
Abstract
This multi-lingual study presents the awareness, perceptions, and behavior regarding COVID-19 “misinformation” and “fake news,” among the rural population of the South Asian (SA) countries of Bangladesh, India, and Pakistan. The survey questionnaire was distributed to a convenient sample of 400 respondents from the three most populated SA countries selected due to their shared socio-cultural history; limited by fund availability and travel restrictions due to the prevailing lockdowns during the data collection period of early 2022. Results indicate that 92.98% of the participants perceived the presence of COVID-19 misinformation to varying degrees around them with less than 10% finding it easy to verify the accuracy of the information. The results indicate that the participants initially believed the made-up news and information to be true and then experienced fear or uncertainty upon realizing that it was fake. Results further show significant differences in perception and behavior when analyzed with the parameters of gender, age, education, and religion. Our study highlighted that female respondents perceived less than male respondents that fake news was around them, and younger participants of the study had less perception of the presence of fake news around them. The present study also found that the education level of respondents is a strong predictor of their perception of COVID-19 misinformation. Respondents with high school degrees perceived less made-up news and information than associate and master-level degree holders. The findings indicate a lack of media literacy, with a vast majority of individuals being susceptible to false information. The findings of the study will help healthcare professionals, information professionals, social workers, extension workers, and policymakers to deal with the Infodemic and further also assist in designing shared health information literacy programs across the region.
Keywords
Introduction
COVID-19 misinformation has seen a parallel growth since the first news of the virus was reported in December 2019, growing exponentially across the globe (Depoux et al., 2020). Termed the “virus within” (Doheny, 2020), COVID-19 misinformation became as much of a global phenomenon as the virus itself. The terms misinformation, disinformation, and fake news are explained as, “information that is false but not created with the intention of causing harm,” and “information that is based on reality, used to inflict harm on a person, social group, organization or country” and “false stories that appear to be news, spread on the internet or using other media, usually created to influence political views or as a joke” respectively (UNESCO, 2018). The scope of the current study is limited to “misinformation” and “fake news” and the terms fake news and made-up news have been used interchangeably.
The situation was further aggravated by the COVID-19 Infodemic (Bradd, n.d.; The Lancet, 2020) which made it impossible to keep track of the sheer quantum of information being published on COVID-19. Studies show the dangers caused by COVID-19 misinformation (Agley and Xiao, 2021; Nelson et al., 2020; Wang et al., 2022); the role of social media in spreading this misinformation (Ahmed et al., 2021; Pennycook et al., 2020); and proliferation of fake news related to COVID-19 (Apuke and Omar, 2020; Orso et al., 2020). Moreover, it is cumbersome to detect misinformation because information can be generated and disseminated at a fast pace using a variety of ICT tools and techniques (Singh et al., 2021). Furthermore, the novelty of the disease, lack of expertise among journalists, inadequate moderation of content, and algorithmic biases were some of the other hurdles to countering the misinformation (Fan et al., 2020; Gisondi et al., 2022; Morrow et al., 2022). The prevalent atmosphere of misinformation resulted in undermining national and international responses and creating an atmosphere of mistrust, fear, and disbelief among the masses. Misinformation managed to cut across the digital divide affecting both the urban and rural landscapes across the region.
South Asia (SA), a subregion with a quarter of the world’s population, includes Afghanistan, Bangladesh, Bhutan, India, Maldives, Nepal, Pakistan, and Sri Lanka. Comprising a rural population of 64.66% (World Bank, 2021), these countries shared common challenges in fighting the pandemic with large populations having low literacy rates, low socio-economic conditions (Rasul et al., 2021), with less than 50% of the population with access to the internet (Delaporte and Bahia, 2022). Studies focusing on the rural population from Bangladesh, India, and Pakistan (Bin Naeem and Kamel Boulos, 2021; Kritika, 2022; Shahid et al., 2022; Sultana and Fussell, 2021) have focused on perceptions toward fake news and social media and present isolated cases for each country.
The region saw collaborations through various initiatives either bilaterally (Fruman and Kaul, 2020; United Nations ESCAP, 2020) with specific goals of economic recovery, sharing of resources (Mobarak et al., 2021) or targeted toward specific audiences like people with disabilities (International Disability Alliance, 2021) or children (UNICEF, 2021) showing a lack of collaborative initiatives to provide accurate COVID-19 information and reducing misinformation. Members from the South Asia Chapter of the Association for Information Science and Information Technology (ASIS&T) identified shared socio-economic, cultural, and religious factors (ASIS&T South Asia Chapter, 2022; Gala et al., 2022) that helped in perceiving the awareness of misinformation among the SA population.
The current research is significant as it provides a collaborative approach to identifying the perceptions and behavior of the rural population from Bangladesh, India, and Pakistan—three countries with shared cultural, political, and geographical histories. Perception is how something is regarded, understood, or interpreted and behavior is how one acts or conducts oneself with a clear order of the latter following the former. The current study takes these into cognizance within the context of studying COVID-19 misinformation in the selected SA countries. The study particularly addresses the following research questions:
RQ 1. How does the rural population in the South Asian countries of Bangladesh, India, and Pakistan perceive COVID-19 misinformation?
RQ 2. Are there any significant differences of opinions between the perception and behavior of COVID-19 misinformation based on demographic parameters of education, age, gender, and religion?
The current study makes significant contributions to the collective findings of the study helping information and healthcare professionals, social workers, extension workers, and policymakers to deal with existing challenges related to misinformation among the rural populations of the selected countries. Further, the study shall also assist in designing shared information literacy programs to deal with misinformation across SA countries and be better prepared for the future.
Literature review
The efforts and responses of the scientific community to the COVID-19 pandemic have been unprecedented, and researchers have contributed several important advances. Like other parts of the world, the SA region has been studied well in the context of COVID-19 research. Researchers, scientists, and practitioners across the world are continuously publishing research articles, letters, reviews, notes, and editorials related to COVID-19. As an apex body of COVID-19 in the global context, WHO is maintaining a global research database on COVID-19-related studies (WHO, 2022), and different publishers across the world are offering free access to online resources on COVID-19. Several studies focused on the region looked at the COVID-19 pandemic and its related research areas. We have summarized some of the recent and relevant studies in the COVID-19 context of Bangladesh, India, Pakistan, and SA as a whole. Considering the research areas, we have mostly focused on mis and disinformation, fake news, rumors, vaccine hesitancy, and pandemic information management studies of COVID-19 in this region.
