
Abstract
Ischaemic colitis is relatively uncommon in systemic lupus erythematosus (SLE), with only very few case reports or case series in world literature. Ischaemic colitis occurs when SLE activity is high and is inarguably due to small vessel vasculitis affecting the large or small intestine. Ischaemic proctitis with rectal ulceration, as a presenting feature in SLE, is even rarer with only two case reports in the world to date. We present the case of a 38-year-old woman, who presented with haematochezia which subsequently proved to be due to ischaemic proctitis with a large rectal ulcer in a case that was subsequently diagnosed as SLE. The clinical course in this patient greatly improved with aggressive management with systemic steroids.
Introduction
Colitis due to ischaemia can be due to varied reasons such as infection, neoplasms, drugs, post-operative, inflammatory conditions of the gut, hypercoagulable states, liver diseases and vasculitis syndromes. Systemic lupus erythematosus as a cause of ischaemic colitis is quite rare. 1 It is due to small vessel vasculitis affecting the gut circulation which can be confirmed by a sigmoidoscopy and histopathology. 2 We present a case of ischaemic colitis, in the form of a large rectal ulcer, in a patient with SLE whose primary presentation was haematochezia.
Case report
A 38-year-old lady, a mother of two teenage boys without any history of previous foetal loss, presented to our outpatient department with chief complaints of bloody diarrhoea associated with severe bouts of colicky lower abdominal pain for a period of 1 month. She also complained of chronic symmetric inflammatory non-deforming polyarthritis, significant loss of weight, anorexia and low-grade fever for a period of 3 months. On further questioning, she revealed that there was no history of skin or mucosal rash, oro-genital ulcerations, jaundice, haematuria, chest pain, palpitations or cough associated with her symptoms. Two years previously she had a past history of right-sided pleural effusion, which was treated empirically at a local hospital as tubercular pleural effusion with combination antitubercular drugs for 6 months and resolved.
On examination, she was anaemic and febrile (101°F), with a blood pressure of 130/70 mmHg and a pulse rate of 84 beats/min, without any significant lymphadenopathy and with features of arthritis involving the distal and proximal interphalangeal joints, wrist joints, elbow, knee and ankle joints bilaterally. The skin examination was within normal limits. Systemic examination revealed a diffusely tender lower abdomen without any palpable organomegaly or free fluid in the abdomen. Her baseline complete blood count revealed a haemoglobin level of 10.3 g/dl, total leukocyte count of 8500 cells/mm3 (normal 4500–10,500 cells/mm 3 ) with neutrophilic predominance, an erythrocyte sedimentation rate of 48 mm in the first hour (Westergren), C-reactive protein (CRP) 0.4 mg/dl (normal <0.5 mg/dl), a normal liver and renal function test. Urine routine examination revealed active sediment with 14–15 pus cells and 10–12 red blood cells (RBCs)/high-power field, granular and RBC cast. Twenty-four-hour urinary protein excretion was 850 mg.
