
Abstract
The study aimed at modeling the factors that influence health information avoidance behavior, as well as measuring and validating the stimulus organism response (S-O-R) theory. A seven-factor (information overload, information sources exposure, risk perception, health information anxiety, cognitive dissonance, sadness, and health information avoidance) measurement model was used to estimate the health information avoidance behavior using the structural equation modeling (SEM). The findings show that risk perception had a significant positive influence on sadness (β = 0.492, CR = 7.445, p < 0.05), information overload exerts a significant positive impact on cognitive dissonance (β = 0.174, CR = 2.192, p < 0.05) and sadness significantly influence health information avoidance (β = 0.174, CR = 2.342, p < 0.05). Information overload exhibits a positive, but statistically non-significant influence on health information anxiety (β = 0.83, CR = 1.094, p > 0.05). The findings of SEM demonstrate acceptable model fit indices: χ2 = 1.493, DF = 732; p = 0.000; IFI = 0.931; and TLI = 0.925, CFI = 0.930, SRMR = 0.045, RMSEA = 0.044. The study concludes that risk perception, sadness, and information overload are the main predictors of health information avoidance behavior. Other factors such as health information anxiety, exposure to different information sources, and cognitive dissonance had a non-significant impact on information avoidance behavior. The findings hold significant global relevance, potentially contributing to improved information-seeking behavior research. Our study also contributes to the advancement of the S-O-R (Stimulus-Organism-Response) framework
Keywords
Introduction
Information avoidance is a specific behavior where individuals actively choose not to seek out information, particularly when they perceive it might be unpleasant or unwanted (Sweeny and Miller, 2012). Information avoidance can manifest in two distinct ways: active and passive avoidance. Active avoidance refers to an intentional lack of information seeking, it happens when an individual deliberately takes steps to avoid seeking unwanted information, such as filtering out certain information or news sources or neglecting to seek information from reliable sources (Khaleel et al., 2020). Passive avoidance refers to an unintentional lack of information seeking. In this situation, individuals do not actively pursue relevant information, even if they have not necessarily made a conscious effort to avoid it. It mainly happens due to a lack of awareness about the information resources, their availability, or feeling overwhelmed by the flood of information, or simply not prioritizing information seeking. There are three main reasons behind individuals’ avoidance of information: (i) new information may change their perception and beliefs; (ii) new information may work or enforce to implement against their behavior; and (iii) new information might lead to unfavorable emotional attitudes (Link, 2021).
The widespread adoption of information and communication technologies has led to an exponential growth in the volume of information (Soroya et al., 2021). While social networking platforms like Facebook, Twitter, and YouTube offer a wealth of health information, they can also be a source of information overload and anxiety. This can lead to a phenomenon known as information avoidance, where individuals deliberately avoid health information (Soroya et al., 2021). Therefore, the frequency of health information avoidance is very high during the global health crisis due to different factors, such as information source exposures, information overload (Soroya et al., 2021), anxiety, cognitive dissonance (Song et al., 2021), low health literacy (Yoon and Lee, 2023), and low self-efficacy (Zhao and Cai, 2009) of consumers. Multiple factors contribute to health information avoidance, including environmental, physiological, psychological, cognitive, and personal (Chae and Lee, 2019). The abundance of online health information during global health crises presents a significant challenge. This unrestricted flow of information, lacking verification of source and accuracy, can be misleading and potentially detrimental to public health efforts (Jean Tsang, 2019; Link, 2021). Several studies indicated that individuals avoid health-related information that produces feelings of uncertainty and confusion (Miles et al., 2008). Many studies reported that refusal of health information about health screening and disease prevention (Howell and Shepperd, 2013b; Laato et al., 2020; Rimal and Real, 2003), as well as treatment avoidance (Golman et al., 2017) negatively affect people health.
Therefore, there is a need to explore health information avoidance behavior concerning public health because health information avoidance has been given less priority compared to health information seeking. Moreover, the risk factors of health information avoidance are not completely explored. Whereas, making informed health decisions requires access to and engagement with health information (Swar et al., 2017). It highlights the importance of collaboration between information professionals and the public. By working closely together, information professionals can gain a deeper understanding of people’s attitudes toward health information. This includes investigating the factors and motivations behind information avoidance behavior (Song et al., 2021). In this context, the present study will play a significant role in presenting the proposed framework based on the stimulus organism response (S-O-R) model that can provide a further roadmap to policymakers, health organizations, government, information professionals, and political leaders in terms of facilitating, promoting, and implementing effective health communication strategies, health information policies, procedures, and resources to overcome the health information avoidance behavior.
Therefore, the present study is conducted with the following objectives;
• To model the factors that influence health information avoidance behavior, as well as to measure and validate the stimulus organism response (S-O-R) theory among faculty members working in universities of Azad Jammu and Kashmir.
Theoretical framework
Numerous models and theories have been reported in the literature to understand human behavior, particularly information behavior. For example, the Comprehensive Model of Information Seeking (CMIS; Johnson et al., 1995; Johnson and Meischke, 1993) is a widely employed framework in information behavior literature (Choo, 2017; Deline and Kahlor, 2019; Li, 2023; Zhou et al., 2023). The Theory of Planned Behavior (TPB) is another widely used framework for understanding individuals’ information behavior. It provides a framework to predict behavior based on an individual’s attitude toward the behavior, subjective norms, and perceived behavioral control (Ajzen, 1991). It has been employed to examine various aspects, including the acceptance of information systems (Martono et al., 2020), and information-seeking and sharing behaviors (Mohammad et al., 2024; Shamlou et al., 2022). Health Belief Model (HBM), is another widely employed model, it was originally developed to understand health-related behaviors (Abraham and Sheeran, 2005), and its constructs (e.g. perceived susceptibility, perceived severity) have been widely adapted to explore information behavior, such as health information seeking (Mugunga, 2022; Zhao et al., 2022), social media use for health information (Arif et al., 2020; Liu and Wang, 2023) and health information avoidance (Chen et al., 2022). Risk Information Seeking and Processing (RISP) Model presented by Griffin, Dunwoody, & N et al. (1999) is another useful model that provides a framework for understanding risk information seeking and processing behaviors (Yang et al., 2014, 2022), such as air pollution (Acevedo et al., 2019), and health information avoidance during COVID-19 (Barbour et al., 2012; Link, 2021; Spleen et al., 2014).
The Stimulus-Organism-Response (S-O-R) is a framework that explains how individuals reach external stimuli. It offers a different perspective, examining how external stimuli elicit responses through internal processes (Mehrabian and Russell, 1974). The S-O-R framework has been successfully applied to understand consumer health information behavior (Ahn and Kahlor, 2020; Peng, 2022; Song et al., 2021; Soroya et al., 2021; Yang et al., 2021b), and information behavior during the COVID-19 pandemic (Kumalasari and Priharsari, 2023; Pandita et al., 2021; Song et al., 2021). Research consistently demonstrates the framework’s utility in explaining how S-O-R factors influence human information behaviors (Wu et al., 2023), such as health information management (Yang et al., 2021a), and health information avoidance and preventive behavior (Song et al., 2021; Soroya et al., 2021; Wu et al., 2023). Mehrabian and Russell (1974) introduced the S-O-R framework, positing that stimuli (S) constitute a collection of sensory predictors in a particular environment, and information overload denotes associations between stimulus variables. Organism (O) exhibits emotional responses to their surroundings, which can be further divided into three categories: levels of happiness and sadness, levels of cognitive activities, and levels of emotional restraint. Responses (R) show avoidance behavior. Researchers in information behavior, public health, and health communication have extensively employed (S-O-R) framework to analyze how external stimuli (information), individual characteristics (organism), and responses (seeking, learning, avoidance) interact and influence behavior (Link, 2021; Liu et al., 2021, 2024).
