
Abstract
Background
Delayed neurological complications are an important cause of disability after acute carbon monoxide (CO) poisoning, but an effective pharmacological preventive treatment has not been established. Acetylcysteine may reduce oxidative injury after CO exposure and could therefore lower the risk of later cognitive deterioration.
Methods
In this single-blinded randomized pilot trial, 63 adults with acute CO poisoning were assigned to receive either intravenous acetylcysteine at 300 mg/kg/day for 3 days or placebo, in addition to standard hyperbaric oxygen. The primary outcome was delayed cognitive deterioration, measured as change in Mini-Mental State Examination category between recovery from the acute episode and 3-month follow-up, signaling worsening cognitive status.
Results
In the intention-to-treat population, delayed cognitive deterioration occurred in 2 of 31 patients (6.5%) in the acetylcysteine group, and in 5 of 32 patients (15.6%) in the placebo group. The difference did not reach statistical significance (odds ratio: 0.37, 95% CI: 0.07–2.08, Fisher’s exact p=0.426). No serious adverse effects were observed.
Conclusion
Adjunctive intravenous acetylcysteine did not significantly reduce delayed cognitive deterioration in this pilot study. Any apparent inter-group difference should be interpreted cautiously given the limited sample size and the MMSE-based outcome definition. Further studies with larger samples and more standardized outcome assessment are needed.
Keywords
Introduction
Carbon monoxide (CO) poisoning is a significant public health concern, leading to substantial morbidity and mortality worldwide. 1 The harmful effects of CO arise through its strong competition with oxygen for the binding sites on hemoglobin, leading to decreased oxygen delivery at the cellular level. 2 Additionally, CO often induces neurological and cardiovascular injury. 3 Among the neurological complications of CO poisoning, delayed neurological sequelae are the most common, presenting with diverse neurological, psychiatric, behavioral and cognitive disorders. 2 However, the pathogenesis of delayed neurological sequelae remains poorly understood. Proposed mechanisms include ischemia-reperfusion injury, mitochondrial dysfunction, and immune-mediated injury.3–16
CO poisoning generates oxidative stress by inducing the production of reactive oxygen species (ROS).4–12 CO disrupts mitochondrial enzyme function, causing electron leakage and subsequent formation of ROS, which in turn damage cellular components, including lipids, proteins and DNA. Additionally, CO depletes the body’s antioxidant defenses by interfering with the activity of heme oxygenase-1 (HO-1), a critical antioxidant enzyme. This interference reduces the body’s ability to scavenge ROS, thereby exacerbating oxidative stress. In summary, beyond hypoxia, oxidative stress caused by CO contributes to extensive cellular injury, underscoring the need for further research into therapeutic strategies that reduce oxidative stress. Furthermore, oxidative stress may also intersect with inflammatory and immune-mediated pathways that contribute to delayed white matter injury and demyelination after CO poisoning. Therefore, therapies that replenish glutathione and reduce reactive oxygen species, such as acetylcysteine, may attenuate one component of this delayed injury pathway, even though the overall pathogenesis is likely multifactorial.
Currently, high-concentration normobaric oxygen therapy and hyperbaric oxygen (HBO) are widely accepted as standard treatments for CO poisoning, although the efficacy of HBO in reducing delayed neurological sequelae remains debated.3,17–19 Many studies suggest that antioxidants may hold promise for the treatment of CO poisoning,3,20 as therapies targeting oxidative stress induced by CO poisoning appear to be effective.21–24 Clinical studies also indicate that antioxidants may help mitigate neurological sequelae following CO poisoning.25–27 Among the antioxidants, acetylcysteine stands out as a well-known treatment with significant potential. Acetylcysteine acts as a glutathione precursor, replenishing cellular antioxidant capacity and scavenging ROS. 28 Its well-documented safety, accessibility and neuroprotective potential make it a strong candidate for the treatment of oxidative stress-related diseases. 29 In an animal study, acetylcysteine significantly reduced brain tissue damage caused by CO poisoning. Microscopic examination revealed that while all rats in the control group exhibited brain damage, only 3 out of 9 rats in the acetylcysteine group did so. These findings highlight acetylcysteine’s potential neuroprotective effects with regard to CO-induced brain damage. 21 Moreover, acetylcysteine’s antioxidant and anti-inflammatory properties have been extensively studied in the context of other neurological disorders, such as traumatic brain injury and neurodegenerative diseases.30–32 The effects are largely attributed to its antioxidant and cell-protective functions.
Our study aimed to evaluate whether the addition of acetylcysteine to HBO therapy could reduce delayed cognitive deterioration, one component of neurological sequelae, in patients with acute CO poisoning.