In the SA region, knowledge, attitude, practices, perceptions, and health information system is not well organized. Specifically in Bangladesh, people face significant challenges in accessing and utilizing information related to COVID-19, indicating a lack of effective organization and dissemination of health information in the country (Joarder et al., 2021). Al-Zaman (2021b) extracted COVID-19 misinformation from fact-checking websites and analyzed six popular themes of misinformation which included health, politics, religion, crime, entertainment, and miscellaneous. Some misinformation prevention strategies like myth busters, monitoring fake news, digital surveillance, identifying online rumor spreaders through technology, and anti-misinformation campaigns from government initiatives are also discussed. Sultana and Fussell (2021) employed ethnography in rural villages of Bangladesh to investigate information-sharing channels, fact-checking websites, and both online and offline COVID-19-related misinformation. Fondazione Bruno Kessler highlighted that out of 112 million posts about COVID-19 on social media, 40% contained information from unreliable sources (FBK, n.d.). Floating disinformation during the COVID-19 in India, one out of six COVID-19 information generated in 2020 was fake, and this has made India the leading country of COVID-19 misinformation (Kanozia et al., 2021; Sharma, 2022). Al-Zaman (2021a) analyzed 125 online fake news and found Twitter, Facebook, WhatsApp, and YouTube, produce most of the health-related fake news in India. Fake news and mis-disinformation about COVID-19 have become the major challenges.
A direct outcome of COVID-19 misinformation was the hesitancy toward vaccination and associated behavior. Verma et al. (2022) found that trust in direct personal contacts and considering the quality of information relating to COVID-19 positively impacted self-efficacy in dealing with situations during a pandemic. Sun and Monnat’s (2022) study comparing rural and urban populations revealed a vaccination rate of 45.8% among adults in rural areas, while urban areas had a higher rate of 59.8%. The study identified lower educational attainment as a significant factor contributing to this disparity. Amponsah-Tabi et al. (2023) investigated COVID-19 vaccine acceptability in rural Ghana and found that a significant proportion of respondents lacked sufficient knowledge (55.0%), poor attitudes (59.4%) toward the COVID-19 vaccine and 55.4% of respondents held negative perceptions of the vaccine. Tolia et al. (2022) studied vaccine adoption in Gujarat (India) and found vaccine adoption is largely influenced by government, religious and political leadership. Hawlader et al. (2022) found that more than 50% of the respondents from Bangladesh, India, Pakistan, and Nepal were willing to be vaccinated in their respective countries. In a commentary, Kanozia and Arya (2021) discussed COVID-19 vaccine hesitancy in South Asia due to fake news and misinformation. Their suggestions include robust vaccine campaigns, enhanced transparency, and collaboration with religious and public leaders to encourage vaccine uptake and dispel fears.
Studies (Callaghan et al., 2021; Chen and Chen, 2020) with rural population found disinclination toward wearing masks in public and participating in COVID-19-related preventive health measures with lower levels of information appraisal skills. Balakrishnan (2022) found that socio-demographic predictors for misinformation-sharing behavior are accidental instead of intentional.
Malik et al. (2023) examined the misinformation-combating behavior of social media users during the COVID-19 pandemic in Pakistan, and found that prior experiences and self-efficacy help to mitigate the use of misinformation. Javed et al. (2020) analyzed the COVID-19 misinformation dissemination discourse of text and images on WhatsApp and Twitter in Pakistan, and identified misinformation has a longer life span in WhatsApp compared to Twitter. In a cross-sectional survey, Abbas et al. (2021) measured myths, beliefs, and conspiracies about COVID-19 Vaccines in Pakistan and found that the majority of respondents are not aware of the COVID-19 vaccine and conspiracies become major barriers to taking vaccines in Pakistan. In another study on Pakistan, Rafi (2020) suggested that social media education for internet users to deal with misinformation can be helpful. In a health informatics project focused on combating COVID-19 mis and disinformation in South Asia, a YouTube channel was created to produce nine multilingual videos containing COVID-19 information from reliable sources. Project members put their insights on the challenges, experiences, resilience, and collaborative efforts related to COVID-19 in the South Asian region (Chan et al., 2022; Gala et al., 2022)
The reviewed research studies indicate a diverse range of topics related to the COVID-19 pandemic across South Asian countries, focusing on Bangladesh, India, Pakistan, and other regions. The topics cover various aspects, including the impact of misinformation and fake news on pandemic management, vaccine hesitancy in different religious and socio-demographic contexts, differences in preventive behaviors between urban and rural populations, and the dissemination of COVID-19-related information through social media. However, very few studies focused on the perceived mis and disinformation of COVID-19 in the rural context from this region, and are not explicitly stating the COVID-19 misinformation, perceptions, and behavior of the rural population from SA countries. There is a need for a comprehensive understanding of misinformation, vaccine acceptance, and preventive behaviors across diverse cultural and geographic contexts in this region. The present study aims to provide a platform for more focused and in-depth exploration within the broader context of COVID-19 perceptions and behaviors in this region.
Methodology
Study sample and data collection
In this study, we investigated the perceptions and behavior of the rural population from three SA countries—Bangladesh (n = 49), 1 India (n = 300), and Pakistan (n = 50). The convenience sampling method was applied to choose both the representative sample area and respondents. The selection of these specific countries was based on the fact that these are the top three most populated countries in the SA region and collectively represent approximately 70% (Worldbank, 2022) of the total population of the SA region. Further, the significance of selecting the population from the three selected countries was governed by the fact that the countries share a common sociocultural history influencing shared perceptions and behavior. The sample number was decided in proportion to the population and the geographical area of Bangladesh and Pakistan being much smaller countries in comparison to India.
In Bangladesh and Pakistan, the survey was conducted from May to June 2022. Due to the prevailing COVID-19 situation in India during the early part of 2022, the survey was delayed and was conducted between April and June 2022. The responses were collected by personally visiting the selected areas. Another critical factor in data collection was also the literacy levels of respondents in the rural areas of the selected countries which are plagued by extremely low literacy rates. Thus, the data collectors were also instructed to read the questions, explain if necessary, and write or note down the responses response for the respondents. In each country, the data collecting team was compensated for their travel, printing, data, and other associated costs incurred for collecting the data.
Informed consent was taken from all the respondents (Appendix A; Supplemental Material). In the survey instrument (Appendix A; Supplemental Material), respondents were asked to share demographic information to capture their geographical area, age, gender, educational qualification, and religion. The demographic questions were prepared, being mindful of the nature of the participants who were from rural areas. The respondents were invited to share their religion as an open-ended question to respect the religious diversity in these countries.
