
Abstract
The antiphospholipid syndrome (APS) is defined by the presence of thrombosis and/or pregnancy morbidity in combination with the persistent presence of circulating antiphospholipid antibodies: lupus anticoagulant, anticardiolipin antibodies and/or anti-β2-glycoprotein I antibodies in medium to high titers. The management of thrombosis in patients with APS is a subject of controversy. This set of recommendations is the result of an effort to produce guidelines for therapy within a group of specialist physicians in Cardiology, Neurology, Hematology, Rheumatology and Internal Medicine, with a clinical and research focus on APS.
Keywords
Introduction
The antiphospholipid syndrome (APS) is defined by the presence of thrombosis and/or pregnancy morbidity in combination with the persistent presence of circulating antiphospholipid antibodies (aPL): lupus anticoagulant (LA), anticardiolipin antibodies (aCL) and/or anti β2 glycoprotein I antibodies (anti-β2 GPI) in medium to high titers. Specific clinical and immunological criteria have been developed to classify patients as having definite APS. 1
The management of thrombosis in patients with APS is a subject of controversy. On the one hand, APS is well known as an acquired thrombophilia affecting approximately 20% of young patients with venous thromboembolism or stroke, 2,3 with observational studies suggesting high recurrence rates in untreated patients. 4 On the other hand, lifelong oral anticoagulation is associated with an increased rate of serious bleeding, which is higher as the international normalized ratio (INR) increases; the inconvenience of regular INR testing is also a factor influencing the quality of life. Thus, any therapeutic decision would potentially face the risk of either insufficient antithrombotic coverage or excessive exposure to major side effects. Moreover, there is also a potential need for primary thromboprophylaxis in individuals with aPL who have not yet suffered any thrombosis.
Recently, two systematic reviews 4,5 and an academic review, 6 all published in high-impact journals, included treatment recommendations. However, some controversial management issues remain unresolved, particularly with respect to patients with APS and cerebral arterial events. Primary thromboprophylaxis has been less extensively investigated.
In the setting of the 13th International Congress on Antiphospholipid Antibodies, held in Galveston in April 2010, an international Task Force composed of clinicians and researchers with experience in the field jointly elaborated a consensus document on the primary and secondary thromboprophylaxis in individuals with aPL, after a systematic and critical review of the literature.
Methods
The group identified five key questions to be answered by the literature review: What is the risk of first thrombosis in lupus patients with aPL, women with purely obstetric APS, and asymptomatic healthy aPL carriers? What is the risk of recurrent events in untreated patients with APS and previous thrombosis (arterial and venous)? What are the factors that influence the risk of vascular events (first or recurrent) in patients with aPL? Is primary thromboprophylaxis with aspirin and/or hydroxychloroquine effective and safe? What is the best treatment to prevent recurrent thrombosis in patients with aPL and arterial or venous events fulfilling and not fulfilling criteria for APS?
A systematic literature review using PUBMED and EMBASE was performed using the following strategies: (Antiphospholipid syndrome OR antiphospholipid antibodies OR Lupus coagulation inhibitor OR anticardiolipin antibodies OR beta 2-Glycoprotein I) AND Thrombosis (all the 16 MeSH headings) NOT review NOT Children NOT Recurrent (Antiphospholipid Syndrome OR Lupus Anticoagulant OR Phospholipid Antibody) AND (Therapy OR Anticoagulant Therapy) (“Antiphospholipid Syndrome/drug therapy”[MeSH] OR “Antiphospholipid Syndrome/therapy”[MeSH]) AND “Thrombosis”[MeSH] “Antibodies, Antiphospholipid”[MeSH] AND (“Thrombosis/drug therapy”[MeSH] OR “Thrombosis/therapy”[MeSH]) Antibodies, Antiphospholipid/blood*[MESH] AND recurrence[MESH].
Papers containing original data relevant to the clinical questions were selected. Additional papers were obtained by scanning the references of the selected articles. Data were extracted by three authors (GR-I, M-JC, IR-A) and summarized in tables. The tables and the complete reference list were then distributed among the members of the Task Force. The entire group met on 13 April 2010 in a preconference workshop of the 13th International Congress on Antiphospholipid Antibodies. A preliminary consensus document was agreed and distributed among the members of the Task Force for further discussion.