However, each model has limitations. For example, HBM emphasizes individual perceptions of susceptibility, severity, benefits, and barriers to influence health behaviors. But it does not fully account for social influence and behavioral intentions in the context of health information seeking (Abraham and Sheeran, 2005). Similarly, TPB primarily focuses on predicting behaviors based on attitudes, subjective norms, and perceived behavioral control. While effective for understanding deliberate, socially influenced behaviors, the TPB’s focus on conscious decision-making limits its applicability to habitual or emotionally driven actions (Ajzen, 1991). The S-O-R framework, while useful, may not adequately capture the cognitive processes involved in health information behavior (Mehrabian and Russell, 1974). To address this limitation, this study incorporates cognitive dissonance into the S-O-R model to enhance its explanatory power. Moreover, given its applicability and wide adoption during the COVID-19 pandemic to assess health information behavior (Ma et al., 2024; Song et al., 2021), particularly information avoidance (Kumalasari et al., 2022; Soroya et al., 2021), the S-O-R framework, is well-suited in the context of this study for predicting health information avoidance behavior. Notably, constructs like information overload, anxiety, and avoidance have been explored within this framework by other researchers (Song et al., 2021; Soroya et al., 2021). Building on this foundation, we propose a conceptual framework based on the S-O-R framework, hypothesizing that emotions such as anxiety, sadness, cognitive dissonance can be considered internal states (organisms) that are influenced by external stimuli (information overload, information sources exposure, risk perception) and can lead to specific responses, such as health information avoidance (as shown in Figure 1).
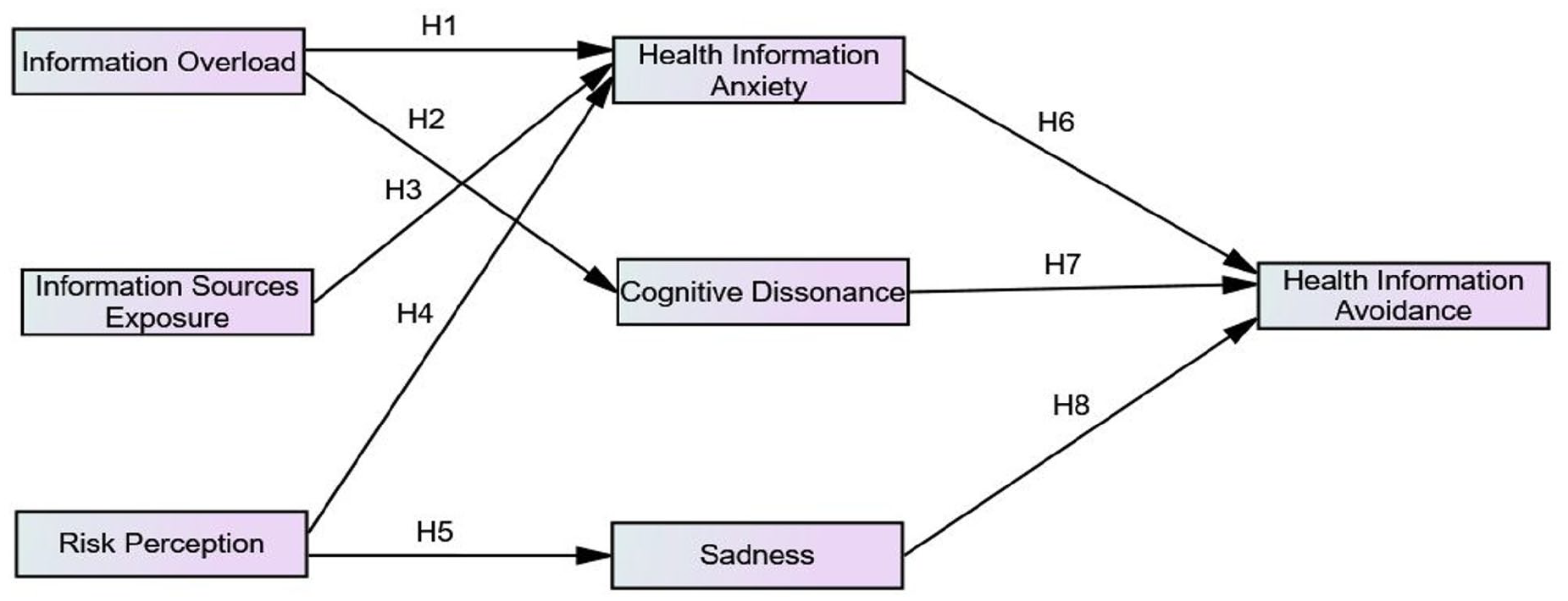
The S-O-R-based conceptual framework and subsequent hypothesis development.
Information overload and health information anxiety
People who use social media channels more frequently are more likely to feel overwhelmed by information compared to those who use them less (Belabbes et al., 2023). The exposure to information from social networks is statistically correlated with information overload which develops stress and anxiety among individuals (Jia et al., 2023; Lee et al., 2016). The vast amount of information readily available online can contribute to feelings of information overload (Hall and Walton, 2004; Jiang and Beaudoin, 2016). Consumer involvement with various health-related sources of information enhances the probability of anxiety and information explosion (Bapat et al., 2017; Zhao and Cai, 2009). Similarly, Swar et al. (2017) reported that information overload positively influences psychological factors that include; sadness, and anxiety. Moreover, the conditions of dissonance, confusion, stress symptoms, anxiety and low motivation are the result of information overload (Belabbes et al., 2023; Eppler and Mengis, 2004; Kim and Cameron, 2011; Schick et al., 1990). Several researchers established the relationship between information overload and health information anxiety (Bawden and Robinson, 2009; Charpentier et al., 2022; Jia et al., 2023; Williamson et al., 2012b).
Information overload and cognitive dissonance
The prior research studies reported that information overload positively influences cognitive dissonance (Mehrabian and Russell, 1974; Song et al., 2021). The cognitive dissonance theory proposes that encountering two psychologically inconsistent cognitions (thoughts, beliefs, or attitudes) can induce a state of dissonance in an individual (Harmon-Jones and Mills, 2019; Thamrin et al., 2023). Social networking sites offer a wealth of information, but the sheer volume and often unfiltered nature of content can lead to information overload. Users may struggle to distinguish reliable sources from misinformation, leading to cognitive dissonance (mental conflict) as they encounter conflicting viewpoints. This can ultimately make it difficult for individuals to find and utilize helpful information about mental health (Lv and Liu, 2022; Thamrin et al., 2023; Yahya and Sukmayadi, 2020). Several factors can contribute to cognitive dissonance, including negative emotions like frustration, anxiety, and encountering aggressive attitudes (Fontanari et al., 2012). In the era of digital disruption information explosion is linked with cognitive dissonance (Morvan and O’Connor, 2017; Yahya and Sukmayadi, 2020).
Information sources exposure and health information anxiety
Several studies identified the positive relationship between information overload and social media use in the context of the global health crisis (Link, 2021; Song et al., 2021). The uses of information sources positively influence the information anxiety of health information seekers (Kim and Cameron, 2011). The generation of information from different information sources; newspapers, social media, health websites and healthcare providers developed uncertain feelings such as sadness, and anxiety which are the main contributors to health information anxiety (Charpentier et al., 2022; Sultana et al., 2023). Several studies (Nekliudov et al., 2020; Shabahang et al., 2020) reported that frequent online health information seeking from different information sources is positively associated with information anxiety.
Risk perception and health information anxiety
Risk refers to hazards that exist in our surroundings. Every individual has their beliefs about risk perception based on past experiences and personality traits (Butler and Mathews, 1987; Zhao and Cai, 2009). However, the variables; individual information gathering capacity in RISP, and self-efficacy beliefs in CMIS exhibit certain behavior under control and threat conditions that positively influence individual health information anxiety (Hwang and Jeong, 2023; Wang et al., 2021). The literature indicated that perceived risk develops negative psychological conditions that increase the level of anxiety among health information seekers (Zhou et al., 2023). According to risk perception attitude (RPA), risk is a factor that is associated with information acquisition anxiety (Rimal and Real, 2003). For example, Zhao and Cai (2009) stated that smokers’ awareness of the risk of lung cancer positively influences their level of anxiety in the information acquisition process. Therefore, we proposed that risk perception is positively associated with health information anxiety.
Risk perception and sadness
The perceived threat is a component of the environmental exposure, from which a huge amount of information is received that brings change into the internal state of an individual in response to an increase in their sadness level (Chen et al., 2009; Eppler and Mengis, 2004; Song et al., 2021). The threat of disease negatively affects people’s psychology which may contribute toward the state of sadness. Individuals who are less interactive with society are likely to perceive psychological problems like anxiety and sadness (Mehrabian and Russell, 1974). Similarly, information received from multiple channels increases the chances of health-related threats (Bawden, 2001; Sairanen and Savolainen, 2010).