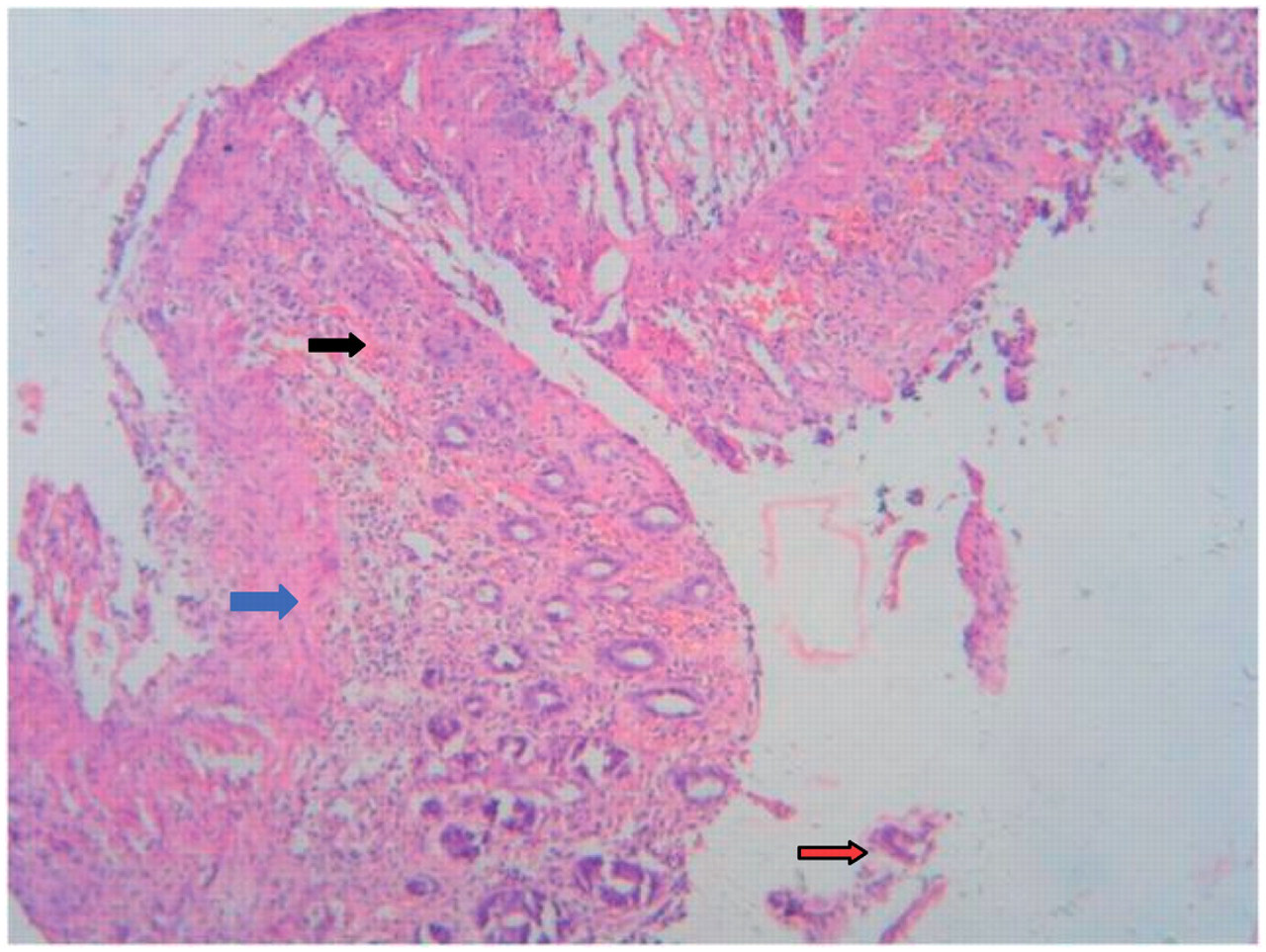
An antinuclear antigen (ANA) test performed by immunofluorescence technique in Hep 2 cell line showed strong positivity with a dilution of 1 : 320 (normal <1 : 40) with a homogenous pattern. An anti-double stranded DNA was strongly positive, with a value of 43.2 IU/ml (normal <5.30 IU/ml). The evaluation of complement levels revealed a low CH50, a C3 level of 52 mg/dl (normal 84–151 mg/dl) and a C4 level of 28 mg/dl (normal 17–40 mg/dl). IgG and IgM anti-phospholipid antibody was negative. Serum homocysteine level was within normal range. Electrocardiography, chest roentgenogram (PA View) and an abdominal ultrasonography revealed no significant findings. A colonoscopy revealed a large irregular rectal ulcer with yellowish exudates and with contact bleeding; the rest of the colon was free from the disease (Figure 1). Histopathological examination of the biopsy taken from the ulcerated region revealed small vessel narrowing with lymphocytic infiltration suggestive of small vessel vasculitis and eosinophilic glazing of the lamina propria layer with atrophy of crypts and superficial necrosis, suggestive of ischaemia (Figure 2).