American College of Chest Physicians grades of recommendation (modified from Guyatt GH, et al) 7
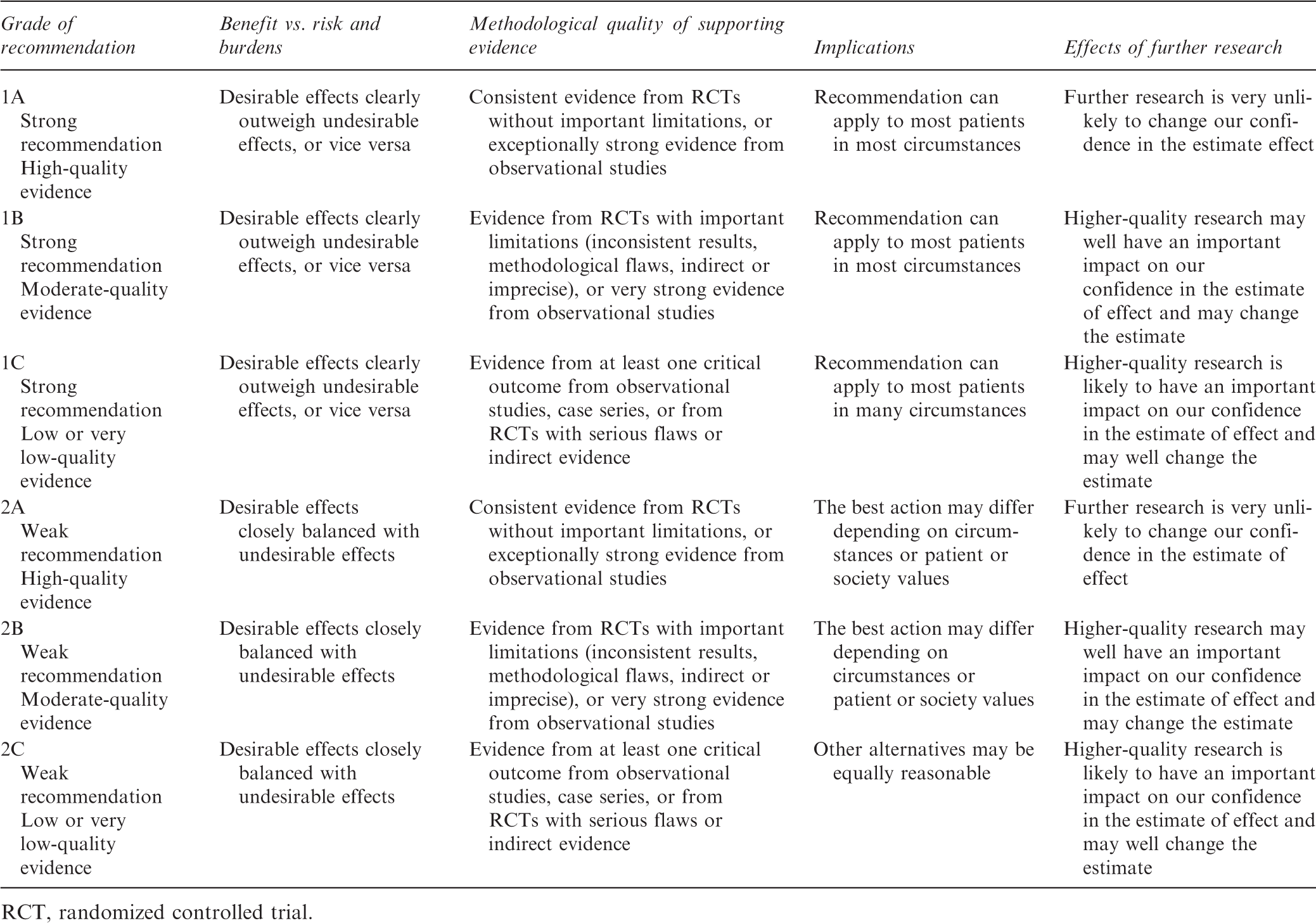
RCT, randomized controlled trial.
Recommendations
General background
aPL increase the risk for thrombotic events. 8 However, the relationship between aPL and thrombosis is not ‘all or nothing’. Circulating aPL should be considered a thrombotic risk factor, with several other variables modulating the final clinical expression. 9 Among these, the most important are the aPL profile (type, level and persistence), the coexistence of other thrombotic risk factors, and the presence of an underlying autoimmune disease.
The classical systematic reviews by Galli et al. established LA as the individual aPL most strongly related to thrombosis. 10,11 On the other hand, isolated anti-β2-GPI were weakly associated with clinical manifestations of APS. 11,12 This has been recently confirmed in a population-based case-control study of Dutch women under 50 years of age, 203 with myocardial infarction, 175 with ischemic stroke and 628 healthy controls: 13 LA positivity increased the risk of stroke 48-fold, and the risk of myocardial infarction 11-fold. Anti-β2-GPI only doubled the risk of stroke, but not of myocardial infarction. The role of aCL in the absence of LA is more debated, with no associated increased risk for stroke or myocardial infarction in the Dutch study. 13 It must be noted, though, that single aPL determinations were performed in this study.
Two observational studies suggested that patients with systemic lupus erythematosus (SLE) and isolated medium–high titer, persistently positive aCL (defined as more than 2/3 of serial determinations positive) had an increased risk for thrombosis, while those with occasional aCL positivity did not. 14,15 On the other hand, combined aPL positivity has been associated with increasing thrombotic risk, 16,17 with the so-called triple-positive population (LA plus aCL plus anti-β2-GPI) being the highest risk group. 15,18,19 Individuals with multiple positive aPL tend to have more stable antibody levels on repeated determinations. 20 This probably reflects the fact that aPL levels are routinely much higher in this group. 9
The role of vascular risk factors in patients with APS has become more clear. aPL patients presenting with thrombosis frequently have one or several additional cardiovascular risk factors such as hypertension, smoking, hypercholesterolemia or estrogen use. The co-existent presence of these factors is associated with thrombosis. 21–25 Moreover, the interaction between aPL and smoking and oral contraceptives has been clarified in the case-control study by Urbanus et al.: 13 the risk for suffering a stroke doubled among smoking LA-positive women, as compared with non-smokers; the risk of stroke among oral contraceptive users multiplied more than sevenfold. All LA-positive women who suffered a myocardial infarction smoked.