Methods
Study design and setting
This single-blinded, randomized controlled trial was conducted from January 2018 to July 2019 in the emergency department of China Medical University Hospital, a tertiary medical center in central Taiwan. The emergency department has an annual census of approximately 140,000 visits, and CO poisoning accounts for about 100 visits per year. At our institution, conventional management for CO poisoning consisted of normobaric oxygen therapy for 3 days and a single session of HBO.
For the study, a contemporaneous, written institutional study protocol, including a general statistical analysis plan, was drawn up before enrollment began in January 2018, and was approved by the Institutional Review Board of China Medical University Hospital (CMUH106-REC2-154). Target clinical outcomes, follow-up framework, and analysis populations were defined before outcome data were reviewed. After enrollment began, no further amendments to protocol affecting the target clinical outcome or follow-up framework were made. The final analyses were conducted after the completion of data collection. This trial was not prospectively registered in a public clinical trial registry, and at the time of study initiation, trial registration had not been incorporated into our local workflow for investigator-initiated pilot trials.
Participants
Patients suspected of CO poisoning were initially evaluated by emergency physicians, who reviewed the patient’s history, symptoms and carboxyhemoglobin levels. Cases that met the diagnostic criteria were then confirmed by toxicologists to ensure consistency and accuracy before enrollment in the study. The emergency physicians and toxicologists confirmed the diagnosis based on the following criteria: 1) symptomatic carboxyhemoglobin level > 10%; or 2) obvious CO exposure (e.g., charcoal-burning suicide attempt) combined with evidence of target organ injury, such as central nervous system symptoms (altered consciousness or seizures) or elevated cardiac enzymes (hs-Troponin I ≥0.02 ng/mL). We then excluded patients based on the following exclusion criteria: 1) patients with concomitant ingestion of other substances associated with high mortality risk (e.g., organophosphates, paraquat or cyanide); 2) patients with severe trauma or burn injuries in addition to CO poisoning; 3) patients for whom more than 24 hours had elapsed between poisoning and arrival at our emergency department; 4) patients younger than 20 years of age; 5) patients for whom informed consent could not be obtained; and 6) pregnant patients.
Patients who were alert and able to understand the study were approached directly for written informed consent by the toxicologist or research nurse after eligibility had been confirmed. For patients with impaired consciousness or altered mental status, informed consent was obtained from the closest available surrogate. Patients who were unconscious and had no available surrogate were not enrolled; i.e., deferred consent was not sought. Additionally, formal re-consent after recovery of decision-making capacity was not routinely obtained. This consent procedure was included in the study protocol approved by the Institutional Review Board.
Randomization
We used simple randomization to assign the participants to one of two groups, with allocation determined by a list of computer-generated random numbers prepared before enrollment. Participants were assigned to either the acetylcysteine group or the placebo group and were blinded to allocation and treatment assignment. Meanwhile, the clinical staff involved in treatment administration were not blinded to group assignment. The principal investigator held the randomization list and the numbered drug packages, and upon enrollment of each individual participant, the research nurse revealed the assignment number and opened the corresponding study package. Through this procedure, the research nurse and toxicologists involved in patient screening and enrollment were unable to predict the next assignment in advance.
Interventions
All patients in both groups received supplemental oxygen via a non-rebreather mask for 3 days following admission. HBO was administered to all patients as soon as possible after the diagnosis was confirmed in the emergency department. The HBO regimen, which was designed by pulmonologists, was 3 ATA for 90 minutes. All patients received only one HBO treatment, ensuring consistency across all participants.
Participants in the acetylcysteine group received intravenous acetylcysteine (300 mg/kg/day) for 3 days, divided into 4 doses per day. The acetylcysteine regimen was selected pragmatically based on prior toxicology experience with acetylcysteine as an antioxidant in other indications, 33 and its established intravenous safety profile in acetaminophen poisoning. 34 Participants in the placebo group received an identical volume of placebo (normal saline) for 3 days. To maintain consistency, both drugs were diluted in 100 mL sodium chloride and infused slowly over one hour to reduce the risk of allergic reactions. Although the study was single-blinded (with blinding limited to participants), the drug preparation and administration procedures were standardized across both groups. Both drugs were initiated immediately after study enrollment, with the goal of drug administration within 24 hours of CO exposure.
Outcome assessment
We collected demographic data (age, gender), physiological details, information about the CO poisoning episode, and bloodwork reports. We assessed changes in patients' cognitive function using the Mini-Mental State Examination (MMSE) at two points in time. All MMSE assessments were administered by two trained study nurses and one physician using a standard procedure, the same structured MMSE form, and the same scoring rules throughout the study. These assessors rotated in performing the tests. However, due to manpower constraints, they were not blinded to group assignment. The study nurses participated in opening the allocation assignment and administering the study drug but did not make clinical treatment decisions. The physician assessor was not involved in clinical care or treatment decisions regarding the enrolled patients.