To assess the perception and behavior toward COVID-19, respondents were specifically asked about their behavior and perception toward misinformation. The participant’s responses to the open-ended statement helped us identify their feelings and mental health related to the pandemic by performing sentiment analysis. The questionnaire allowed us to understand various aspects, such as the relationships between gender, age, religion, news, and misinformation related to COVID-19.
In Bangladesh, three graduate students from the Department of Information Science and Library Management, University of Dhaka who live in the northern rural part of Bangladesh were assigned to collect the responses. Five villages in Mohanpur upazila (Sub-district) under the Rajshahi district have been chosen for the respondents of this study.
In India, the survey was conducted in rural areas of Uttar Pradesh and Rajasthan, two Indian states where Hindi is the primary language spoken. To collect the data, we recruited a researcher who was actively working in these states and had fluency in both Hindi and English, as well as familiarity with the rural areas selected for the study. The researcher’s knowledge of these regions was crucial to ensuring the quality and accuracy of the data collected.
In Pakistan, the data was collected during the months of June–July 2022 with the help of graduate students of the Institute of Information Management, University of the Punjab, Pakistan who belonged to rural areas of Pakistan. Most of the graduates were from the eastern-central part of the country and lived in the province of Punjab. Punjab is the second largest province of Pakistan regarding population size and land. The graduates went to their hometowns during the summer holidays of 2022 and conveniently selected participants willing to participate in the survey.
Survey instrument
The questionnaire (Appendix A; Supplemental Material) for this paper was adapted from the Pew Research Center (2021) survey. 2 However, as the Pew Research Center survey focused on Americans, we made major revisions to better capture South Asian people’s behavior and perception of COVID-19 misinformation. The survey instrument was prepared initially in English and was then translated into three languages viz., Bengali, Hindi, and Urdu to be surveyed in Bangladesh, India, and Pakistan respectively. The language was selected based on the predominant language spoken in the respective country. India is a country of many languages, with no single national language (Constitution of India). Of the 22 major languages recognized by the Government of India, Hindi is spoken by more than 57% (insert citation) of the population as the first language. Thus, in India, Hindi was chosen as the language of the survey instrument. The questionnaire was divided into two blocks viz. (i) demographic information, and (ii) COVID-19-related perception and behavioral queries. A total of 12 questions were posed to respondents in the questionnaire. The COVID-19 Misinformation block had 7 questions while the demographic block contained 5 questions.
Data analysis
The responses underwent descriptive and sentiment analysis using R and SPSS for RQ-1. Initially, the Excel spreadsheets containing the responses from various countries were combined and pre-processed in R. This was followed by country-wise and cumulative descriptive analysis. Sentiment analysis was performed on open-ended questions (Q-F) using syzuhet library 3 in R.
Sentiment analysis is a natural language processing (NLP) method that helps extract significant informational patterns and characteristics from a text corpus. It determines the overall emotion of a text expressed by the author (Lamba and Madhusudhan, 2022). Syuzhet is a dictionary-based tool that uses the Bing, Afinn, Syuzhet, and NRC lexicons to analyze sentiment in texts (Kim, 2022). We added the code and data used for sentiment analysis to the GitHub repository. 4 Figure 1 shows the step-by-step procedure used to perform sentiment analysis in R.
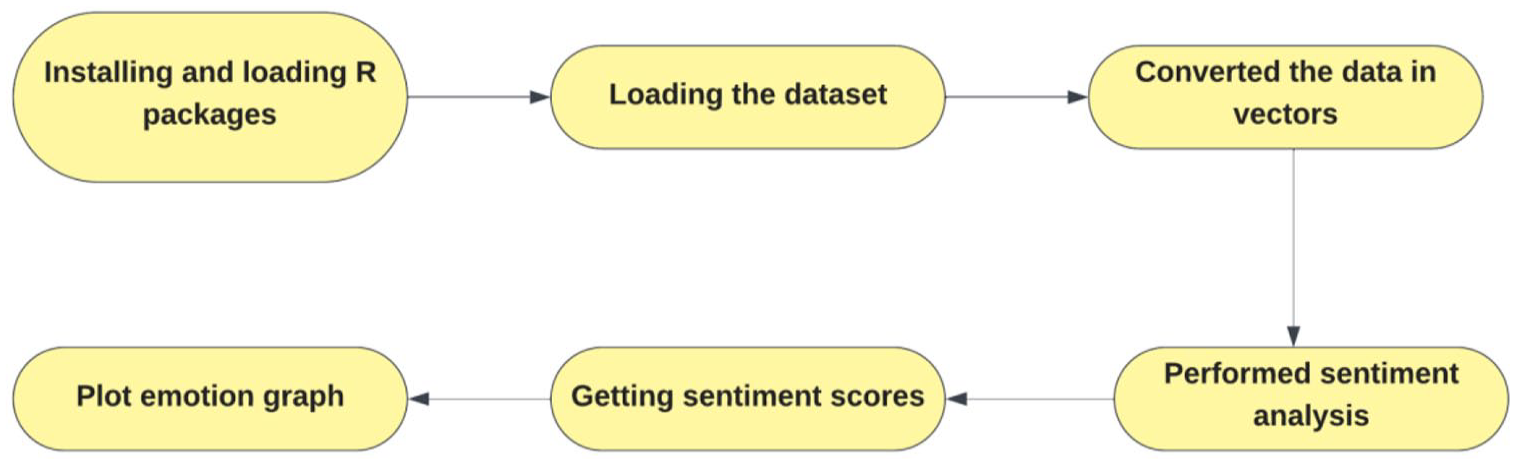
Step-by-Step Procedure to Perform Sentiment Analysis in R.
The significant influence of demographic variables (education, age, gender, religion) for RQ-2, was measured through Mann Whitney U and Kruskal-Wallis tests.
The formula used to compute the z score in Mann Whitney U test was:

where
U1 is the sum of ranks in new treatment group
U2 is the sum of ranks in standard treatment group
n1 is the distribution in new treatment group
n2 is the distribution in standard treatment group
Both serve as non-parametric alternatives to t-test and one-way ANOVA. The researchers used non-parametric tests as the study data is not normally distributed and the independent variables are of categorical or ordinal nature. We also fulfilled the safety checks before applying the Mann U Whitney U and Kruskal-Wallis tests.
