
Abstract
The objectives of this study were to measure the prevalence of adherence to drug treatment and analyze associations with characteristics pertaining to the treatment, disease, health professionals and services, and socio-demographic issues in patients with systemic lupus erythematosus (SLE) in the city of Rio de Janeiro, Brazil. A sample of 246 women with SLE was analyzed. The data were collected through individual interviews and a review of patient charts. Adherence was estimated according to the Morisk criteria, and the associated factors were analyzed by hierarchical modeling. The percentage of patients classified as adherent to treatment was 31.7%. The reasons cited for non-adherence were: carelessness with drug administration times (52.43%), forgetfulness (38.21%), adverse drug reaction (13.8%), and interruption of treatment due to improvement in symptoms (7.72%). Factors associated with adherence were: behavior towards the presence of adverse drug reaction, hematological alterations, presence of mucocutaneous manifestations, legibility of the medical prescription, schooling, and family support. The study concludes that adherence to drug treatment in SLE is a complex and multifactorial phenomenon, and the results corroborate findings from studies conducted in developed countries. The hierarchical modeling proved to be a good alternative for evaluating adherence, since it allowed visualizing the various stages in the analysis.
Introduction
One important problem that frequently hinders obtaining the intended results from drug treatment (DT) is that of adherence to the proposed treatment. The issue’s relevance is beyond question, since inadequate treatment adherence can lead to therapeutic failure, for example delaying the healing process, hindering the control of a chronic disease, or even leading to death in extreme cases. 1,2
Among users of medicines, those with chronic diseases are potential candidates for inadequate adherence to the therapeutic regimen. The resulting problems include clinical and social complications, decreased quality of life, and increased costs for health systems. 1,3–5
Defining the expression ‘treatment adherence’ (TA) is a difficult task, since there is no consensus among the authors. The terms ‘compliance’ and ‘adherence’ are often used interchangeably. According to some authors, 3,6,7 the two terms do not mean the same thing. ‘Compliance’ assumes a passive role by patients towards their treatment, accepting the prescribed recommendations, while ‘adherence’ is their free choice to adopt or reject such recommendations.
The term ‘adherence’ is more widely accepted, since it expresses understanding and cooperation. Thus, a partnership is developed in which the patient not only obeys (i.e. complies with) the physician’s recommendations, but understands, agrees to, and follows (adheres to) the established prescription. This means that a ‘therapeutic alliance’ must exist between patients and their physicians, acknowledging the responsibilities of all those involved either directly (patient/health professional) or indirectly (family/friends) in the treatment.
Chambers et al. 8 highlight the importance of studies for the evaluation of adherence to drug treatment in patients with systemic lupus erythematosus (SLE). Repeated relapses and treatment extensions lead to otherwise avoidable suffering and high treatment costs.
Few studies have evaluated treatment adherence in rheumatic diseases, and in the specific case of SLE the studies are even scarcer and are mainly conducted in developed countries, where the cultural, social, and economic reality often differs from that of developing countries like Brazil.
The objectives of this study were to measure the prevalence of treatment adherence in a cohort of patients with SLE in Rio de Janeiro, Brazil, evaluate factors previously suggested as associated with adherence, and propose the use of hierarchical modeling as an analytical approach.
Material and methods
Study setting and population
The study population was selected from the Lupus Outpatient Clinic at the Pedro Ernesto University Hospital, Rio de Janeiro State University (UERJ). The SLE outpatient clinic is a reference unit for lupus care in Rio de Janeiro. All patients were treated by rheumatologists and nephrologists.
A simple random sample was calculated according to the following parameters: estimated 50% prevalence of adherence, 95% confidence interval, and 5% margin of error (α error). Only female patients were included, because male patients only constituted some 5% of the cohort. If the same homogeneity and proportion were maintained in the sample, it would have been impossible to establish the relationship between gender and adherence, due to the small number of participants.
The inclusion criteria were: patients with confirmed diagnosis of SLE according to the classification criteria of the American College of Rheumatology (ACR); 9 having at least one medical appointment scheduled during the study period; in use of at least one specific drug for treatment of SLE; age equal or greater than 18 years; and understanding and agreement to the study’s objectives and methodology. The study excluded patients that required a caregiver to administer their medicines or that presented some cognitive disorder that prevented them from understanding the study questionnaire.
Data collection
Data were obtained through an interview and review of patient charts, using two instruments: a structured, coded questionnaire, and a sheet for collecting data from the patient chart, focused on information pertaining to clinical manifestations, aspects of the disease, and medicines prescribed in the last consultation. The inflammatory activity and severity index was not evaluated for the disease, due to the difficulty in obtaining all the necessary information when reviewing the patient charts.