The influence of concomitant SLE may also impact the risk of thrombosis. SLE is a risk factor for thrombosis in isolation. Patients with SLE have a higher than expected incidence of vascular events, 26 not completely explained by traditional vascular risk factors. 27 The combination of SLE and aPL is particularly worrisome, since aPL positivity has been shown to increase the risk of thrombosis in patients with lupus, 14,15,28,29 and the diagnosis of SLE appears to further enhance the likelihood of vascular events in patients with aPL. 30–32 Observational studies suggest that manifestations of APS other than clinical classification criteria, such as heart valve lesions, 15 livedo reticularis, 33 and thrombocytopenia 24,25 may be associated with thrombosis; however, such association is not considered strong enough to guide clinical decisions.
High- and low-risk serological features in patients with antiphospholipid antibodies
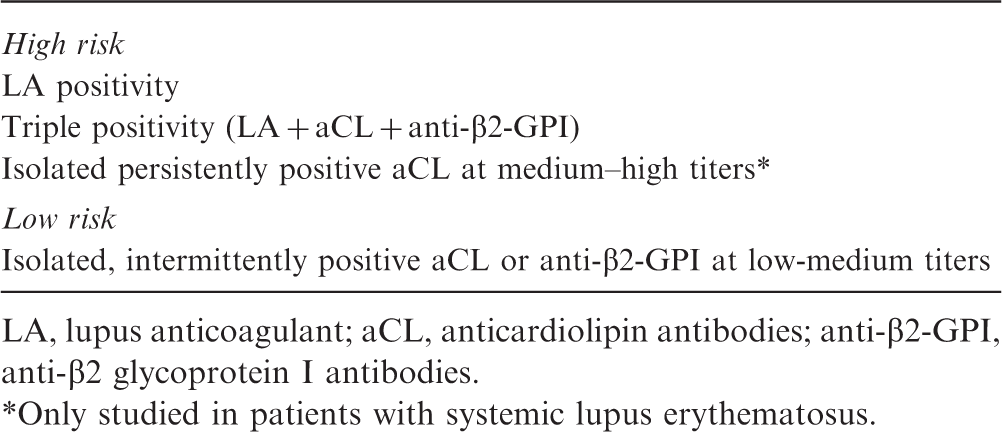
LA, lupus anticoagulant; aCL, anticardiolipin antibodies; anti-β2-GPI, anti-β2 glycoprotein I antibodies.
Only studied in patients with systemic lupus erythematosus.
1. General measures for aPL carriers
1.1. A strict control of cardiovascular risk factors should be accomplished in all individuals with a high-risk aPL profile, irrespective of the presence of previous thrombosis, concomitant SLE or additional APS features.
1.2. We recommend that all aPL carriers receive thromboprophylaxis with usual doses of low molecular weight heparin in high-risk situations, such as surgery, prolonged immobilization and the puerperium.
Rationale
There is no study addressing the effect of controlling cardiovascular risk factors on the risk of thrombosis in individuals with aPL. However, given the consistent association of these factors with vascular events in the general population as well as in APS patients (see ‘General background’), the recommendation of an adequate management of hypertension, obesity and dyslipidemia and the avoidance of smoking and estrogen-containing therapy is warranted.