The formula used to compute Kruskal-Wallis test was:

where
K = the number of groups used for comparison
N = total size of the sample
ni = is the group’s sample size
Ri = total of the ranks related to the group
The few assumptions are (1) the dependent variable should be of ordinal or continuous nature (2) the independent variable should be categorical in nature and consist of two or more than two groups (3) the independence of observations means there should be different participants in each population group. Our study fulfills the above-stated conditions of the Mann-Whitney U and Kruskal-Wallis tests (Cohen et al., 2017).
Analysis and interpretation
This subsection presents the findings of both RQ 1 and RQ 2 that aimed to investigate the perception and behavior of COVID-19 misinformation among the rural population in Bangladesh, India, and Pakistan. By examining the specific context of rural communities, the study sought to shed light on the unique challenges and dynamics that influence the spread and reception of misinformation in these regions.
Demographics
Table 1 provides an overview of the demographic characteristics of the participants in a research study. The study included a total of 399 participants from rural regions of three SA countries: Bangladesh, India, and Pakistan. The table presents data on participants’ gender, age, education, area, and religion, distributed by country.
Participants’ demographics (N = 399).

In terms of gender, most participants were female (67.92%), with the remaining participants identifying as male (32.08%). The distribution by country shows that the proportion of female participants was highest in India (74.67%) and lowest in Pakistan (42%).
The age distribution of participants varied, with 30.58% falling in the 25–34 age range, followed by 48.62% falling in the 35–50 age range. The distribution by country shows that the proportion of participants in the 18–24 age range was highest in Pakistan (50%) and lowest in India (1.33%). On the contrary, India had the highest proportion of participants in the rest of the age ranges.
In terms of education, most participants had completed high school (53.13%) or a bachelor’s degree (31.08%), with smaller proportions having completed some college but no degree (6.77%), an associate degree (4.26%), or a master’s degree or higher (4.26%). The distribution by country shows that the proportion of participants with a bachelor’s degree was highest in India (28.67%) and lowest in Pakistan (16%).
In terms of religion, many participants identified as Hindu (74.19%) or Muslim (25.31%), with smaller proportions identifying as Buddhist (0.25%) or Christian (0.25%). The distribution by country shows that all participants from Pakistan identified as Muslim, while the majority of participants from India identified as Hindu (97.67%) and Bangladesh as Muslim (89.90%).
COVID-19 perception
Figure 2 presents the participants’ responses to seven questions stated from QA to QG from the survey regarding their perception of COVID-19, self-perceived knowledge of the virus, mask-wearing behavior, vaccination status, exposure to made-up news and information, and difficulty verifying news and information related to COVID-19. The findings from the table are described below:
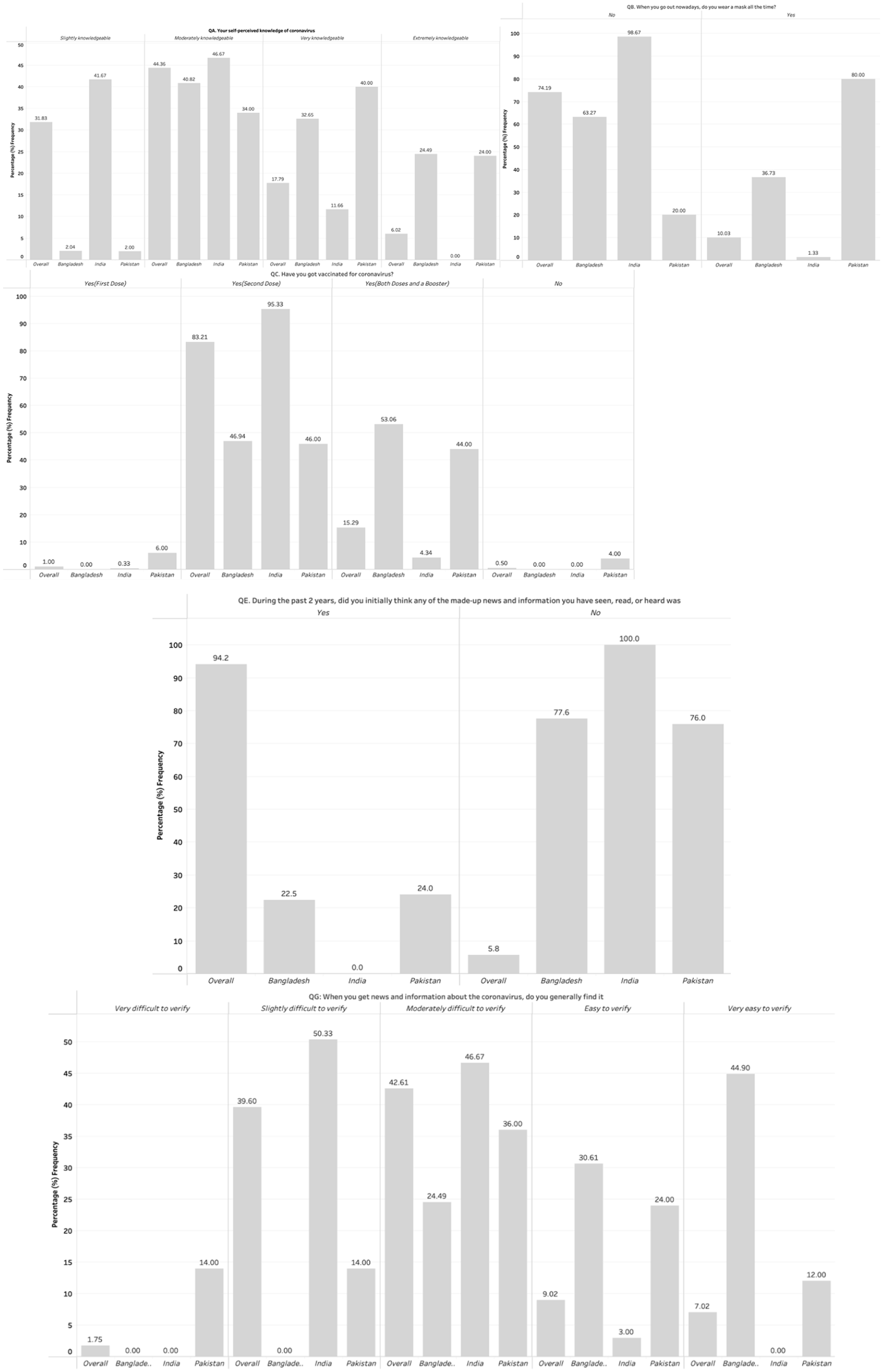
COVID-19 perception by South Asian rural population (N = 399).