When the research instruments were being constructed, there were no previously validated Portuguese-language questionnaires for evaluating treatment adherence in SLE. Our instruments were thus developed by evaluating articles, original studies, and systematic reviews of the medical literature, which contained questionnaires for evaluating treatment adherence in chronic diseases. The MEDLINE (National Library of Medicine), LILACS (Latin American and Caribbean Center on Health Sciences Literature), and SCIELO (Scientific Electronic Library Online) databases were used. The study questionnaire aimed to collect data on the five dimensions proposed by the World Health Organization (WHO) in order to better understand the problem of adherence, namely: factors related to social and economic issues, health professionals and services, characteristics of the treatment regimen and the disease, and those related to the patients. 1
Face-to-face interviews using a validated structured questionnaire were conducted by one of the authors, a pharmacist with a Master’s degree in epidemiology.
The evaluation and classification of the patients’ answers to the open questions in the questionnaire were done by two independent reviewers (a pharmacist and a physician). When there was disagreement between the reviewers, a third reviewer was consulted to decide on the question.
The therapeutic regimen that served as the basis for estimating adherence was the one that the patient reported using at the time of the interview, and the specific medicines for treatment of SLE and co-morbidities were included. The drugs used and prescribed were classified according to the Anatomical Therapeutic Chemical Classification System (ATC).
Evaluation of clinical manifestations in patients during the evolution of SLE only included the ACR classification criteria. Immune alterations and antinuclear antibodies were excluded. Although they are important for the diagnosis of SLE, positive results for these tests would not produce symptoms that could be perceived by the patient or influence their adherence.
Measures of adherence to drug treatment
Adherence was evaluated using the Morisk Medication Adherence Scale (MMAS), 10 modified by Delgado and Lima, 11 and analyzed as a dichotomous variable (adherent versus non-adherent). In this study, patients were considered adherent when they answered all the questions in the negative, that is, when they used their medicines exactly as prescribed.
Statistical analysis
Statistical analysis of the data, modeling, and interpretation of the results followed the procedures suggested by Fuchs et al. (1996) 12 and Victora et al. (1997) 13 for hierarchical analysis.
The first step in this analysis is to establish a conceptual theoretical framework that explains the relations between the risk factors, followed by a proposed hierarchical order for the independent variables.
12
A theoretical framework was built with the adherence-related variables, based on the five dimensions proposed by the WHO, dividing them into three hierarchical levels: distal, intermediate, and proximal variables (Figure 1). Since no studies were found on the joint association of these dimensions, the conceptual theoretical framework prioritized the treatment regimen and the disease over the patient’s economic, social, and demographic characteristics. That is, the disease establishes the treatment options independently of socio-demographic characteristics, and the health professional and institution act by mediating the patient’s relationship to the treatment.