Health information anxiety and health information avoidance
Information anxiety arises from the widening gap between our perceived knowledge and the perceived need for more knowledge (Eklof, 2013). As discussed by Manheim (2014) information anxiety is composed of different types of negative feelings, that result in avoidance behavior and undesired information. The field of health communication dealt with information avoidance behavior for the last 50 years (Charpentier et al., 2022). Individuals are confined to specific sources to search for them to fulfill their information needs and they ignore all other irrelevant information sources that cause anxiety (Sultana et al., 2023). The health-related information collected from different media increases information anxiety and information avoidance behavior (Bawden, 2001; Sairanen and Savolainen, 2010). Negative feelings like fear and anxiety are also strongly linked with information avoidance behavior (Tan-Kristanto and Kiropoulos, 2015).
Cognitive dissonance and health information avoidance
According to Harmon-Jones and Mills (2019), Jean Tsang (2019), and Thamrin et al. (2023) cognitive conflict is an uncertain position during which individuals are animated to decrease it whenever it occurs. Furthermore, cognitive disagreement lowers the frequency of people’s information acceptance responses (Sachdeva, 2022). As stated by Gaspar et al. (2016), individuals prevent themselves from seeking health information about the harmful aspects of a particular disease because of cognitive conflict (Fuertes et al., 2020; Golman et al., 2017; Harmon-Jones and Mills, 2019). Cognitive dissonance is strongly associated with people’s behavior. According to the dissonance theory, there are different ways to lower dissonance that may involve individuals’ perception of seeking information about a particular disease or risk during dissonance conditions. The regular fluctuations in the behavior of individuals during a dissonance state motivate them to accept or reject health information (Connole et al., 1977; Cotton and Hieser, 1980; Oshikawa, 1969).
Sadness and health information avoidance
The risk perception attitude framework suggests that individuals may be more likely to downplay or disregard information about potential threats, particularly when such information evokes negative emotions (Rimal and Real, 2003; Zhao and Cai, 2009). Negative perceptions of individuals encourage them to avoid seeking health-related information (Bapat et al., 2017; Sultana et al., 2023). In most of the situations, negative feelings develop due to health threats. For example, when faced with incurable and fatal health problems, some individuals may feel a lack of hope or control, leading to decreased motivation to seek health information (Dwyer et al., 2015; Howell and Shepperd, 2013a; Melnyk and Shepperd, 2012; Sweeny and Miller, 2012). Similarly, breast cancer threats can prevent females from seeking health information (Ek and Heinström, 2011; Melnyk and Shepperd, 2012). Several factors can discourage individuals and act as barriers to information seeking. These factors include emotional distress, perceived health risks associated with the topic, and emotional instability (Swar et al., 2017).
Hypotheses of the study
The following hypotheses are proposed based on the S-O-R conceptual framework (as shown in Figure 1).
H5. Risk perception (RIS) has a significant influence on sadness (SAD).
Research methodology
A cross-sectional survey design was employed to collect data from faculty members at five public sector universities in Azad Jammu and Kashmir, Pakistan. The sample included both male and female participants. These universities are (i) University of Poonch (ii) Mirpur University of Science and Technology, (iii) University of Azad Jammu & Kashmir (iv) University of Kotli, and (v) Women University Bagh.
The State of Azad Jammu and Kashmir (AJ&K) is a self-governing entity with its own constitution (enacted in 1974), president, prime minister, parliamentary assembly, and judiciary. It covers an area of 84,471 square miles and is located northeast of Pakistan and northwest of India. Russia, China and Afghanistan are located at the North Pole of the AJ&K. The government of AJ&K was established on October 24, 1947. The literacy rate in AJ&K is 70% (Dar, 2003; Snedden, 2017).
Data collection tool
A two-part questionnaire was developed based on a thorough review of relevant literature (Li, 2023; Link, 2021; Narayan et al., 2011; Park et al., 2023; Soroya et al., 2021; Soroya and Faiola, 2023; Williamson et al., 2012b; Zhou et al., 2023) and assessing the health information avoidance situation in the participating universities. The first part comprised questions relating to demographic information such as gender, age, qualification, discipline, geographical area, and health status of the respondents. The second part comprised sub-scales relating to seven components of the proposed framework based on the S-O-R framework (as shown in Figure 1). The construct’s information overload’, “information sources exposure” and “cognitive dissonance” were measured using five items each. The constructs “risk perception,” “sadness,” and “health information avoidance” were measured using six statements on each construct. However, “health information anxiety” was measured using seven statements. Overall, the questionnaire comprised seven constructs and 41 statements.
Sample size calculation
To determine the required sample size, a medium effect size of 0.3 (conventionally: small. 0.1, medium. 0.3, large. 0.5) was estimated. Given the model’s complexity (seven latent and 40 observed variables), a desired statistical power of 0.95 (conventionally, >0.80) (Cohen, 1988), and an alpha level of 0.05, the “A-Priori Sample Size Calculator for Structural Equation Models” (Soper, 2020) determined a minimum sample size of 247 participants.
Data collection process
Data collection for this study occurred between January and April 2024. A purposive sampling approach was employed to collect data from faculty members working at universities within Azad Jammu and Kashmir. The research team approached 500 faculty members and provided them with a copy of the questionnaire. These copies were provided to them in university libraries, faculty hostels, faculty common rooms, and faculty offices in the departments. Moreover, an online version of the questionnaire was developed using Google Forms. A link to the online version was given to only those respondents who preferred the online version. Out of the 500 questionnaires distributed (both online and physical), we received 268 responses. Following an initial screening process, 8 questionnaires were excluded due to incomplete data and having outliers. This resulted in a final sample of 260 valid responses for data analysis, translating to a response rate of 52%. The larger sample size provides more statistical power.
Reliability and validity measures
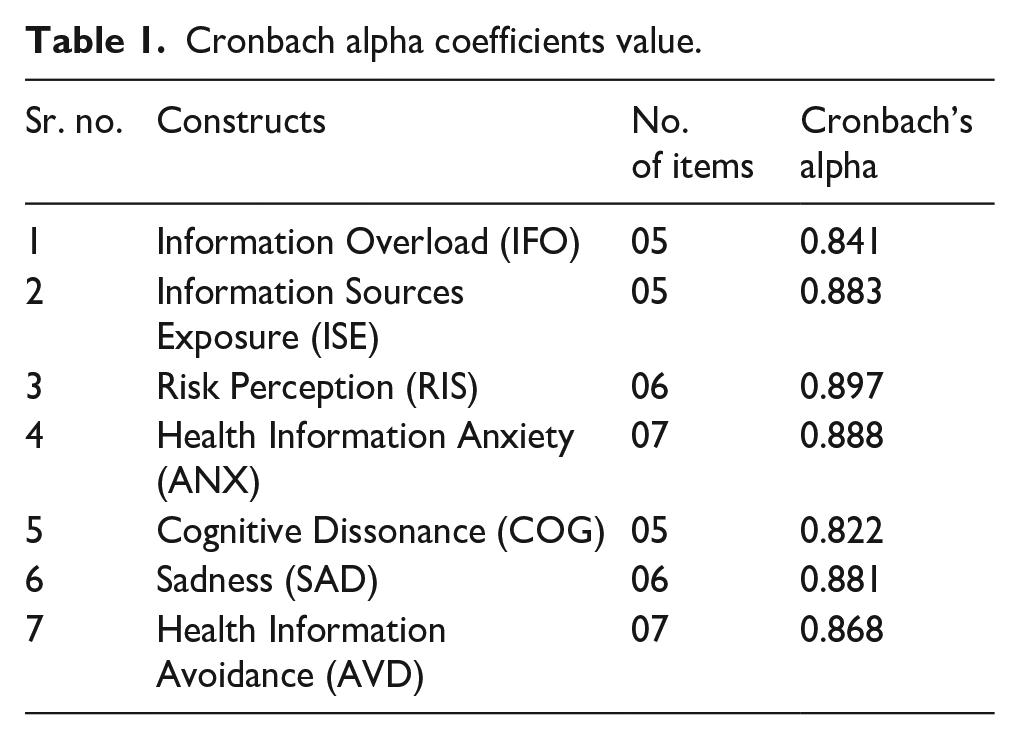
To assess the questionnaire’s reliability, three experts in information management, health communication, and public health conducted a pre-test. To improve the flow and clarity of the text, minor adjustments were made. This involved rearranging some sentences and rephrasing specific phrases to enhance overall readability. The questionnaire was pilot-tested with the first 30 responses. To assess the questionnaire’s reliability, we employed Cronbach’s Alpha, a statistical measure of internal consistency. This analysis yielded a score of 0.862 for the 41 statements across the seven constructs, indicating good reliability. Cronbach’s alpha coefficients for each construct measured in this study are reported in Table 1.