QA: Your self-perceived knowledge of coronavirus
The figure shows that 31.83% of participants perceive themselves as slightly knowledgeable, while 44.36% perceive themselves as moderately knowledgeable. Only 6.02% consider themselves extremely knowledgeable, and no participant responded as having no knowledge of the virus. In Bangladesh, 2.04% of participants perceive themselves as slightly knowledgeable, while 40.82% and 32.65% consider themselves moderately knowledgeable and very knowledgeable, respectively. In India, 46.67% of participants perceive themselves as moderately knowledgeable, while 41.67% consider themselves slightly knowledgeable. In Pakistan, the majority (40%) of participants responded as very knowledgeable, while 34% and 2% perceived themselves as moderately knowledgeable and slightly knowledgeable, respectively.
QB: When you go out nowadays, do you wear a mask all the time?
The figure shows that out of all participants, 74.19% reported not wearing a mask all the time when going out, while only 10.03% said they always wear a mask. In Bangladesh, only 36.73% of participants wear masks all the time, while 63.27% do not. In India, 98.67% of participants responded as not wearing masks all the time, and only 1.33% wore masks all the time. In Pakistan, the majority (80%) of participants wear masks all the time, while 20% do not.
QC: Have you got vaccinated for coronavirus?
The figure shows that most of all participants (83.21%) received the second dose of the vaccine, while 15.29% received both the doses and a booster. Only 0.50% of participants reported not receiving any vaccine dose. In Bangladesh, 46.94% of participants received the second dose, while 53.06% received both doses and a booster. In India, 95.33% of participants received the second dose, while 4.34% received both doses and a booster. In Pakistan, 46% of participants received the second dose, while 44% received both doses and a booster.
QD: How much do you think made-up news and information about the basic facts of the coronavirus is around you?
The figure shows that 42.11% of participants reported “a great deal” of made-up news and information around them related to coronavirus, while 41.60% reported a “moderate amount.” Only 6.77% of participants as having “a little.” In Bangladesh, 69.39% of participants perceived “a lot” of made-up news and information, while 4.08% perceived “a little.” In India, the majority (53.33%) of participants responded as having “a great deal” of made-up news and information, while 46.67% perceived them as “a moderate amount.” In Pakistan, 50% of participants perceived the news about coronavirus as “a little,” while 6% as “a lot.”
QE: During the past 2 years, did you initially think any of the made-up news and information you have seen, read, or heard was true before realizing it was made-up?
According to the figure, most participants, 94.24%, initially believed made-up news and information to be true before realizing it was fake. Only 5.76% of participants were confident in their ability to identify fabricated news. In Bangladesh, 22.45% of participants initially believed false news before recognizing it as such. Conversely, in India, all participants were able to correctly identify made-up news, whereas 76% of participants from Pakistan were able to recognize false information related to coronavirus.
QG Asks participants how easy or difficult they find it to verify news and information about coronavirus
The figure reveals that only 9.02% and 7.02% of all participants found it “easy” and “very easy,” respectively, to verify coronavirus-related information. Meanwhile, 39.60%, 42.61%, and 1.75% of participants reported finding it “slightly,” “moderately,” and “very” difficult to verify such information. When examining country-specific data, the majority of participants in Bangladesh (44.90%) found it “very easy” to verify coronavirus information. However, 24.49% of participants from Bangladesh reported finding it “moderately difficult” to verify such information. In contrast, the majority of participants from India found it either “slightly” (50.33%) or “moderately” (46.67%) difficult to verify coronavirus-related information. Responses from participants in Pakistan were evenly distributed, with 14% reporting finding it either “very” or “slightly” difficult to verify information. In comparison, most found it either “moderately” difficult (36%) or “easy” (24%) to verify.
Sentiment analysis
Sentiment analysis was performed on the open-ended question (Q-F) which resulted in the distribution of emotions (Figure 3). Each response for Q-F was analyzed using syuzhet package 5 in R and was labeled with an emotion category. The figure displays a histogram that shows the frequency of each emotion category. These categories were trust, fear, sadness, anger, joy, disgust, anticipation, and surprise. The y-axis of the histogram represents the different emotion categories, while the x-axis represents the number of instances of each emotion category in the participants’ responses for Q-F in percentage. The histogram shows that most of the instances were labeled as trust and fear, followed by sadness and anger. Joy, disgust, and anticipation had relatively lower frequencies. Surprise had the lowest frequency among all emotion categories.
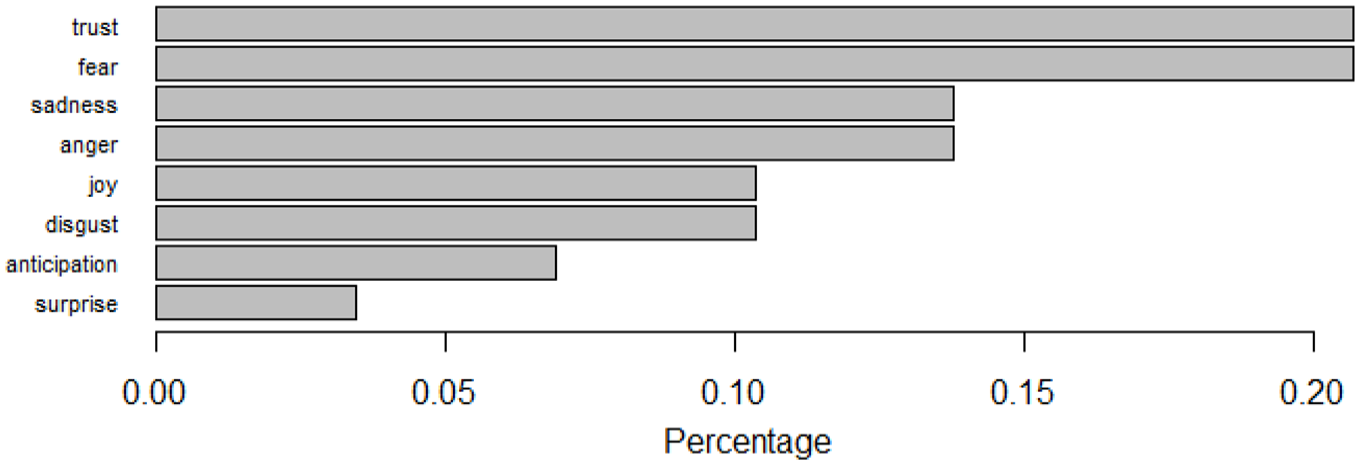
Sentiment analysis result for question QF (QF: If you selected Yes in QE, please specify).