The MMSE consisted of a 30-point questionnaire that is widely used in clinical and research settings to measure cognitive impairment.35,36 It is used to estimate the severity and progression of cognitive impairment and to follow the course of cognitive changes in an individual over time, making it a practical tool for the assessment of cognitive changes in our study. The MMSE is widely used to evaluate neurological sequelae of CO poisoning.37–39 A score of 24 or higher (out of 30) is considered normal cognition. Scores below this threshold are categorized as mild (19–23 points), moderate (10–18 points), or severe (≤9 points) cognitive impairment.
We performed the MMSE at two time points, three months apart. The first assessment was conducted after recovery from the acute poisoning phase, and before discharge, usually around hospital day 3 to 4 when the patient was able to cooperate with testing. In a small number of patients, particularly those requiring prolonged intubation, the first assessment was delayed and performed as soon as feasible before discharge. We scheduled the second assessment (the endpoint assessment) three months after the initial poisoning in an outpatient setting. We arranged monthly follow-ups either through outpatient visits or telephone calls to monitor for early signs of cognitive deterioration, and we asked patients to return early for MMSE if we discovered impairment. Otherwise, for patients without reported symptoms, we performed the MMSE at the scheduled three-month follow-up. We defined delayed cognitive deterioration as a worsening in the MMSE category between the two assessment time points; specifically, when a participant’s cognitive status declined, such as shifting from normal to mild cognitive dysfunction, or from mild cognitive dysfunction to moderate or severe cognitive dysfunction.
We originally specified the MMSE-based follow-up framework in the institutional study protocol. However, the final operationalization of the primary outcome based on the worsening of MMSE category was determined during data analysis in order to focus on clinically more substantial cognitive decline and to reduce the influence of small raw-score fluctuations that may have reflected measurement variability. While we retained the paper-based item-level MMSE source forms as part of the original study records, the analysis files recorded only the total MMSE scores and corresponding cognitive categories.
We defined complications of CO poisoning as aspiration pneumonitis, rhabdomyolysis, acute kidney injury, acute myocardial infarction, thromboembolism, or other clinically documented in-hospital complications.
Statistical analysis
We used SAS (Version 9.4, SAS Institute, Inc., Cary, NC) to analyze the data collected in this study. The target sample size was determined pragmatically based on the expected number of eligible patients at our institution during the planned recruitment period, available study resources, and the feasibility constraints of this investigator-initiated pilot trial, rather than by a formal efficacy-based sample size calculation. We presented continuous data as median (IQR), and categorical data as number (percentage), and used the Mann-Whitney U-test and chi-squared test to assess differences in baseline characteristics between the groups. We used Fisher’s exact test to compare the incidence of delayed cognitive deterioration between the groups, and considered a p-value of <0.05 as statistically significant. We performed the primary analysis in the intention-to-treat population, defined as all randomized participants according to their assigned groups, with missing outcome data conservatively assumed to indicate no cognitive deterioration. We conducted a per-protocol analysis as a supportive secondary analysis including participants who completed follow-up and received the intended intervention. As a sensitivity analysis with regard to missing outcome data, we performed a complete-case analysis including all randomized participants with available follow-up outcome assessment, regardless of protocol completion.
Baseline characteristics of participants who completed follow-up.