Hierarchical theoretical model for adherence to drug treatment in SLE.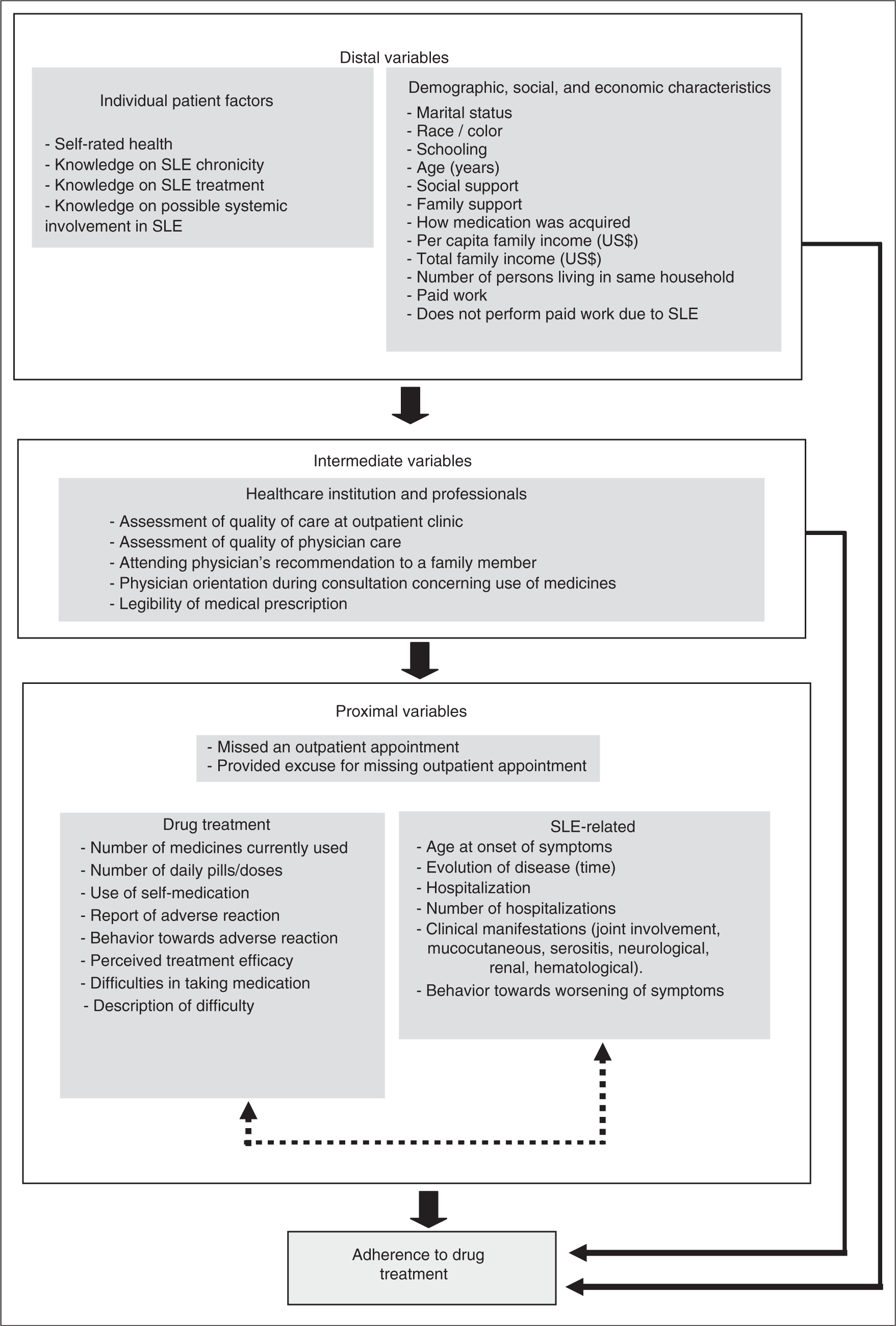
Failure to appear for an outpatient appointment is used as an indirect measure of TA, since it is directly related to adherence. This variable was included in the proximal level of the hierarchical analysis.
The odds ratio (OR) and its respective confidence interval (CI) were used to measure the association between the response variable (adherence to drug treatment) and the variables analyzed in each hierarchical block. Multivariate analysis was performed using multiple logistic regression and the model’s adjustment as a whole using the ‘deviance’ statistic, since the explanatory variables were all categorical and the final models in each stage displayed a relatively small number of variables.
To avoid exclusion of potentially important variables that might be associated with adherence, bivariate analysis was used with 20% significance level in the maximum likelihood analysis.
Hierarchical modeling methods have been suggested as an alternative for dealing with the limitations of conventional models applied to epidemiological studies with a large number of variables. 12 When studying multiple exposures, the hierarchical model indicates the order in which the variables should enter, beginning with the most distal levels. 12 Thus, the social, demographic, and economic characteristics of the theoretical framework were the first to be included and acted to adjust for the variables from the following blocks. Those presenting statistical significance in the analysis (p < 0.05) were kept in the model and entered the adjustment in the next (intermediate) level.
In this analytical proposal, the variables selected in the previous block are kept in the model, even when their statistical significance is not maintained with the inclusion of the subsequent hierarchical levels. This procedure was used through the inclusion of all the blocks.
The variables from the previous stages acted to control for possible confounding factors. The model’s goodness-of-fit was done by residue analysis.
Data were processed with the R statistical package, version 2.7.1.
Ethical considerations
All stages of the study complied with the basic ethical principles guiding research with human beings. Study subjects signed a free and informed consent form, and were ensured of the absolute anonymity and secrecy of the information provided by them. Interviews were held in an individual examining room in the SLE Outpatient Clinic. The study was approved by the Institutional Review Board of the National School of Public Health, Oswaldo Cruz Foundation (ENSP/FIOCRUZ).
Results
Demographics of survey populations
A total of 246 patients were interviewed, all female, mean age 41.59 ± 12.35 years, predominantly Afro-descendents (54.88%), and with complete secondary education as the most common level of schooling (37.81%). Mean total family income was US$836.67 ± 699.16 and mean per capita family income was US$302.02 ± 321.04. An average of three persons lived in the same household.