The high frequency of trust and fear in the participants’ responses suggests that they might have initially believed the made-up news and information to be true and then experienced fear or uncertainty upon realizing that it was fake. The relatively high frequency of sadness and anger could reflect the negative emotional impact of realizing that they had been misled or deceived. The lower frequencies of joy, disgust, and anticipation suggest that participants did not experience positive or excited emotions in relation to the topic. The low frequency of surprise could indicate that many participants were not caught off guard or shocked by the realization that the news and information were fake, which might suggest that they were aware of the prevalence of misinformation or fake news.
The second research question (RQ2) of the study was to determine the difference of opinions between the demographic parameters (gender, age, religion, education) and the perception and behavior of COVID-19 misinformation primarily led the researchers to formulate eight directional hypotheses as below:
H1: There is a significant difference between the perception of COVID-19 misinformation and demographic parameter gender.
H2: There is a significant difference between the COVID-19 misinformation behavior and demographic parameter gender.
H3: There is a significant difference between the perception of COVID-19 misinformation and demographic parameter age.
H4: There is a significant difference between the COVID-19 misinformation behavior and demographic parameter age.
H5: There is a significant difference between the perception of COVID-19 misinformation and demographic parameter religion.
H6: There is a significant difference between the COVID-19 misinformation behavior and demographic parameter religion.
H7: There is a significant difference between the perception of COVID-19 misinformation and demographic parameter education.
H8: There is a significant difference between the COVID-19 misinformation behavior and demographic parameter education.
To analyze the difference between the COVID-19 misinformation perception between genders (male/female), the Mann-Whitney U test was applied. The test is an alternative nonparametric test to the t-test. The independent variable (gender) has three groups (male, female, non-binary), however, none of the respondents identified themselves in the third category (non-binary). Therefore, to see the difference of opinion between males and females, the Mann-Whitney U test was considered appropriate. The test statistics revealed significant differences between both groups’ male (Median = 3.00, n = 128) and female (Median = 3.00, n = 271), U = 14,821, z = 2.519, p = 0.12, r = 0.12) and COVID-19 misinformation perception, hence, hypothesis H1 was accepted (Table 2). Similarly, the analysis found significant differences of opinion between demographic parameter (gender), male (Median = 3.00, n = 128) and female (Median = 3.00, n = 271) and COVID-19 misinformation behavior of study respondents, U = 14,875, z = 2.475, p = 0.13, r = 0.12), so H2 was accepted (Table 2). According to Cohen et al. (2017), the effect size or value of r can be calculated with the formula: Z/√N.
Mann-Whitney U test results based on demographic parameter “gender.”
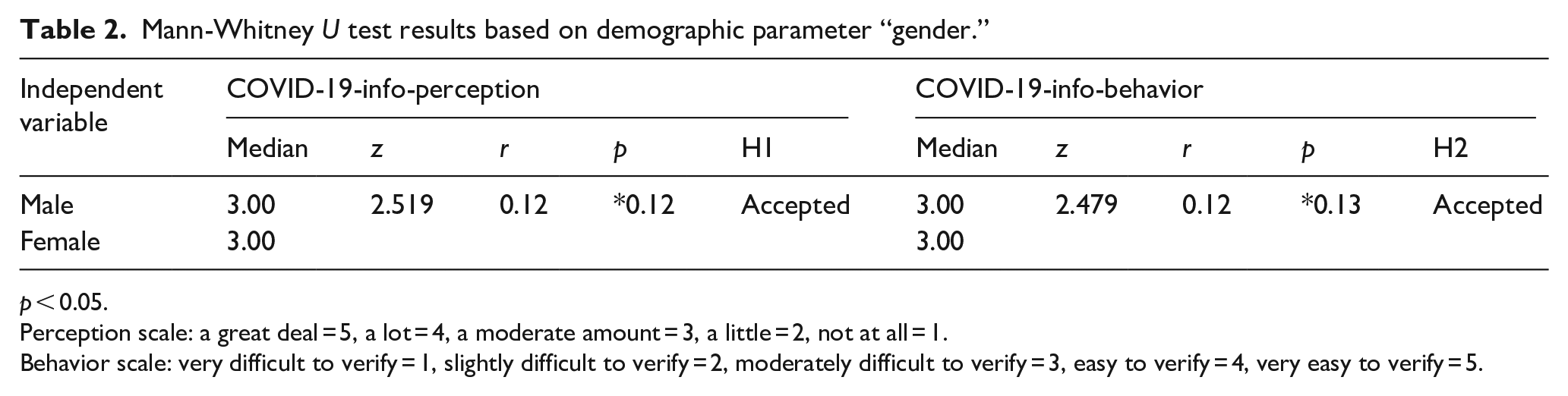
p < 0.05.
Perception scale: a great deal = 5, a lot = 4, a moderate amount = 3, a little = 2, not at all = 1.
Behavior scale: very difficult to verify = 1, slightly difficult to verify = 2, moderately difficult to verify = 3, easy to verify = 4, very easy to verify = 5.
The effect size measure would be considered as 0.1 ⩽ small, 0.3 ⩽ moderate, and 0.5 ⩽ large effect. The present study results reported an r value below 0.1, therefore, the difference effect size can be considered as small. Interestingly, in both cases of perception, the mean rank of respondents indicates that male respondents moderately perceived (Mean rank = 219) that made-up news was around them, and female participants perceived little (Mean rank = 190) that fake or made-up news was around them during COVID-19. Similarly, statistics for verification of COVID-19 information (behavior) show that male participants found it moderately difficult to verify the information when they received it. In contrast, female respondents exhibited lower levels of confidence and perceived that verifying the information was slightly difficult for them.
A Kruskal-Wallis H test was conducted to know the influence of participants’ age level on their perception of made-up news and information. The results (Table 3) depict significant impact, x2 (2, N = 399) = 31.187, p < 0.000, and differences in the made-up news perceptions over respondents’ age level. The age group 18–24 years perceived less (Md = 1.00) than other age groups (Md = 3.00) that made up news around them during the pandemic. A post-hoc test using Dunn’s test with Bonferroni correction showed significant differences between the group 25 and 35 and 18–24 years (p < 0.000), 35–50 and 18–24 years (p < 0.000), and between 51 and 65 and 18 and 24 years (p < 0.021). This means that the age group 18–24 years is significantly different from other age groups and perceived less that fake news was around them during the COVID-19 pandemic.
Kruskal Wallis test results based on demographic parameters “age, religion, and educational level” in relation to COVID-19 perception and behavior.