Cronbach alpha coefficients value.
Construct reliability and validity
Construct reliability refers to the consistency and precision of a measure in representing the underlying construct. Two popular measures are Composite Reliability (CR) which is a commonly used measure of internal consistency, and Maximal Reliability MaxR(H) which provides a conservative estimate of reliability. Both are used to evaluate the reliability of a scale. The estimation showed that the CR values for latent constructs IFO (0.770), ISE (0.839), and RIS (0.867) were above the acceptable threshold of 0.7. The MaxR(H) values for IFO (0.845), ISE (0.890), and RIS (0.905) also indicated acceptable reliability. Overall, the MaxR(H) values for all constructs ranged from 0.845 to 0.905, suggesting good construct reliability.
Univariate and multivariate normality assessment
Assessing normality is important in SEM as violations can compromise parameter estimates, standard errors, and hypothesis testing. To evaluate normality, we assessed skewness and kurtosis using maximum likelihood estimation (MLE). Outliers (n = 4) were identified and removed using Mahalanobis d-squared (observations farthest from the centroid). All variables met the accepted thresholds for skewness (<3; Kline, 2023), kurtosis (<7), and multivariate kurtosis (<5; Yuan et al., 2005) indicating reasonable symmetry and adherence to univariate and multivariate normality assumptions (West et al., 1995).
Data analysis procedure
Data analysis was performed using statistical package for social sciences (SPSS) version 26. Descriptive statistics were employed to summarize demographic information, with results reported as percentages and frequencies. Chi-square tests were utilized to assess potential differences in the distribution of male and female participants across various categories, including age, qualifications, discipline, geographical location, and health status. To test the research hypotheses and estimate the measurement model, Analysis of Moment Structures (AMOS) software was used. Confirmatory Factor Analysis (CFA) was employed to assess the relationships among latent variables and their corresponding indicators. Finally, a Structural Equation Model (SEM) was used to evaluate the overall validity of the proposed hypotheses. A significance level of alpha <0.05 was adopted to determine the significant level.
SEM is a powerful tool for modeling complex relationships, allowing for the simultaneous examination of both observed and latent variables. It enables hypothesis testing and model evaluation, offering a more sophisticated approach than traditional methods like regression. While SEM has limitations, including model specification, sample size requirements, and assumptions about the normality of data and linearity of relationship. We have carefully addressed these limitations in our study. Data normality was assessed using maximum likelihood estimation (MLE), with outliers identified and removed using Mahalanobis distance. The sample size was estimated with a statistical power of 0.95 using the sample size calculator. Construct reliability was ensured through composite and maximal reliability estimates. Model fit was evaluated using absolute fit indices (χ2, RMSEA) and additional fit (SRMR, IFI, TLI, CFI).
Ethical approval
The study was started after the approval from the Departmental Research Committee (DRC) of the Department of Information Management, The Islamia University of Bahawalpur, Pakistan. The study adhered to ethical research principles by ensuring informed consent from all participants. Participation in the study was voluntary, and participants could withdraw at any time without providing a reason.
Findings
Demographic information
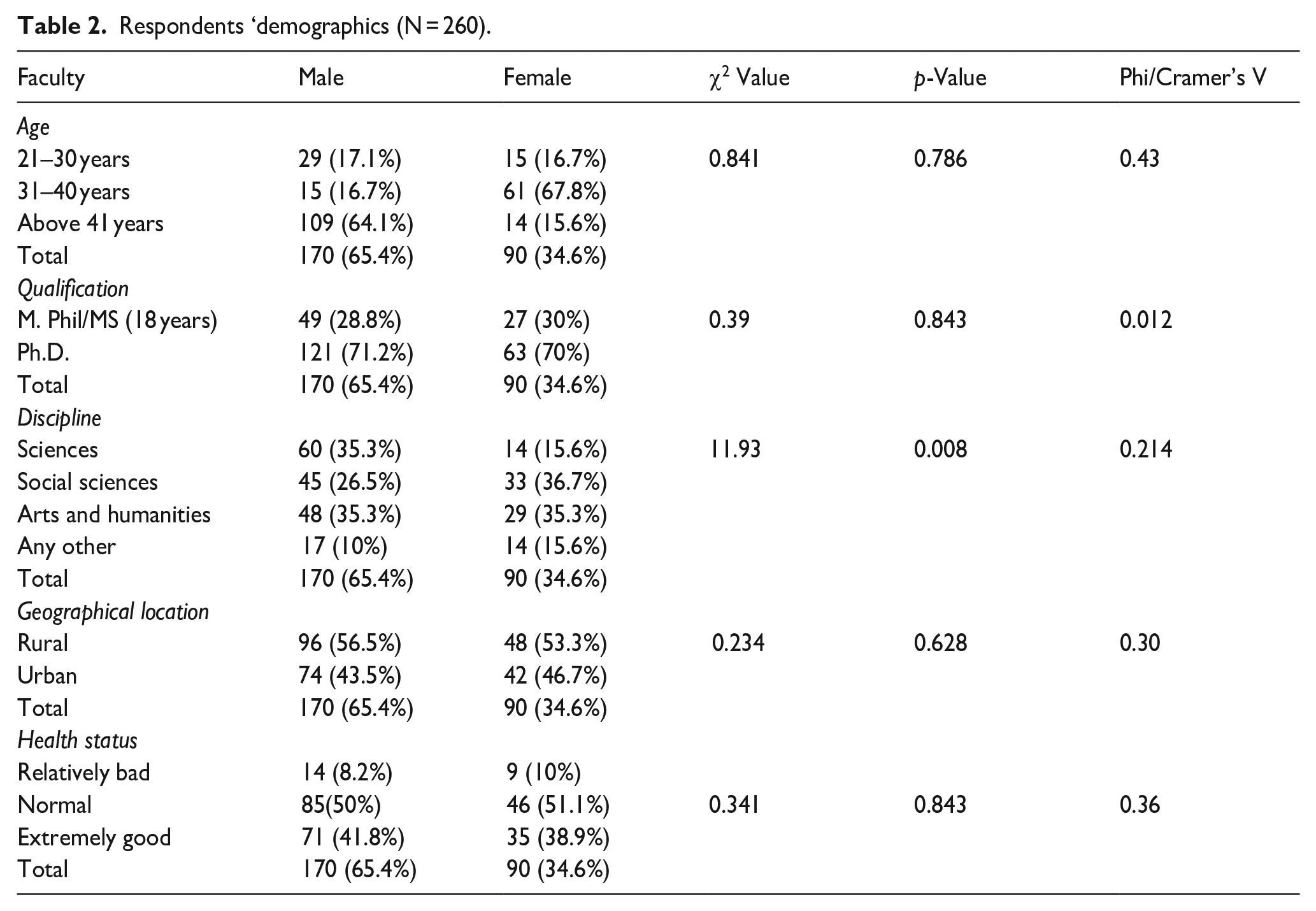
Of the 260 respondents, the majority 170 (65.4%) were males and 90 (34.6%) were females. Using Chi-square, we found a statistically non-significant difference in the distribution of males and females in different age groups (χ2 = 0.841, p = 0.786, phi’s value = 0.43). We also found a statistically non-significant difference in the qualifications of male and female respondents (χ2 = 0.39, p = 0.0843, phi’s value = 0.012). For example, the majority (121 or 71.2%) of male and (63 or 70%) of female respondents held PhD degrees. Our data showed similar percentages of respondents with M.Phil. qualifications: males (49 or 28.8%) and females (27 or 30%).