In addition, observational studies suggest that standard thromboprophylaxis in high-risk periods, such as surgery or the puerperium, is effective. 24,25
2. Primary thromboprophylaxis in SLE patients with aPL
2.1. Clinicians should regularly assess patients with SLE for the presence of aPL.
2.2. We recommend that patients with SLE and positive LA or isolated persistent aCL at medium–high titers receive primary thromboprophylaxis with hydroxychloroquine
Note: Some members of the Task Force (DE, RD, SK, VP) suggest hydroxychloroquine use in this setting with a grade
Rationale
Primary thrombosis rates in patients with antiphospholipid antibodies
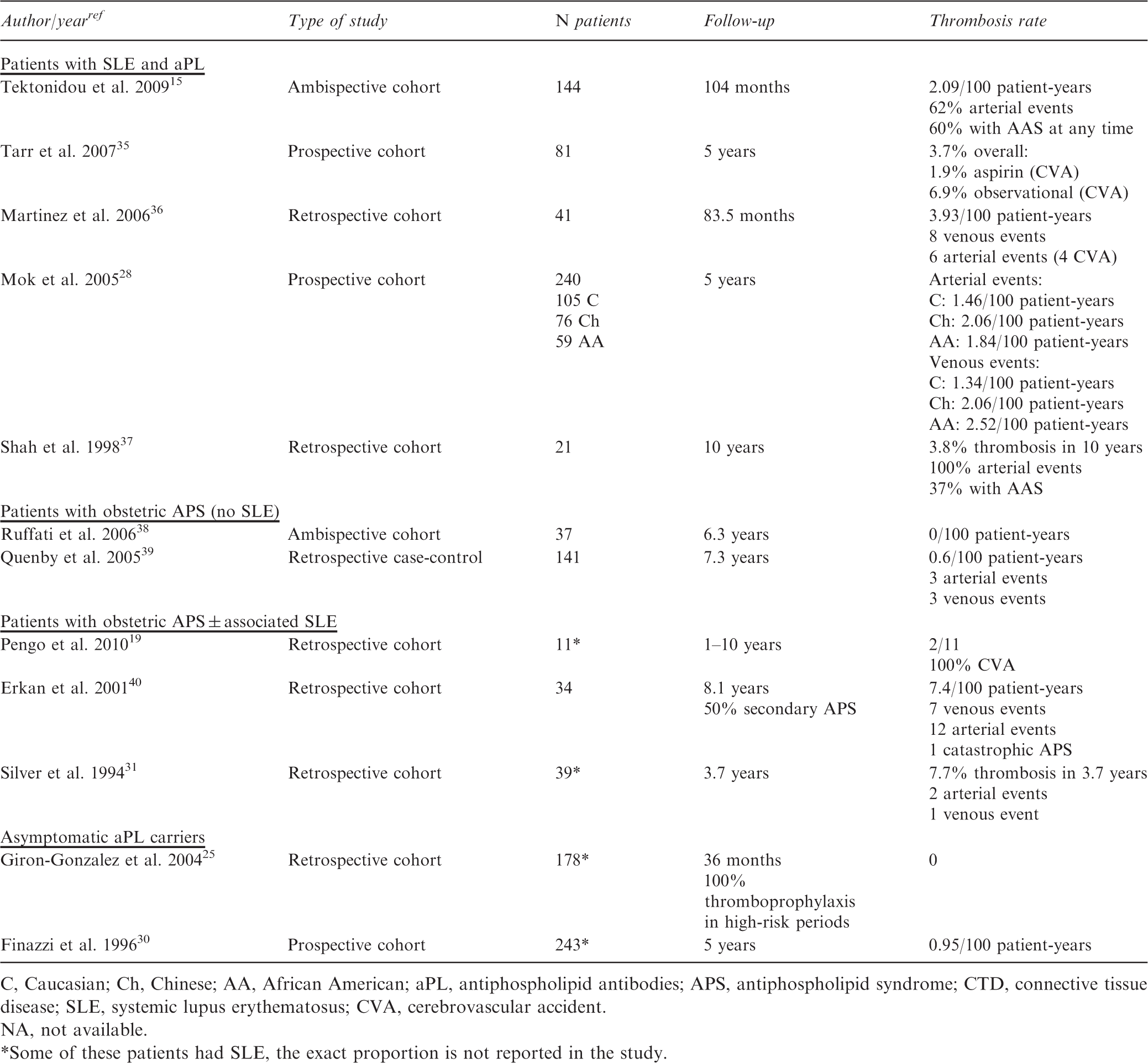
C, Caucasian; Ch, Chinese; AA, African American; aPL, antiphospholipid antibodies; APS, antiphospholipid syndrome; CTD, connective tissue disease; SLE, systemic lupus erythematosus; CVA, cerebrovascular accident.
NA, not available.
Some of these patients had SLE, the exact proportion is not reported in the study.
A recent systematic review has found moderate-quality evidence that antimalarials have antithrombotic effects in patients with SLE. 42 Such effects are further supported by a case-control study that found a significant reduction of thromboembolic events over 2-year follow-up in SLE patients treated with hydroxychloroquine. 43 In the subgroup of lupus patients with aPL, observational studies also point to a protective effect of hydroxychloroquine against thrombosis. 15,44
Moreover, moderate and high-quality evidence provides support that antimalarials decrease damage accrual and increase the survival of lupus patients, respectively, with little associated toxicity. 42 Thus, hydroxychloroquine is currently recommended as baseline therapy in all lupus patients without known contraindications. 42
Primary intervention studies in patients with antiphospholipid antibodies
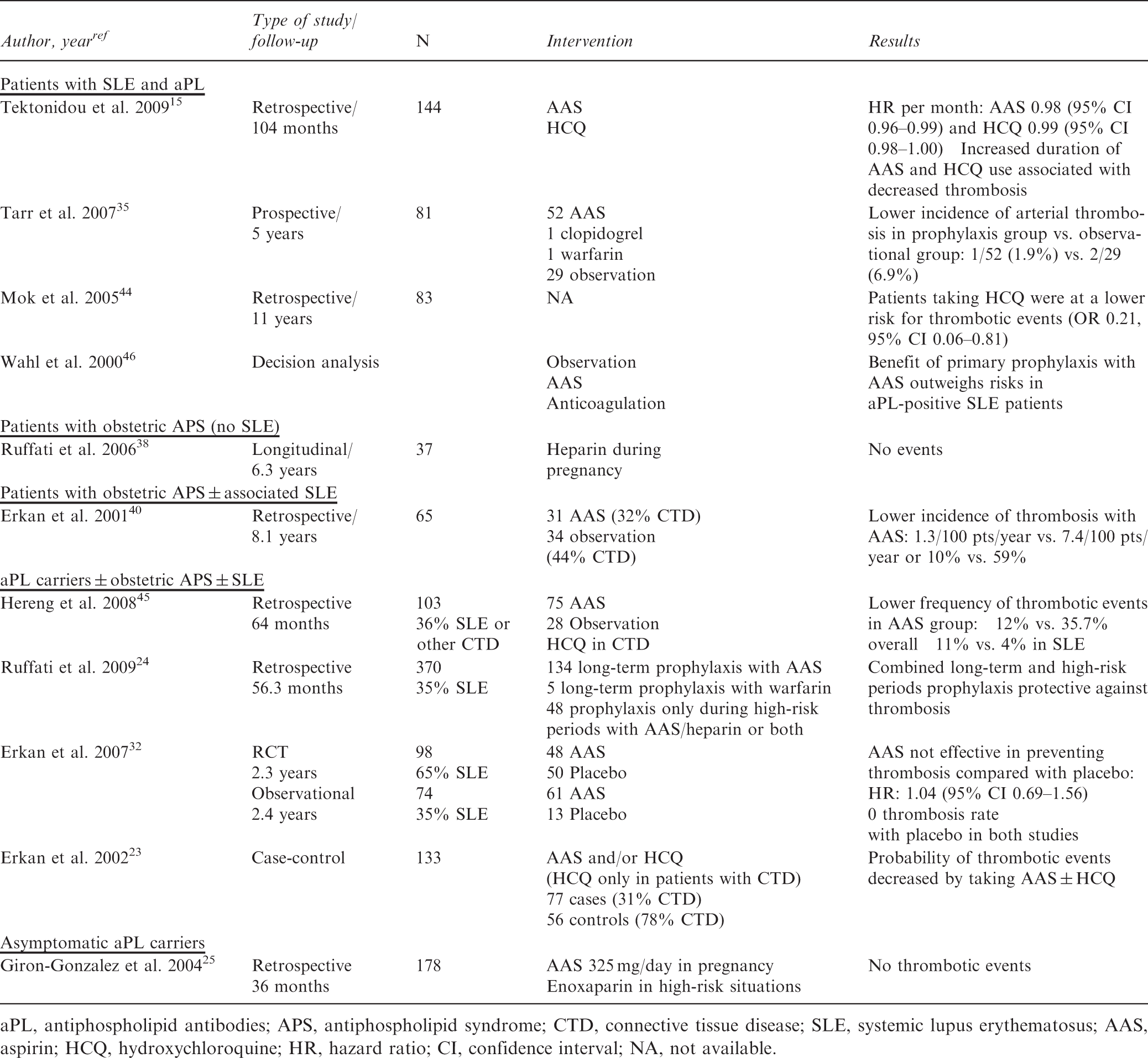
aPL, antiphospholipid antibodies; APS, antiphospholipid syndrome; CTD, connective tissue disease; SLE, systemic lupus erythematosus; AAS, aspirin; HCQ, hydroxychloroquine; HR, hazard ratio; CI, confidence interval; NA, not available.