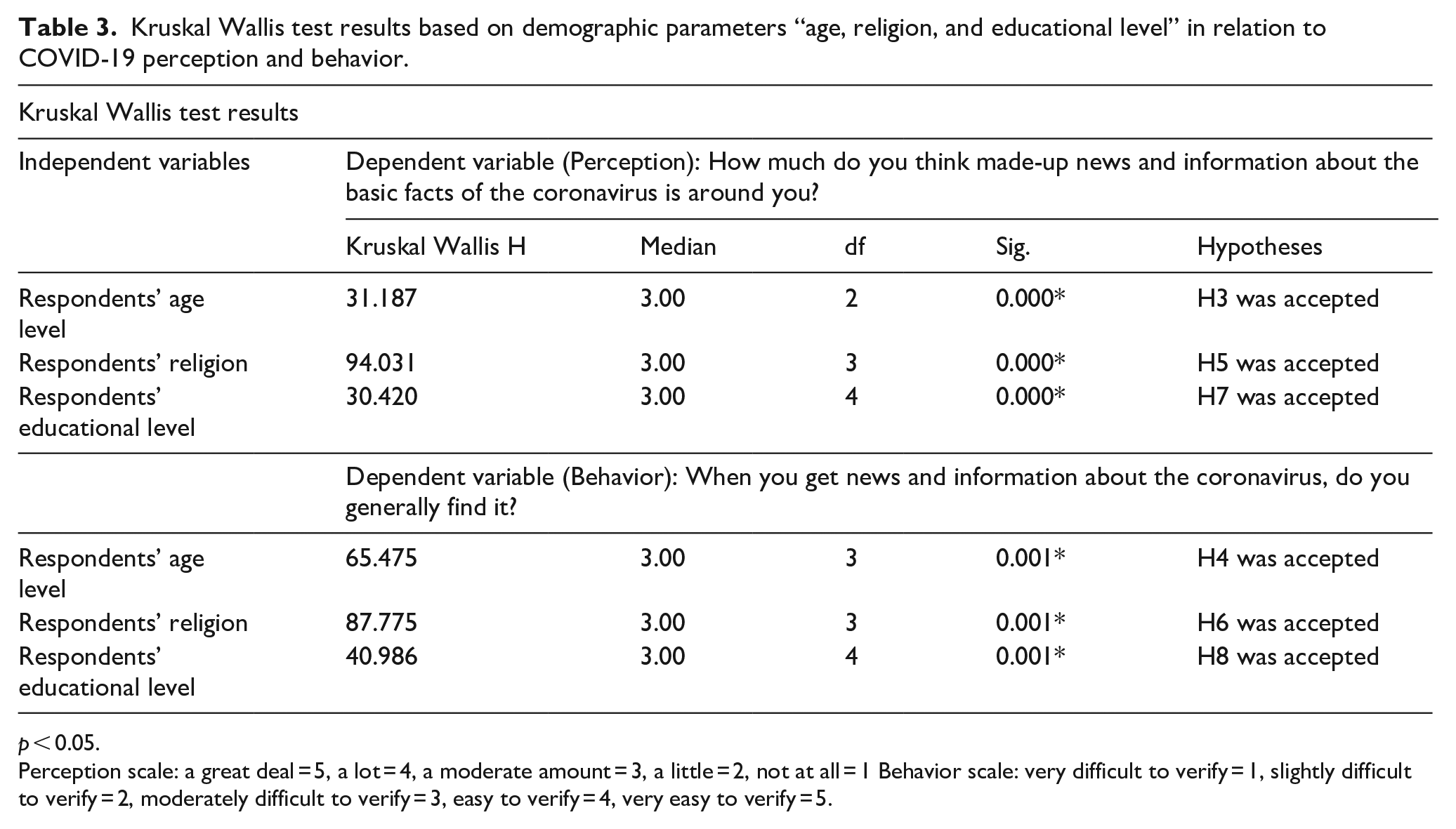
p < 0.05.
Perception scale: a great deal = 5, a lot = 4, a moderate amount = 3, a little = 2, not at all = 1 Behavior scale: very difficult to verify = 1, slightly difficult to verify = 2, moderately difficult to verify = 3, easy to verify = 4, very easy to verify = 5.
The results of the Kruskal Wallis test revealed that the religion of respondents is also a strong predictor of their perception of made-up news x2(3, N = 399) = 94.031, p < 0.000. Interestingly, the Hindus perceived most of the made-up news around them (Md = 5.00) than Muslims (Md = 3.00). To see the differences between groups a post-hoc test using Dunn’s test with Bonferroni correction was applied. The results show that significant differences were found only when pairing the religions “Hinduism” with “Islam” (p < 0.000). The data depicts that participants who belong to the religion Hinduism perceived more of the made-up news around them than their counterparts who belonged to religion “Islam.” The respondents from Christianity and Buddhism were considered outliers with only two responses each.
Similarly, the Kruskal Wallis test was applied to know the impact of respondents’ education on their perception of made-up news and information around them. The test revealed that “education” is also strongly associated with the perception of respondents’ made-up news and information around them, x2(4, N = 397) = 30.420, p < 0.000. However, the participants with high school, college, associate, and master’s degrees perceived at a moderate level (Md = 3.00) that the made-up news was around them during the pandemic than the respondents who hold bachelor’s degree (Md = 2.00, a little). Moreover, a post-hoc test using Dunn’s test with Bonferroni correction results found significant differences between two groups, high school, and associate degree holder participants (p < 0.017) and high school and master degree holder respondents (p < 0.000). Respondents with high school degrees perceived less made-up news and information than associate and master level degree holders. The other groups were not significantly different from each other.
The Kruskal Wallis H test was significant for the difference of opinions between respondents’ behavior and age levels. The results exhibit significant results, x2 (3, N = 399) = 65.475, p < 0.001. Three groups were significantly different from each other, such as age groups (25–34 and 18–24 years, (p < 0.000)) (35–50 and 18–24 years, (p < 0.000)) (51–65 and 18–24 years, (p < 0.000)). The overall findings analyze that younger respondents found COVID-19 information difficult to verify than older respondents. The results for other demographics such as “religion (p < 0.001)” and “educational level (p < 0.001)” are also statistically significant. With reference to religion parameters only one pair (Hinduism-Islam) opinions were significantly different (p < 0.001). Other groups did not show significant values (Figure 1). The results were significant based on education between found groups such as high school-associate degree (p < 0.000), high school-master or higher education (p < 0.000), bachelor-associate degree (p < 0.013), and bachelor-master or higher education (p < 0.003). The participants having school and bachelor-level education found it slightly and moderately difficult to verify COVID-19 information than other counterparts.
