
Abstract
Squamous cell carcinoma is a rare consequence of lupus erythematosus and it is generally associated with skin lesions rather than with oral mucosa. This paper reports a patient diagnosed with systemic lupus erythematosus who developed a squamous cell carcinoma on the palate as an outcome of a persistent ulcer, a frequent lesion in patients with this disease and, in fact, clinical criterion for its diagnosis. A 38-year-old female patient diagnosed with systemic lupus erythematosus 12 years previously, who attended the dental school for routine dental control. The patient was being treated with prednisone 10 mg per day and cyclophosphamide 750 mg per month until 10 months prior to her diagnostic biopsy. She had, however, been previously treated with chloroquine. Oral lesions started 6 months before consultation as symptomatic multiple ulcers on the palate. After topical treatment with steroids for 1 month, the lesions regressed except for the central lesion, from which an incisional biopsy was taken and a well differentiated squamous cell carcinoma was diagnosed. The oncological phase consisted of partial palatectomy. To date, 3 years after surgery, the patient is free from malignant lesions. Lupus erythematosus is considered a potentially malignant disorder, although the cause for neoplasic transformation in these patients is still not clear, but cyclophosphamide consumption may be implicated; the case emphasizes the importance of periodical oral evaluation of such patients. Repeated biopsies should be performed if there is failure to respond to conventional therapy.
Introduction
Lupus erythematosus (LE) is a chronic autoimmune disease with cyclic periods of exacerbation in which the body produces autoantibodies directed to nuclear products that act as antigens. Mucosal and skin manifestations are denoted as cutaneous LE (CLE) and at the other extreme of the spectrum, systemic LE (SLE), which affects a variety of organs and tissues and frequently also courses with cutaneous lesions. 1
LE affects mainly women of reproductive age, especially from the end of adolescence until approximately the age of 40, in a female:male proportion of 9:1. 1–5 The frequency with which the mouth is affected varies according to whether it is SLE (50%) or CLE (20–25%). 5 Manifestations in oral mucosa are variable, but can be grouped as: erosive lesions, desquamative plaques, erythematous maculae or plaques, white plaques over pigmented surfaces, and ulcerative lesions including what has been called discoid lesions (ulcers or erosions surrounded by white plaque or striations). 1,4
LE has been associated with an augmented risk of malignant neoplasias. Malignant transformation might be produced by the disease per se, or possibly because of the immunosuppressive treatment. 6,7 There are reports associating SLE with cancer, among which skin carcinomas and lymphomas are the most common. 6,8,9 Few cases of oral carcinomas associated with LE have been reported and these were mainly on the lip. 5,9,10
This report describes the case of a patient with SLE who developed several oral lesions on the palate, one of which persisted and resulted in an oral squamous cell carcinoma (OSCC).
Case report
A 38-year-old female lawyer, single, Latin-American, native of Venezuela, was referred to the Oral Medicine Service of the School of Dentistry regarding symptomatic lesions on the palate. She referred an approximate 6 month evolution period with very painful oral lesions. She had, a month before consulting the Oral Medicine Service, applied a homemade aloe vera preparation, resulting in a minor remission.
Personal background
She referred tobacco consumption from the age of 21 (eight cigarettes per day), although with a low nicotine dependence (2 on the Fagerström scale). In 1997 she was diagnosed with SLE. Her first symptoms were arthralgia and difficulty in holding objects. Subsequently, she suffered a mitral valve prolapse, panic crisis, toxic retinopathy, lupic mesenteric vasculitis, non-erosive polyarthritis, alopecia, Raynaud’s phenomenon, anaemia, leucopenia, thrombocytopenia and amaurosis.
The patient’s therapeutic regime at the time of consultation consisted of cyclophosphamide 750 mg/month, chloroquine 250 mg b.i.d., methylprednisolone 8 mg o.d., alendronate with calcium supplement 70 mg/week, enalapril 5 mg o.d., omeprazole 20 mg o.d., ranitidine 150 mg b.i.d., alprazolam 0.25 mg b.i.d., ondasentron 8 mg/month, folic acid 10 mg o.d., simvastatin 10 mg o.d. and acetylsalicylic acid 100 mg o.d. She had received six-monthly boluses of cyclophosphamide, for a total cumulative dose of 4.5 g until 10 months previous to her oral biopsy. Family records were non-contributory to the case.
Clinical examination
Extraorally she showed a discrete cushingoid facie. Cervico-facial and mammarian ganglia were non-palpable and skin lesions were not observed at the time. Intraorally several lesions were observed on the hard palate. The central portion of the hard palate showed an irregular shaped ulcerative lesion with an erythematose macular border of approximately 25 mm in the broadest portion (Figure 1). On the right lateral side, an approximately 4 mm erythematose macula with white portions on its surface was detected. On the left posterior portion of the hard palate, an ulcerative lesion was present covered with a white desquamative pseudomembrane, approximately 15 mm in diameter, irregular in shape and defined elevated erythematose borders, with mild whitish striations perpendicular to the lesion, resembling ‘sun rays’ (Figure 2). Radiographic examination showed no related lesions.
Erosive and ulcerative lesions in palate. Ulcerative lesion.

Topical steroid therapy was started (dexametasone rinses four times per day) together with general restorative dental treatment. After a month the patient was re-evaluated by the Oral Medicine Service evidencing remission of ulcerative lesions, with the exception of the central palatal lesion with persistence of painful symptomatology (Figure 3). Blood tests and incisional biopsy were indicated. The histopathological study revealed an epithelial malignant tumour conformed by keratinocytes with altered nucleus-cytoplasm proportion, hyperchromatism, pyknosis, atypical mitosis, and cellular and nuclear pleomorphism. Keratin pearls were present immersed in epithelial isles which invaded the subjacent tissue in a cohesive pattern. A definitive diagnosis of a well differentiated OSCC was concluded. The time between the diagnosis of SLE and the diagnosis of oral cancer was 10 years.
