
Abstract
Diffuse alveolar haemorrhage (DAH) is a rare but life-threatening complication of systemic lupus erythematosus (SLE). Specific therapy is based on a heavy immunosuppressive treatment that usually associates corticosteroid and cyclophosphamide boluses and plasma exchange. Despite this treatment, an early mortality rate of 20–50% is reported in the literature. Immunosuppression-related complications are responsible for further mortality and morbidity. Rituximab, a specific anti-CD20 antigen B-cell antibody, has been used with success for the treatment of several refractory autoimmune disorders, but rarely for SLE-induced DAH. We report here the first case of SLE-induced DAH treated successfully with rituximab without cyclophosphamide administration in a patient intolerant to cyclophosphamide. We review the two other cases of SLE-induced DAH managed with rituximab as a part of the immunosuppressive regimen.
Introduction
Diffuse alveolar haemorrhage (DAH) is a life-threatening manifestation occurring in less than 5% of systemic lupus erythematosus (SLE) patients. 1 Early mortality rates ranging from 20% to 50% are reported in the small published series of the literature. 1,2 After exclusion of differential diagnosis, specific therapy must be started immediately and usually includes an aggressive immunosuppression regimen associating high-dose steroids and cyclophosphamide (CYC). We report here a case of severe DAH in a young SLE male successfully treated with rituximab (RTX).
Case report
The patient, an 18-year-old White man, was diagnosed with SLE when he was 12. On diagnosis he presented with osteoarticular and skin involvement and classical biological features (positive antinuclear antibodies (ANA) and anti-dsDNA antibodies, and low C3 and C4 complement components). He had no antiphospholipid antibodies. A few months after the initial diagnosis, the patient developed a severe exacerbation, with fever, arthritis and nephritis treated with pulse corticosteroids and CYC. Immediately following the first CYC pulse he developed a severe bronchospasm and pulmonary infiltrates consistent with acute lung injury. At this time, imputability of CYC was retained on the basis of similar described cases in the literature and the patient was contra-indicated for further CYC administration. 3 SLE flare was controlled with corticosteroid treatment associated with mycophenolate mofetil. He developed three others mild articular flares between 2003 and 2008 managed with corticosteroid dose adaptations.