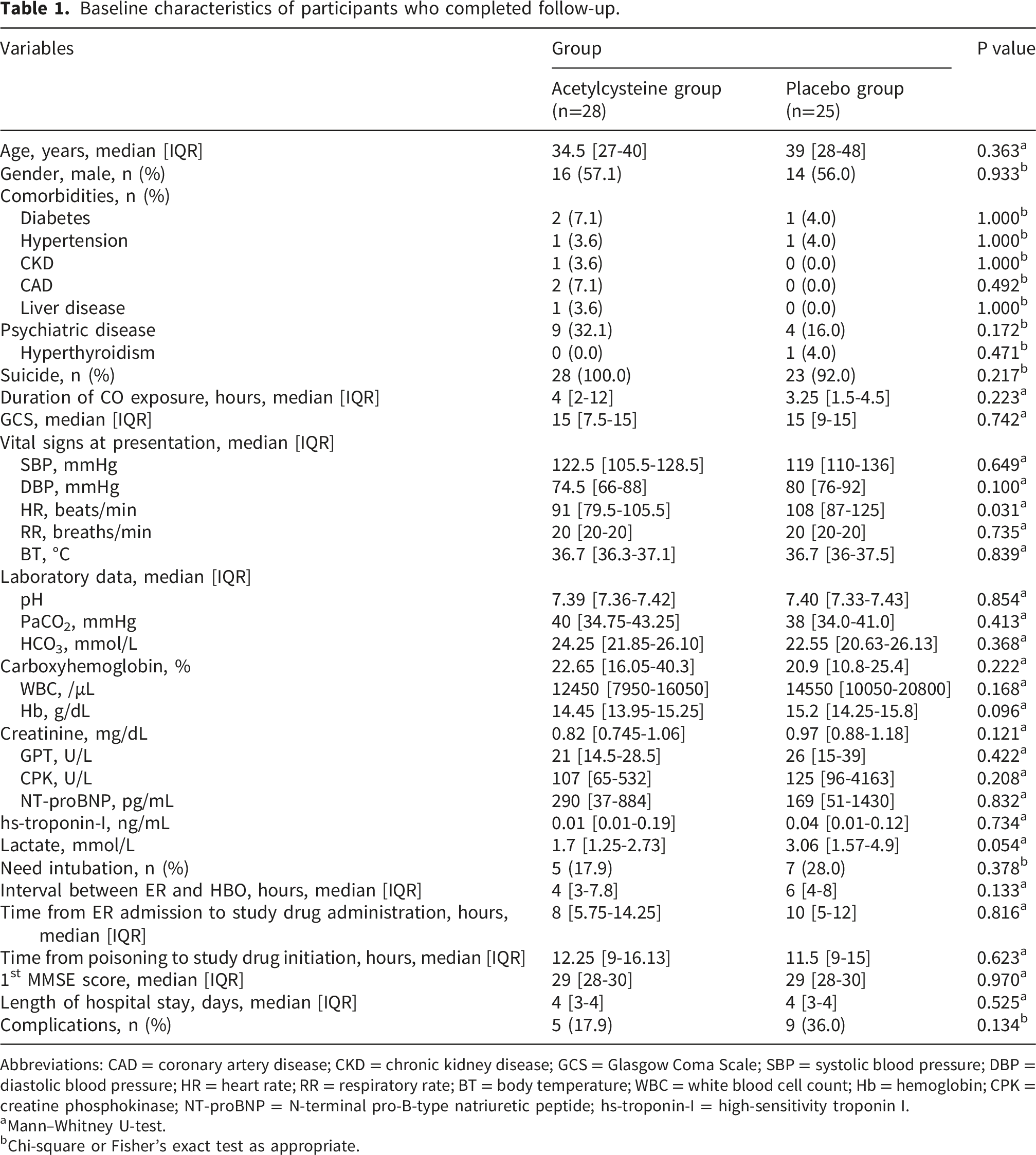
Abbreviations: CAD = coronary artery disease; CKD = chronic kidney disease; GCS = Glasgow Coma Scale; SBP = systolic blood pressure; DBP = diastolic blood pressure; HR = heart rate; RR = respiratory rate; BT = body temperature; WBC = white blood cell count; Hb = hemoglobin; CPK = creatine phosphokinase; NT-proBNP = N-terminal pro-B-type natriuretic peptide; hs-troponin-I = high-sensitivity troponin I.
aMann–Whitney U-test.
bChi-square or Fisher’s exact test as appropriate.
Results
A total of 63 patients were assessed to be eligible for the study (Figure 1). After randomization, 31 patients were allocated to the acetylcysteine group, and 32 to the placebo group. In the acetylcysteine group, two patients were lost to follow-up and one discontinued treatment after refusing HBO during hospitalization. In the placebo group, three patients were lost to follow-up and four did not complete treatment; one died of acute coronary syndrome on the second day after intoxication and the other three refused HBO. Detailed reasons for the losses to follow-up were not available. In total, 28 patients in the acetylcysteine group and 25 in the placebo group completed follow-up. Study flow diagram showing patient enrollment, randomization, and follow-up. NAC stands for acetylcysteine.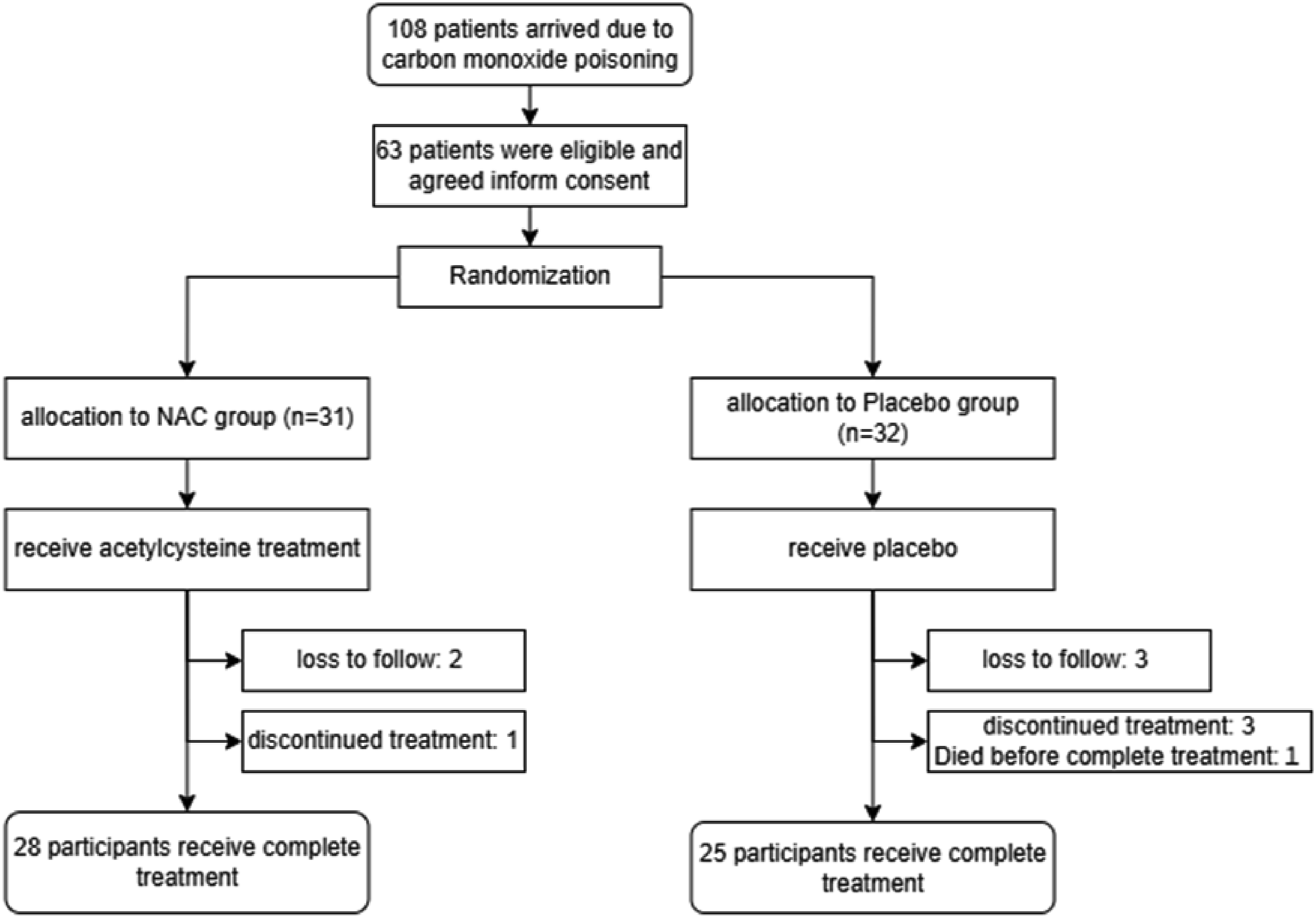
Among patients who completed follow-up, 30 (56.6%) were men, and the overall age range was 20–87 years (median age: 36 yrs). As CO poisoning patients, most (96.2%) had suicidal intent. Twenty-eight patients (52.8%) presented directly to our hospital after intoxication, while the remaining 25 patients (47.2%) received initial care at another local hospital before being referred to our emergency department for HBO. The