No studies have analyzed whether the combination of both therapies (antimalarials plus low-dose aspirin) increases the efficacy of primary thromboprophylaxis in this group of patients with SLE and aPL.
3. Primary thromboprophylaxis in aPL-positive individuals without SLE
3.1. In non-SLE individuals with aPL and no previous thrombosis, we suggest long-term thromboprophylaxis with low-dose aspirin in those with a high-risk aPL profile, especially in the presence of other thrombotic risk factors.
Rationale
The actual risk of thrombosis in aPL-positive individuals without SLE is not well established, since reported incidence data vary considerably (Table 3). APS-associated obstetric morbidity in the absence of SLE has not been clearly associated with a higher risk of thrombosis. 31,39 In the study by Ruffatti et al., women with obstetric APS who had thrombosis during the subsequent follow-up had all suffered previous thromboembolic events and were triple aPL positive. 38 Likewise, the risk of thrombosis in healthy individuals with aPL as an incidental finding seems low. 25 The APLASA clinical trial, performed in a mixed population of individuals with and without a concomitant connective tissue disease, did not find differences between placebo and low-dose aspirin 32 (see previous section for comments regarding this study).
Based on this evidence, universal thromboprophylaxis with aspirin cannot be recommended for asymptomatic carriers of aPL. However, there is some concern that those with a high-risk aPL profile (Table 2), especially if combined with additional thrombotic risk factors, could be at a higher risk for subsequent vascular events; thus, therapy with aspirin could be considered in such individuals.
4. Secondary thromboprophylaxis
4.1. We recommend that patients with either arterial or venous thrombosis and aPL who do not fulfill criteria for APS be managed in the same manner as aPL-negative patients with similar thrombotic events.
4.2. We recommend that patients with definite APS and a first venous event receive oral anticoagulant therapy to a target INR 2.0–3.0.
Rationale
A recent systematic review has concluded, based on subgroup analyses, that patients with aPL and thrombosis who do not fulfill laboratory criteria for APS have rates of recurrent events with standard therapy similar to aPL-negative patients. 4
For patients with definite APS who present with non-recurrent venous thromboembolism, standard anticoagulation to a target INR 2.0–3.0 is effective in preventing further events, while higher-intensity anticoagulation has not been demonstrated to decrease the rate of recurrences in two randomized controlled trials. 47,48 Although the quality of these studies was limited by the insufficient anticoagulation in a substantial number of patients randomized to the high-intensity arm, the low frequency of recurrent events seen in all groups supports the efficacy of standard intensity anticoagulation in this clinical setting. 4
4.3. Patients with definite APS and arterial thrombosis should be treated with warfarin at an INR >3.0 or combined antiaggregant-anticoagulant (INR 2.0–3.0) therapy.
Note: Some members of the Task Force (MC, DE, RD, SK, VP) believe that other options such as antiaggregant therapy alone or anticoagulant therapy to a target INR 2.0–3.0 would be equally valid in this setting.