In January 2009, he was admitted to the intensive care unit (ICU) for septic shock secondary to cervical cellulitis. On ICU admission, his immunosuppressive treatment consisted of 15 mg/day of prednisone and 500 mg/day of mycophenolate mofetil. Septic shock was managed with conventional therapy associating fluid resuscitation, antibiotics administration and norepinephrine. He did not develop respiratory failure. Mycophenolate mofetil was withdrawn and prednisone was replaced by 300 mg/day of hydrocortisone. His condition improved rapidly in the next days and he was transferred to the nephrology’s department on day 7 from admission.
He was readmitted to the ICU on day 13 with dyspnoea and haemoptysis. On admission, he had acute respiratory failure that required mechanical ventilation, profound sedation, curarization and nitric oxide treatment. Chest X-ray and computed tomographic scan showed diffuse bilateral alveolar infiltrates (Figure 1) and hemodynamic monitoring demonstrated low capillary wedge pressure consistent with acute respiratory distress syndrome.
Chest computed tomography at diagnosis showing diffuse alveolar infiltrates.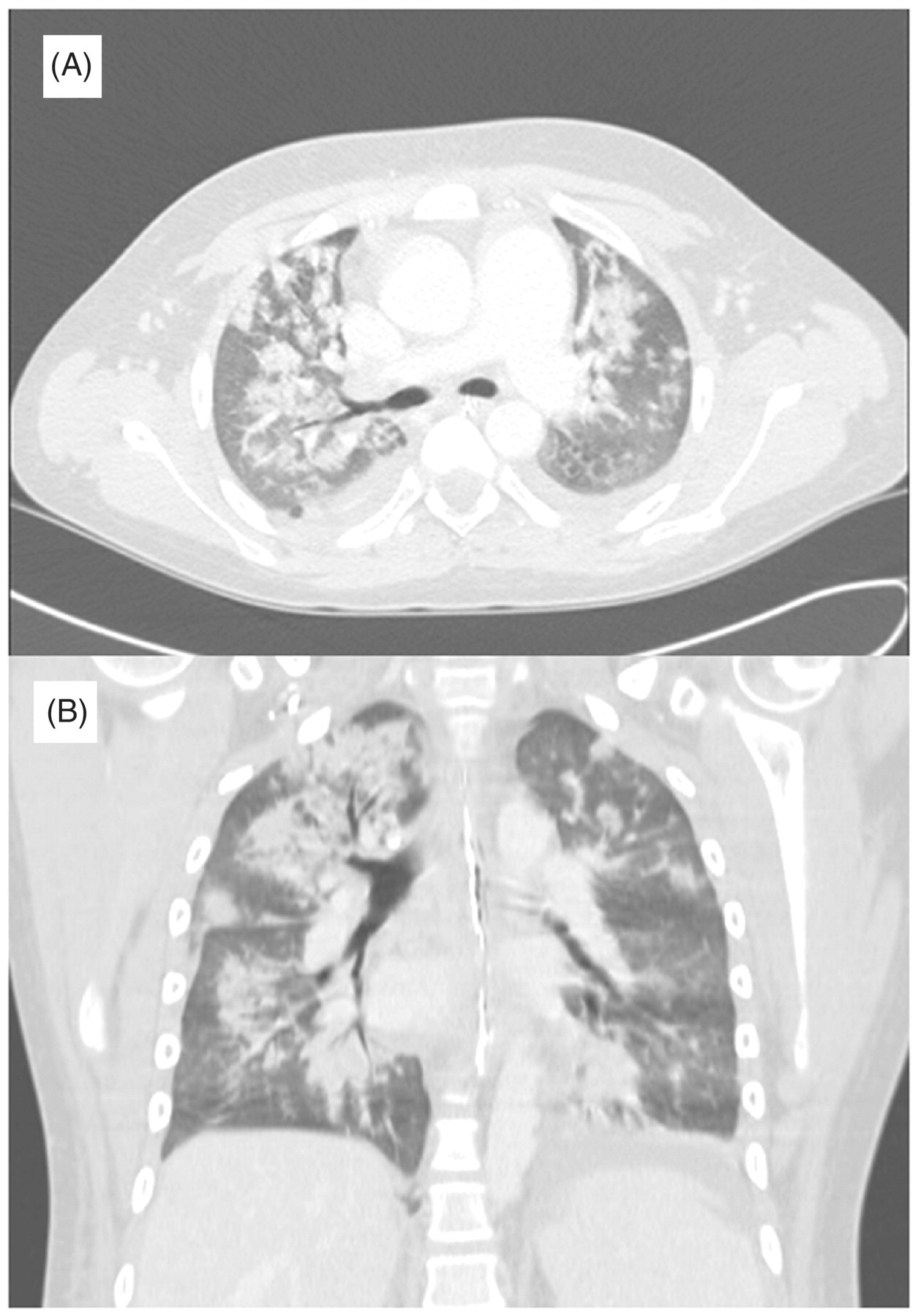
Bronchoalveolar lavage (BAL) revealed a haemorrhagic return suggesting DAH. Bacterial, viral and parasitic cultures and stains of BAL remained negative. Immunological analyses were consistent with SLE flare: ANA titre was 1/1280, anti-dsDNA antibodies 92.7 IU/ml (normal value, <20 IU/ml), complement C3 28 mg/dl (normal range, 75–146 mg/dl), and complement C4 5 mg/dl (normal range, 15–39 mg/dl), CH 50 40% (normal value, >70%). Haemoglobin level fell from 12 g/dl before admission to 8 g/dl on admission.
The diagnosis of DAH was then considered and the patient received 2 g/day of mycophenolate mofetil and 1 g/day of intravenous methylprednisolone for 3 days, followed by 1 mg/kg/day. In addition, daily plasma exchanges with albumin substitution were administered for 3 days. Despite this treatment, after 6 days, the respiratory condition worsened and the patient required ventilation with 100% FiO2. At this time, RTX was considered as a salvage therapy. He received 715 mg (375 mg/m2) of RTX at days 6 and 21, with an excellent tolerance. In the days following the first RTX injection, an improvement of his respiratory condition was observed. The patient was progressively weaned from sedation and extubation was allowed at day 20. B lymphocytes CD19-positive cells decreased from 21.1% to 0.1% 10 days after the second RTX injection. He was transferred to the nephrology department under a regimen of prednisolone 70 mg/day and mycophenolate mofetil 2000 mg/day on day 22. Up to now, no further SLE flare has occurred after 15 months of surveillance.
Discussion
This observation supports the hypothesis that RTX could be an alternative to CYC treatment in severe forms of SLE-induced DAH or in CYC-resistant forms of DAH.