Persistent lesions after 1 month.
The patient was referred to an oncological centre where she was classified as T1N0M0. A partial palatectomy was performed. After three years, the patient has evolved satisfactorily, maintaining periodic controls both in the oncologic hospital and in the Oral Medicine Service. There have been no signs of recurrence or metastasis to date.
Discussion
Oral ulcers can be present in a 40% of LE, as in this case, as well as erythematous plaques or maculae. 1 The behaviour of the lesions was clearly different, for whereas the discoid forms followed a curative course, the central and satellite ones persisted and aggravated, which leads to the assumption that in the same anatomical site, different patterns of oral LE can coexist and behave in a different manner.
The increased risk of malignancy in these patients may be due to abnormalities of the immunological system, which predispose to cancerous mutations. These immunological abnormalities also fail in the vigilance of such aberrations when they occur, aided by the use of immunosuppressive drugs. 8,11
The index of haematological cancers seems to be increased in SLE patients, but there is also the possibility that ‘solid’ neoplasias of other tissues could be augmented. 6,11 Of note is that, whereas the first seems to be attributed to chronic stimuli of the lymphocytes, the latter appears to be associated with conductal factors, such as cigarette smoking or sun exposure. 12 There is a burden of genetic, ethnic and environmental factors that exerts its influence, both on the development of LE and on cancer. 8
Cases of oral and lip cancers associated to lupus reported in the literature
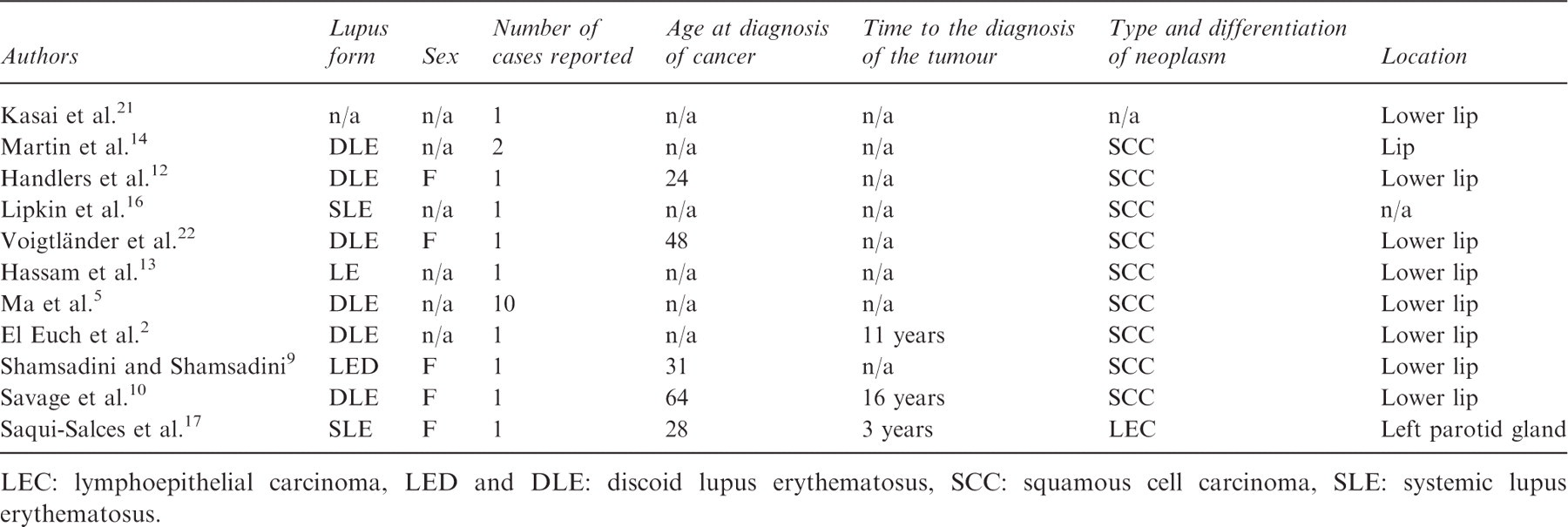
LEC: lymphoepithelial carcinoma, LED and DLE: discoid lupus erythematosus, SCC: squamous cell carcinoma, SLE: systemic lupus erythematosus.
It has been stated that the use of immunosuppressant drugs could be implicated in the occurrence of cancer in these patients. 16 This has not yet, however, been established. 6,7 Recently, it has been proved that cyclophosphamide may enhance tumor growth and metastasis, including increasing vascular growth factor expression. 18,19 The patient described in this paper received cyclophosphamide previous to her clinical examination and biopsy.
Interestingly, it has been proposed that the use of antimalarials such as chloroquine would seem to have a protective effect against malignant neoplasias. The mechanism of this possible ‘protection’ consists in the prevention of mutations in cells with a high mitotic rate, inhibition of the telomerase (implicated in the indefinite replication of tumour cells), increase of synthesis of p53 and improvement of cell repair of DNA; unfortunately smoking greatly reduces the efficiency of these drugs. 20
Oral ulcerative lesions are common in LE, but, as in this case, the importance of considering malignant transformation of the aforementioned is a real and important possibility. The health team should endeavour to focus not only on curative treatment but also on preventative treatment, in an attempt to reduce risk behaviour in these patients.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Acknowledgments
The authors thank the Specialty of Oral Surgery of the Faculty of Dentistry of Universidad Central de Venezuela (Central University of Venezuela) and the Luís Razzetti Oncological Hospital in Caracas.