Rationale
Recurrent thrombosis rates in studies published after 2007
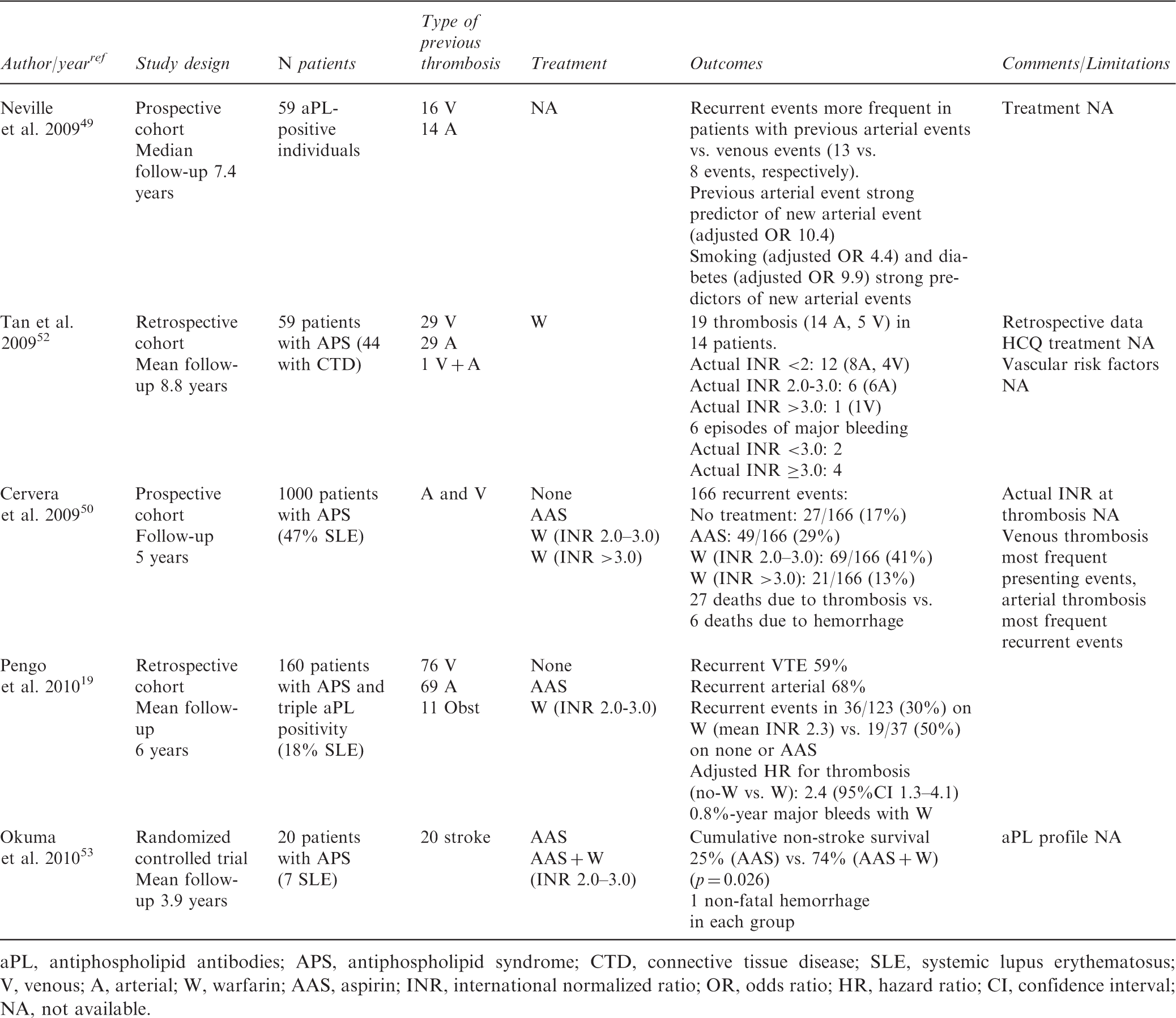
aPL, antiphospholipid antibodies; APS, antiphospholipid syndrome; CTD, connective tissue disease; SLE, systemic lupus erythematosus; V, venous; A, arterial; W, warfarin; AAS, aspirin; INR, international normalized ratio; OR, odds ratio; HR, hazard ratio; CI, confidence interval; NA, not available.
In addition to these observational studies, a small randomized controlled trial, enrolling 20 Japanese APS patients with stroke with a mean age below 50 years, compared combined therapy with warfarin (target INR 2.0–3.0) plus low-dose aspirin with aspirin alone. 53 Combined therapy was statistically more effective, with a low frequency and severity of bleeding in both groups (Table 5). This study is subject to important limitations (lack of data regarding aPL profiles, lack of data on the actual number and type of events in each group, one patient with atrial fibrillation treated with aspirin only); however, it is the only randomized controlled trial focused on arterial events in APS and opens the door to the use of combined antiaggregant–anticoagulant drugs as first-line therapy in patients with APS and stroke.
Some authors (GR-I, M-JC, IR-A, RB, SM, SP, MT, MK) agree that more intense therapy, such as oral anticoagulation to an INR higher than 3.0 or combined therapy with warfarin, INR 2.0–3.0, and low-dose aspirin should be indicated in patients with APS presenting with arterial thrombosis. Other members of the panel (MC, RD, DE, SK, VP) believe that other options (antiaggregant therapy alone or warfarin INR 2.0–3.0) are equally valid alternatives. We all agree that the evidence supporting any option must be considered low quality (grade C).
4.4. An estimation of the patient’s bleeding risk should be performed before prescribing high-intensity anticoagulant or combined antiaggregant-anticoagulant therapy.
Rationale
Estimating the patient’s bleeding risk is essential before starting long-term anticoagulant therapy, particularly in patients who are candidates to receive high-intensity anticoagulation or combined therapy. The risk of major bleeding increases with rising INRs; however, the relationship is not linear, with a sharp increase at INRs >4.0–5.0. 54 Concomitant aspirin therapy doubles the risk of bleeding in patients on oral anticoagulants. 54,55 A dose of 100 mg/day is safer than higher doses. 54 Age over 75 years, history of severe bleeding, polypharmacy, insufficient education on anticoagulant therapy, malignancy 54 and the presence of leukoaraiosis 56 have all been related to a higher frequency of hemorrhages.