median time between poisoning and arrival at our emergency department was 2 hours (range: 0.5–10 hrs.). All patients received drugs within 24 hours of arrival at our hospital, although in two cases the time from poisoning to study drug initiation exceeded 24 hours, on account of inter-hospital transfers.
Baseline characteristics were generally similar between the two groups (Table 1). However, median heart rate at presentation was higher in the placebo group than in the acetylcysteine group (median heart rate: 108 vs. 91 beats/min, p = 0.031). Among patients who completed follow-up (n = 53), complications arising during hospitalization after CO poisoning were pneumonia (7 patients, 13.2%), rhabdomyolysis (9 patients, 17.0%), and acute kidney injury (3 patients, 5.7%). Individual complication categories were not mutually exclusive and some patients suffered multiple complications. The incidence of complications did not differ significantly between the two groups (17.9% vs. 36.0%; p = 0.134). The median hospitalization duration was 4 days (range: 3-32 days). There was no significant difference in hospitalization duration between the two groups.
Primary outcome
The MMSE was administered twice (Supplementary Table 1). The median first MMSE score (immediately after recovery from the acute poisoning episode) was 29 (range: 13-30). In the acetylcysteine group, 26 out of 28 patients (93%) were classified as having normal cognition, while 1 out of 28 (3.5%) had mild cognitive impairment and another 1 out of 28 (3.5%) had moderate cognitive impairment. In the placebo group, 23 out of 25 participants (92%) were classified as having normal cognition, while 1 out of 25 (4%) had mild cognitive impairment, and another 1 out of 25 (4%) had moderate cognitive impairment.