Measures of adherence to drug treatment
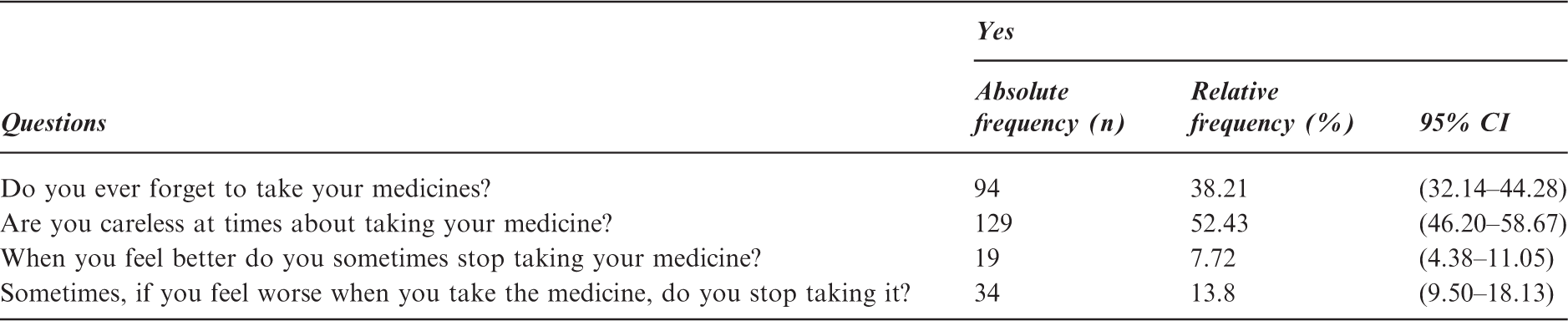
Based on the data analysis and using the MMAS, 12 prevalence of adherence was 31.7% in the sample of patients (n = 78).
Frequency of positive answers to questions in the Morisk Medication Adherence Scale. Rio de Janeiro, March–August 2008 (n = 246)
Statistical analysis
Selection of variables comprising the hierarchical multiple analysis for treatment adherence in SLE. Rio de Janeiro, March–August 2008 (n = 246)
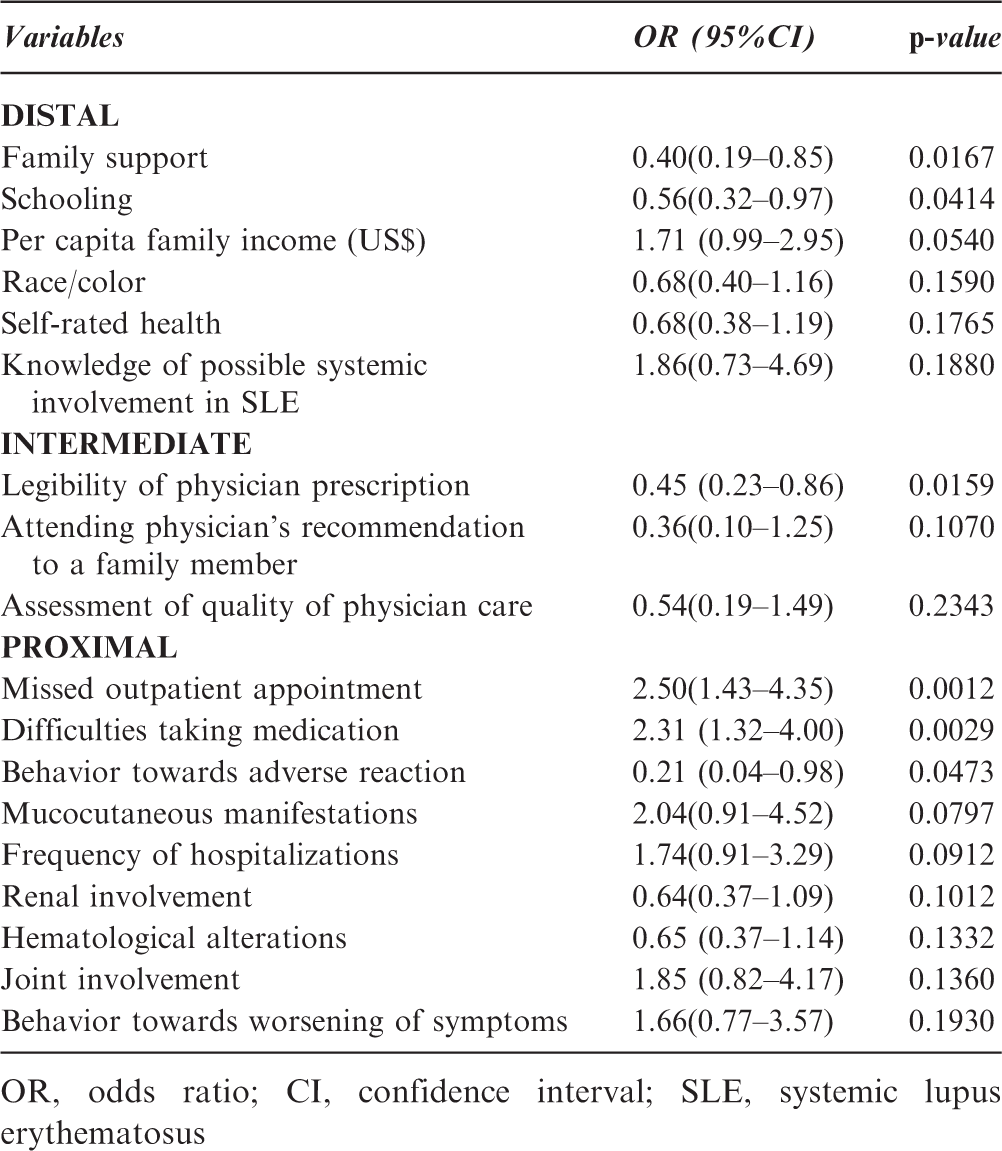
OR, odds ratio; CI, confidence interval; SLE, systemic lupus erythematosus
Despite not showing statistical significance in the proposed range, the variable ‘patient’s assessment of quality of physician care’ was also selected for the multiple regression analysis, because among the patients that considered the outpatient medical consultation fair, poor, or terrible, nearly 80% (79.17%) were classified as non-adherent to the drug treatment.