The physiopathology of SLE-induced DAH has been poorly studied but is admitted to be an immune complex deposition disease. Histopathologic features include inflammatory cell interstitial infiltration, alveolar necrosis and an acute necrotizing capillaritis. Immune complex deposition (IgG and C3) is usually detected in alveolar and in small vessels walls. 4 Data reporting treatment effectiveness and patient’s outcome are scarce and derive from uncontrolled case series. 1,2 The literature suffers from considerable variability in the timing, dosing and treatment duration. A short time delay between disease occurrence and treatment initiation is crucial to maximize the chances of recovery. Standard regimens are based on a heavy immunosuppression associating high-dose steroids plus CYC and plasma exchange. In this setting, remission is achieved in most patients, but disease relapse and treatment-associated toxicity, particularly sepsis, contribute to the mortality and chronic incapacity. 5
Recent advances in SLE physiopathology have identified B-cell activation to take an important place in SLE physiopathology. 6 Autoantibody production, cytokine secretion and T–B cell cooperation are some of the functions that are aimed to be suppressed by depletive B-cell targeted therapies in SLE. RTX is a chimeric murine–human monoclonal antibody directed against the specific B-cell CD20 antigen. After RTX treatment, a reduced number B-cells are observed in the days following RTX administration. 6 The proposed mechanisms of action of RTX include antibody direct cellular toxicity, complement dependant cytotoxicity and B-cell-mediated receptor apoptosis.
Rituximab treatment in SLE patients with DAH
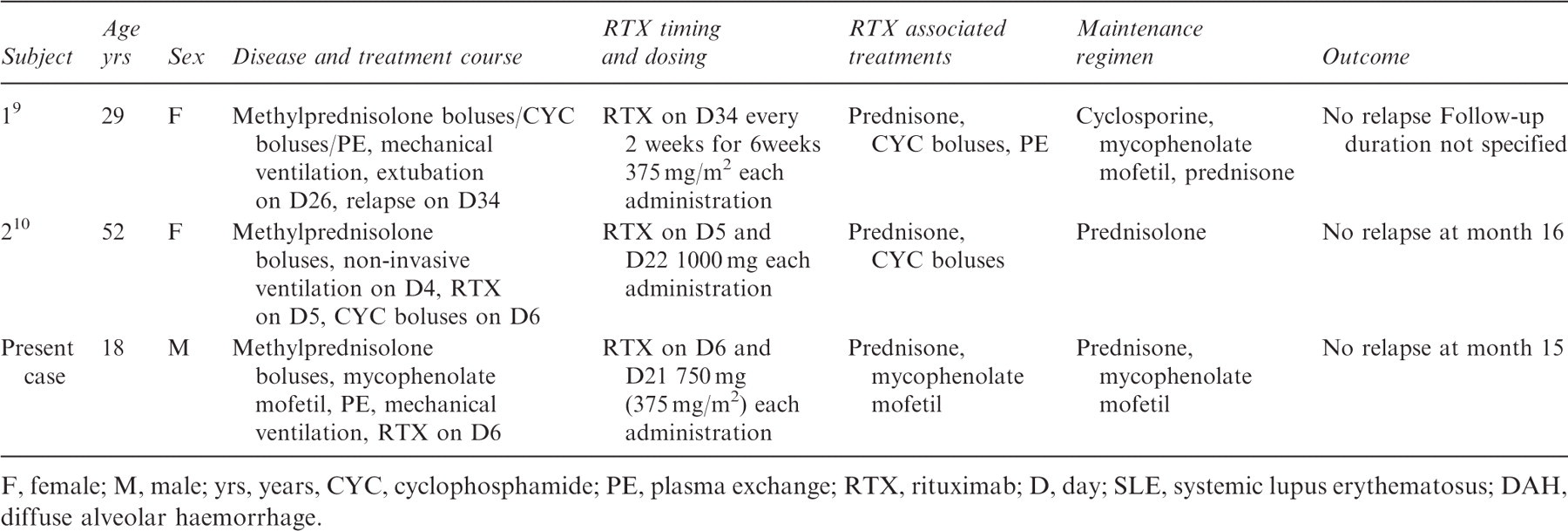
F, female; M, male; yrs, years, CYC, cyclophosphamide; PE, plasma exchange; RTX, rituximab; D, day; SLE, systemic lupus erythematosus; DAH, diffuse alveolar haemorrhage.
This observation suggests two potential benefits of RTX in SLE-induced DAH. The first is an early effect that may contribute to faster pulmonary recovery in severe forms or in CYC-resistant forms of SLE-induced DAH. The second is the long-term remission maintenance of the disease with the use of RTX as a cytotoxic sparing agent. Given its safety profile, RTX should be evaluated in further studies for the initial treatment of severe forms of SLE-induced DAH.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
None disclosed.