4.5. Non-SLE patients with a first non-cardioembolic cerebral arterial event, with a low-risk aPL profile and the presence of reversible trigger factors, could individually be considered candidates to treatment with antiplatelet agents.
Rationale
The authors agree that the relative influence of aPL in the development of thrombosis may vary among individual patients. As discussed in the general background, patients with SLE and those with strongly positive LA, especially if accompanied by other aPL (triple-positive patients), seem to be at the highest risk for thrombosis, whether first or recurrent, while those with isolated low–medium titer aCL or anti-β2-GPI seem to be at the other end of the spectrum, even if fulfilling laboratory criteria for APS. The low risk of recurrent stroke seen in some cohorts of APS patients treated with low-dose aspirin, with a minority of them being concurrently positive for aCL and LA, 57 may reflect the different clinical behavior of this subgroup.
Thus, even with the current lack of clinical data to support this recommendation, the authors agree that patients with non-cardioembolic stroke and a low-risk aPL profile (non-SLE with single, not persistent, low–medium level aCL or anti-β2-GPI positivity), especially in the presence of a reversible risk factor such as smoking or estrogenic therapy, could be individually considered candidates to antiaggregant treatment instead of prolonged high-intensity anticoagulation.
Taking into account the high prevalence of cardiac valve abnormalities seen in patients with APS, 58 it would be important to exclude a cardioembolic source according to established guidelines. 59,60 However, in a recent study by the APASS group, within a well-recognized cohort with stroke and low-risk aPL profile treated with aspirin or warfarin, the simultaneous presence of either valvular thickening or patent foramen ovale – detected by transesophageal echocardiography – and aPL – in a single determination – did not increase the risk of subsequent events. 61 Thus, further studies in patients fulfilling laboratory APS criteria are needed before recommending specific screening of cardioembolic sources in the subpopulation with low-risk aPL profile.
5. Duration of treatment
5.1. We recommend indefinite antithrombotic therapy in patients with definite APS and thrombosis.
5.2. In cases of first venous event, low-risk aPL profile and a known transient precipitating factor, anticoagulation could be limited to 3–6 months.
Rationale
In patients with venous thromboembolism, it has been shown that the presence of single aCL increases the risk of recurrent thromboembolism within 6 months of anticoagulation withdrawal. 62 In the retrospective study by Khamashta et al., 63 the frequency of thrombosis rose sharply shortly after stopping anticoagulant therapy. Moreover, long-term therapy (whether antiaggregant or anticoagulant) is recommended in the general population with stroke, 64 and recent guidelines suggest indefinite oral anticoagulation for all patients with unprovoked venous thromboembolism in whom the bleeding risk is low. 65 Thus, the general rule of indefinite (lifelong) antithrombotic therapy generally applies to patients with APS and thrombosis, whether venous or arterial.
However, stopping oral anticoagulation 3–6 months after a venous thromboembolism due to a transient risk factor is adequate in the general population. 65 What if this clinical scenario is completed with single, not persistent, low–medium titers aCL or anti-β2-GPI: what we previously defined as low-risk aPL profile? (Table 2). There are no data to answer this question. However, as in the case of arterial events, the authors agree that this subgroup of patients would be candidates for less aggressive therapy, which may include a shorter duration of anticoagulant treatment. A recent Spanish series of six patients with venous thromboembolism with single aCL positive at least two times observed no episodes of recurrent thrombosis after a mean follow-up of 21 months after stopping oral anticoagulation following the eventual negativization of aCL. 66 Of note, four of these patients presented reversible risk factors for venous thrombosis.
A negative ultrasound screening for residual thrombosis as well as a negative D-dimers test after 3 months of anticoagulant therapy identify a population at low risk for recurrent thromboembolic events after stopping anticoagulation. 67,68 Although patients with aPL have been excluded from most of these studies, additional evaluation including these techniques could aid in taking the decision of withdrawing anticoagulation in this subgroup of patients with APS.
6. Refractory and difficult cases
6.1. In patients with difficult management due to recurrent thrombosis, fluctuating INR levels, major bleeding or a high risk for major bleeding, alternative therapies could include long-term low molecular weight heparin, hydroxychloroquine or statins.
Rationale
The utility of several alternative treatments for APS has been suggested by several studies, most of them observational. A small, low-quality randomized controlled trial has shown that combination therapy with low-dose aspirin and warfarin to an INR 2.0–3.0 is more effective than aspirin alone in the secondary prevention of stroke in patients with APS 53 (see ‘Secondary thromboprophylaxis’ section). However, no comparative studies against warfarin alone are available.
Very limited data suggest that long-term low molecular weight heparin can be an effective and safe alternative to warfarin in patients with APS. 69 Whether the response is similar in arterial and venous thrombosis and whether there is need for combining antiaggregant drugs are unresolved questions.
Statins have been shown to inhibit NF-κB, an important mediator of platelet activation and tissue factor over-expression induced by aPL. 70 Fluvastatin has been shown to inhibit aPL-induced tissue factor production in mouse models and in cultured human endothelial cells. 70 In a recent pilot trial in nine patients with APS treated with fluvastatin 40 mg/day for 30 days, decreased levels of inflammatory and thrombogenic mediators were seen after treatment. 71 Among non-APS patients, a decreased risk of venous thromboembolism has been shown in healthy people with normal cholesterol levels treated with rosuvastatin. 72 Thus, beyond lipid-lowering activity, statins could have an adjuvant role in preventing thrombosis in patients with aPL/APS, importantly, with no intrinsic additional risk of bleeding.