Findings and discussion
Almost 40% of the respondents perceive that there is “a great deal” of made-up news about COVID-19 with most participants (94.24%), initially believing the made-up news and information to be true before realizing it was fake. This situation creates concern when the data shows that less than 10% of the respondents were able to verify coronavirus-related information.
Our analysis found that there are significant differences in the perceptions of study participants about the made-up or fake news around them concerning demographic variables including education, age, gender, and religion. Prior studies support the results of our study. For example, Balakrishnan et al. (2022) review study reported that low levels of education, juniors in age, and males are more likely to spread fake news. On the contrary, our study found that younger participants of the study had less perception of the presence of fake news around them. Another similar study by Kim and Kim (2020) confirmed that older age groups are more inclined toward fake news than younger generations. With relevance to this, Balakrishnan et al. (2022) study also mentioned that younger people are good at hunting fake news and checking the credibility of digital information sources. In contrast to these results, Laato et al. (2020) measured a negative impact of age on sharing of fake news. A qualitative study brought the facts that young people believe that elderly people have less ability to combat fake news, on the other hand, older respondents experienced that the younger generation is more vulnerable to the fake world (Martínez-Costa et al., 2023).
The present study found that the education level of respondents is also a strong predictor of their perception of COVID-19 misinformation. The significant results of the Kruskal Wallis test (Table 3) revealed that respondents who achieved high school or above level education moderately believe that fake or made-up news was around them. Prior studies (Balakrishnan et al., 2022; Kim and Kim, 2020) confirm that participants with low education levels believe and spread fake news more than their counterparts (people with higher education). Another study found that respondents with a university education are more confident about spotting fake news (Martínez-Costa et al., 2023)
Similarly, the demographic variable “gender” also predicts significant differences between the opinions of study respondents. Our study highlighted that female participants perceived less than male participants that fake news was around them. These interesting results also resonate with the findings of (Kim and Kim, 2020) study. The researchers found that males were more inclined toward fake news than female respondents. Some other researchers (Laato et al., 2020) also observed that females are less likely to share fake news on social media but suffer from cyberchondria (panic searching behavior). Conversely, a prior study by Chen et al. (2015) investigated that females had more tendency to share made-up or fake news.
Religion is also a determinant of perception of made-up or fake news as evidenced by the present study analysis. Earlier research by Wasserman et al. (2021) confirms that people believe and share information when it comes from religious organizations. In relation to this, studies argued that belief in religious leaders and intuitive reasoning played a significant role in the perception of falsehood on social media (Froehlich, 2019; Pennycook and Rand, 2021). Additionally, the findings related to the differences between the perceptions of participants who belong to Hinduism and Islam have connections with the prior studies (Al-Zaman, 2021b; Badrinathan and Chauchard, 2021). The studies identified similar facts that a strong level of religiosity or affirmed belief is a strong predictor of penetration of social media misinformation. In relevance to our study, Al-Zaman (2021b) examined the social media analytics from 138 countries and found that India (where Hinduism is a dominant religion) is largely affected by the misinformation diffusion than other countries.
The findings suggest a concerning lack of information literacy, with a vast majority of individuals being susceptible to false information. However, the varying percentages across countries demonstrate the potential for targeted interventions and education efforts to improve individuals’ ability to identify and discern fake news from factual information.
Limitations
The present study was limited to the three most densely populated countries (Bangladesh, India, and Pakistan) from the South Asian region with shared socio-cultural heritage. The study was further limited by funding and travel limitations due to the series of lockdowns during the Covid period. Within India language limitations also played a critical role in selection of specific states. These limitations allowed the researchers, being citizens of these respective countries, to facilitate in-person data collection.
Conclusion
Our study investigated the perceptions and behavior of the rural population of South Asian countries (Bangladesh, India, Pakistan) about COVID-19 misinformation or fake news. The prevailing pandemic situation during the data collection period, illiteracy of the study participants, language barriers, sociological issues of gender, and religion, and geographic locations were limitations of the study.
The study found that the majority of respondents were unable to spot fake news easily. Similarly, a predominant finding is that participants believed initially made-up news and information to be true before realizing it was fake. Moreover, the study respondents fall on the quantum between the feelings of trust and fear in their emotional intelligence. The high levels of trust and fear show that study respondents initially found fake news to be true, however, they experienced fear or uncertainty upon realizing that it was fake. Additionally, the Mann Whitney U and Kruskal Wallis results revealed that there are statistically significant differences between the opinions of respondents based on demographic variables. The findings show that females, younger respondents, and participants with high school and bachelor degrees were more likely to perceive COVID-19 information around them. Additionally, females, younger respondents, and participants with high school and bachelor degrees found it more difficult to verify the COVID-19 information than respondents in other categories.
The results have significant implications for information professionals to play their active role in designing and implementing information literacy instruction programs with a specific focus on combating misinformation. The special information literacy instruction programs for the SA region should incorporate the components of critical thinking, digital literacy, fact-checking, and emotional intelligence. These instructional programs should be run by the public and academic libraries in the outreach areas of SA countries.
The study shall help government and non-government organizations in these countries deal with misinformation in rural areas. Moreover, the findings of the study will also help healthcare professionals, information professionals, social workers, extension workers, and policymakers to deal with the infodemic. It can also be used to develop health information literacy programs to educate the rural populations in these countries to cope with misinformation. A further study may be conducted to compare the findings of this study comparing the perceptions of urban populations in SA countries.
Supplemental Material
sj-pdf-1-lis-10.1177_09610006241241065 – Supplemental material for Dueling COVID-19 misinformation: Perceptions and behavior of the rural population from South Asian countries
Supplemental material, sj-pdf-1-lis-10.1177_09610006241241065 for Dueling COVID-19 misinformation: Perceptions and behavior of the rural population from South Asian countries by Bhakti Gala, Manika Lamba, Syeda Hina Batool, Md Anwarul Islam and Raj Kumar Bhardwaj in Journal of Librarianship and Information Science
Footnotes
Acknowledgements
We acknowledge the guidance received from Dr. Chu, Samuel KW, University of Hong Kong, and the support and contribution received from Ms. Prasadi Jayasekara Kanchana, University of Ruhuna, Sri Lanka and Ms. Helen Chan, University of Hong Kong for the completion of the ASIS&T South Asia Chapter Special Project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The financial support for the study was received from the Association for Information Science & Technology (ASIS&T, USA).
Supplemental material
Supplemental material for this article is available online.
Notes
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.