The second MMSE was conducted three months after the intoxication incident. The median score for the second MMSE was 29 with a range of 0-30. In the acetylcysteine group, 25 out of 28 patients (89%) demonstrated normal cognitive function, while 1 out of 28 (3.5%) had mild cognitive impairment, 1 out of 28 (3.5%) had moderate cognitive impairment, and 1 out of 28 (3.5%) showed severe cognitive impairment. In the placebo group, 20 out of 25 patients (80%) had normal cognitive function, while 2 out of 25 (8%) had moderate cognitive impairment and 3 out of 25 (12%) showed severe cognitive impairment. Supplementary Figure 1 presents the percent differences in MMSE categories between the first and second assessments in both groups.
Primary outcome: incidence of delayed cognitive deterioration in the intention-to-treat and per-protocol populations.
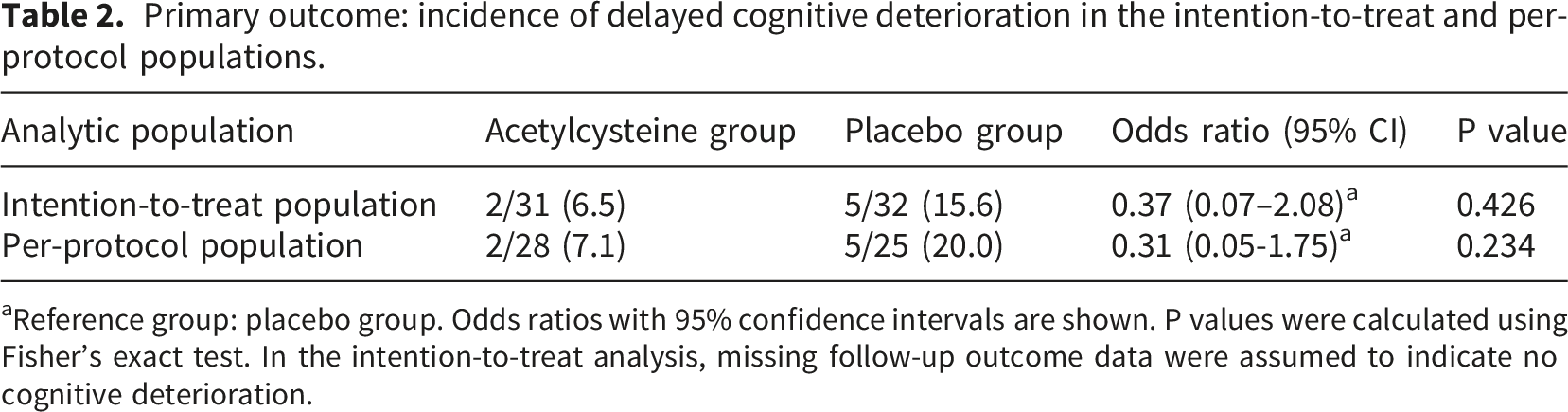
aReference group: placebo group. Odds ratios with 95% confidence intervals are shown. P values were calculated using Fisher’s exact test. In the intention-to-treat analysis, missing follow-up outcome data were assumed to indicate no cognitive deterioration.
In an exploratory analysis stratified by baseline heart rate (<100 vs. ≥100 beats/min), the inter-group difference in delayed cognitive deterioration remained statistically non-significant in both strata. Among patients with baseline heart rate <100 beats/min, delayed cognitive deterioration occurred in 2 out of 20 patients in the acetylcysteine group, and 2 out of 13 patients in the placebo group (Fisher’s exact p = 1.000). Among patients with baseline heart rate ≥100 beats/min, delayed cognitive deterioration occurred in 0 out of 11 patients in the acetylcysteine group, and 3 out of 19 patients in the placebo group (Fisher’s exact p = 0.279). This heart-rate-stratified analysis was not pre-specified and was conducted without correction for multiple comparisons; therefore, the results should be considered hypothesis-generating only.
Discussion
In this randomized controlled trial, no significant difference in the incidence of delayed cognitive deterioration after treatment for acute CO poisoning was observed between the acetylcysteine and placebo groups. Several factors may explain this result. First, the sample size may have been insufficient to detect a significant effect. This challenge is common in pilot toxicology trials, particularly in resource-limited settings. Second, the duration and dose of acetylcysteine administration may have been suboptimal. Third, the antioxidant effect of acetylcysteine may not have been sufficient in the context of CO poisoning. Fourth, although acetylcysteine has been detected in cerebrospinal fluid in human studies, its ability to reach sufficient concentrations in the central nervous system to act therapeutically in the prevention of delayed CO-related cognitive injury remains uncertain.30,40 Finally, baseline heart rate was higher in the placebo group, which may have reflected greater acute physiological stress at presentation and possibly greater poisoning severity. Since the confounding impact of this imbalance cannot be determined with certainty in this small trial, residual confounding cannot be excluded. The exploratory heart-rate-stratified analysis did not materially alter this interpretation, was not pre-specified, and should not be overinterpreted.