The explanatory variables were entered in stepwise fashion, in keeping with the hierarchical level in determination of the outcome, as proposed in the theoretical model.
Final hierarchical model for treatment adherence in systemic lupus erythematosus, with three hierarchical levels. Rio de Janeiro, March–August 2008 (n = 246)
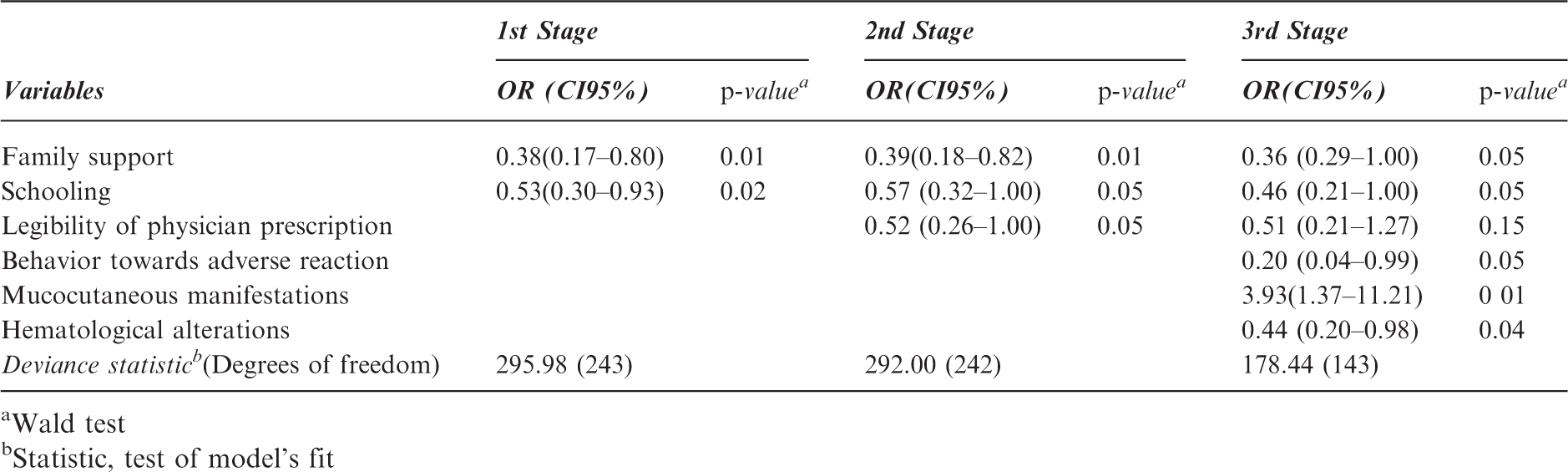
Wald test
Statistic, test of model's fit
Clinical manifestations
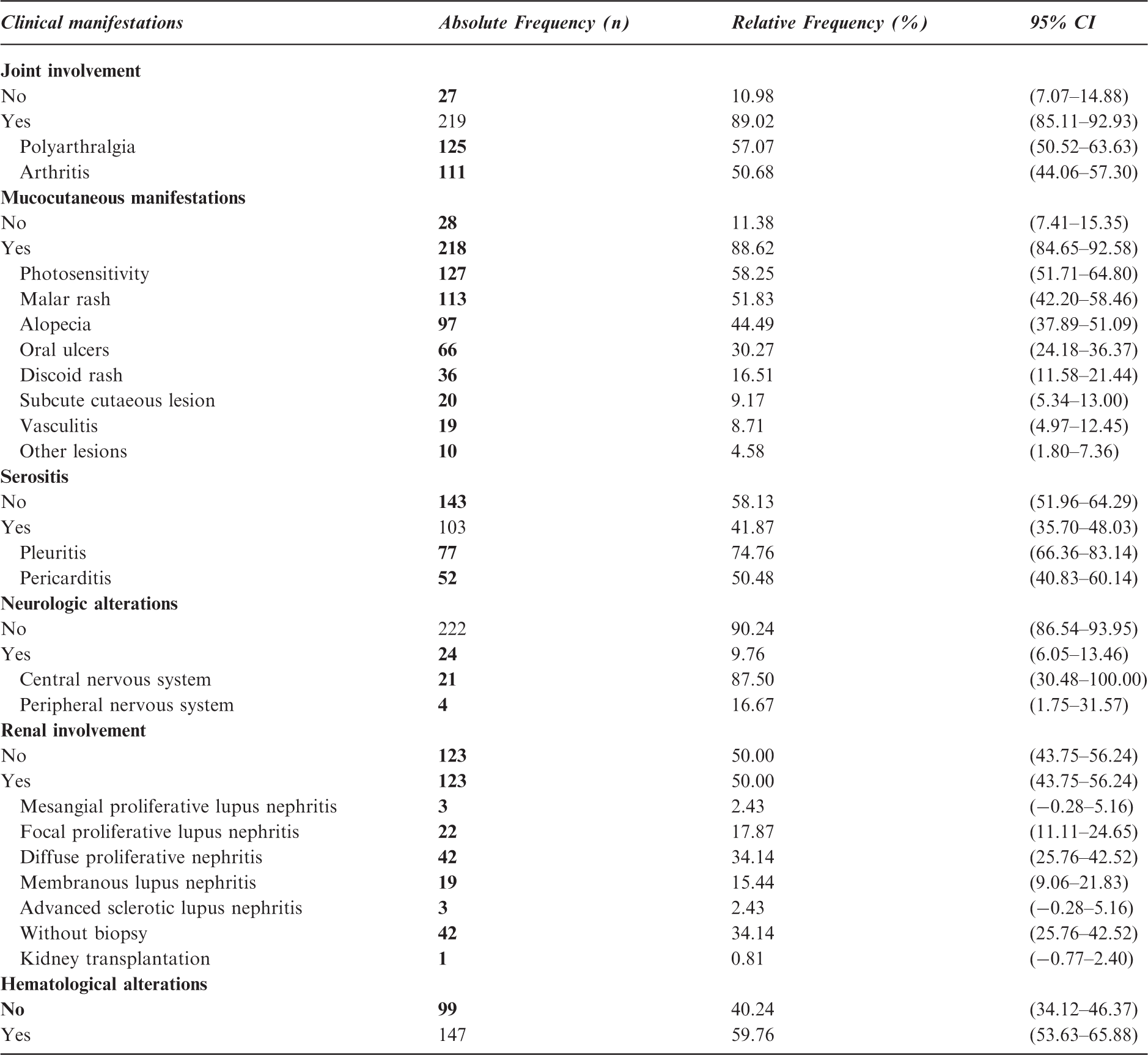
Age at onset of clinical manifestations had an average of 28 ± 11 years. The evolution of disease (time between onset of the first ACR criterion for SLE and the interview date) was divided into periods of five years to facilitate data analysis. We found that half of the patients (n = 123, 95% CI = 43.75–56.24) presented an evolution of up to 10 years.
The evolution of disease was included in the first stage of modeling (bivariate analysis). As it was not statistically significant either as continuous variable (p = 0.2704) or as dichotomous (p = 0.4119), it was not included in the next steps.
Distribution of patients according to observed clinical manifestations. Rio de Janeiro, March–August 2008 (n = 246)
Prescribed drugs
The mean number of currently used medicines was 5.09 ± 2.48, and mean number of prescribed medicines was 4.9 ± 2.34. There was no statistically significant difference between the median number of medicines used and prescribed (Wilcoxon signed rank test, W = 31486.5, p > 0.05). More than half of the patients interviewed (55.29%) were taking five or more medicines. The maximum number of daily pills or doses taken per patient was 22, and the mean number was 7.32 ± 4.48 doses. It was not possible to assess the prescribed number of pills or doses, since this information was not available on the patient chart.
Of the total of 95 medicines reported by patients, the most frequently used was prednisone (taken by 79.27% of the patients).
The most widely-used drug classes for specific treatment of SLE were the glucocorticoids (80.08%), followed by antimalarials (69.51%), and immunosuppressants (47.15%). For treatment of co-morbidities of SLE, mineral supplements (54.06%) were the most widely used, followed by drugs acting on the renin–angiotensin system (38.22%) and antithrombotics and/or platelet aggregation inhibitors (29.27%).