Large rectal ulcer with dirty exudates and contact bleeding points. Areas of small vessel narrowing (black arrow) with eosinophilic glazing of the lamina propria (blue arrow) and superficial necrotic areas (red arrow): rectal mucosal histopathology, H&E Stain, 400×.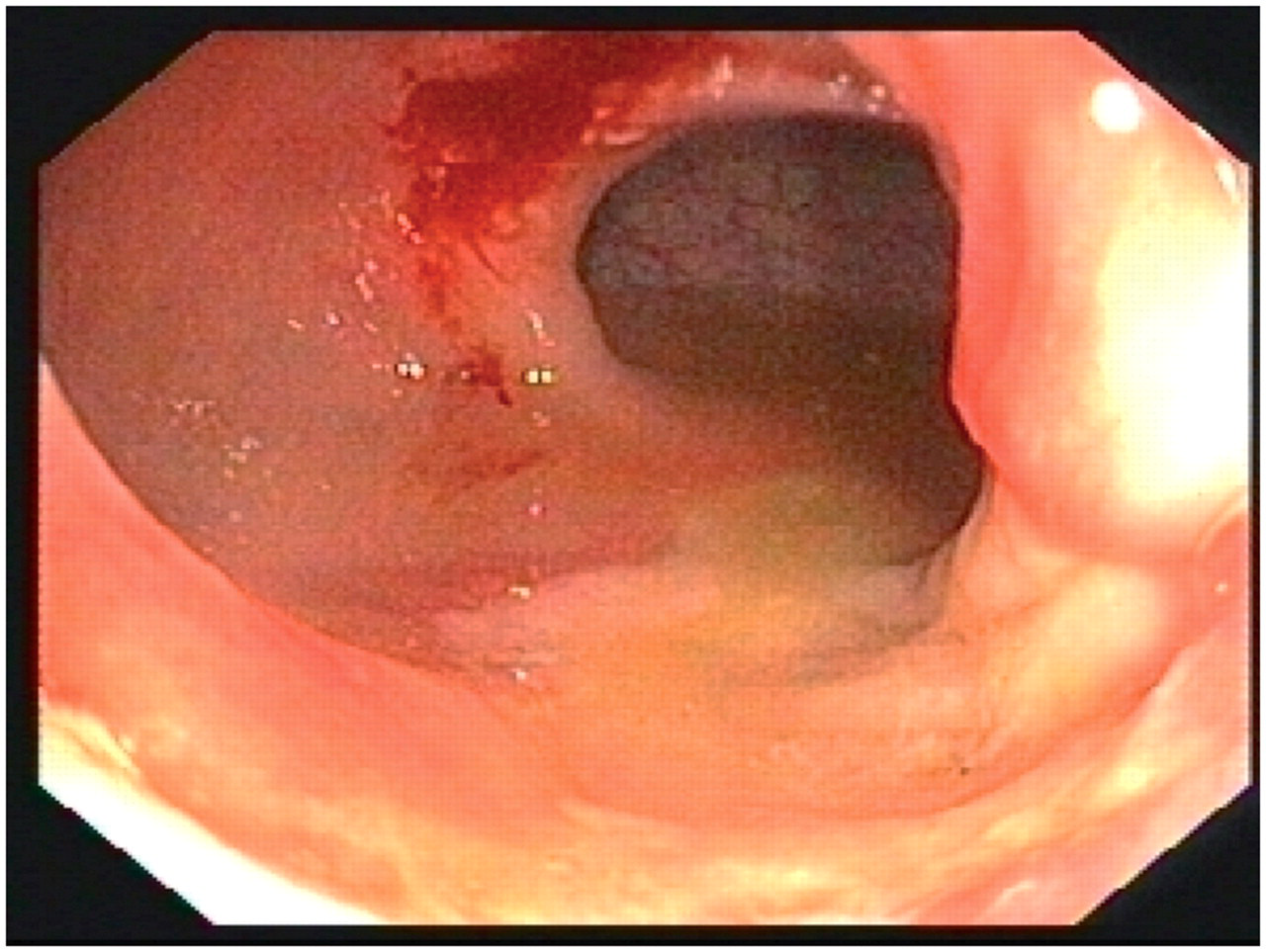
Hence, a diagnosis of ischaemic colitis (proctitis with a solitary rectal ulcer) in a patient with active SLE was made and the patient started on intravenous (IV) methylprednisolone for 6 days, followed by corticosteroid suppositories, proper antibiotic cover, IV fluid support and bowel rest. The patient improved steadily over the next 5 days; symptoms resolved with improvement of nutritional status. She was discharged on the 15th day of hospital stay with an advice to continue oral steroids at the dose of 1 mg/kg/body weight.