A significant difference was found between respondents’ genders and their field of study (χ2 = 11.93, p = 0.008, phi’s value = 0.214). In the sciences, males formed the majority (60 or 35.3%) compared to females (14 or 15.6%). In the social sciences, we found a more balanced distribution with (45 or 26.5%) males and (33 or 36.7%) females. In our cohort, both genders were least represented in other fields (such as management, engineering and agriculture) with only (17 or 10%) males and (14 or 15.6%) females. We found no significant difference in the distribution of gender in rural and urban areas (χ2 = 0.234, p = 0.628, phi’s value = 0.30), as well as health status (χ2 = 0.341, p = 0.843, phi’s value = 0.36; Table 2).
Respondents ‘demographics (N = 260).
Confirmatory factor analysis (CFA)
A seven-factor measurement model for IFO, ISE, ANX, COG, RIS, SAD, and AVD was estimated by applying CFA (Figure 2).
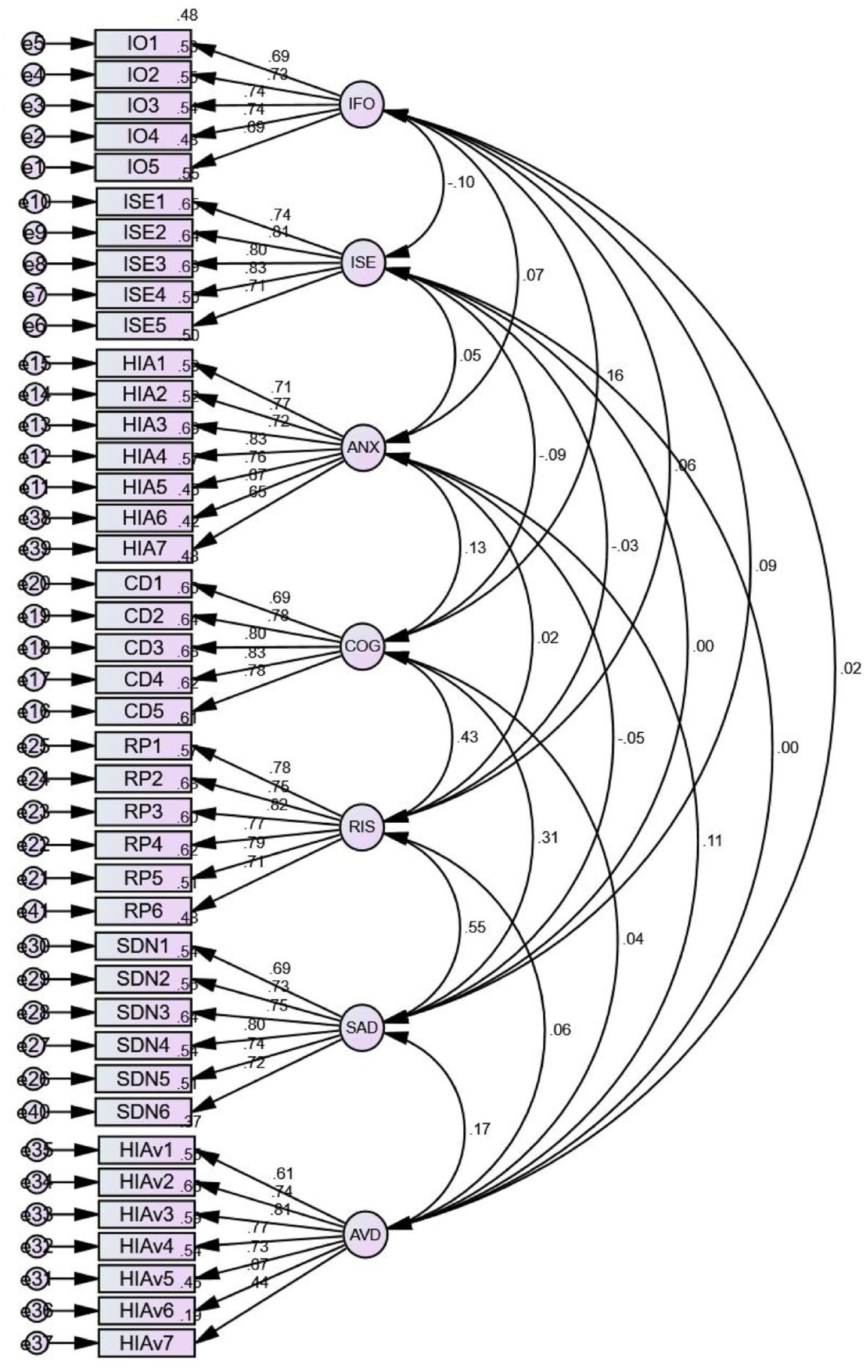
Confirmatory factor analysis (CFA) estimating the constructs (N = 260).
Regression weights
Figure 2 presents the standardized regression weights for the construct loadings. The path coefficients for the latent variables (IFO, ISE, ANX, COG, RIS, SAD, and AVD) ranged from β = 0.61 to β = 0.83. The latent variables IFO, ISE, and COG were measured using five indicators with loadings between β = 0.69 and β = 0.83, indicating strong construct validity. ANX was measured by seven items with loadings ranging from β = 0.65 to β = 0.83, demonstrating adequate construct reliability. RIS, SAD, and AVD were each assessed using six items with loadings between β = 0.61 and β = 0.82, suggesting good construct representation.
Estimation of correlation
The standardized correlations among the seven latent variables are presented in Figure 2. A negative correlation (β = −0.10) was found between IFO and ISE. The latent variables ISE and ANX (β = 0.06), ANX and COG (β = 0.13), SAD and AVD (β = 0.17) were weakly correlated with each other. The correlation between COG and RIS (β = 0.43) was moderately strong. However, RIS had a strong positive correlation with SAD (β = 0.55). We found a weak correlation between the latent variables that is, IFO and ANX (β = 0.07), ANX and RIS (β = 0.02), RIS and AVD (β = 0.06), IFO and COG (β = 0.16), COG and AVD (β = 0.04), IFO and RIS (β = 0.06), ANX and AVD (β = 0.11), IFO and SAD (β = 0.09), IFO and AVD (β = 0.02). On the other hand, ISE and COG (β = −0.9), ISR and RIS (β = −0.03), and ANX and SAD (β = −0.05) were weakly negatively correlated. The construct COG and SAD (β = 0.31) had a moderately strong correlation with each other.
Model fit indices for CFA
Model fit indices indicated acceptable model fit: χ² = 1.424, df = 758, p = 0.000, RMSEA = 0.040, CFI = 0.938, IFI = 0.933, and TLI = 0.939.
Structural equation model
Structural equation modeling (SEM) was employed to measure and validate the S-O-R framework of health information avoidance behavior and to test the study’s hypotheses. The path coefficient values of constructs (IFO, ISE, ANX, COG, RIS, SAD, and AVD) ranged between β = 0.62 and β = 0.83, showing good loadings on the constructs. Regression values of the item’s loadings on the constructs IFO, ISE and COG ranged between β = 0.69 and β = 0.83, showing strong loadings on the constructs. Similarly, item loadings on the constructs ANX, RIS, SAD and AVD ranged between β = 0.62 and β = 0.83, indicating good factor loadings (Figure 3).