Slightly more than half of the sample (51.21%) reported that in the seven days prior to the interview they had presented some type of difficulty in taking their medicines. The main difficulties reported were: lack of money to purchase the medicine (52.38%), forgetting (27.78%), and failure to receive the medicine free of cost from the Unified National Health System, or SUS (6.35%).
The majority of the interviewees (60.97%) reported some unpleasant reaction to taking the medicines; of these, 87% stated that they knew which medicine had caused the adverse drug reaction (ADR). Glucocorticoids, antimalarials, and immunosuppressants together accounted for 73.33% of the complaints, with prednisone (29.00%), chloroquine diphosphate (25.19%), and mycophenolate mofetil (8.40%) as the most widely cited. When they felt some ADR, 69.33% did not suspend the treatment, 12.67% took some other medication to improve the symptoms, and 18.00% reduced the number of doses or stopped taking the drug they felt was responsible for the adverse reaction.
Discussion
The number of participants included in the study (n = 246) was within the calculated range and comprised a significant sample of patients. Mean age (41.59 ± 12.35 years) was similar to that found in other studies in Brazil, 14,15 confirming a higher incidence of SLE in this age bracket.
The proportion of 31.7% of patients adhering to their drug treatment using the MMAS, found in this study, was considered low. The low prevalence of adherence may have been due to the rigorous criterion that was adopted, that is, taking 100% of medicines as prescribed by the medical team.
The results for the answers to the MMAS questions are consistent with those of other studies in which similar questions were asked. Inattention to drug administration times and forgetting to take medication were cited by patients classified as non-adherent in the current study as the main reasons for not taking their medicines as prescribed. Among users of prednisone and hydroxychloroquine, present in the study by Koneru et al., 16 38% and 32%, respectively, identified forgetting as the reason for not taking their medicines. Two-thirds of the patients evaluated by Garcia-Gonzales et al. 17 reported forgetting to take their medicines. As for ADRs, 40% of subjects interviewed by Garcia-Gonzales et al. 17 reported interrupting their medication due to adverse reactions, a proportion that was higher than we observed (13.8%). Suspension of medication when the patient was asymptomatic showed the lowest percentage, thus denoting our patients’ perception of the importance of continuous use. In the sample studied by Chambers et al., 18 some patients reported only taking their medicines when the disease was in activity.
Evaluation of the demographic data showed a predominance of Afro-descendent patients. Importantly, the high miscegenation rate in Brazil may have hindered a more objective classification of this characteristic.
White race or color acted as a protective factor for adherence, but in addition to genetic aspects, the interpretation of this result in Brazil should take schooling and income into account. Unequal access to schools and other forms of social support, which differs according to race or skin color, may be explained mainly by the history of immigration of blacks to Brazil (imported as unpaid labor). There is a long-standing debate on the relationship between race/color and treatment adherence in SLE, with no consensus among the authors on this association. 16,17,19–21
Schooling was associated with treatment adherence in the current study. This finding corroborates other studies, like Koneru et al. 16 and Garcia-Gonzales et al., 17 who also identified low schooling as a significant factor for non-adherence in SLE.
The presence of some type of difficulty that prevented administration of the drug in the seven days prior to the interview, reported by 51.21% of the interviewees, was related to financial factors, given that subjects with per capita monthly income from zero to US$250.00 had twice the odds of reporting such a difficulty when compared with those with per capita income greater than US$250.00. Lack of money to purchase medicine was identified as the main difficulty. Chambers et al. 18 call attention to low socioeconomic status in Jamaica, which the authors considered an important factor impacting adherence. Garcia Popa-Lisseanu et al. 22 also highlight low income as a barrier to adherence among patients in North America.
Adverse drug reactions occurred in a considerable percentage of patients, and prednisone was reported as the main drug involved. It is important to highlight that patients should receive information on probable adverse effects resulting from their treatment and on ways they should behave when such events occur. Approximately 20% of patients reduced the dose or stopped taking their medication when they noted some ADR. The possibility of a drug causing adverse events is often omitted by the prescriber, who may be fearful that negative information on the medicine will jeopardize the patient’s adherence to treatment or that the patient may even feel such an adverse event due to self-suggestion. 23 Maintaining the medication even in the face of some negative symptom during its use increased the odds of adherence by 81% among those who continued taking the medication as compared with those that suspended it. Chambers et al., 18 Garcia-Gonzales et al., 17 and Garcia Popa-Lisseanu 22 identified ADRs as a determinant factor in adherence.