The median time from poisoning to the initiation of acetylcysteine was 12.3 hours in the acetylcysteine group and 11.5 hours in the placebo group, with no statistically significant difference between the groups. Thus, the timing of drug administration was well-matched between the groups, and differences in timing are unlikely to explain the observed clinical outcomes. However, given acetylcysteine’s primary mechanism as an antioxidant, its therapeutic efficacy in reducing oxidative stress-induced injury is likely time-dependent. In our study, the overall timing of acetylcysteine administration, exceeding 12 hours from poisoning exposure, may have missed the optimal therapeutic window required for maximal antioxidant benefit. Earlier initiation of acetylcysteine (ideally within 6-12 hours post-exposure or even sooner) may be necessary in order to achieve significant clinical benefits. The delays in initiating treatment observed in our study were primarily due to two factors: first, our medical center frequently receives referrals from satellite hospitals, resulting in delays due to inter-hospital transfer; and second, our inclusion criteria required confirmation of diagnosis by both emergency physicians and toxicologists, but our toxicologists and research personnel were not available round the clock. These stringent criteria and staffing limitations contributed further to delays in drug administration.
Psychiatric sequelae are also frequently observed following CO poisoning, but they were not included in the assessment of sequelae in this study for the following three reasons. First, it is challenging to quantify psychiatric symptoms using standardized scoring systems. Second, emotional symptoms may be influenced by multiple factors other than CO poisoning sequelae. Third, 96.2% of participants who completed follow-up had attempted suicide by burning charcoal, and this population already had pre-existing depression or emotional issues. Therefore, assessment of psychiatric sequelae may not provide meaningful differentiation. Accordingly, this pilot study focused on delayed cognitive deterioration rather than the full spectrum of delayed neurologic or psychiatric sequelae after CO poisoning.
The MMSE is a simple tool with a low entry threshold that can be administered by trained personnel. Prior studies of CO poisoning have also used neurological assessments that included MMSE.37,38 More sensitive instruments, such as the Montreal Cognitive Assessment or a domain-specific neuropsychological battery, were not used because this investigator-initiated pilot trial was conducted in an emergency and toxicology clinical setting with limited personnel and follow-up resources. We selected the MMSE pragmatically because it was feasible for repeated bedside and outpatient application by trained, non-specialist personnel. However, MMSE scores can be influenced by factors such as age and education levels, potentially leading to false positives in older individuals or those with lower educational levels. To reduce the potential for misclassification, we measured MMSE scores twice over a three-month interval, rather than relying on a single time point. In this study, we used the change in MMSE category as an operational measure of cognitive deterioration, captured over time. This approach was intended to identify substantial cognitive deterioration and may therefore have overlooked milder cognitive symptoms that did not result in category change. Notably, all seven participants who were classified with cognitive deterioration showed declines of 10 points or more on the MMSE, indicating that the observed outcomes were not driven by minor score changes that merely crossed category thresholds.
In our study, no serious adverse effects, such as anaphylactic reactions, were observed in either the acetylcysteine or placebo groups. At most, participants reported mild symptoms such as headache and dizziness, which were difficult to distinguish from the symptoms of CO poisoning and were therefore not classified as adverse effects. These symptoms may have been related to the dosing schedule used in this study, whereby acetylcysteine was administered in divided doses over 24 hours, as well as the slow IV infusion rate employed, both of which were intended to reduce the likelihood of infusion-related adverse effects.
