fragmented industrial relations systems and weak collective actors − the trilemma has been addressed through a generalised sacrifice of working conditions, with deteriorating employment standards across the entire care workforce. In others, especially where collective bargaining remains centralised but poorly coordinated across public and private providers, the resolution of the trilemma has taken the form of a dualised ‘low road’, characterised by growing segmentation between different groups of care workers and between public and private provision. By contrast, countries with more encompassing and coordinated industrial relations institutions − such as Denmark and, to a lesser extent, the Netherlands − have mitigated these dynamics. Nevertheless, even in these institutional settings, the care trilemma has not been resolved through a genuine high-road strategy, as hypothesised. Although job quality has been relatively better protected, working conditions remain weaker than in other sectors of the economy, and workload pressures have intensified.
Overall, these findings suggest that differences in the resolution of the care trilemma are explained less by levels of public expenditure and care policy legacies alone than by the institutional configuration of industrial relations systems and actors. The degree of coordination in collective bargaining, the fragmentation of worker and employer representation, and the extent of marketisation in service provision shape whether countries follow a dualised or generalised ‘low road’ trajectory in job quality, while prioritising service coverage in addressing the trilemma.
Overall, this article and the Special Issue aim to open a research agenda that places care work at the centre of industrial relations scholarship. Three main avenues for future research emerge.
First, the findings highlight the need for a more systematic investigation into the politics of job quality in public services and, from this perspective, the care trilemma provides a useful analytical lens for understanding the tensions shaping the development of public services’ labour markets. While industrial relations research has long examined the effects of marketisation, outsourcing, and the erosion of collective bargaining on working conditions, the care sector offers a particularly revealing testing ground. Its hybrid governance, highly gendered workforce, and rapid policy expansion make the mechanisms of job-quality deterioration especially visible.
Second, care work challenges conventional assumptions about worker power and collective representation. Compared with healthcare and education, the care sector combines low professional status, gendered norms, and high labour replaceability, weakening the structural and associational power of trade unions. This calls for renewed attention to how power resources operate in highly feminised and hybrid public–private service sectors. Future research should therefore explore emerging forms of worker voice, mobilisation, and coalition-building.
Finally, as shown by Galetto and Neri (2026) in this Special Issue, the growing role of the European level in shaping these dynamics deserves closer attention. Recent EU initiatives − including the Directive on adequate minimum wages, the European Care Strategy, the revitalisation of collective bargaining, the creation of the European Sectoral Social Dialogue Committee for Social Services, and the governance mechanisms of the European Semester − signal a more active EU role in promoting labour standards and strengthening social partner capacity. Although national institutions remain central, EU-level initiatives may gradually reshape the politics of the care trilemma by encouraging upward convergence in job quality.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Findings of this paper are drawn from the project funded by the EU Commission – DG Employment, Social Affairs and Inclusion ‘SOWELL – Social dialogue in welfare services. Employment relations, labour market and social actors in the care services’ (GA VS/2020/0242).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.