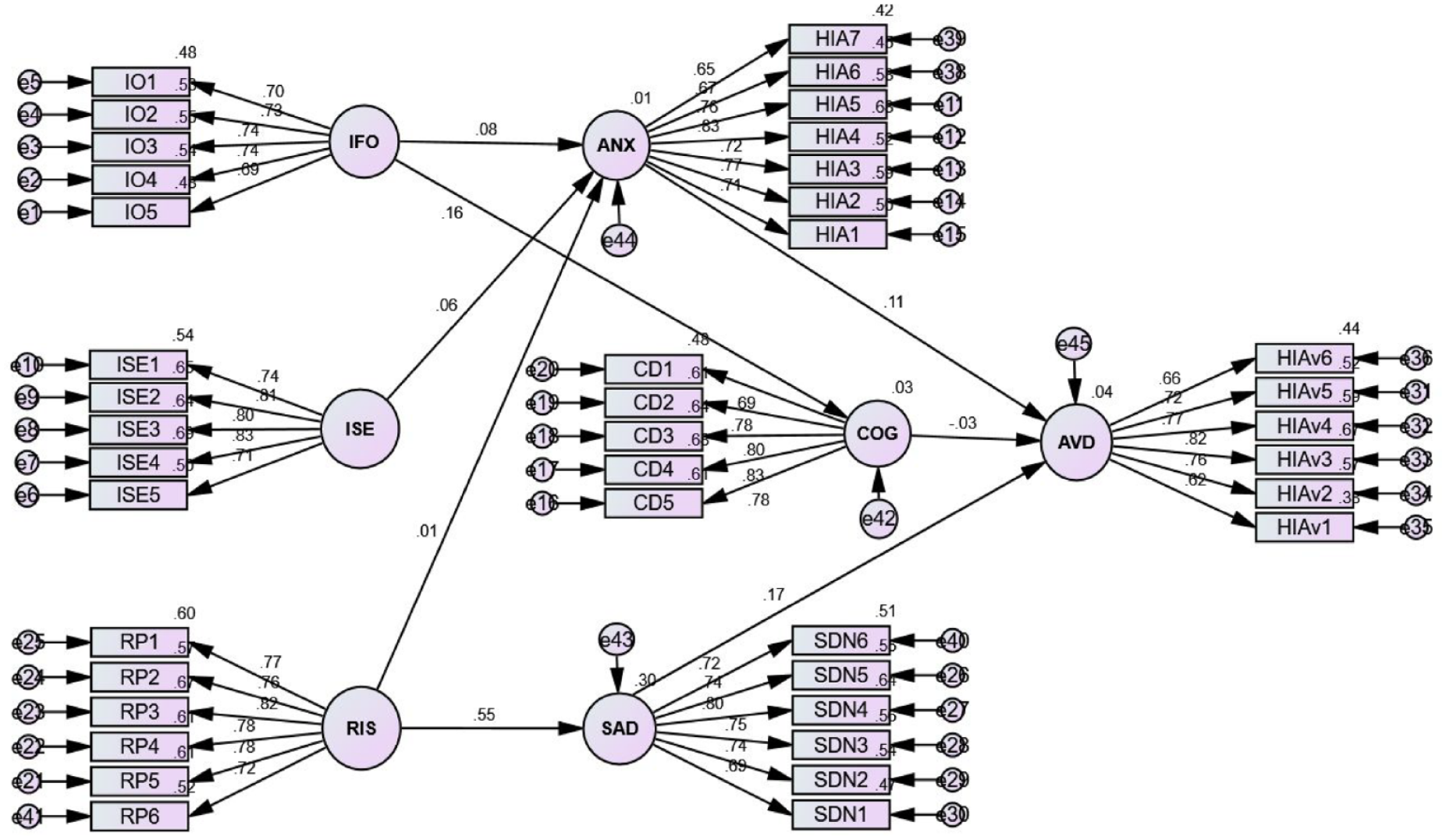
Structural Equation Model estimating the health information avoidance behavior (N = 260). Constructs: Information Overload (IFO), Information Sources Exposure (ISE), Risk Perception (RIS), Health Information Anxiety (ANX), Sadness (SAD), Cognitive Dissonance (COG), Health Information Avoidance (AVD). See detail in Annexure 1.
Our structural equation model suggests that ANX, COG, and SAD act as intermediary factors. It partially explains how IFO, ISE, and RIS can lead to AVD (Figure 3). The estimation indicates that IFO (β = 0.08), ISE (β = 0.06) and RIS (β = 0.01) had a positive influence on ANX (as shown in H1, H3, H4). Similarly, RIS (β = 0.55) had a positive influence on SAD (as shown in H5), and IFO had a positive influence on COG (β = 0.16) (as shown in H2). However, COG had a negative influence on AVD (β = − 0.03). On the other hand, ANX (β = 0.11), and SAD (β = 0.17) had a positive influence on AVD (as shown in H6 and H8).
Multiple squared correlations
The squared multiple correlations values showed that ANX accounts for only a 1% variance in the relationship between IFO, ISE, RIS, and AVD. On the other hand, SAD accounts for a 30% variance in the relationship between RIS and AVD. COG accounts for a 3% variance in the relationship between IFO and AVD (Figure 3).
Standardized regression weights and hypothesis testing
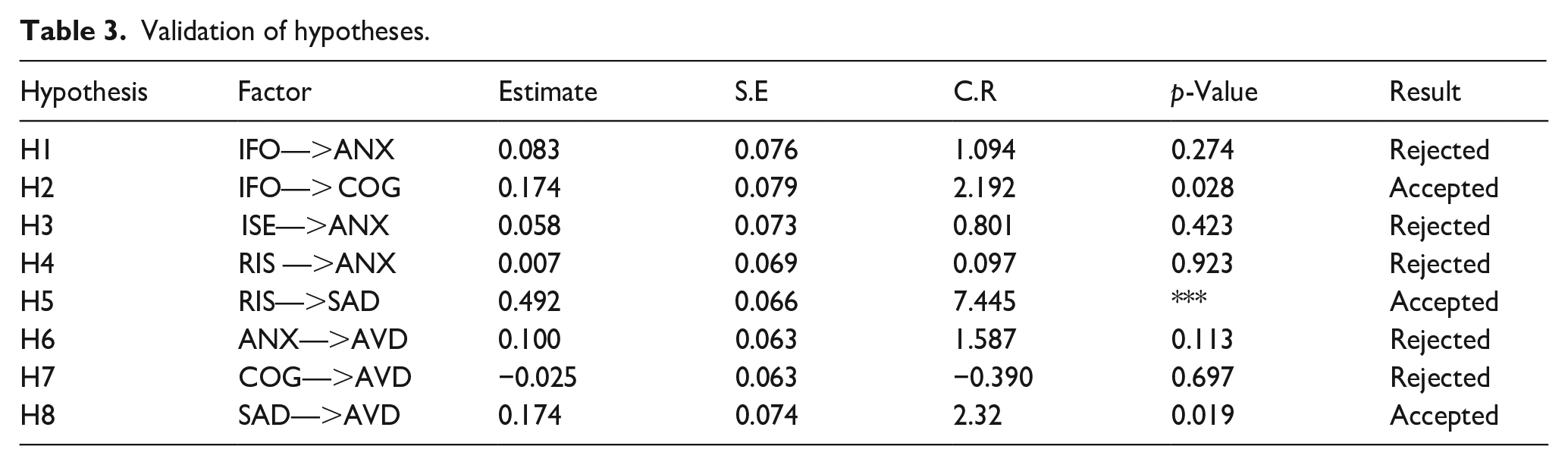
Several statistical measures play a crucial role in evaluating the support for the research hypotheses. These included the standardized regression estimate, standard error (SE) for variable measurement, critical ratio (CR), and the level of significance among the factors (as presented in Table 3). Table 3. indicates that RIS (β = 0.492, CR = 7.445, p < 0.05) exert a significant positive influence on SAD (Testing: H5), and IFO exhibits a significant positive influence on COG (β = 0.174, CR = 2.192, p < 0.05) (Testing: H2). Similarly, SAD significantly influences AVD (β = 0.174, CR = 2.32, p < 0.05) (Testing: H8). On the other hand, IFO (β = 0.83, CR = 1.094, p > 0.05), ISE (β = 0.58, CR = 0.801, p > 0.05), and RIS (β = 0.007, CR = 0.69, p > 0.05) exert positive but statistically non-significant influence on ANX (Testing: H1, H3, H4,). Furthermore, we found a positive but non-significant influence of ANX on AVD (β = 0.100, CR = 1.587, p > 0.05; Testing: H6). On the other hand, COG had a negative non-significant influence on AVD (β = −0.025 CR = −0.390, p > 0.05; Testing: H7).
Validation of hypotheses.
Model fit indices
We employed absolute fit (χ2, RMSEA) and additional fit (SRMR, IFI, TLI, CFI) measures to assess how well the proposed theoretical model aligns with the observed data. Generally, accepted cutoffs are IFI, TLI, and CFI values ⩾0.90, and an SRMR ⩽ 0.08 (Hu and Bentler, 1999). The goodness of fit indices suggests a good fit for the model: χ2 = 1.493, DF = 732; p = 0.000; IFI = 0.931; and TLI = 0.925, CFI = 0.930, SRMR = 0.045, RMSEA = 0.044.