The antithrombotic properties of hydroxychloroquine in patients with aPL and SLE has already been noted 42 (see section ‘Primary thromboprophylaxis in patients with systemic lupus erythematosus’). Studies have shown that hydroxychloroquine reduces aPL-induced platelet activation and clotting and inhibits the formation of aPL-β2 GPI–phospholipid bilayer complexes. 70 Although clinical studies in patients with APS without SLE are lacking, hydroxychloroquine could be used as an adjuvant agent in patients with APS with difficult management, taking into account the excellent safety profile and the lack of associated bleeding. 42
Final remarks
Summary of recommendations
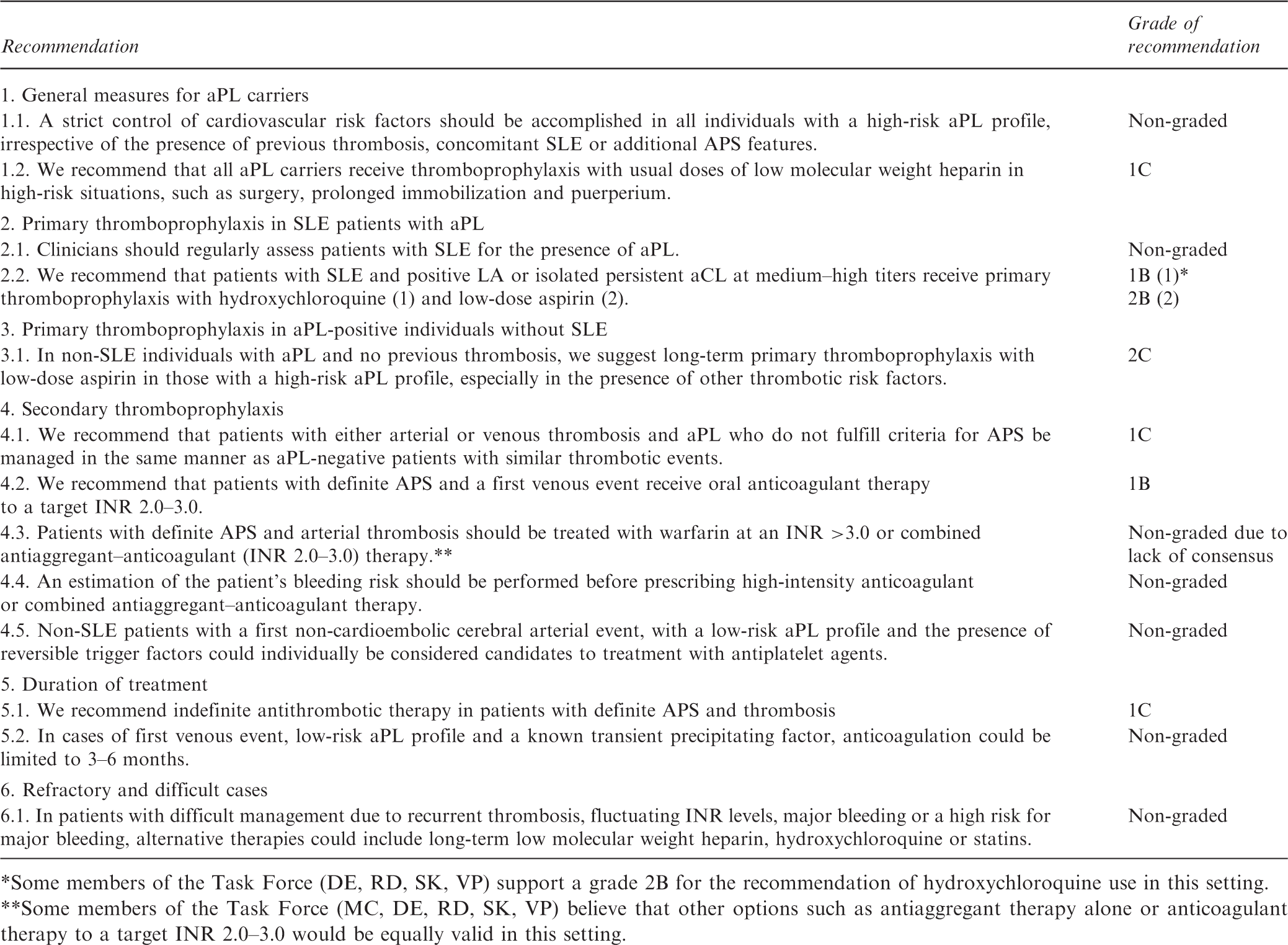
Some members of the Task Force (DE, RD, SK, VP) support a grade 2B for the recommendation of hydroxychloroquine use in this setting.
Some members of the Task Force (MC, DE, RD, SK, VP) believe that other options such as antiaggregant therapy alone or anticoagulant therapy to a target INR 2.0–3.0 would be equally valid in this setting.
In this set of recommendations, we acknowledge that the house of APS has more rooms than we initially believed. The categorization of different risk subgroups, using both clinical and immunological features (first versus recurrent thrombosis, arterial versus venous events, SLE versus non-SLE, single versus multiple aPL positivity, etc.), opens the door for more tailored therapy. Future advances in the detection of ‘real’ pathogenic aPL, such as antibodies against the domain I of β2-GPI, 73 will hopefully provide us with new tools to better define the risk profile of patients with APS.
Footnotes
Funding
Dr Ruiz-Irastorza is supported by the Department of Education, Universities and Research of the Basque Government.
Conflict of interest
The authors declare that they have no conflicts of interest.