Discussion
Common causes of haematochezia in an adult are namely haemorrhoids, diverticulosis, colorectal carcinoma, inflammatory bowel disease, solitary rectal ulcer and massive upper gastrointestinal (GI) bleed. Ischaemic colitis is a rare cause of haematochezia. History, clinical findings, endoscopy and subsequent histopathological study of biopsy specimen usually resolves the diagnostic difficulty.
The bowel involvement in lupus enteritis is usually due to widespread fibrinoid vasculitis and multifocal, as multiple vessels are involved. The small bowel, especially the jejunum and ileum, is mostly involved. 3 Ischaemic colitis in SLE is very rare occurring in 0.2% patients and when present, can be life threatening especially if there is a delay in diagnosis. 4 Owing to its rich and multiple vascular supplies, the rectum is relatively protected. Lupus enteritis is the most common cause of lower GI bleeds with severe abdominal pains in a known patient of SLE as the incidence varies from 0.2% to 53%. 3 – 5 Difficulty occurs in an undiagnosed patient of SLE presenting with lower abdominal pain and lower GI bleed.
GI vasculopathy in SLE is seen mostly due to immune complex mediated vascular damage, during heightened activity of SLE. Diverse predisposing factors, namely embolism, thrombosis, vasospasm, drugs (steroids and immunosuppressive agents), vasculitis, performed colonoscopy and enema, are responsible for ischaemic colitis in SLE caused by decreased blood perfusion of mesenteric vasculature.
There is no histopathological hallmark of SLE enteritis. 6 Even then, features of vasculitis admixed with features of ischaemia in the biopsy specimen usually point to the diagnosis and the cause. In the presence of constellations of clinical, laboratory and characteristic immunological findings, a diagnosis of ischaemic colitis secondary to SLE can be made with certainty. The vasculitis usually does not affect the medium and large vessels of the intestine. A case of abdominal manifestation of SLE if diagnosed promptly, in the absence of surgical indications, can be managed by way of systemic steroids, antibiotics and fluid support. There have been case reports of ischaemic colitis in SLE affecting the rectal region. This is the rarest part of the lower GI system to be affected in SLE. 7,8 Even rarer is SLE presenting primarily as isolated ischaemic proctitis. 9,10 Our patient came to us with similar presentation with isolated ischaemic rectal ulcer. Successful treatment of ischaemic colitis in SLE has been reported before with systemic corticosteroids only. 3,5 Even relapse cases during tapering of oral steroid respond well to IV methylprednisolone. 3
In conclusion, haematochezia and abdominal pain in SLE can also be due to ischaemic colitis with excellent outcome on timely treatment with corticosteroids. Treating physicians should always rule out ischaemic colitis as a differential diagnosis in a known SLE or suspected SLE patient with similar constellations of clinical findings.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
None declared.