Discussion
Our study estimated health information avoidance behavior among university faculty members through a seven-factor measurement model (information overload, information sources exposure, risk perception, health information anxiety, cognitive dissonance, sadness and health information avoidance). These factors were based on the stimulus organism response model (S-O-R). Several studies have attempted to validate the S-O-R framework predicting health information avoidance behavior (Li, 2023; Song et al., 2021; Soroya et al., 2021). Based on the conceptual framework (Figure 1), we developed eight hypotheses (H1 to H8). Overall, our analysis validates three hypotheses (H5, H2, & H8) that is, risk perception (RIS) has a positive influence on sadness (SAD), information overload (IFO) has a positive influence on cognitive dissonance (COG), and sadness (SAD) has a positive influence on health information avoidance (AVD). Although we found a positive influence of (H1) information overload (IFO) on health information anxiety (ANX), (H3) information sources exposure (ISE) on health information anxiety (ANX), (H4) risk perception (RIS) on health information anxiety (ANX), (H6) health information anxiety (ANX) on health information avoidance (AVD). However, this influence was statistically non-significant. On the other hand, H7 cognitive dissonance (COG) had a statistically negative influence on health information avoidance (AVD). Therefore, these five hypotheses (H1, H3, H4, H6, H7) could not be validated due to the hypothesized relationships between the factors were not statistically significant at the chosen alpha level. The results of the Structural Equation Modeling (SEM) analysis indicate an acceptable overall fit of the proposed model to the data: χ2 = 1.493, DF = 732; p = 0.000; IFI = 0.931; and TLI = 0.925, CFI = 0.930, SRMR ⩽ 0.08, RMSEA = 0.044, suggesting that the hypothesized relationships between the constructs in the S-O-R theory are supported within the context of this study’s population and setting.
Our findings are consistent with the findings of previous studies that risk perception positively influences health information anxiety (Hwang and Jeong, 2023; Song et al., 2021; Zhou et al., 2023). This finding reinforces the notion that perceiving oneself at greater risk for health problems can increase anxiety around health information. Furthermore, our findings that information overload significantly influences cognitive dissonance, support the findings of a previous study (Song et al., 2021). This indicates that seeking health information from a flood of information might create a state of mental discomfort due to potentially conflicting information sources or difficulty appraising or understanding all the information.
Our study adds to the existing body of knowledge by highlighting the significant positive influence of sadness on health information avoidance. This finding is comparable with the findings of previous studies (Link, 2021; Song et al., 2021), suggesting a potential emotional dimension to information avoidance behavior. Our findings also support the findings of previous studies that information source exposure and risk perception have a positive influence on health information anxiety (Soroya and Faiola, 2023; Xu and Peng, 2015; Zhao and Cai, 2009). These findings indicate a potential link between exposure to health information sources and a tendency to encounter information about health risks that may shape health information avoidance behavior. Our findings also support the findings of previous studies that health information anxiety positively influences health information avoidance (Song et al., 2021; Soroya et al., 2021). These findings validate the relationship between anxiety and avoidance behavior in the context of health information. Our findings indicate that individuals who experience anxiety while seeking health-related information, or anxiety while understanding, appraising, or interpreting these sources, are likely to avoid seeking or engaging with health-related information. On the other hand, our findings negate the studies (Song et al., 2021; Thamrin et al., 2023; Yahya and Sukmayadi, 2020) that cognitive dissonance influences health information avoidance. We suggest that further studies are required to determine the influence of cognitive dissonance on health information avoidance behaviors.
Furthermore, health information avoidance behavior leads toward healthcare negligence and a decrease in preventive actions. The findings of previous studies reported that individuals who tend to avoid health information are also more likely to delay or avoid seeking healthcare services (Li et al., 2021; Yu et al., 2021). This means that decreasing the frequency of information avoidance through effective health risk communication could be an effective way to control health risks.
Implications of the study
The findings of this study have significant implications for various stakeholders involved in public health communication, including government organizations, health departments, policymakers, libraries, and the general public. Individuals overwhelmed by complex or limited health information may be less likely to adopt preventive health measures, potentially hindering their ability to make informed decisions and impacting their overall health. The findings highlight the need for government agencies to prioritize timely initiatives in risk communication and health information management for public health. Moreover, in the absence of reliable health information, misinformation and disinformation can flourish. It can prevent faculty from seeking health-related information or potentially encountering information sources that spread ineffective treatments or guidance about the disease.
Our study’s findings can inform the development of targeted inventions to reduce information overload and address cognitive dissonance, ultimately decreasing sadness and increasing health information-seeking behaviors among faculty. These interventions include: developing and implementing tools to filter irrelevant or low-quality information, and providing faculty with a curated stream of relevant health information. Libraries can organize information literacy sessions on information searching, evaluating, and critical thinking to help faculty navigate information overload effectively. Libraries can create dedicated knowledge management systems for storing and organizing health-related information, reducing the need for extensive searches. Moreover, understanding the relationship between risk perception and sadness can help libraries develop effective communication strategies through educational campaigns or information literacy programs to address common misconceptions about information overload and health information-seeking concerns. Libraries can provide an opportunity for open dialog and feedback mechanisms, through which faculty can share their perspectives and concerns about health information sources and seeking behaviors, fostering a sense of transparency and trust. Moreover, libraries can ensure that health information is readily available through easily accessible and user-friendly platforms. The findings can be used to design workplace health education programs that focus on managing information overload, reducing stress, and promoting health information-seeking behaviors. The study can inform the development of policies and guidelines to optimize the dissemination of health information, considering the potential impact on faculty health.
Study contribution
The study makes a significant contribution to the field of information management, library and information science, health communication, health information behavior, and information science. It contributes to the existing body of knowledge by expanding our understanding of information avoidance behaviors of faculty by highlighting the relationship between information overload, cognitive dissonance, risk perception, and health information avoidance. The study highlights the role of sadness as a mediator between risk perception and health information avoidance, providing valuable insights for future research and interventions. The proposed model can serve as a foundation for further research on health information avoidance behavior in academic settings. The findings can inform the development of evidence-based strategies for mitigating health information avoidance and promoting health information seeking and utilization among faculty members. Our study contributes to the advancement of the S-O-R (Stimulus-Organism-Response) framework by emphasizing the influence of external environmental factors. Traditionally, the S-O-R model primarily focuses on the internal response (organism) of an individual triggered by a stimulus. This study broadens the framework by demonstrating that external factors, such as exposure to various health information sources, can significantly shape an individual’s internal state. These internal changes, including anxiety or information overload, can then directly influence avoidance behavior related to health information. Ultimately, this avoidance behavior can impact individuals’ health decisions
The phenomenon of information overload is not confined to a specific region or culture. The study’s findings can contribute to the development of strategies to manage information overload in various academic settings. Moreover, our study addressed several health challenges, such as information overload, information sources exposure, health information anxiety, misinformation and health disparities, which are global concerns. Our findings can serve as a foundation for comparative studies in different cultural and educational contexts. This can help identify both universal and culturally specific predictors influencing health information avoidance behavior and health outcomes.
Limitations of the study
The study has several limitations. We used a survey approach to collect data that depended on respondents’ self-understanding of the questions. There is always the risk that respondents’ self-reports of the question’s statement may differ from the actual circumstances. To address potential questionnaire limitations, a questionnaire was assessed by three experts in information management, public health, and health communication. Cronbach’s alpha was used to assess reliability, with a score of 0.862 for the 41 statements across the seven constructs, indicating good overall reliability. Construct reliability was ensured through composite and maximal reliability estimates. Factors like geographical location, demographics, infrastructure, and health literacy levels can influence how information is perceived and processed. Therefore, caution should be exercised when applying these results to other groups or organizations. Another limitation of the study was its focus on specific factors such as anxiety, sadness, cognitive dissonance, information overload, and information sources exposure, based on theoretical and empirical grounds. Future studies could incorporate trust and privacy concerns to gain a more comprehensive understanding of health information avoidance.
Conclusion
The study validates the stimulus organism response (S-O-R) framework among university faculty members in Azad Jammu and Kashmir. It concludes that risk perception with health information, feelings of sadness, and information overload are significant predictors of health information avoidance behavior, while health information anxiety and information source exposure are non-significant predictors.