Limitations
Several limitations of this study should be acknowledged. First, this was a small pilot randomized trial and was underpowered to detect a definitive treatment effect. Because prior clinical data on acetylcysteine for this specific indication were insufficient, no formal efficacy-based sample size calculation was available at trial initiation. Therefore, our negative result should be interpreted cautiously. Moreover, because the trial was not prospectively registered and the final MMSE category-based endpoint operationalization was not pre-specified in a detailed statistical analysis plan, selective outcome reporting and outcome-definition bias cannot be fully excluded. Second, as a single-blinded trial, this study was vulnerable to detection bias because the outcome assessors who administered the MMSE were not blinded to the treatment allocation. Although MMSE administration was standardized, no formal inter-rater reliability assessment was performed, and MMSE scoring was not reviewed or adjudicated by a blinded assessor. This limitation reduces confidence in the observed inter-group difference, and the direction and magnitude of this bias cannot be determined with certainty. However, because all participants classified as showing delayed cognitive deterioration had clear declines of 10 points or more on the MMSE, minor assessor-related variation alone was unlikely to fully explain the observed events, although detection bias also cannot be excluded. Third, the change in Mini-Mental State Examination category reflected only one dimension of cognitive outcome and has not been specifically validated for the assessment of delayed cognitive sequelae after CO poisoning. Accordingly, the endpoint construct may not fully capture the broader spectrum of delayed neurologic sequelae. In addition, baseline MMSE scores were high in both groups, and most participants were classified as cognitively normal, creating a ceiling effect that limited sensitivity to milder forms of delayed cognitive change. Category-based classification is fundamentally vulnerable to threshold artefacts when scores lie near category boundaries, although the observed events in this study involved MMSE declines of 10 points or more. Fourth, the timing of the first MMSE assessment was not fully standardized, and the source records did not contain sufficient date- or time-level information to calculate the interval from poisoning to the first MMSE assessment by group. This may have introduced measurement variability which might, in turn, have biased the study toward under-detection of delayed cognitive deterioration if some baseline assessments were performed relatively early during recovery. However, baseline first-MMSE status appeared similar across the groups, with a median score of 29 in both groups and most participants classified with normal cognition, suggesting that major baseline category-level cognitive imbalance was unlikely among participants who completed the assessment. Future studies should implement and document a fixed time point for baseline cognitive assessment. Fifth, the high prevalence of psychosocial and psychiatric problems in this cohort may have confounded cognitive outcomes, as depression-related pseudodementia could mimic cognitive decline. In addition, concomitant medications and post-discharge psychiatric treatment, which may influence MMSE performance, were not systematically recorded. However, since the primary outcome was based on category changes rather than small changes in raw score, and since all participants classified with cognitive deterioration showed MMSE declines of 10 points or more, minor medication-related fluctuations were unlikely to fully explain the observed outcomes. Nonetheless, some residual confounding cannot be excluded. Sixth, in the intention-to-treat analysis, participants with missing follow-up outcome data were conservatively classified without delayed cognitive deterioration. This assumption may have biased the estimated treatment effect toward the null. However, the complete-case sensitivity analysis yielded similar results. Seventh, neuroimaging was not incorporated into the outcome assessment. Although delayed cognitive deterioration after CO poisoning is primarily a clinical diagnosis, the absence of standardized neuroimaging reduced diagnostic specificity, as some follow-up cognitive decline may have reflected other neurological or psychiatric processes. In real-world practice, standardized magnetic resonance imaging may be difficult to obtain in some patients because of cognitive impairment, behavioral symptoms, or clinical instability. Finally, because the study population was limited to an Asian cohort, the generalizability of the findings to other populations may be restricted. Larger multicenter studies with more standardized outcome assessment and better control of confounding factors are needed.
In conclusion, adjunctive acetylcysteine did not significantly reduce delayed cognitive deterioration in this pilot study. Any apparent between-group difference should be interpreted with caution, given the limited sample size, the MMSE-based outcome definition, and the lack of blinding during outcome assessment. Given the pilot nature, sample size, and design limitations of this study, the findings should be regarded as hypothesis-generating and should not guide clinical practice at present. Further studies with larger sample sizes and more standardized outcome assessment are needed to evaluate any treatment effect more confidently.
Supplemental material
Supplemental material - Acetylcysteine for delayed cognitive deterioration after acute carbon monoxide poisoning: A pilot randomized controlled trial
Supplemental material for Acetylcysteine for delayed cognitive deterioration after acute carbon monoxide poisoning: A pilot randomized controlled trial by Han-Wei Mu, Fen-Wei Huang, Chun-Yen Kuo, Hong-Mo Shih, Kai-Wei Yang, Chun-Hung Chen, Dong-Zong Hung in Human & Experimental Toxicology
Footnotes
Acknowledgements
We wish to acknowledge the invaluable support of the Emergency Department staff of China Medical University Hospital for their assistance in data collection. We also acknowledge China Medical University Hospital for research funding.
Ethical considerations
This randomized controlled trial was approved by the Institutional Review Board of China Medical University Hospital, Taichung, Taiwan (Approval No: CMUH106-REC2-154). All procedures involving human participants were conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments.
Consent to participate
Written informed consent was individually obtained from all participants or their closest available surrogates before enrollment. The IRB-approved protocol included the use of surrogate consent for participants with impaired consciousness or altered mental status, but did not include routine re-consent after recovery of decision-making capacity or the use of deferred consent.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by China Medical University Hospital (DMR-107-161 and DMR-113-192).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.