Cruciol-Souza et al. 24 (2008) considered the importance of self-rated health for treatment adherence and thus for the efficacy of drug treatment. According to the authors, patients first assess the actions of the prescribed drugs and what they themselves know and think about the disease and the medicines, and then choose whether or not to adhere to the medical prescriptions. In the study, patients with positive self-rated health showed higher odds of adhering to treatment when compared with those with negative self-rated health. However, the perceived efficacy of drug treatment did not show a statistically significant relationship, unlike the results obtained by Garcia Popa-Lisseanu et al., 22 who observed low perceived efficacy as a barrier to treatment adherence in 22 patients with SLE and 18 with rheumatoid arthritis in Houston, Texas.
Family support was strongly associated with adherence, corroborating other authors who described it as a highly important factor for treatment adherence in various chronic diseases. 7,25 It is necessary to understand issues related to patients and the sociocultural setting to which they belong. Persons who are isolated from family and social contact may be more likely not to adhere to treatment.
Patients with joint involvement or mucocutaneous manifestations showed higher odds of not adhering to treatment. These results corroborate the findings of Mosley-Williams et al. 21 and Garcia Popa-Lisseanu et al. 22 when evaluating barriers to adherence in African-Americans, noting that episodes of pain, fatigue, and functional incapacity were reported by patients as reasons for not taking their medication as prescribed.
Every medication was explained and discussed with each patient by the physician responsible for the consultation and, exclusively regarding anticoagulation, brochures were handed to the patients. Nonetheless 30% of patients considered the medical prescription illegible. Patients with less than a complete secondary education showed twice the odds of not understanding the medical prescription (OR = 2.18, 95% CI = 1.20–3.96, p < 0.05) when compared with those with complete secondary or university education. Patients reporting that they could understand the physician’s handwriting had 55% greater odds of being adherent when compared with those who could not. This is a complex and controversial issue. The quality of the prescription and patient chart plays a crucial role in drug treatment. The main factor conferring such importance in both the hospital and outpatient setting is the interconnection it provides among the entire health team. Another closely related and (even more important) factor is that the prescription is the instrument that guarantees implementation of key pillars in the proper use of medicines. 24
Evaluating the results obtained with the instruments employed here, the data analysis shows that the factors identified in the multiple logistic regression with the proposed hierarchical model were: behavior towards the presence of an adverse drug reaction, hematological alterations, presence of mucocutaneous manifestations, legibility of the medical prescription, schooling, and family support.
One of the study’s limitations was selecting the method for measuring treatment adherence, given the lack of a gold standard. Estimating adherence by counting pills would not have been possible. SLE is not covered by programs for access to medicines through a regular supply of treatment in the hospital pharmacy at the health unit where the study was performed. Quantifying attendance at outpatient appointments during a given time period would also have been impossible; when the data were collected, this information was not available on the patient charts, so it was limited to self-reporting by patients. Using clinical results to evaluate treatment adherence would assume that there was a direct relationship between clinical recovery and adherence. However, even though the patient adheres, the drug treatment may fail to produce the desired effect.
Given the above, and within Brazil’s public health reality, we chose to use a structured interview, which may overestimate the number of patients defined as adherent, but which is easy to apply and allows evaluating the reasons why adherence fails to occur.
Based on the literature search and using the search tools mentioned above, we verified that this is one of the few studies in a developing country to evaluate treatment adherence in SLE, since we found only the study by Chambers et al. 18 (2008) which evaluated factors influencing TA in SLE in a group of patients in Jamaica.
We found that treatment adherence is a complex and multifactorial problem, present in both developed and developing countries.
The hierarchical modeling proposed here proved to be a good alternative for evaluating adherence, since it allowed visualizing the various stages in the analysis. There is no perfect model, and it is up to the researcher to review and evaluate the selected model using statistical methods and to decide (based on prior knowledge) which model best meets the study’s objectives.
Knowledge of the profile of patients with SLE in outpatient care and identification of factors related to lack of adherence to drug treatment allow preparing a set of suggestions and public health measures aimed at planning and implementing healthcare policies for this group of patients, thus ensuring improved quality of life for them.
Amongst the suggestions we highlight a few: patients should receive information on probable adverse effects resulting from their treatment and on ways they should behave when such events occur; stimulate family support as a highly important factor for treatment adherence; quantify clinic attendance and contact all missing patients since recurrent non-attendance may constitute an alert factor; brochures should be handed to the patients regarding most frequent SLE clinical course and disease complications, importance of adherence to most frequently used medication (steroids, immunosuppressive agents and anti-hypertensive drugs); improve affordability and availability of all SLE treatment drugs at outpatient clinics. We believe the problem of access to medicines is not unique to Brazil, but it affects a vast majority of countries in Latin America. Chambers et al., 18 assessing adherence to medication in Jamaica, also report difficulty of access. In Brazil only the high-cost medications are provided free of charge by the government.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.