The study suggests that university librarians can play an effective role in addressing factors that contribute to health information avoidance. They can implement tailored interventions such as information literacy sessions, information filtering tools, communication strategies, and workplace health education programs, to address these issues and promote health information seeking among faculty members. The study suggests a need for further research to measure the long-term impact of information overload and cognitive dissonance on faculty health and to conduct cross-cultural studies to identify similarities and differences in information avoidance behaviors.
Footnotes
Appendix
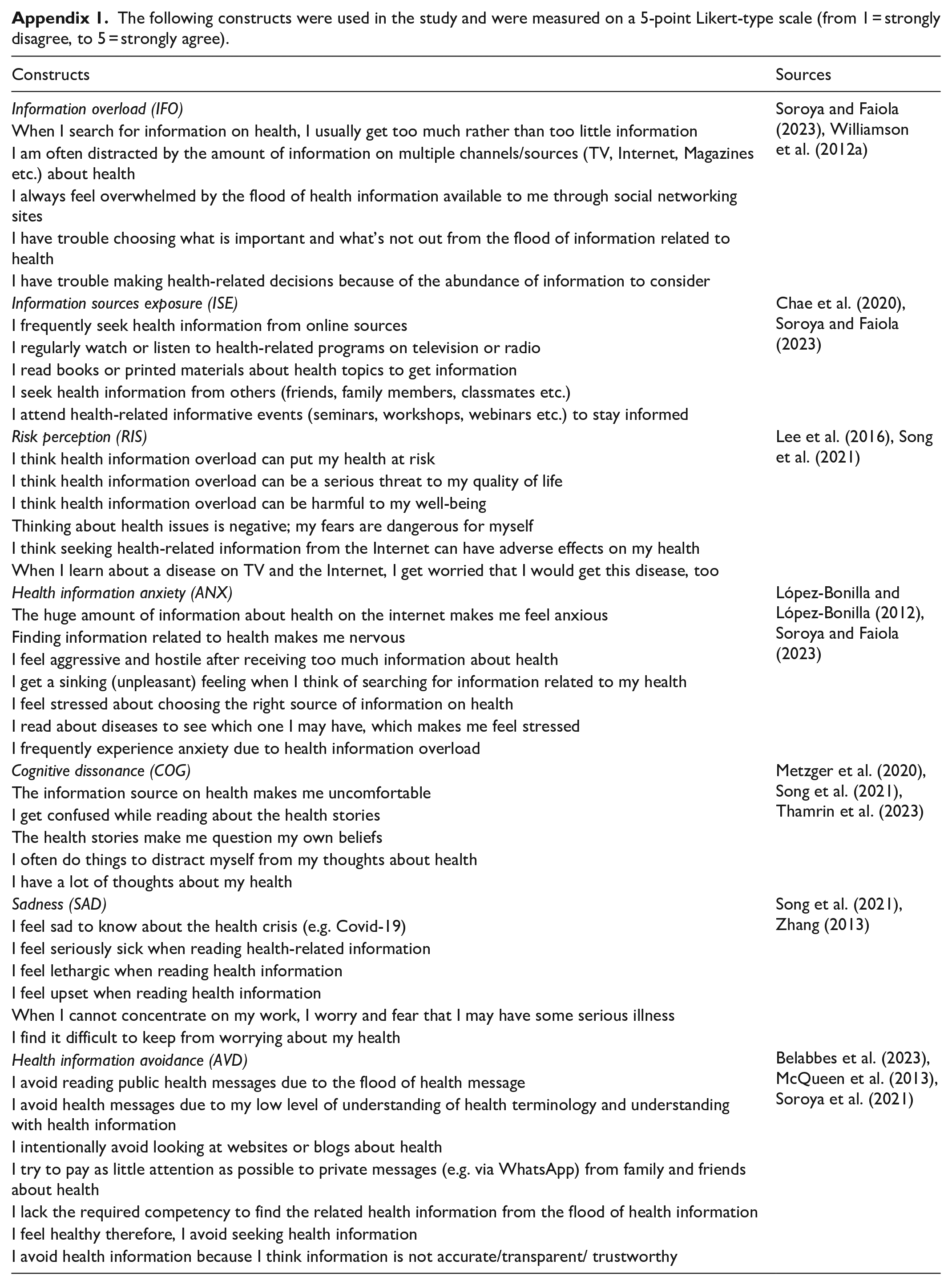
The following constructs were used in the study and were measured on a 5-point Likert-type scale (from 1 = strongly disagree, to 5 = strongly agree).
| Constructs | Sources |
|---|---|
| Information overload (IFO) | Soroya and Faiola (2023), Williamson et al. (2012a) |
| When I search for information on health, I usually get too much rather than too little information | |
| I am often distracted by the amount of information on multiple channels/sources (TV, Internet, Magazines etc.) about health | |
| I always feel overwhelmed by the flood of health information available to me through social networking sites | |
| I have trouble choosing what is important and what’s not out from the flood of information related to health | |
| I have trouble making health-related decisions because of the abundance of information to consider | |
| Information sources exposure (ISE) | Chae et al. (2020), Soroya and Faiola (2023) |
| I frequently seek health information from online sources | |
| I regularly watch or listen to health-related programs on television or radio | |
| I read books or printed materials about health topics to get information | |
| I seek health information from others (friends, family members, classmates etc.) | |
| I attend health-related informative events (seminars, workshops, webinars etc.) to stay informed | |
| Risk perception (RIS) | Lee et al. (2016), Song et al. (2021) |
| I think health information overload can put my health at risk | |
| I think health information overload can be a serious threat to my quality of life | |
| I think health information overload can be harmful to my well-being | |
| Thinking about health issues is negative; my fears are dangerous for myself | |
| I think seeking health-related information from the Internet can have adverse effects on my health | |
| When I learn about a disease on TV and the Internet, I get worried that I would get this disease, too | |
| Health information anxiety (ANX) | López-Bonilla and López-Bonilla (2012), Soroya and Faiola (2023) |
| The huge amount of information about health on the internet makes me feel anxious | |
| Finding information related to health makes me nervous | |
| I feel aggressive and hostile after receiving too much information about health | |
| I get a sinking (unpleasant) feeling when I think of searching for information related to my health | |
| I feel stressed about choosing the right source of information on health | |
| I read about diseases to see which one I may have, which makes me feel stressed | |
| I frequently experience anxiety due to health information overload | |
| Cognitive dissonance (COG) | Metzger et al. (2020), Song et al. (2021), Thamrin et al. (2023) |
| The information source on health makes me uncomfortable | |
| I get confused while reading about the health stories | |
| The health stories make me question my own beliefs | |
| I often do things to distract myself from my thoughts about health | |
| I have a lot of thoughts about my health | |
| Sadness (SAD) | Song et al. (2021), Zhang (2013) |
| I feel sad to know about the health crisis (e.g. Covid-19) | |
| I feel seriously sick when reading health-related information | |
| I feel lethargic when reading health information | |
| I feel upset when reading health information | |
| When I cannot concentrate on my work, I worry and fear that I may have some serious illness | |
| I find it difficult to keep from worrying about my health | |
| Health information avoidance (AVD) | Belabbes et al. (2023), McQueen et al. (2013), Soroya et al. (2021) |
| I avoid reading public health messages due to the flood of health message | |
| I avoid health messages due to my low level of understanding of health terminology and understanding with health information | |
| I intentionally avoid looking at websites or blogs about health | |
| I try to pay as little attention as possible to private messages (e.g. via WhatsApp) from family and friends about health | |
| I lack the required competency to find the related health information from the flood of health information | |
| I feel healthy therefore, I avoid seeking health information | |
| I avoid health information because I think information is not accurate/transparent/ trustworthy |
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional Review Board Statement
The study was approved by the Departmental Research Committee (DRC), Department of Information Management, The Islamia University of Bahawalpur, Pakistan under approval code 15-2023/DoIM.
No personally identifiable information was collected from questionnaire respondents. Participation consents were obtained in verbal or written from each individual participant in the study.
Informed consent statement
Informed consent was obtained from all questionnaire respondents.
Data availability statement
The core data supporting the findings of this study are available within the article; further details can be obtained from the authors upon reasonable request.